Pelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP. The major risk factors include parity, vaginal delivery, age, obesity, and conditions characterized by increased abdominal pressure. Affected individuals typically present with vaginal pressure and the sensation of a vaginal bulge, often with associated urinary and defecatory urges. Diagnosis is clinical, and POP is classified using either the Pelvic Organ Prolapse Quantitation (POP-Q) staging system or the Baden-Walker grading system. Management is based on the subject's desires and symptoms. Conservative approaches include vaginal pessaries, pelvic muscle strengthening exercises, and reducing modifiable risk factors. Surgical repair is an option for individuals with more severe symptoms.
Pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse (POP): a general term referring to prolapse of 1 or more of the pelvic organs (e.g., bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy, rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy) into the vaginal canal
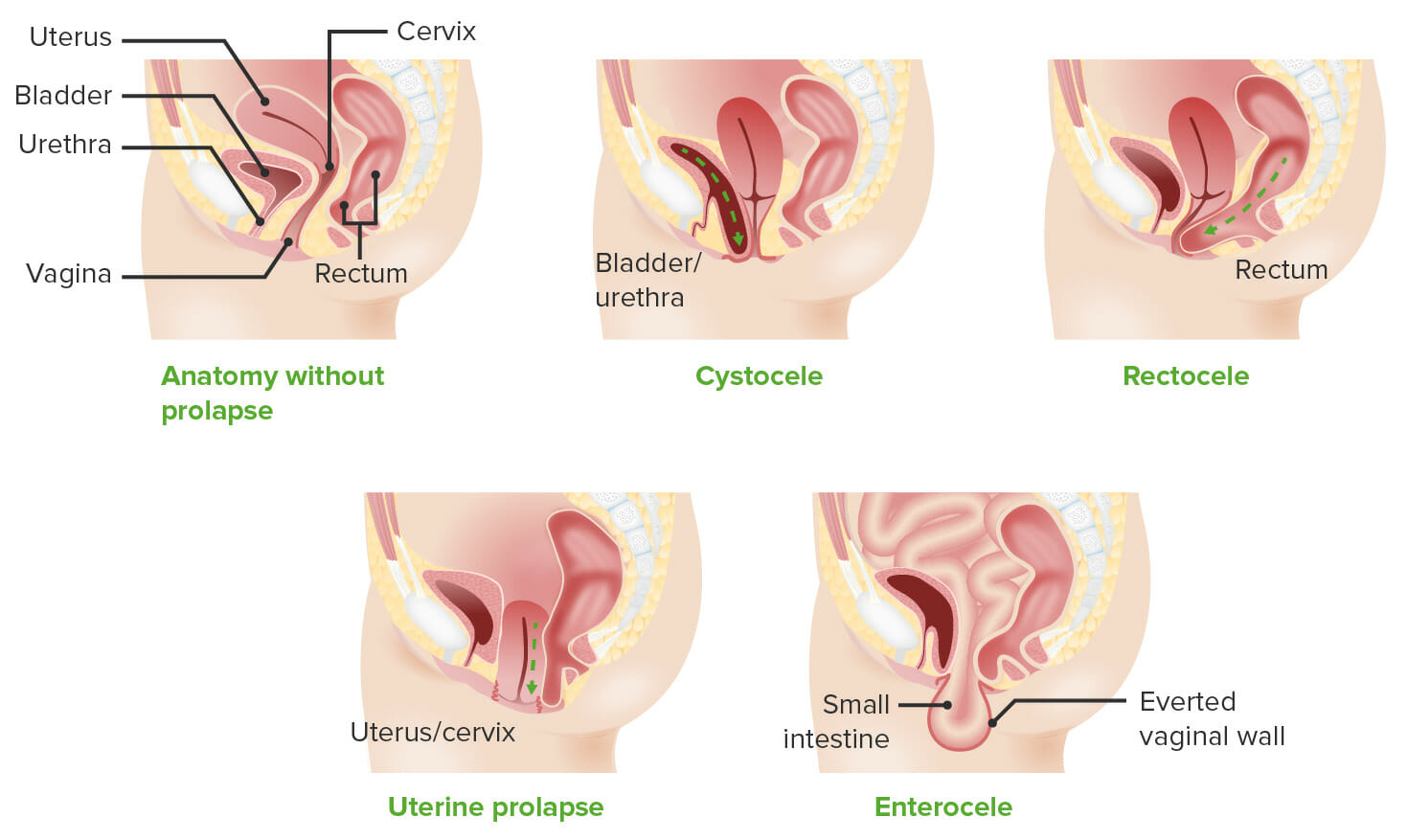
Organs prolapse through the vaginal canal/orifice, pushing the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy with it → POP is defined by the vaginal wall that is prolapsing and the organs behind that wall
Anterior compartment prolapseAnterior compartment prolapseA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse:
Classically referred to as a cystoceleCystoceleA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse
HerniationHerniationOmphalocele of the posterior vaginal wall and rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
The uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy and cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy (normal anatomy)
The cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy (if the subject has had a supracervical hysterectomy)
Vaginal cuff (if the subject has had a total hysterectomy)
If the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy is present, the prolapse is referred to as uterine prolapseUterine prolapseDownward displacement of the uterus. It is classified in various degrees: in the first degree the uterine cervix is within the vaginal orifice; in the second degree the cervix is outside the orifice; in the third degree the entire uterus is outside the orifice.Pelvic Organ Prolapse.
If the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy is absent, the intestine typically prolapses behind the vaginal cuff, classically known as an enteroceleEnterocelePelvic Organ Prolapse.
Types of pelvic organ prolapse: Vaginal wall is outlined in a darker pink. Note how with cystoceles and rectoceles, the bladder and rectum, respectively, are pushing on the vaginal walls and herniating through the vaginal orifice. With apical prolapse, the vagina gets “scrunched up,” as shown in the uterine prolapse image, and may even completely evert itself, as shown with the enterocele.
Image by Lecturio.
A 40-year-old woman with uterine prolapse: Note the smooth tissue of the cervix protruding through the vaginal introitus (the external cervical os is not well visualized in this image) compared with the rugal folds of the anterior vaginal wall.
Image: “A 40 year old woman with uterine prolapse” by Mikael Häggström. License: Public Domain
Visualizing POP
Visualizing POP, especially apical POP, can be difficult.
Envision holding a sock up by the toe:
Your handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy is the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy.
The sock is the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy.
The open part of the sock is secured to a fixed location:
The open part of the sock is the vaginal introitus.
The “fixed location” is the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy.
Begin moving your handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy down → the lower position of your handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy represents apical/uterine prolapseUterine prolapseDownward displacement of the uterus. It is classified in various degrees: in the first degree the uterine cervix is within the vaginal orifice; in the second degree the cervix is outside the orifice; in the third degree the entire uterus is outside the orifice.Pelvic Organ Prolapse
As you keep moving your handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy down through the sock opening, the sock begins turning inside out and is similar to how prolapsed organs can end up completely “outside” the body, yet still remain covered by vaginal mucosa.
Etiology[1,4]
Prolapse is due to weakness and insufficiency of the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy, which normally keeps organs in place. Risk factors include:
Multiple parityParityThe number of offspring a female has borne. It is contrasted with gravidity, which refers to the number of pregnancies, regardless of outcome.Pregnancy: Diagnosis, Physiology, and Care (risk increases with each additional birth)
Vaginal delivery
Advancing age
Menopausal status
Increased intraabdominal pressure:
Chronic cough
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology abnormalities (e.g., Ehlers-Danlos syndromeEhlers-Danlos syndromeEhlers-Danlos syndrome (EDS) is a heterogeneous group of inherited connective tissue disorders that are characterized by hyperextensible skin, hypermobile joints, and fragility of the skin and connective tissue. Ehlers-Danlos Syndrome)
The exact prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of uterine and vaginal prolapse is uncertain.
Peak incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: women aged 70–79 years
Lifetime risk of women in the US undergoing surgery for POP: 13%
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of POP based on reported symptoms: 3%–6%
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of POP identified on exam: 40%–50%
Take-home message: Many women with mild POP are asymptomatic and do not require management beyond reducing modifiable risk factors to prevent symptoms from developing (e.g., weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation).
Surgical Anatomy and Pathology
Pelvic organs are supported by the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy, connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology, and the bony pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy. Additionally, the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy is supported by 3 levels of support along its length.
Pelvic diaphragmPelvic diaphragmSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy
The most internal layer of the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy:
Functions:
Provides structure to the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy, separating the internal pelvic cavity from the external perineumPerineumThe body region lying between the genital area and the anus on the surface of the trunk, and to the shallow compartment lying deep to this area that is inferior to the pelvic diaphragm. The surface area is between the vulva and the anus in the female, and between the scrotum and the anus in the male.Vagina, Vulva, and Pelvic Floor: Anatomy
Resists intra-abdominal pressure
Structure:
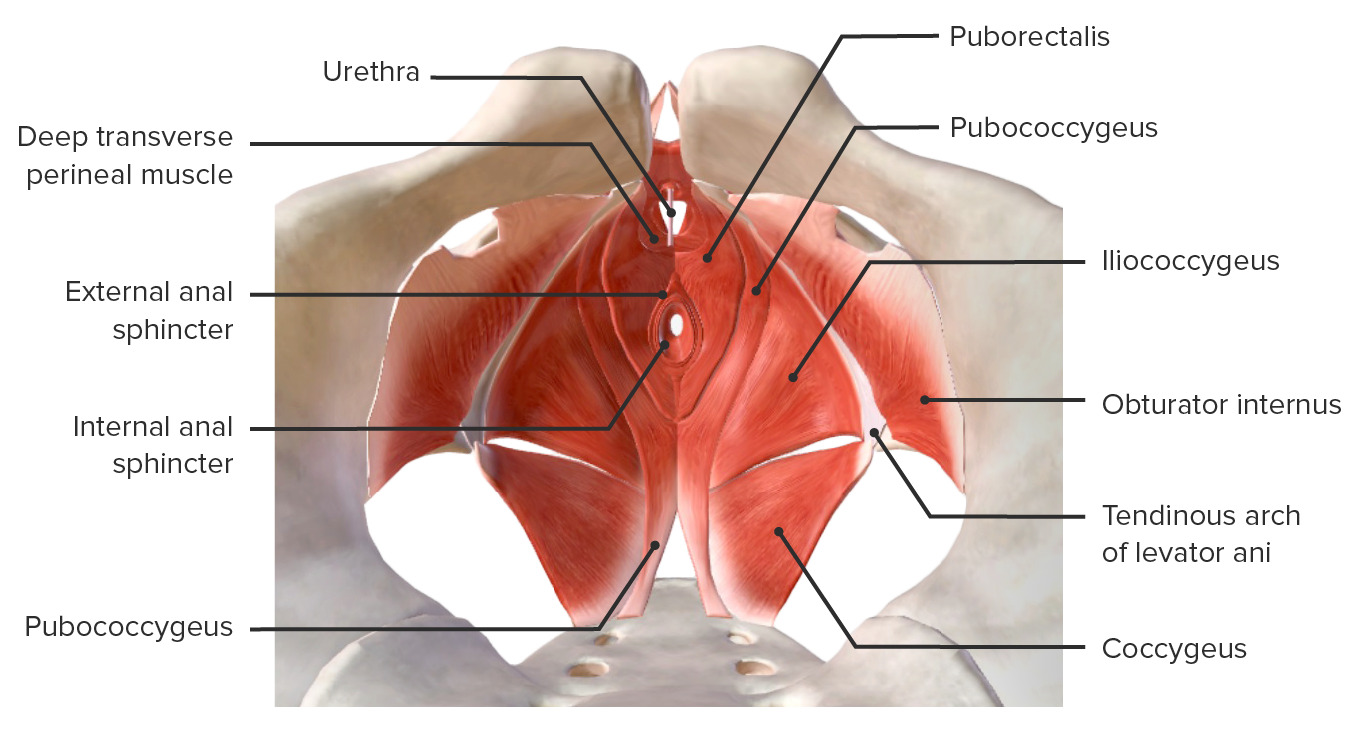
Muscles begin at the tendinous arch (below and parallel to the inferior margin of the pubic bones).
Muscles extend posteriorly toward the coccyxCoccyxThe last bone in the vertebral column in tailless primates considered to be a vestigial tail-bone consisting of three to five fused vertebrae.Vertebral Column: Anatomy → “wrap around” the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, and rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy, providing lateral support
Perineal body: the central tendonCentral tendonDiaphragm: Anatomy and site of attachment for the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscles
Muscles of the pelvic diaphragmPelvic diaphragmSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy:
PuborectalisPuborectalisVagina, Vulva, and Pelvic Floor: Anatomy: the innermost muscle, originating from the tendinous arch just below the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and forming a sling around the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy; in direct contact with the lateral vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy and the lateral and posterior rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Other muscles of the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy:
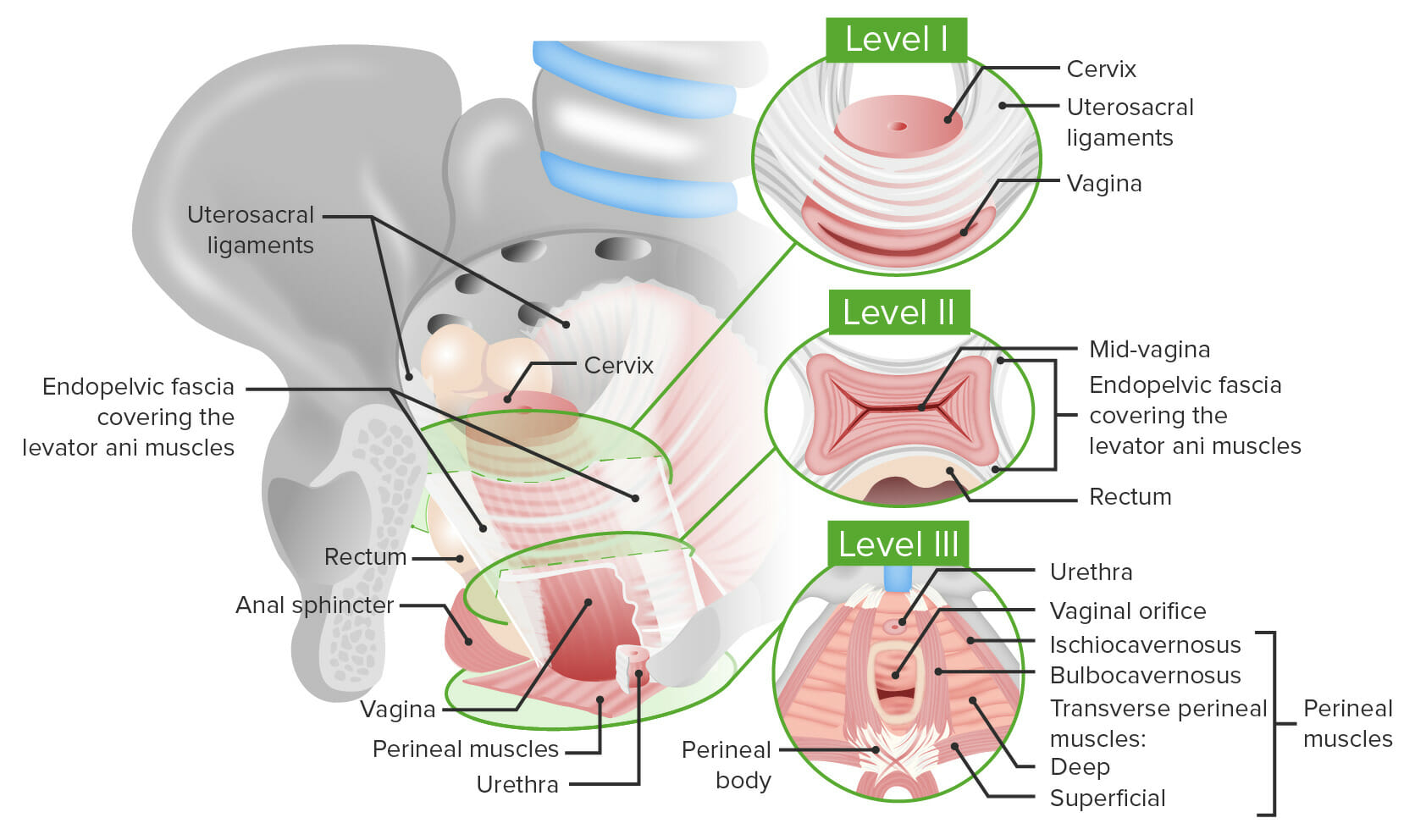
Consists of the uterosacral ligamentsUterosacral ligamentsVagina, Vulva, and Pelvic Floor: Anatomy that suspend the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy and upper vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy to the sacrumSacrumFive fused vertebrae forming a triangle-shaped structure at the back of the pelvis. It articulates superiorly with the lumbar vertebrae, inferiorly with the coccyx, and anteriorly with the ilium of the pelvis. The sacrum strengthens and stabilizes the pelvis.Vertebral Column: Anatomy, and the lateral pelvic wall
Level II support:
Lateral connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology attachments along the length of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Paravaginal attachments to the endopelvic fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis of the levator ani musclesLevator ani musclesVagina, Vulva, and Pelvic Floor: Anatomy surrounding the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Level III support:
The most distal level of support
Consists of the perineumPerineumThe body region lying between the genital area and the anus on the surface of the trunk, and to the shallow compartment lying deep to this area that is inferior to the pelvic diaphragm. The surface area is between the vulva and the anus in the female, and between the scrotum and the anus in the male.Vagina, Vulva, and Pelvic Floor: Anatomy and perineal muscles
Supports the distal 3rd of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Pathology:
Loss of level I support → apical prolapse into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Loss of level II support → most commonly results in anterior vaginal wall and bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess prolapse (cystoceleCystoceleA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse)
Loss of level III support →
Anteriorly: urethral hypermobility and incontinence
Posteriorly: posterior vaginal wall and rectal prolapseRectal prolapseRectal prolapse, also known as rectal procidentia, is the protrusion of rectal tissue through the anus. The tissue may include just the mucosa or the full thickness of the rectal wall. Common risk factors include chronic straining, constipation, bowel motility disorders, and weakening of the pelvic floor muscles. Rectal Prolapse
Levels of vaginal support: Level I: the most proximal level supporting the upper vagina. Consists of uterosacral ligaments connecting the upper vagina at the level of the cervix to the sacrum Level II: support along the length of the vagina provided by the endopelvic fascia covering the levator ani muscles. The fascia inserts in the tendinous arch of the levator ani muscles just below the pubic bones. Level III: the most distal level of support. Level III supports the lower vagina and the vaginal orifice and is provided by the perineal muscles and the perineal body.
Individuals with POP typically present with:[4,7,8]
Vaginal symptoms:
Sensations of:
Vaginal fullness
Pressure
Bulge
“Something falling down”
Symptoms typically worsen with activity, Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse, and/or at the end of the day.
Urinary symptoms:
Incomplete emptying of urine
Difficulty in voiding urine
Urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence
Rectal symptoms:
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Incomplete emptying
Splinting: placing fingers in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy and pushing down in order to evacuate stool
Fecal urgency
Rectal fullness
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways symptoms:
DyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency
Lower back and pelvic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways that is exacerbated on activity
Vaginal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways if the prolapse is severe and erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes or ulcerations are present
Bimanual pelvic examination: helpful in assessing apical prolapse
Rectovaginal examination
Assess pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomymuscle toneMuscle toneThe state of activity or tension of a muscle beyond that related to its physical properties, that is, its active resistance to stretch. In skeletal muscle, tonus is dependent upon efferent innervation.Skeletal Muscle Contraction (with 1 or 2 fingers in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, have the patient squeeze).[1]
Examine the patient at rest and during the Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse.
Take note of:
Which portions of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy are prolapsing (e.g., anterior wall, posterior wall, apex)
How far the prolapse descends (use the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy as a reference point)
Rectal tone
Urethral mobility
If significant prolapse is not appreciated lying down, examine the patient while they are standing up.[1]
Findings are reported using either:
Pelvic Organ ProlapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse Quantitation (POP-Q) stagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis system
A majority of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with relatively mild POP are asymptomatic (POP discovered incidentally on exam). Because management is primarily aimed at relieving symptoms, it is important to ask about the presence of any of the following:[1]
Symptoms bothersome enough to want treatment
Limited activity due to POP
Sexual dysfunctionSexual dysfunctionPhysiological disturbances in normal sexual performance in either the male or the female.Sexual Physiology (e.g., dyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency due to POP)
Urinary dysfunction (e.g., is voiding more difficult later in the day, when POP is more pronounced)
Defecatory dysfunction (e.g., Does the patient need to splint to defecate?)
Assess the patient if they are experiencing stress urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence (SUI):
Ask the patient to cough while observing the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy for leaks.
Should be assessed when the prolapse has reduced (sometimes, especially anterior prolapse may actually improve SUI)
Consider urodynamics studies, especially if planning surgery, to see if a concurrent incontinence procedure may be indicated.
The American Urogynecologic Society (AUGS) and the Society of Gynecologic Surgeons (SGS) recommend using the POP-Q staging systemPOP-Q staging systemPelvic Organ Prolapse over the Baden-Walker systemBaden-Walker SystemPelvic Organ Prolapse because the former is the only validated method for the objective measurement of a prolapse.
The POP-Q system is best for:
Tracking progression of prolapse over time
Assessing response to treatment
Standardizing researchResearchCritical and exhaustive investigation or experimentation, having for its aim the discovery of new facts and their correct interpretation, the revision of accepted conclusions, theories, or laws in the light of newly discovered facts, or the practical application of such new or revised conclusions, theories, or laws.Conflict of Interest
The POP-Q system is used to stage prolapse based on 9 measurements:
6 of the measurements compare defined/fixed points in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy to the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy during Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse:
Points proximal to the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy (toward the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy) are given negative values.
Points distal to the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy (toward the introitus) are given positive values.
3 additional measurements are used to provide a more comprehensive picture.
Table: Classification based on stages
Stage 0
No prolapse
Stage I
The most distal portion of the prolapse is > 1 cm proximal to the level of the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy.
Stage II
The most distal portion of the prolapse is within 1 cm or less of the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy.
Stage III
The most distal portion of the prolapse is > 1 cm distal to the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy, but no further than 2 cm less than the TVL.
Stage IV
The vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy is completely everted (within 2 cm of +TVL) or uterine procidentiaProcidentiaPelvic Organ Prolapse has occurred.
TVL: total vaginal length
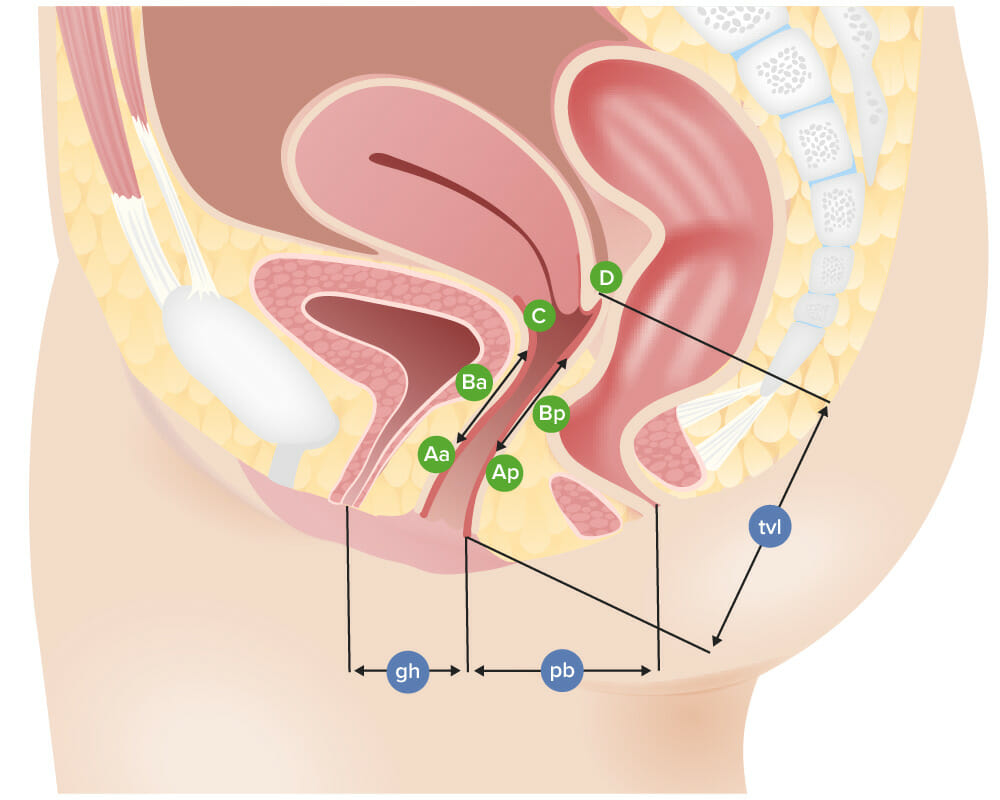
Points and landmarks used in the POP-Q system:
The stage is defined by the largest number associated with each compartment. For example, if Aa = 0 and Ba = +2, then an individual would have stage 3 anterior prolapse.
The measurements:
Total vaginal length (tvl): the distance between the hymen and the deepest point of the posterior fornix (point D) if a cervix is present, or the vaginal cuff (point C) if the cervix is absent
Aa: midline of the anterior vaginal wall, 3 cm proximal to the external urethral meatus
Ba: the lowest point of prolapse of any part of the anterior vaginal wall that is between point Aa and the vaginal apex; if there is no prolapse, defined as -3
Ap: midline of the posterior vaginal wall, 3 cm proximal to the posterior hymen
Bp: lowest point of prolapse of any part of the posterior vaginal wall that is between point Ap and the vaginal apex; if there is no prolapse, defined as -3
C: distance from the hymen to the cervix or vaginal cuff
D: deepest point of the posterior fornix (only measured in women with a cervix)
Genital hiatus (gh): the distance between the external urethral meatus (anteriorly) and the posterior midline hymen
Perineal body (pb): the distance between the posterior midline hymen and the midanal opening
Image by Lecturio.
Table: The POP-Q grid: The 9 POP-Q values are frequently recorded in a standardized grid[1]
An easier but less precise system of assessing a prolapse
Compares the maximal point of descent of the prolapse to the hymenHymenA thin fold of mucous membrane situated at the orifice of the vagina.Vagina, Vulva, and Pelvic Floor: Anatomy during valsalva
All 3 compartments (anterior, posterior, and apex) should be assessed and can be graded separately
GradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis:
Grade 0: no prolapse, normal position for each compartment
An 87-year-old woman with stage IV (POP-Q) and grade 4 (Baden-Walker) uterine prolapse
Image: “An 87-year-old woman with uterine prolapse Stage IV” by Asama Vanichtantikul et al. License: CC BY 4.0
Management
Management of POP is based on stage/grade, symptoms, and overall well-being of the subject. All cases should be offered conservative management. Some individuals with more severe symptoms may desire surgery.
Reduce straining with defecationDefecationThe normal process of elimination of fecal material from the rectum.Gastrointestinal Motility (i.e., constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation) via dietary changes and medications.
Avoid smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases to reduce chronic cough.
Pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscle training
Usually used as a primary prevention technique
Also aids in controlling urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence
One-to-one PFPT is effective for improving stages I and II POP.[2]
Vaginal pessaryVaginal pessaryDevices worn in the vagina to provide support to displaced uterus or rectum. Pessaries are used in conditions such as uterine prolapse; cystocele; or rectocele.Pelvic Organ Prolapse:
A medical grade silicone- or latex-based device that is inserted into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Supports the pelvic organs and restores pelvic anatomy
Multiple shapes available (see image)
Fit in the office by a clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship:[4]
Ensure that the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and bowel are empty.
Place a “trial” pessary in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy.
Have the patient walk, bend, jump, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC). to ensure comfort and effectiveness.
Have the patient attempt to void, to ensure that micturition is not inhibited.
Goal is to fit the largest pessary that does not cause discomfort.
A finger should be able to pass between the pessary and the wall of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy.
Vaginal estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy cream is often used as an adjunct to prevent vaginal erosionsErosionsCorneal Abrasions, Erosion, and Ulcers.
Can be removed by the individual at home as often as desired, or every 3‒6 months by a clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship in the office
Indicated in symptomatic individuals if they express a desire for surgical correction. Note that unless the POP is causing urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium, the decision for surgery is driven primarily by the patient’s desires after undergoing counseling on risks/benefits/alternatives.
Refer patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who desire surgical management to a urogynecologist (or general gynecologist with appropriate training).[2]
Reconstructive surgery:[1]
Anterior repair (anterior colporrhaphyAnterior ColporrhaphyPelvic Organ Prolapse): strengthening the “ceiling” of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, between the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy and the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess
Posterior repair (posterior colporrhaphyPosterior ColporrhaphyPelvic Organ Prolapse): strengthening the “floor” of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, between the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy and the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Suspensory procedures: to fix parts of the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, and/or uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy to the internal structures (usually involves permanent sutures and/or the use of a mesh)
Sacrocolpopexy (cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy to sacrumSacrumFive fused vertebrae forming a triangle-shaped structure at the back of the pelvis. It articulates superiorly with the lumbar vertebrae, inferiorly with the coccyx, and anteriorly with the ilium of the pelvis. The sacrum strengthens and stabilizes the pelvis.Vertebral Column: Anatomy):
Requires a supracervical hysterectomy
Typically considered the most effective suspensory procedure
Indications/candidates: high risk for recurrence (age < 60, stage III or IV POP, BMIBMIAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity > 26), shortened vaginal length, and intra-abdominal pathology
Often done robotically by urogynecologists
Hysteropexy (attaches the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy to the sacrospinous ligaments, anterior longitudinal ligament, or uterosacral ligamentsUterosacral ligamentsVagina, Vulva, and Pelvic Floor: Anatomy with sutures or mesh)
Benefits of hysteropexy compared to sacrocolpopexy: shorter operative timeOperative timeThe duration of a surgical procedure in hours and minutes.Surgical Infections, lower incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of mesh erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes
Benefits of sacrocolpopexy: lower risk of mesh complications, lower risk of uterine and cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer, no uterus-related bleeding/painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Sacrospinous ligament fixation (sutures suspend the vaginal apex to the sacrospinous ligament, typically on the right side in order to avoid the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy)
Obliterative surgery:
Surgical obliteration/closing off the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy to prevent further prolapse (colpocleisis)
Reserved for women who no longer desire vaginal penetrationPenetrationX-rays and who cannot tolerate more extensive surgeries
Complications of surgical management[1,3]
Complications associated with the use of mesh:
Risk of complications are significantly higher when mesh (as opposed to native tissue) is used.
Around 12% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship experience complications with mesh.
Often require repeat operations
Mesh complications include:
ErosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes and contracture into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, and/or rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Chronic painChronic painAching sensation that persists for more than a few months. It may or may not be associated with trauma or disease, and may persist after the initial injury has healed. Its localization, character, and timing are more vague than with acute pain.Pain Management
Small-bowel obstruction or ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Because of these risks:
Transvaginal “mesh kits” are not recommended (taken off the market in the US around 2011 owing to unacceptably high risks for complications).[1]
Synthetic mesh for POP should be used only in complex cases with recurrent prolapse (e.g., sacrocolpopexy) and by surgeons with advanced training in multidisciplinary referral centers.[3]
Risk of failure/high risk of recurrent POP (may be as high as 50% for some procedures)
Injury to the surrounding organs (e.g., bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy, urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, bowel)
Bleeding
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula (rectovaginal or vesicovaginal)
Sexual dysfunctionSexual dysfunctionPhysiological disturbances in normal sexual performance in either the male or the female.Sexual Physiology due to:
Shortened vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy/changes in anatomy
Restriction of the vaginal caliber (can potentially be managed with estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy cream and vaginal dilators)
Billing and Coding
Diagnosis Codes:
These codes are used to classify Pelvic Organ ProlapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse, a condition where pelvic organs like the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess or uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy descend from their normal position. Specific codes identify the type of prolapse, such as a cystoceleCystoceleA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse (bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess) or uterine prolapseUterine prolapseDownward displacement of the uterus. It is classified in various degrees: in the first degree the uterine cervix is within the vaginal orifice; in the second degree the cervix is outside the orifice; in the third degree the entire uterus is outside the orifice.Pelvic Organ Prolapse.
Domain
Code
Description
ICD-10-CM
N81.10
CystoceleCystoceleA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse, unspecified
Pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse (disorder)
Evaluation & Workup:
This CPT code is used for urodynamic studies, which are tests performed to assess bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and urethral function, often used in women with prolapse who also experience urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence.
These codes represent common treatments for prolapse, including the non-surgical fitting of a pessary (a supportive device inserted into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy) and surgical procedures like sacrocolpopexy to restore organ support.
Domain
Code
Description
CPT
57160
Fitting and insertion of pessary or other intravaginal support device
Anterior colporrhaphyAnterior ColporrhaphyPelvic Organ Prolapse, repair of cystoceleCystoceleA hernia-like condition in which the weakened pelvic muscles cause the urinary bladder to drop from its normal position. Fallen urinary bladder is more common in females with the bladder dropping into the vagina and less common in males with the bladder dropping into the scrotum.Pelvic Organ Prolapse with or without repair of urethrocele
Medications:
This code is used to prescribe topical estrogen therapyEstrogen therapyThe use of hormonal agents with estrogen-like activity in postmenopausal or other estrogen-deficient women to alleviate effects of hormone deficiency, such as vasomotor symptoms, dyspareunia, and progressive development of osteoporosis. This may also include the use of progestational agents in combination therapy.Menopause, which does not fix the prolapse itself but can improve the health and thickness of vaginal tissues, potentially reducing symptoms like irritation and discomfort.
Domain
Code
Description
RxNorm
4099
EstradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins (ingredient)
Complications & Supportive Procedures:
These codes are used to document complications arising from severe prolapse, such as ulcerationUlcerationCorneal Abrasions, Erosion, and Ulcers of the exposed vaginal tissue and acute urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium if the prolapse kinks the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy.
American College of Obstetricians and Gynecologists and the American Urogynecologic Society. (2019). Pelvic organ prolapse (interim update). Female Pelvic Medicine & Reconstructive Surgery, 25(6), 397–408. https://doi.org/10.1097/SPV.0000000000000794
Chapple, C. R., Cruz, F., Deffieux, X., Milani, A. L., Arlandis, S., Artibani, W., Bauer, R. M., Burkhard, F., Cardozo, L., Castro-Diaz, D., Cornu, J. N., Deprest, J., Gunnemann, A., Gyhagen, M., Heesakkers, J., Koelbl, H., MacNeil, S., Naumann, G., Roovers, J., Salvatore, S., … Abdel-Fattah, M. (2017). Consensus statement of the European Urology Association and the European Urogynaecological Association on the use of implanted materials for treating pelvic organ prolapse and stress urinary incontinence (abstract). European Urology, 72(3), 424–431. https://doi.org/10.1016/j.eururo.2017.03.048
ACOG Committee on Practice Bulletins—Gynecology. (2007). ACOG practice bulletin no. 85: Pelvic organ prolapse. Obstetrics and Gynecology, 110(3), 717–729. https://doi.org/10.1097/01.AOG.0000263925.97887.72
Create your free account or log in to continue reading!