An important complication of anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts is malignant hyperthermia, an autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance disorder of the regulation of calcium transportCalcium transportCalcium Hemostasis and Bone Metabolism in the skeletal musclesSkeletal musclesA subtype of striated muscle, attached by tendons to the skeleton. Skeletal muscles are innervated and their movement can be consciously controlled. They are also called voluntary muscles.Muscle Tissue: Histology resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, muscle rigidityMuscle rigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Motor Neuron Lesions, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, and respiratory and metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis. The mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate reaches 90% if not quickly identified and treated. Management involves stopping the offending agent and administering dantroleneDantroleneSkeletal muscle relaxant that acts by interfering with excitation-contraction coupling in the muscle fiber. It is used in spasticity and other neuromuscular abnormalities. Although the mechanism of action is probably not central, dantrolene is usually grouped with the central muscle relaxants.Spasmolytics.
Malignant hyperthermia (MH) is a hypermetabolic response in a patient exposed to a volatile anesthetic or succinylcholineSuccinylcholineA quaternary skeletal muscle relaxant usually used in the form of its bromide, chloride, or iodide. It is a depolarizing relaxant, acting in about 30 seconds and with a duration of effect averaging three to five minutes. Succinylcholine is used in surgical, anesthetic, and other procedures in which a brief period of muscle relaxation is called for.Cholinomimetic Drugs resulting in feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, muscle rigidityMuscle rigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Motor Neuron Lesions, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, and pulmonary and cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP).
Seen in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship of all ethnicities and geographic distributions
Twice as common in males
Up to 50% of cases occur in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship < 19 years of age.
Etiology
Triggering substances:
Inhalation anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts (e.g., halothaneHalothaneA nonflammable, halogenated, hydrocarbon anesthetic that provides relatively rapid induction with little or no excitement. Analgesia may not be adequate. Nitrous oxide is often given concomitantly. Because halothane may not produce sufficient muscle relaxation, supplemental neuromuscular blocking agents may be required.Inhaled Anesthetics, enflurane, and isofluraneIsofluraneA stable, non-explosive inhalation anesthetic, relatively free from significant side effects.Inhaled Anesthetics)
SuccinylcholineSuccinylcholineA quaternary skeletal muscle relaxant usually used in the form of its bromide, chloride, or iodide. It is a depolarizing relaxant, acting in about 30 seconds and with a duration of effect averaging three to five minutes. Succinylcholine is used in surgical, anesthetic, and other procedures in which a brief period of muscle relaxation is called for.Cholinomimetic Drugs (muscle relaxant)
“Safe” anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with previously diagnosed malignant hyperthermia:
“Laughing gas” (nitrous oxideNitrous oxideNitrogen oxide (N2O). A colorless, odorless gas that is used as an anesthetic and analgesic. High concentrations cause a narcotic effect and may replace oxygen, causing death by asphyxia.Inhaled Anesthetics)
BarbituratesBarbituratesA class of chemicals derived from barbituric acid or thiobarbituric acid. Many of these are gaba modulators used as hypnotics and sedatives, as anesthetics, or as anticonvulsants.Intravenous Anesthetics
BenzodiazepinesBenzodiazepinesBenzodiazepines work on the gamma-aminobutyric acid type A (GABAA) receptor to produce inhibitory effects on the CNS. Benzodiazepines do not mimic GABA, the main inhibitory neurotransmitter in humans, but instead potentiate GABA activity. Benzodiazepines
EtomidateEtomidateImidazole derivative anesthetic and hypnotic with little effect on blood gases, ventilation, or the cardiovascular system. It has been proposed as an induction anesthetic.Intravenous Anesthetics
PropofolPropofolAn intravenous anesthetic agent which has the advantage of a very rapid onset after infusion or bolus injection plus a very short recovery period of a couple of minutes. Propofol has been used as anticonvulsants and antiemetics.Intravenous Anesthetics
KetamineKetamineA cyclohexanone derivative used for induction of anesthesia. Its mechanism of action is not well understood, but ketamine can block NMDA receptors (n-methyl-d-aspartate receptors) and may interact with sigma receptors.Intravenous Anesthetics
OpioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics
Non-depolarizing muscle relaxants
Pathophysiology
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance genetic disorder of hypermetabolism of skeletal muscle after exposure to certain anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts
Due to mutations encoding for:
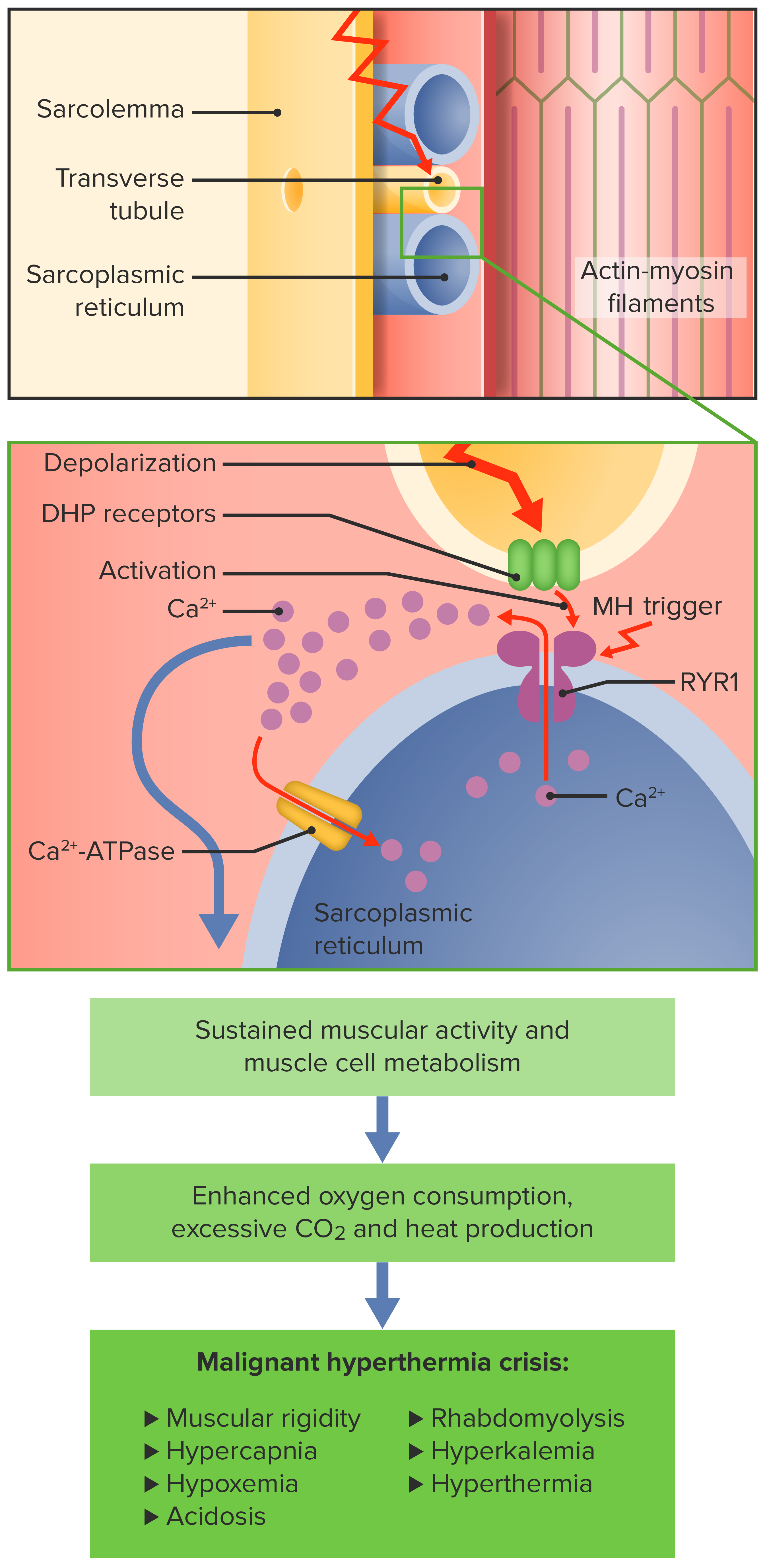
DihydropyridineDihydropyridinePyridine moieties which are partially saturated by the addition of two hydrogen atoms in any position.Class 4 Antiarrhythmic Drugs (Calcium Channel Blockers) (DHP) receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors → sense action potentialAction PotentialAbrupt changes in the membrane potential that sweep along the cell membrane of excitable cells in response to excitation stimuli.Membrane Potential in T tubules
Ryanodine (RYR1) receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors → release calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes from sarcoplasmic reticulumSarcoplasmic ReticulumA network of tubules and sacs in the cytoplasm of skeletal muscle fibers that assist with muscle contraction and relaxation by releasing and storing calcium ions.Muscle Tissue: Histology into intracellular space
Defects lead to continuous muscle contraction, causing:
↑ Cellular metabolismCellular metabolismThe chemical reactions in living organisms by which energy is provided for vital processes and activities and new material is assimilated.Thyroid Hormones (hypermetabolism)
Cell destruction causing CK release and myoglobinuriaMyoglobinuriaThe presence of myoglobin in urine usually as a result of rhabdomyolysis.Rhabdomyolysis
Pathophysiology of malignant hyperthermia (MH)
DHP: dihydropyridine
RYR1: ryanodine
Symptoms may appear at any point during anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts (induction, maintenance, rarely after discontinuation). Symptoms follow a regularRegularInsulin pattern; the speed of progression through symptoms varies, however.
Early signs:
Rapid rise in end-tidal carbon dioxide (ETCO₂): earliest symptom
Arrhythmias:
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Peaked T waves
Due to hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Often misinterpreted as too low a depth of anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts
Muscular rigor (masseterMasseterA masticatory muscle whose action is closing the jaws.Jaw and Temporomandibular Joint: AnatomyspasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy specific for succinylcholine-induced MH): blood pressure is initially ↑ (decreased blood pressure is sign of circulatory failure)
Late signs:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever (not required for diagnosis)
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis
MyoglobinuriaMyoglobinuriaThe presence of myoglobin in urine usually as a result of rhabdomyolysis.Rhabdomyolysis
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema
Laboratory findings
Metabolic/respiratory acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis:
Respiratory acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis: caused by ↑ CO₂ production
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis: due to lactic acid production
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia: due to potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia released from damaged cells
↑ CK: released by muscle breakdown
MyoglobinuriaMyoglobinuriaThe presence of myoglobin in urine usually as a result of rhabdomyolysis.Rhabdomyolysis:
Skeletal muscle cell breakdown releases myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis.
MyoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis spills into urine.
Management
Care in the ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus is necessary as the condition can reactivate after apparent improvement.
Immediate actions
Termination of triggering substances
HyperventilationHyperventilationA pulmonary ventilation rate faster than is metabolically necessary for the exchange of gases. It is the result of an increased frequency of breathing, an increased tidal volume, or a combination of both. It causes an excess intake of oxygen and the blowing off of carbon dioxide.Respiratory Alkalosis with 100% oxygen100% OxygenCluster Headaches
Terminating surgery as soon as possible
If necessary, change to safer anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts (IV agents).
DantroleneDantroleneSkeletal muscle relaxant that acts by interfering with excitation-contraction coupling in the muscle fiber. It is used in spasticity and other neuromuscular abnormalities. Although the mechanism of action is probably not central, dantrolene is usually grouped with the central muscle relaxants.Spasmolytics
Inhibits ryanodine receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors
Prevents release of CaCACondylomata acuminata are a clinical manifestation of genital HPV infection. Condylomata acuminata are described as raised, pearly, flesh-colored, papular, cauliflower-like lesions seen in the anogenital region that may cause itching, pain, or bleeding.Condylomata Acuminata (Genital Warts)2+ from sarcoplasmic reticulumSarcoplasmic ReticulumA network of tubules and sacs in the cytoplasm of skeletal muscle fibers that assist with muscle contraction and relaxation by releasing and storing calcium ions.Muscle Tissue: Histology of skeletal muscle
Cooled IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids
Flushing bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess with cold fluid
Balance acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis with sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes.
Treat electrolyte abnormalities.
Treat hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with arrhythmias.
Potential complications
Severe metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema
Clinical Relevance
Related conditions
SerotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome: feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, autonomic dysfunctionAutonomic DysfunctionAnterior Cord Syndrome, rigidityRigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Megacolon/spasticitySpasticitySpinal Disk Herniation related to overdoses of selective serotonin reuptake inhibitorsSelective Serotonin Reuptake InhibitorsSerotonin Reuptake Inhibitors and Similar Antidepressants (SSRIsSSRIsSerotonin Reuptake Inhibitors and Similar Antidepressants) or other antidepressantsOther antidepressantsAntidepressants encompass several classes of medications and are used to treat individuals with depression, anxiety, and other psychiatric conditions, as well as to manage chronic pain and menopausal symptoms.Other Antidepressants. Presents with more GI symptoms (nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia) than in MH.
Neuroleptic malignant syndromeNeuroleptic malignant syndromeNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction. Neuroleptic Malignant Syndrome (NMSNMSNeuroleptic malignant syndrome (NMS) is a rare, idiosyncratic, and potentially life-threatening reaction to antipsychotic drugs. Neuroleptic malignant syndrome presents with ≥ 2 of the following cardinal symptoms: fever, altered mental status, muscle rigidity, and autonomic dysfunction.Neuroleptic Malignant Syndrome): rare, idiosyncratic, and potentially life-threatening reaction to neuroleptic (e.g., antipsychoticAntipsychoticAntipsychotics, also called neuroleptics, are used to treat psychotic disorders and alleviate agitation, mania, and aggression. Antipsychotics are notable for their use in treating schizophrenia and bipolar disorder and are divided into 1st-generation antipsychotics (FGAs) and atypical or 2nd-generation antipsychotics. First-Generation Antipsychotics) drug. Very similar to serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome, but without the GI symptoms and more muscle rigidityMuscle rigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Motor Neuron Lesions. Treated similarly to serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS syndrome, by discontinuing causative drugs and offering supportive care.
Differential diagnosis
Presentations with altered mental statusAltered Mental StatusSepsis in Children, autonomic dysfunctionAutonomic DysfunctionAnterior Cord Syndrome, and feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever:
MeningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis/encephalitisEncephalitisEncephalitis is inflammation of the brain parenchyma caused by an infection, usually viral. Encephalitis may present with mild symptoms such as headache, fever, fatigue, and muscle and joint pain or with severe symptoms such as seizures, altered consciousness, and paralysis.Encephalitis
Excited deliriumDeliriumDelirium is a medical condition characterized by acute disturbances in attention and awareness. Symptoms may fluctuate during the course of a day and involve memory deficits and disorientation. Delirium
HeatstrokeHeatstrokeHeatstroke is an illness characterized as a core body temperature exceeding 40°C (104°F) with accompanying neurological symptoms including ataxia, seizures, and/or delirium. Heatstroke is usually due to the body’s inability to regulate its temperature when challenged with an elevated heat load. Heatstroke
Status epilepticusStatus EpilepticusA prolonged seizure or seizures repeated frequently enough to prevent recovery between episodes occurring over a period of 20-30 minutes. The most common subtype is generalized tonic-clonic status epilepticus, a potentially fatal condition associated with neuronal injury and respiratory and metabolic dysfunction. Nonconvulsive forms include petit mal status and complex partial status, which may manifest as behavioral disturbances. Simple partial status epilepticus consists of persistent motor, sensory, or autonomic seizures that do not impair cognition. Subclinical status epilepticus generally refers to seizures occurring in an unresponsive or comatose individual in the absence of overt signs of seizure activity.Seizures
ThyrotoxicosisThyrotoxicosisA hypermetabolic syndrome caused by excess thyroid hormones which may come from endogenous or exogenous sources. The endogenous source of hormone may be thyroid hyperplasia; thyroid neoplasms; or hormone-producing extrathyroidal tissue. Thyrotoxicosis is characterized by nervousness; tachycardia; fatigue; weight loss; heat intolerance; and excessive sweating.Thyrotoxicosis and Hyperthyroidism
Rosenberg, H., Pollock, N., Schiemann, A., Bulger, T., & Stowell, K. (2015). Malignant hyperthermia: A review. Orphanet Journal of Rare Diseases, 10(1), Article 93. https://doi.org/10.1186/s13023-015-0310-1
Larach, M. G., Gronert, G. A., Allen, G. C., Brandom, B. W., & Lehman, E. B. (2010). Clinical presentation, treatment, and complications of malignant hyperthermia in North America from 1987 to 2006. Anesthesia & Analgesia, 110(2), 498–507. https://doi.org/10.1213/ANE.0b013e3181c6b9b2
Malignant Hyperthermia Association of the United States. (n.d.). Malignant Hyperthermia Association of the United States. Retrieved April 12, 2025, from https://www.mhaus.org/
Create your free account or log in to continue reading!