SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome is a life-threatening condition caused by large increases in serotonergic activity. This condition can be triggered by taking excessive doses of certain serotonergic medications or taking these medications in combination with other drugs that increase their activity. Hallmarks of this condition are autonomic hyperactivityHyperactivityAttention Deficit Hyperactivity Disorder, neuromuscular instability, and altered mental statusAltered Mental StatusSepsis in Children. Management involves discontinuation of all serotonergic agents, sedation with benzodiazepine, and cyproheptadine (a serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS antagonist) if supportive measures fail.
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome is a potentially life-threatening condition caused by large increases in serotonergic activity due to exposure to serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS agonists. Defining symptoms include altered mental statusAltered Mental StatusSepsis in Children, autonomic instabilityAutonomic instabilityRabies Virus, and neuromuscular abnormalities (tremors, myoclonusMyoclonusInvoluntary shock-like contractions, irregular in rhythm and amplitude, followed by relaxation, of a muscle or a group of muscles. This condition may be a feature of some central nervous system diseases; (e.g., epilepsy-myoclonic). Nocturnal myoclonus is the principal feature of the nocturnal myoclonus syndrome.Neurological Examination).
Epidemiology
Exact incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency is unknown due to:
Lack of confirmatory testing
Wide spectrum of severity
Cases appear to be increasing:
Increased awareness of disease by providers
Increased use of serotonergic medication
Etiology
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome occurs secondary to use of therapeutic medication, drug interactions, or overdose.
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS modulators (e.g., trazodoneTrazodoneA serotonin uptake inhibitor that is used as an antidepressant agent. It has been shown to be effective in patients with major depressive disorders and other subsets of depressive disorders. It is generally more useful in depressive disorders associated with insomnia and anxiety.Serotonin Reuptake Inhibitors and Similar Antidepressants)
Monoamine oxidaseOxidaseNeisseria inhibitors (e.g., tranylcypromineTranylcypromineA propylamine formed from the cyclization of the side chain of amphetamine. This monoamine oxidase inhibitor is effective in the treatment of major depression, dysthymic disorder, and atypical depression. It also is useful in panic and phobic disorders.Monoamine Oxidase Inhibitors, phenelzinePhenelzineOne of the monoamine oxidase inhibitors used to treat depression; phobic disorders; and panic.Monoamine Oxidase Inhibitors, isocarboxazidIsocarboxazidAn mao inhibitor that is effective in the treatment of major depression, dysthymic disorder, and atypical depression. It also is useful in the treatment of panic disorder and the phobic disorders.Monoamine Oxidase Inhibitors, selegilineSelegilineA selective, irreversible inhibitor of type B monoamine oxidase that is used for the treatment of newly diagnosed patients with parkinson disease, and for the treatment of depressive disorders.Monoamine Oxidase Inhibitors)
Tricyclic antidepressantsTricyclic antidepressantsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants (TCAsTCAsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants)
Buspirone
Nonpsychiatric drugs:
TramadolTramadolA narcotic analgesic proposed for severe pain. It may be habituating.Opioid Analgesics
LinezolidLinezolidAn oxazolidinone and acetamide derived anti-bacterial agent and protein synthesis inhibitor that is used in the treatment of gram-positive bacterial infections of the skin and respiratory tract.Oxazolidinones
Illicit drugsIllicit DrugsDrugs that are manufactured, obtained, or sold illegally. They include prescription drugs obtained or sold without prescription and non-prescription drugs. Illicit drugs are widely distributed, tend to be grossly impure and may cause unexpected toxicity.Delirium:
MDMAMDMAAn n-substituted amphetamine analog. It is a widely abused drug classified as a hallucinogen and causes marked, long-lasting changes in brain serotonergic systems. It is commonly referred to as mdma or ecstasy.Stimulants (3,4-MethylenedioxymethamphetamineMethamphetamineA central nervous system stimulant and sympathomimetic with actions and uses similar to dextroamphetamine. The smokable form is a drug of abuse and is referred to as crank, crystal, crystal meth, ice, and speed.Stimulants, ecstasyEcstasyAn n-substituted amphetamine analog. It is a widely abused drug classified as a hallucinogen and causes marked, long-lasting changes in brain serotonergic systems. It is commonly referred to as mdma or ecstasy.Stimulants, or molly)
LSD (lysergic acid diethylamide)
AmphetaminesAmphetaminesAnalogs or derivatives of amphetamine. Many are sympathomimetics and central nervous system stimulators causing excitation, vasopressin, bronchodilation, and to varying degrees, anorexia, analepsis, nasal decongestion, and some smooth muscle relaxation.Stimulants
CocaineCocaineAn alkaloid ester extracted from the leaves of plants including coca. It is a local anesthetic and vasoconstrictor and is clinically used for that purpose, particularly in the eye, ear, nose, and throat. It also has powerful central nervous system effects similar to the amphetamines and is a drug of abuse. Cocaine, like amphetamines, acts by multiple mechanisms on brain catecholaminergic neurons; the mechanism of its reinforcing effects is thought to involve inhibition of dopamine uptake.Local Anesthetics
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome occurs from any combination of drugs that have the net effect of increasing serotonergic neurotransmissionNeurotransmissionThe communication from a neuron to a target (neuron, muscle, or secretory cell) across a synapse. In chemical synaptic transmission, the presynaptic neuron releases a neurotransmitter that diffuses across the synaptic cleft and binds to specific synaptic receptors, activating them. The activated receptors modulate specific ion channels and/or second-messenger systems in the postsynaptic cell. In electrical synaptic transmission, electrical signals are communicated as an ionic current flow across electrical synapses.Synapses and Neurotransmission.
Stimulation of postsynaptic 5-HT1A and 5-HT2A receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS (5-HT5-HTA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS) receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors normally found in the CNS regulate:
AttentionAttentionFocusing on certain aspects of current experience to the exclusion of others. It is the act of heeding or taking notice or concentrating.Psychiatric Assessment
Behavior
ThermoregulationThermoregulationBody temperature can be divided into external temperature, which involves the skin, and core temperature, which involves the CNS and viscera. While external temperature can be variable, the core temperature is maintained within a narrow range of 36.5-37.5ºC (97.7-99.5ºF).Body Temperature Regulation
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS (5-HT5-HTA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS) receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors found in the peripheral nervous systemPeripheral nervous systemThe nervous system outside of the brain and spinal cord. The peripheral nervous system has autonomic and somatic divisions. The autonomic nervous system includes the enteric, parasympathetic, and sympathetic subdivisions. The somatic nervous system includes the cranial and spinal nerves and their ganglia and the peripheral sensory receptors.Nervous System: Anatomy, Structure, and Classification (PNS) regulate:
GI motilityGI MotilityThe primary functions of the GI tract are digestion and absorption, which require coordinated contractions of the smooth muscles present in the GI tract. Peristaltic waves, segmentation contractions, and the migrating motor complex are all important contraction patterns that help to mix contents, get them in contact with the intestinal walls, and propel material down the tract at appropriate times and in appropriate amounts.Gastrointestinal Motility
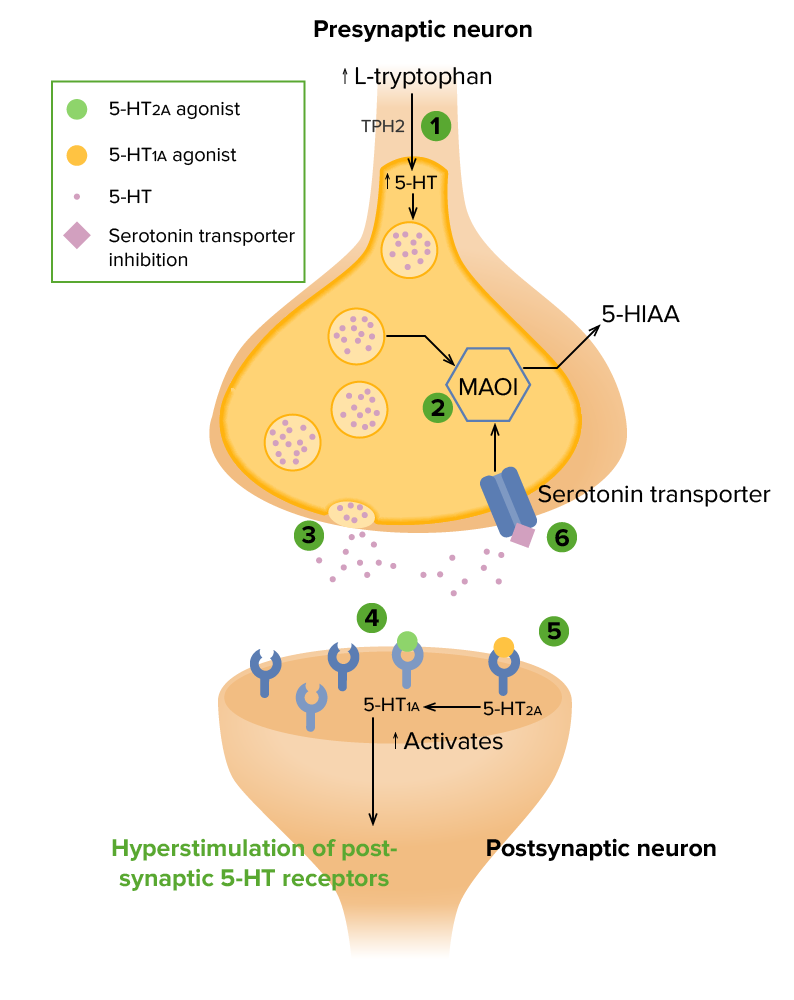
Several potential mechanisms for serotonin syndrome result in hyperstimulation of post-synaptic serotonin receptors (5-HT1A and 5-HT2A):
1. ↑ L-tryptophan → ↑ endogenous serotonin, or 5-hydroxytryptamine (5-HT), catalyzed by tryptophan hydroxylase 2 (TPH2)
2. Inhibition of serotonin metabolism by monoamine oxidase inhibitors (MAOIs) → ↑ presynaptic 5-HT
3. ↑ 5-HT release by drugs and medications (e.g., amphetamines, cocaine, MDMA, levodopa)
4. Activation of post-synaptic 5-HT1A receptors (direct or indirect)
5. Antagonism of post-synaptic 5-HT2A receptors (direct or indirect) (may enhance the effect of 5-HT1A agonists)
6. Inhibition of serotonin transporters (SERTs) by reuptake inhibitors (e.g., selective serotonin reuptake inhibitors, tricyclic antidepressants) → ↑ synaptic levels of 5-HT
5-HIAA: 5-hydroxyindoleacetic acid (a metabolite of serotonin)
MyoclonusMyoclonusInvoluntary shock-like contractions, irregular in rhythm and amplitude, followed by relaxation, of a muscle or a group of muscles. This condition may be a feature of some central nervous system diseases; (e.g., epilepsy-myoclonic). Nocturnal myoclonus is the principal feature of the nocturnal myoclonus syndrome.Neurological Examination
Mental status changes
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
MydriasisMydriasisDilation of pupils to greater than 6 mm combined with failure of the pupils to constrict when stimulated with light. This condition may occur due to injury of the pupillary fibers in the oculomotor nerve, in acute angle-closure glaucoma, and in adie syndrome.Glaucoma
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Unstable blood pressures (usually elevated)
Diaphoresis
Hyperthermia
Gastrointestinal stimulation
Increased bowel sounds
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Mnemonic
MADAM’S TIPS:
Mental status change
Agitation
Diarrhea
Ataxia
Myoclonus
Shivering
Tachycardia
Increased reflexes
Pyrexia
Sweating
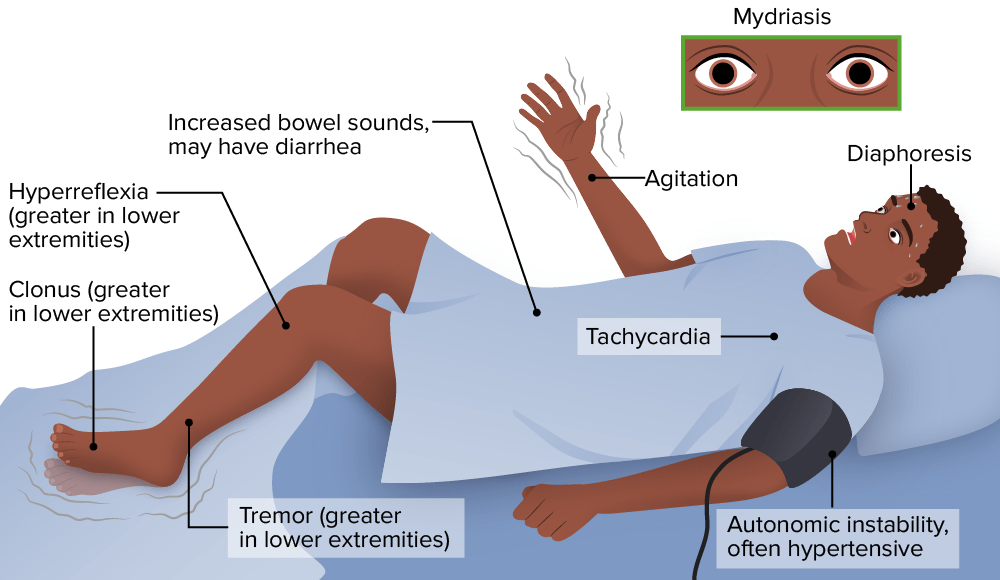
Symptoms of serotonin syndrome
Serotonin syndrome occurs from any combination of drugs that have the net effect of increasing serotonergic neurotransmission, causing altered mental status, autonomic instability, and neuromuscular abnormalities.
Image by Lecturio.
Diagnosis
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome is clinically diagnosed (serum serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS levels have no correlationCorrelationDetermination of whether or not two variables are correlated. This means to study whether an increase or decrease in one variable corresponds to an increase or decrease in the other variable.Causality, Validity, and Reliability to symptoms or toxicityToxicityDosage Calculation). Multiple diagnostic criteria have been developed, with the Hunter SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNSToxicityToxicityDosage Calculation Criteria being the most accurate.
Hunter SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNSToxicityToxicityDosage Calculation Criteria
Patient must have taken a serotonergic drug and be positive for 1 of the following criteria:
TremorTremorCyclical movement of a body part that can represent either a physiologic process or a manifestation of disease. Intention or action tremor, a common manifestation of cerebellar diseases, is aggravated by movement. In contrast, resting tremor is maximal when there is no attempt at voluntary movement, and occurs as a relatively frequent manifestation of parkinson disease.Myotonic Dystrophies + hyperreflexia
HypertoniaHypertoniaAbnormal increase in skeletal or smooth muscle tone. Skeletal muscle hypertonicity may be associated with pyramidal tract lesions or basal ganglia diseases.Neurological Examination + hyperthermia (> 38°C (> 100.4°F)) + ocular/inducible clonusClonusEhrlichiosis and Anaplasmosis
Management
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome often resolves within 24 hours of discontinuing the serotonergic agent and initiating care.
Management
Discontinuation of all serotonergic agents
Supportive care to normalize vital signs:
Control feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever:
Cooling blankets
Ice packs
Antipyretics are ineffective for serotonin-syndrome hyperthermia and are not recommended
IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids
Maintain appropriate blood pressure:
Consensus guidelines do not exist for BP management in this setting.
BenzodiazepinesBenzodiazepinesBenzodiazepines work on the gamma-aminobutyric acid type A (GABAA) receptor to produce inhibitory effects on the CNS. Benzodiazepines do not mimic GABA, the main inhibitory neurotransmitter in humans, but instead potentiate GABA activity. Benzodiazepines may be used to simultaneously lower elevated pressure and control agitationAgitationA feeling of restlessness associated with increased motor activity. This may occur as a manifestation of nervous system drug toxicity or other conditions.St. Louis Encephalitis Virus.
AntidoteAntidoteAn antidote is a substance that counteracts poisoning or toxicity. Substances that can cause poisoning include heavy metals (from occupation, treatments, or diet), alcohols, environmental toxins, and medications. Antidotes of Common Poisonings therapy: cyproheptadine (5-HT2 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonist)
Potential complications
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis and myoglobinuriaMyoglobinuriaThe presence of myoglobin in urine usually as a result of rhabdomyolysis.Rhabdomyolysis
Disseminated intravascular coagulationDisseminated intravascular coagulationDisseminated intravascular coagulation (DIC) is a condition characterized by systemic bodywide activation of the coagulation cascade. This cascade results in both widespread microvascular thrombi contributing to multiple organ dysfunction and consumption of clotting factors and platelets, leading to hemorrhage. Disseminated Intravascular Coagulation (DICDICDisseminated intravascular coagulation (DIC) is a condition characterized by systemic bodywide activation of the coagulation cascade. This cascade results in both widespread microvascular thrombi contributing to multiple organ dysfunction and consumption of clotting factors and platelets, leading to hemorrhage. Disseminated Intravascular Coagulation)
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Acute renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
ARDS
Differential Diagnosis
It is important to distinguish between serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome, malignant hyperthermiaMalignant hyperthermiaAn important complication of anesthesia is malignant hyperthermia, an autosomal dominant disorder of the regulation of calcium transport in the skeletal muscles resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high fever, muscle rigidity, rhabdomyolysis, and respiratory and metabolic acidosis. Malignant Hyperthermia, and neuroleptic malignant syndromeNeuroleptic malignant syndromeNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction. Neuroleptic Malignant Syndrome.
Neuroleptic malignant syndromeNeuroleptic malignant syndromeNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction. Neuroleptic Malignant Syndrome (NMSNMSNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction.Neuroleptic Malignant Syndrome): rare, idiosyncratic, and potentially life-threatening reaction to neuroleptic (e.g., antipsychoticAntipsychoticAntipsychotics, also called neuroleptics, are used to treat psychotic disorders and alleviate agitation, mania, and aggression. Antipsychotics are notable for their use in treating schizophrenia and bipolar disorder and are divided into 1st-generation antipsychotics (FGAs) and atypical or 2nd-generation antipsychotics. First-Generation Antipsychotics) drugs. Very similar to serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome, but without the GI symptoms and more muscle rigidityMuscle rigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Motor Neuron Lesions. Treated similarly to serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome, by discontinuing causative drugs and offering supportive care.
Malignant hyperthermiaMalignant hyperthermiaAn important complication of anesthesia is malignant hyperthermia, an autosomal dominant disorder of the regulation of calcium transport in the skeletal muscles resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high fever, muscle rigidity, rhabdomyolysis, and respiratory and metabolic acidosis. Malignant Hyperthermia: rare complication triggered by certain inhaled anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts or paralytics. Suspect in operating room or anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts procedure. Treatment is nearly the same as NMSNMSNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction.Neuroleptic Malignant Syndrome and clinically indistinguishable except for drugs triggering the syndrome.
Simon LV, Torrico TJ, Keenaghan M. Serotonin Syndrome. [Updated 2024 Mar 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482377/
Create your free account or log in to continue reading!