Pleural effusion refers to the accumulation of fluid between the layers of the parietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: Anatomy and visceral pleuraVisceral pleuraPleura: Anatomy. Common causes of this condition include infection, malignancyMalignancyHemothorax, autoimmune disorders, or volume overload. Clinical manifestations include chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, cough, and dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea. Imaging can confirm the presence of a pleural effusion, and pleural fluid analysis can help in the evaluation of an etiology. Management is dependent on the underlying condition and whether the effusion is causing respiratory distress. Drainage of the effusion may provide symptomatic relief.
Pleural effusion is an excessive accumulation of fluid within the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy (between the parietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: Anatomy and visceral pleuraVisceral pleuraPleura: Anatomy).
Classification
Light’s criteria are used to categorize effusions and to guide further workup.
An effusion is classified as exudative if any of these 3 criteria are metMETPreoperative Care:
If these 3 criteria are not metMETPreoperative Care, the pleural effusion is considered transudative.
Etiology
Common causes of transudate:
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) (HF)
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: AnatomycirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
HypoalbuminemiaHypoalbuminemiaA condition in which albumin level in blood (serum albumin) is below the normal range. Hypoalbuminemia may be due to decreased hepatic albumin synthesis, increased albumin catabolism, altered albumin distribution, or albumin loss through the urine (albuminuria).Nephrotic Syndrome in Children
Nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome
Common causes of exudate:
PneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
MalignancyMalignancyHemothorax (most commonly a primary lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung Cancer)
Connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology diseases
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Transudative or exudative: pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism
The normal mean rate of production and absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of the pleural fluid is 0.2 mL/kg/hour.
The entire volume of pleural fluid normally turns over within 1 hour.
The lymphatic vesselsLymphatic VesselsTubular vessels that are involved in the transport of lymph and lymphocytes.Lymphatic Drainage System: Anatomy can handle flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of up to approximately 20 times more than the normal production rate → lymphatic resorption has a large reserve capacity
Transudative effusions
A transudative pleural effusion may result from increased fluid entry into the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis due to:
↑ Hydrostatic pressureHydrostatic pressureThe pressure due to the weight of fluid.Edema in the vasculature (e.g., HF)
↓ Oncotic forces in the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products (e.g., hypoalbuminemiaHypoalbuminemiaA condition in which albumin level in blood (serum albumin) is below the normal range. Hypoalbuminemia may be due to decreased hepatic albumin synthesis, increased albumin catabolism, altered albumin distribution, or albumin loss through the urine (albuminuria).Nephrotic Syndrome in Children)
Ascitic fluidAscitic fluidThe serous fluid of ascites, the accumulation of fluids in the peritoneal cavity.Ascites movement through the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy (e.g., hepatic hydrothoraxHydrothoraxA collection of watery fluid in the pleural cavity.Edema)
Exudative effusions
An exudative pleural effusion may result from:
↑ Capillary permeability → ↑ pleural levels of:
ProteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis
Cells
Other plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products contents (depending on the etiology)
Impaired lymphatic drainage from:
Malignant infiltration or blockage of the lymphatics
Some pleural effusions may be asymptomatic. Symptoms may vary and can depend on the severity and cause of the effusion.
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea (most common)
Pleuritic chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways:
Indication of pleural inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
PalpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination:
TracheaTracheaThe trachea is a tubular structure that forms part of the lower respiratory tract. The trachea is continuous superiorly with the larynx and inferiorly becomes the bronchial tree within the lungs. The trachea consists of a support frame of semicircular, or C-shaped, rings made out of hyaline cartilage and reinforced by collagenous connective tissue. Trachea: Anatomy is shifted to the opposite side of the effusion.
Seen in large, severe effusions
Auscultation:
↓ or inaudible breath sounds over the effusion
Bronchial breath sounds, bronchophony, and egophony:
Heard over the lung parts directly above the effusion
PercussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination:
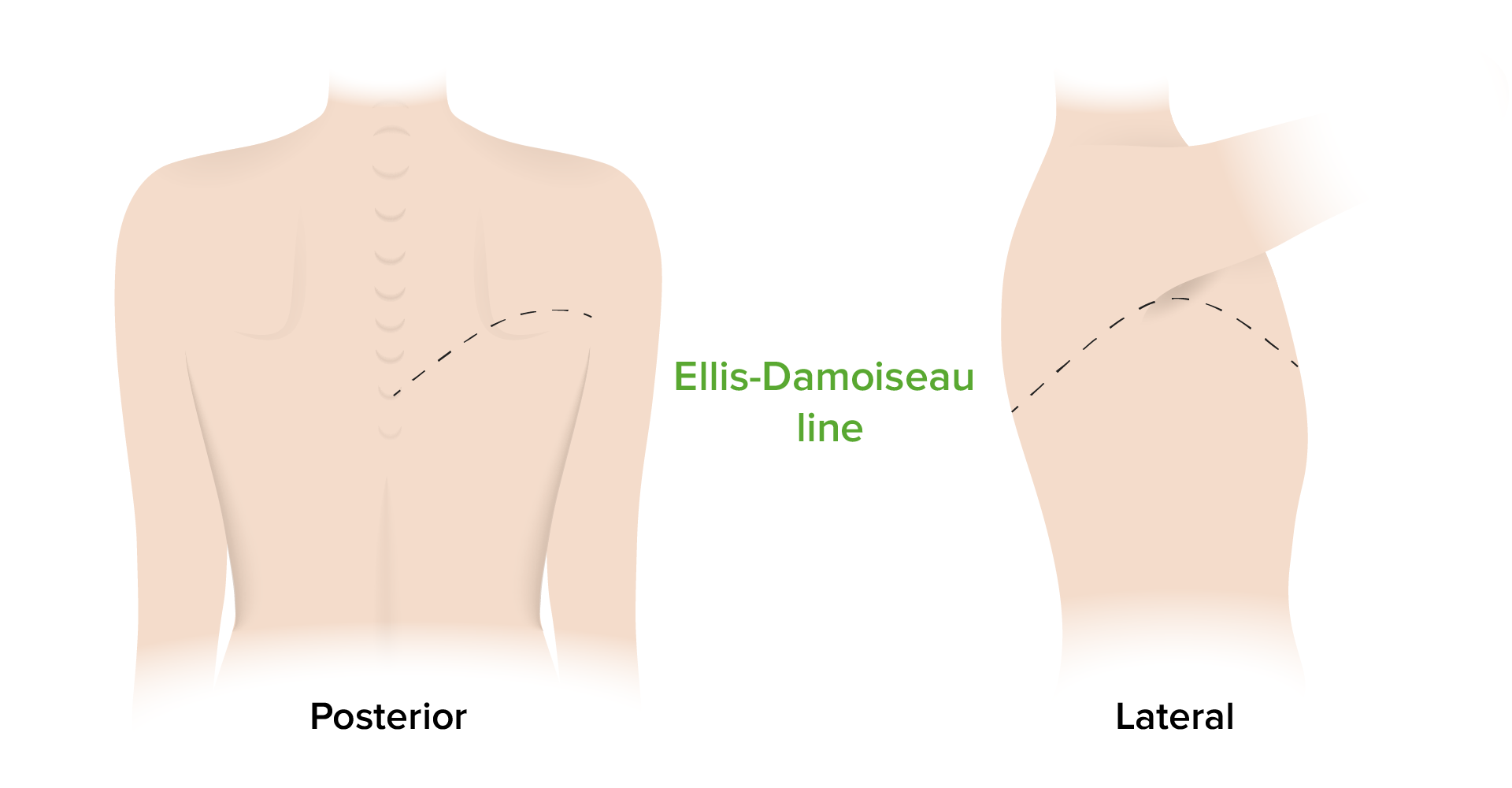
In the case of an effusion > 300 mL, chest examination will also be notable for dullness to percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination.
Ellis–Damoiseau line: This drawing depicts the shape that dullness to percussion will follow when assessing for a pleural effusion.
Image by Lecturio.
Indications of an underlying etiology
Parapneumonic effusions (adjacent to a pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia) can present with signs of sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock or septic shockSeptic shockSepsis associated with hypotension or hypoperfusion despite adequate fluid resuscitation. Perfusion abnormalities may include, but are not limited to lactic acidosis; oliguria; or acute alteration in mental status.Sepsis and Septic Shock.
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Transudative effusions may be associated with:
Weight gain
Peripheral edemaPeripheral edemaPeripheral edema is the swelling of the lower extremities, namely, legs, feet, and ankles.Edema
Pleural effusions are often easily detected on imaging.
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests:
Can demonstrate fluid layering (free-flowing pleural effusion)
CT of the chest:
Can detect small amounts of pleural fluid
Able to evaluate the entire lung parenchyma and mediastinumMediastinumThe mediastinum is the thoracic area between the 2 pleural cavities. The mediastinum contains vital structures of the circulatory, respiratory, digestive, and nervous systems including the heart and esophagus, and major thoracic vessels.Mediastinum and Great Vessels: Anatomy for potential etiologies
Ultrasonography:
High sensitivity for diagnosis of pleural effusions
Can detect small amounts of pleural fluid that may be missed on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests examination
Often used to visualize the effusion for thoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery or chest tube placementTube placementSurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Thoracic Surgery
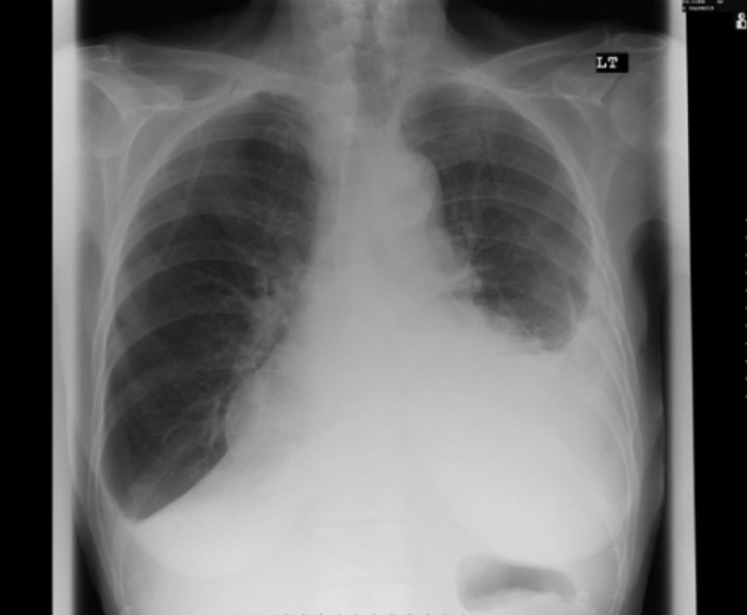
X-ray image of a massive right-sided pleural effusion with complete opacification of the right hemithorax and tracheal deviation to the left
Image: “X-ray of patient’s chest revealing a right-sided pleural effusion” by Department of Gastroenterology, Queen’s Hospital, Burton-on-Trent, West Midlands, UK. License: CC BY 2.0
X-ray image showing bilateral pleural effusions: Note the blunting of the costophrenic angle (particularly on the right) and the appearance of a meniscus on the left.
Image: “Pleural effusion while being on carbimazole” by Department of Diabetes and Endocrinology, Glan Clwyd Hospital, Rhuddlan Road, Bodelwyddan, Rhyl LL18 5UJ, UK. License: CC BY 3.0
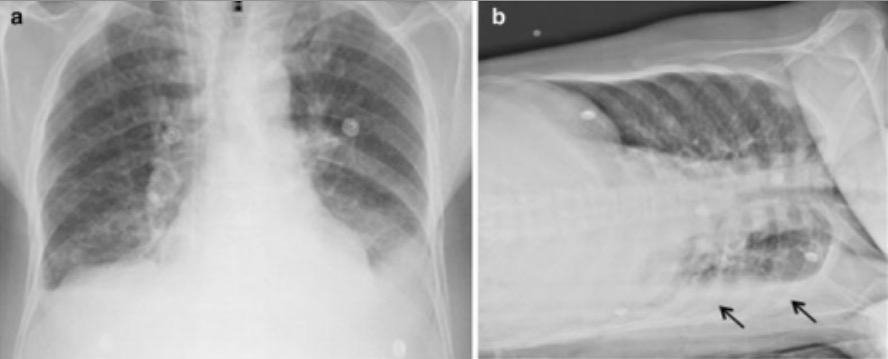
X-ray images demonstrating bilateral pleural effusions:
a: Blunting of both costophrenic angles is shown.
b: A lateral decubitus image shows layering of fluid due to a left pleural effusion (arrows).
Image: “Radiologic findings” by Departamento de Clínica Médica, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo (USP), Ribeirão Preto, São Paulo, 14049-900, Brazil. License: CC BY 4.0, cropped by Lecturio.
CT image demonstrating bilateral pleural effusions in a patient with pulmonary silicosis: The bilateral, crescent-shaped, opacified regions below the lungs are the effusions.
Image: “Chest CT” by Internal Medicine Department, St. Luke’s Hospital, Chesterfield, MO 63017, USA. License: CC BY 3.0
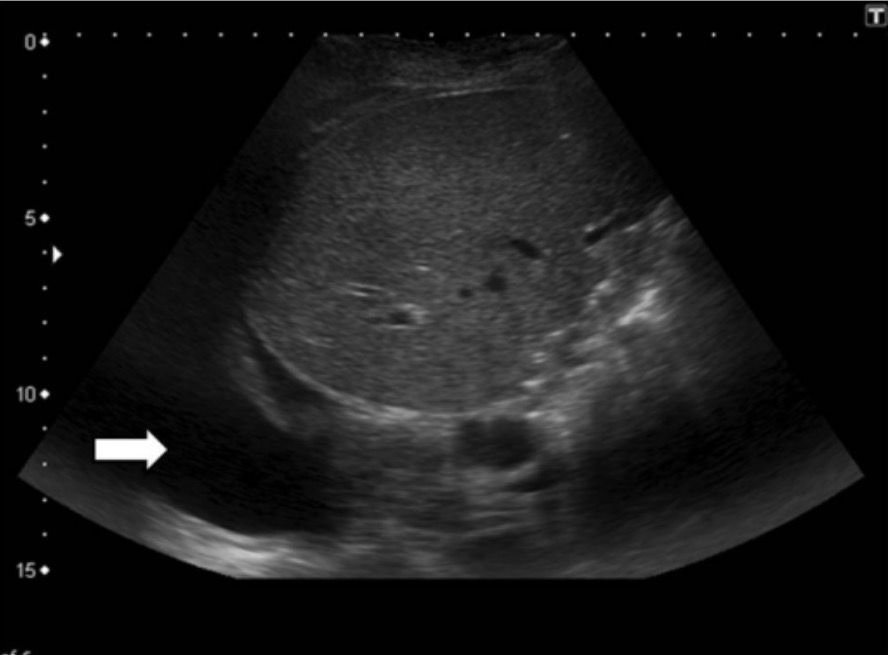
Ultrasound image demonstrating a pleural effusion (arrow pointing at the hypoechogenic region)
Image: “Pleural effusion” by Department of Radiology/Interventional Radiology, Institute of Liver and Biliary Sciences, Vasant Kunj, New Delhi, India. License: CC BY 4.0
Imaging considerations
Some imaging findings may help narrow the list of potential causes of the pleural effusion.
Bilateral pleural effusions:
Most commonly seen in volume overload states (e.g., HF)
Differential diagnosis should also include malignancyMalignancyHemothorax, lupus, and constrictive pericarditisConstrictive pericarditisInflammation of the pericardium that is characterized by the fibrous scarring and adhesion of both serous layers, the visceral pericardium and the parietal pericardium leading to the loss of pericardial cavity. The thickened pericardium severely restricts cardiac filling. Clinical signs include fatigue, muscle wasting, and weight loss.Pericarditis.
Complicated parapneumonic effusion or empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
Loculated effusions:
Caused by adhesions between contiguous pleural surfaces
Most commonly associated with higher inflammatory states (e.g., empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia, hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax, TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis)
Pleural fluid analysis
Once a pleural effusion is found, the next step is to sample the pleural fluid by performing thoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery.
Routine investigations include:
Pleural fluid should be sent for:
Cultures and microscopy
BacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology
FungiFungiA kingdom of eukaryotic, heterotrophic organisms that live parasitically as saprobes, including mushrooms; yeasts; smuts, molds, etc. They reproduce either sexually or asexually, and have life cycles that range from simple to complex. Filamentous fungi, commonly known as molds, refer to those that grow as multicellular colonies.Mycology
Cytology
Cell count with differential
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance
AlbuminAlbuminSerum albumin from humans. It is an essential carrier of both endogenous substances, such as fatty acids and bilirubin, and of xenobiotics in the blood.Liver Function Tests
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance
AlbuminAlbuminSerum albumin from humans. It is an essential carrier of both endogenous substances, such as fatty acids and bilirubin, and of xenobiotics in the blood.Liver Function Tests
Additional investigations include (based on clinical suspicion):
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption → pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, esophageal ruptureEsophageal ruptureEsophageal rupture or perforation is a transmural defect that occurs in the esophagus, exposing the mediastinum to GI content. The most common cause of esophageal perforation is iatrogenic trauma by instrumentation or surgical procedures.Esophageal Perforation
Rheumatoid factorRheumatoid factorAntibodies found in adult rheumatoid arthritis patients that are directed against gamma-chain immunoglobulins.Autoimmune Hepatitis and antinuclear antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions → autoimmune disorders
Acid-fast bacilliAcid-fast bacilliMycobacterium smear and adenosineAdenosineA nucleoside that is composed of adenine and d-ribose. Adenosine or adenosine derivatives play many important biological roles in addition to being components of DNA and RNA. Adenosine itself is a neurotransmitter.Class 5 Antiarrhythmic Drugs deaminase → TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
Common pleural fluid investigations and associated diagnoses
Fluid analysis
Findings
Associated diagnosis
Fluid appearance
Straw color
Transudate
Pus
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
Bloody
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism
Milky
Chylothorax
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance
> 7.55
Normal pleural fluid
< 7.2
Complex parapneumonic effusion
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance
< 60 mg/dL
Complicated parapneumonic effusion
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
Autoimmune conditions
Malignant effusion
Cell count
WBC > 10,000 cells/µL
Parapneumonic effusion
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
Autoimmune conditions
Pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism
Neutrophil predominance
Bacterial infection
Lymphocytic predominance
TuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
AdenosineAdenosineA nucleoside that is composed of adenine and d-ribose. Adenosine or adenosine derivatives play many important biological roles in addition to being components of DNA and RNA. Adenosine itself is a neurotransmitter.Class 5 Antiarrhythmic Drugs deaminase
> 50 µg/L
TuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption
> 200 µg/dL
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Esophageal ruptureEsophageal ruptureEsophageal rupture or perforation is a transmural defect that occurs in the esophagus, exposing the mediastinum to GI content. The most common cause of esophageal perforation is iatrogenic trauma by instrumentation or surgical procedures.Esophageal Perforation
The following may be considered in the workup if the history, physical exam, imaging, and pleural fluid analysis do not reveal a diagnosis and the patient has worrisome symptoms (e.g., weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, persistent feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever).
Pleural biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma:
May be performed if there is clinical suspicion for malignancyMalignancyHemothorax or TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
Options:
Percutaneous needle biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma
Lymphatic fluid in the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy
High concentrations of lipidsLipidsLipids are a diverse group of hydrophobic organic molecules, which include fats, oils, sterols, and waxes.Fatty Acids and Lipids
A large amount of cloudy, milky fluid removed during a thoracentesis for a chylothorax
Image: “600 cubic centimeters of chyle removed from a chylothorax” by Matani S, Pierce JR. License: CC BY 3.0
Parapneumonic effusion
Exudative, neutrophilic pleural fluid associated with pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
Classification:
Uncomplicated
No bacterial invasion of the pleuraPleuraThe pleura is a serous membrane that lines the walls of the thoracic cavity and the surface of the lungs. This structure of mesodermal origin covers both lungs, the mediastinum, the thoracic surface of the diaphragm, and the inner part of the thoracic cage. The pleura is divided into a visceral pleura and parietal pleura. Pleura: Anatomy
Will resolve with management of the pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
Complicated
Bacterial invasion of the pleuraPleuraThe pleura is a serous membrane that lines the walls of the thoracic cavity and the surface of the lungs. This structure of mesodermal origin covers both lungs, the mediastinum, the thoracic surface of the diaphragm, and the inner part of the thoracic cage. The pleura is divided into a visceral pleura and parietal pleura. Pleura: Anatomy
BacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology are rapidly cleared from the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis → cultures are usually negative
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
Bacterial infection of the pleuraPleuraThe pleura is a serous membrane that lines the walls of the thoracic cavity and the surface of the lungs. This structure of mesodermal origin covers both lungs, the mediastinum, the thoracic surface of the diaphragm, and the inner part of the thoracic cage. The pleura is divided into a visceral pleura and parietal pleura. Pleura: Anatomy
Pleural fluid will be thick, viscous, and opaque (pus).
Can lead to fibrinFibrinA protein derived from fibrinogen in the presence of thrombin, which forms part of the blood clot.Rapidly Progressive Glomerulonephritis deposition and restriction of lung movement
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Accumulation of blood within the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy
Connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology or vascular disease
Pleural analysis will reveal:
Frank blood
↑ RBC count
Management
Initial management
Asymptomatic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship do not generally require treatment, and many will have spontaneous resorption of the effusion. However, the following should be done in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with symptoms:
Severe respiratory distress or respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
ThoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery:
Needle aspirationNeedle aspirationUsing fine needles (finer than 22-gauge) to remove tissue or fluid specimens from the living body for examination in the pathology laboratory and for disease diagnosis.Peritonsillar Abscess of pleural fluid
Diagnostic and therapeutic
Can be repeated if there is reaccumulation
Chest tube placementTube placementSurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Thoracic Surgery (tube thoracostomyTube ThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Thoracic Surgery):
Placement of a surgical tube into the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis
Critical in empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia and hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Indwelling pleural catheter:
Catheter that tunnels into the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis
Allows intermittent drainage of pleural fluid
Used in refractory pleural effusions (requiring frequent thoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery for recurrence, such as in malignancyMalignancyHemothorax)
Pleurodesis:
Obliteration of the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis by way of inducing inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans
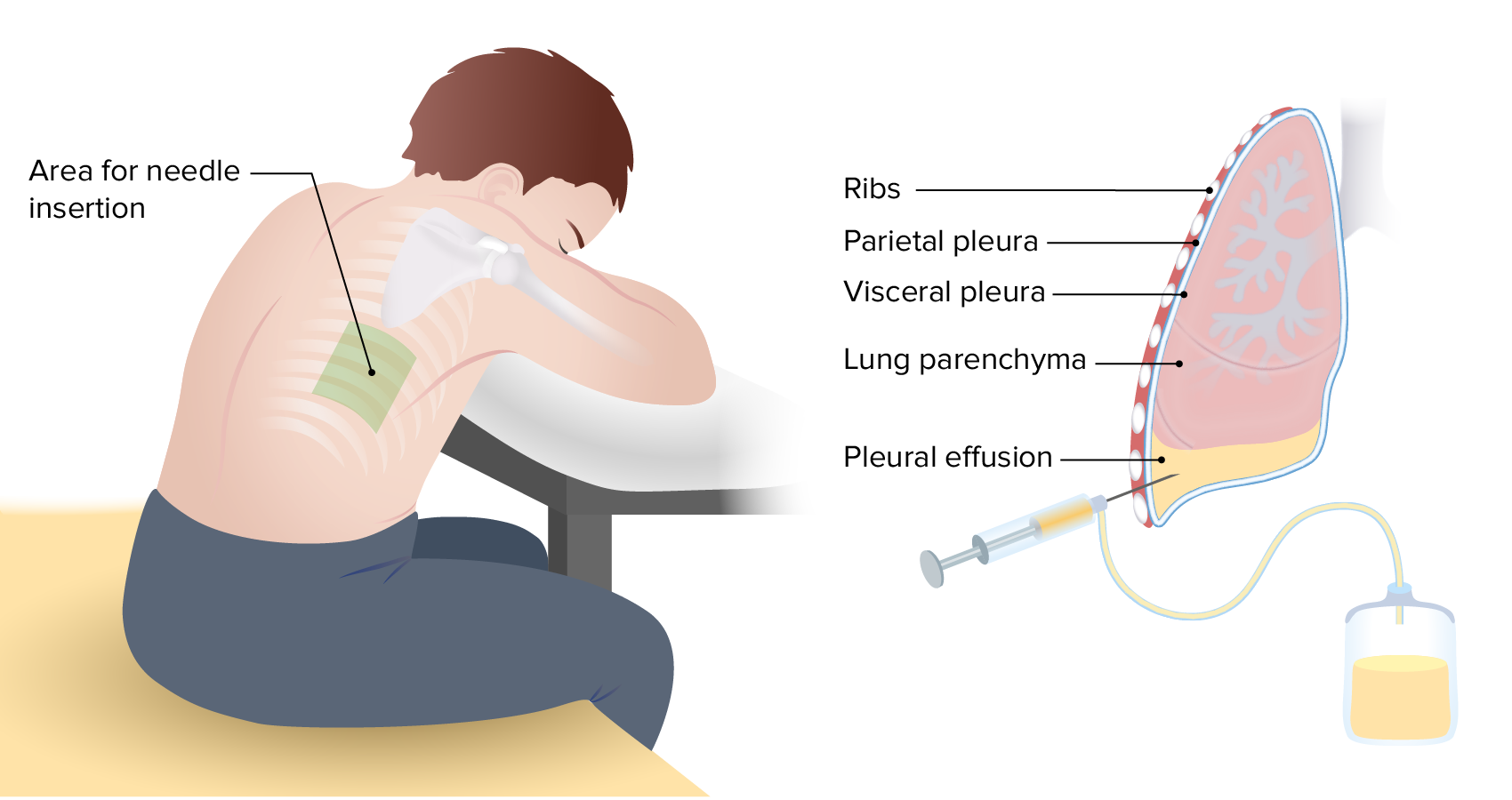
Image depicting the basic technique for thoracentesis, which allows for aspiration of a pleural effusion
Image by Lecturio.
Management of the underlying cause
The management of pleural effusions hinges on finding and treating the underlying etiology.
Parapneumonic effusion and empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia:
Antibiotics
ThoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery or chest tube drainage
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
May require frequent drainage or an advanced intervention (e.g., pleurodesis, pleural catheter)
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax:
Chest tube placementTube placementSurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Thoracic Surgery
Hepatic hydrothoraxHydrothoraxA collection of watery fluid in the pleural cavity.Edema:
Diuresis
Transjugular portosystemic shunt
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome with fluid overload: hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome
Complications
Complications of pleural effusions
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure:
Worsening hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage
Respiratory distress
Loculated pleural effusions:
Compartmentalization of a pleural effusion into smaller spaces by fibrousFibrousFibrocystic Change layers
Classically seen in empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia, hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax, and TBTBTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
Secondary to active pleural inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation, infection, or malignancyMalignancyHemothorax
ShockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock:
Obstructive shockObstructive ShockTypes of Shock: compressive mediastinal effect causing impairment of cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics
Septic shockSeptic shockSepsis associated with hypotension or hypoperfusion despite adequate fluid resuscitation. Perfusion abnormalities may include, but are not limited to lactic acidosis; oliguria; or acute alteration in mental status.Sepsis and Septic Shock: result of infection causing hemodynamic instability and end-organ dysfunction
Hemorrhagic shockHemorrhagic shockAcute hemorrhage or excessive fluid loss resulting in hypovolemia.Hemothorax: seen in traumatic hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Complications of thoracentesisThoracentesisAspiration of fluid or air from the thoracic cavity. It is coupled sometimes with the administration of drugs into the pleural cavity.Thoracic Surgery
PneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax
Vascular injury → hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Re-expansion pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema
References
Na M. (2014). Diagnostic tools of pleural effusion. Tuberculosis and Respiratory Diseases 76(5):199–210.
Jany B, Welte T. (2019). Pleural effusion in adults—etiology, diagnosis, and treatment. Deutsches Aerzteblatt Online 116(21):377–386.
Karkhanis V, Joshi J. (2012). Pleural effusion: diagnosis, treatment, and management. Open Access Emergency Medicine 4:31–52.