Nerve roots emerge from the spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy at the C1 level and below.
Cervical plexus
C1 through C4 nerve roots close to the spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy merge to form the cervical plexus.
Cutaneous branches of the cervical plexus innervate the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions, transmitting sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology information:
C2: The lesser occipitalOccipitalPart of the back and base of the cranium that encloses the foramen magnum.Skull: Anatomy nerve innervates the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions on the posterolateral aspect of the head and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess.
C2, C3: The greater auricular nerve innervates the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions of the ear and the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions over the parotid glandsParotid glandsThe largest of the three pairs of salivary glands. They lie on the sides of the face immediately below and in front of the ear.Gastrointestinal Secretions.
C2, C3: The transverse cervical nerve innervates the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions on the anterior and lateral aspects of the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess.
C3, C4: The supraclavicular nerve innervates the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions of the shoulder and clavicleClavicleA bone on the ventral side of the shoulder girdle, which in humans is commonly called the collar bone.Clavicle Fracture region.
MotorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology branches of the cervical plexus innervate muscles of the shoulders and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess:
C1, C3: The ansa cervicalis (superior and inferior roots) innervates the infrahyoid muscles (omohyoid, sternohyoid, and sternothyroid) of the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess.
C3, C5: The phrenic nervePhrenic nerveThe motor nerve of the diaphragm. The phrenic nerve fibers originate in the cervical spinal column (mostly C4) and travel through the cervical plexus to the diaphragm.Diaphragm: Anatomy innervates the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy.
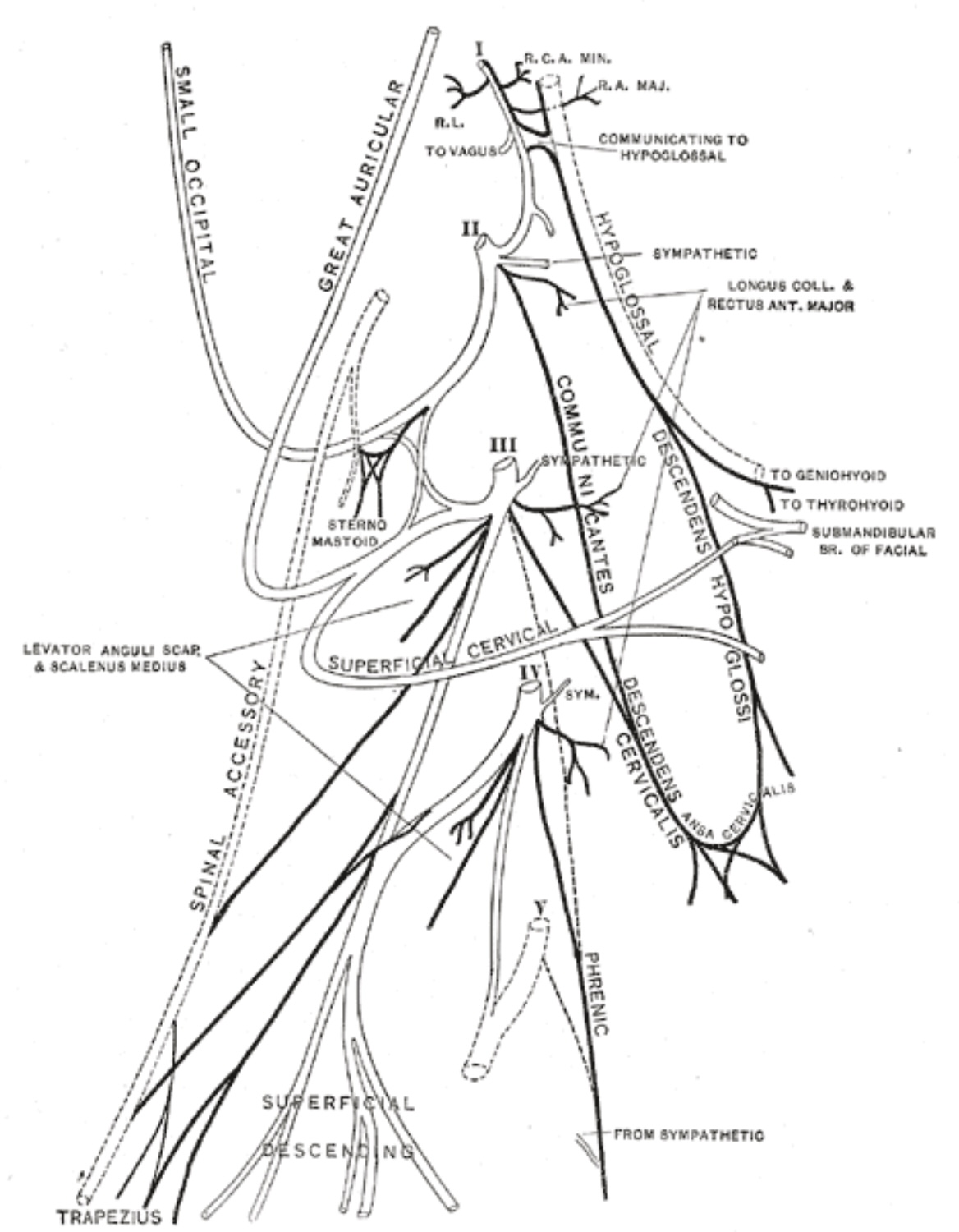
Cervical plexus:
C1 through C4 nerve roots close to the spinal cord merge to form the cervical plexus.
Image: “Cervical plexus” by Henry Vandyke Carter. License: Public Domain
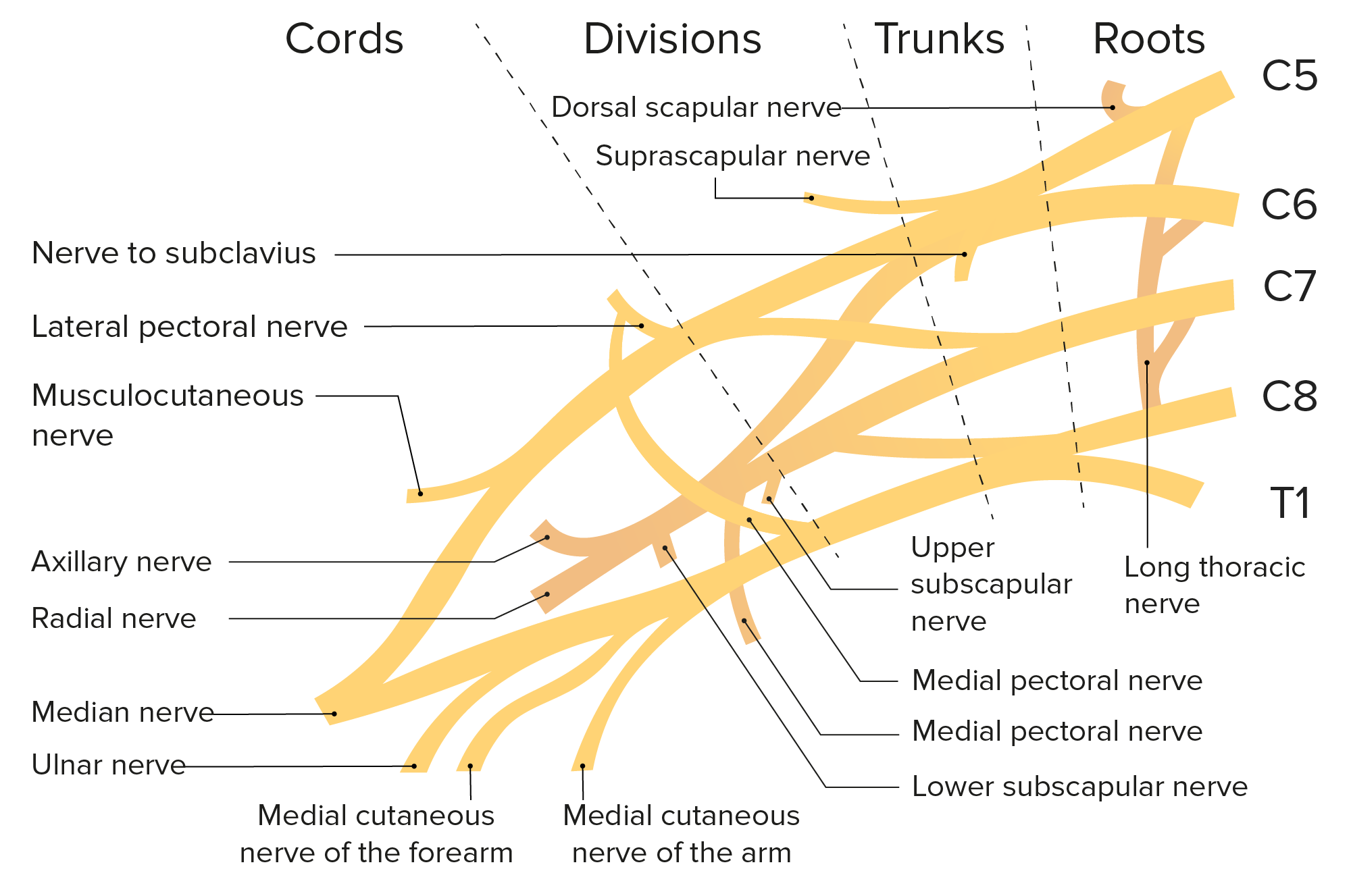
Brachial plexus
C5 through T1 nerve roots merge to form the brachial plexus, which travels from the spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy into the cervicoaxillary canal and the armpit. The nerves are divided into regions called trunks, divisions, cords, branches, and nerves.
Trunks:
C5 and C6 roots merge to form the upper trunk.
The C7 root forms the middle trunk.
C8 and T1 roots merge to form the lower trunk.
Divisions: Each trunk divides into an anterior and posterior division, which creates 6 distinct divisions.
Cords are named with respect to the location of the axillary arteryAxillary ArteryThe continuation of the subclavian artery; it distributes over the upper limb, axilla, chest and shoulder.Axilla and Brachial Plexus: Anatomy:
Anterior divisions of the upper and middle trunk form the lateral cord.
The anterior division of the lower trunk forms the medial cord.
Posterior divisions of all 3 trunks form the posterior cord.
The lateral cord divides and gives rise to the musculocutaneous nerveMusculocutaneous NerveA major nerve of the upper extremity. The fibers of the musculocutaneous nerve originate in the lower cervical spinal cord (usually C5 to C7), travel via the lateral cord of the brachial plexus, and supply sensory and motor innervation to the upper arm, elbow, and forearm.Axilla and Brachial Plexus: Anatomy and contributes to the median nerveMedian NerveA major nerve of the upper extremity. In humans, the fibers of the median nerve originate in the lower cervical and upper thoracic spinal cord (usually C6 to T1), travel via the brachial plexus, and supply sensory and motor innervation to parts of the forearm and hand.Cubital Fossa: Anatomy.
The posterior cord branches and gives rise to the axillary nerveAxillary nerveAxilla and Brachial Plexus: Anatomy, the subscapular nerve, the thoracodorsal nerveThoracodorsal nerveAxilla and Brachial Plexus: Anatomy, and the radial nerveRadial NerveA major nerve of the upper extremity. In humans the fibers of the radial nerve originate in the lower cervical and upper thoracic spinal cord (usually C5 to T1), travel via the posterior cord of the brachial plexus, and supply motor innervation to extensor muscles of the arm and cutaneous sensory fibers to extensor regions of the arm and hand.Axilla and Brachial Plexus: Anatomy.
The medial cord branches and contributes to the median nerveMedian NerveA major nerve of the upper extremity. In humans, the fibers of the median nerve originate in the lower cervical and upper thoracic spinal cord (usually C6 to T1), travel via the brachial plexus, and supply sensory and motor innervation to parts of the forearm and hand.Cubital Fossa: Anatomy and then becomes the ulnar nerveUlnar NerveA major nerve of the upper extremity. In humans, the fibers of the ulnar nerve originate in the lower cervical and upper thoracic spinal cord (usually C7 to T1), travel via the medial cord of the brachial plexus, and supply sensory and motor innervation to parts of the hand and forearm.Axilla and Brachial Plexus: Anatomy. The medial cord also gives rise to the medial cutaneous nerves of the armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy and forearmForearmThe forearm is the region of the upper limb between the elbow and the wrist. The term “forearm” is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: Anatomy.
Schematic of the brachial plexus and the branches of the brachial plexus
Image by Lecturio.
Phrenic Nerve Injury
The phrenic nervePhrenic nerveThe motor nerve of the diaphragm. The phrenic nerve fibers originate in the cervical spinal column (mostly C4) and travel through the cervical plexus to the diaphragm.Diaphragm: Anatomy arises from anterior rami of C3, C4, and C5 nerve roots and provides motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology innervation to the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy:
Etiology of injury
Cardiac and thoracic surgeryThoracic SurgeryBasic surgical intervention in the thoracic cavity has the primary goal of alleviating any malady that mechanically affects the function of the heart and lungs, which can be secondary to underlying pathologies or, most commonly, trauma. Interventions include tube thoracostomy, thoracentesis, and emergency thoracotomy.Thoracic Surgery
Blunt or penetrating trauma
Metabolic diseases (e.g., diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus)
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., Lyme diseaseLyme diseaseLyme disease is a tick-borne infection caused by the gram-negative spirochete Borrelia burgdorferi. Lyme disease is transmitted by the black-legged Ixodes tick (known as a deer tick), which is only found in specific geographic regions. Patient presentation can vary depending on the stage of the disease and may include a characteristic erythema migrans rash. Lyme Disease, herpes zosterHerpes ZosterVaricella-zoster virus (VZV) is a linear, double-stranded DNA virus in the Herpesviridae family. Shingles (also known as herpes zoster) is more common in adults and occurs due to the reactivation of VZV. Varicella-Zoster Virus/Chickenpox)
Multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor
Immunologic diseases (e.g., Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome)
Clinical features
Clinical features vary and depend upon the extent of the injury. Clinical features depend on whether nerves are injured bilaterally or unilaterally:
General:
Shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea
Recurrent pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
AnxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder
InsomniaInsomniaInsomnia is a sleep disorder characterized by difficulty in the initiation, maintenance, and consolidation of sleep, leading to impairment of function. Patients may exhibit symptoms such as difficulty falling asleep, disrupted sleep, trouble going back to sleep, early awakenings, and feeling tired upon waking.Insomnia
Morning headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Unilateral diaphragmatic paralysis:
Asymptomatic at rest
Exertional dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
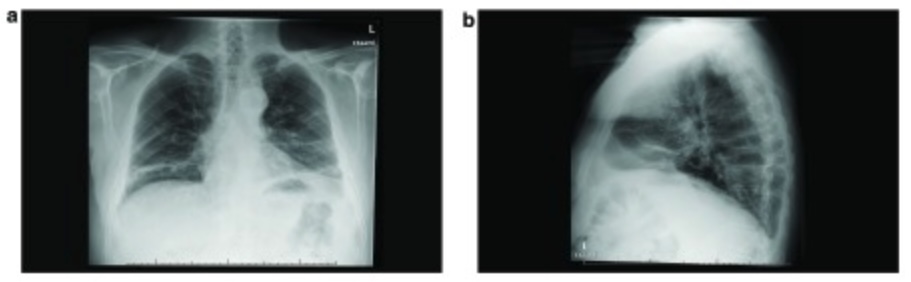
Often found as an incidental finding on chest radiograph
Bilateral diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy paralysis: severe shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea
Physical examination
Decreased breath sounds on the affected side
Dullness on percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination of the affected side
Diaphragmatic ultrasonography (diaphragmatic movement and thickness)
Pulmonary function tests and arterial blood gases
Diaphragmatic electromyographyElectromyographyRecording of the changes in electric potential of muscle by means of surface or needle electrodes.Becker Muscular Dystrophy
Measurement of transdiaphragmatic pressure
Management
Unilateral diaphragmatic paralysis:
Most are asymptomatic and do not require treatment.
Surgical plication
Transient ventilatory support
Bilateral diaphragmatic paralysis:
Ventilatory support
Diaphragmatic pacing
Surgical nerve reconstruction and diaphragmatic pacing
Image: “Chest X-Ray on admission” by Department of medicine (ward 45), the National hospital of Sri Lanka, Regent Street, Colombo 00800, Sri Lanka. License: CC BY 2.0
Image: “(a) Frontal chest radiograph during initial presentation. (b) Lateral chest radiograph during initial presentation” by Department of Respiratory Medicine, Maastricht University, Medical Centre, Maastricht, 6200 MD, Netherlands. License: CC BY 4.0
MotorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology innervation to the supraspinatus and infraspinatus muscles
SensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology innervation to the glenohumeral and acromioclavicular joints
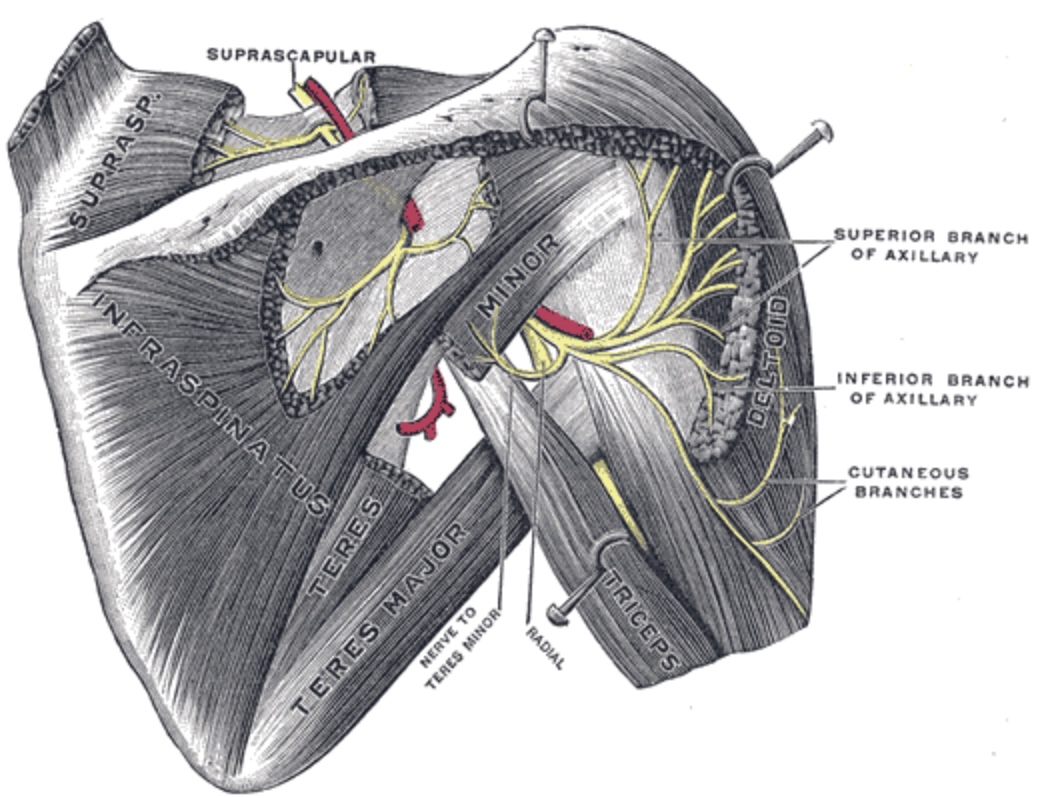
Injury most commonly occurs at the suprascapular notch, the spinoglenoid notch, or the superior transverse scapular ligament.
The path of the suprascapular nerve: The suprascapular nerve is most commonly injured at the suprascapular notch, the spinoglenoid notch, or the superior transverse scapular ligament.
Image: “Suprascapular and axillary nerves of right side, seen from behind” by Henry Vandyke Carter. License: Public Domain
Ganglion cystGanglion cystNodular tumor-like lesions or mucoid flesh, arising from tendon sheaths, ligaments, or joint capsule, especially of the hands, wrists, or feet. They are not true cysts as they lack epithelial wall. They are distinguished from synovial cysts by the lack of communication with a joint cavity or the synovial membrane.Examination of the Upper Limbs
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types cyst
Shoulder painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways (impingement at the suprascapular notch)
Painless weakness (impingement at the spinoglenoid notch)
Muscle atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Diagnosis
Clinical (based on clinical features of disease):
Classic finding: aching painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the superior and posterior shoulder
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways may radiate to the armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy or neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess.
Typically, symptoms worsen slowly.
Electrodiagnostic studies are the gold standard for diagnosis: evaluation of nerve latency, amplitude, fibrillation, and sharp waves
Imaging:
Radiograph can show bony disease.
CT is useful for nerve impingement or abnormality.
Physical therapyPhysical TherapyBecker Muscular Dystrophy (to preserve the range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs and strengthen shoulder/rotator cuff muscles)
The individual should avoid precipitating movements.
Surgical excision (e.g., cystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change, tumors)
Cause of injury: nerve entrapment due to hypertrophyHypertrophyGeneral increase in bulk of a part or organ due to cell enlargement and accumulation of fluids and secretions, not due to tumor formation, nor to an increase in the number of cells (hyperplasia).Cellular Adaptation of the middle scalene muscle
Clinical features vary, but the classic appearance is a “winged scapula”:
Winged scapula: The scapula is further from the midline than the noninjured side.
Limited range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs (inability to pull the shoulder back)
Shoulder painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Muscle spasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy
Surgery (e.g., breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer surgery)
Stretch or traction from repetitive activities (e.g., carrying a heavy weight for a prolonged period of time)
Clinical features
Clinical features are generally minimal. Classic findings and symptoms may be present in more severe cases:
Winged scapula: most prominent when the affected armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy is lifted forward
Demonstrated by the individual pressing against a wall with outstretched arms
A pure motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology nerve branching from the posterior cord
If the latissimus dorsi is used for reconstruction during transplantation, the nerve supply is preserved.
Etiology
Thoracodorsal nerveThoracodorsal nerveAxilla and Brachial Plexus: Anatomy injury can occur from surgical injury during axillary dissection for breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer.
Reece, C. L., Varacallo, M. A., Dulebohn, S. C., & Susmarski, A. J. (2024). Suprascapular Nerve Injury. In StatPearls [Internet]. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK559151/