The brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region is a network of nerves that originate from the lower cervical and upper thoracic nerve roots. The causes of brachial plexopathies include traumatic injuries, birth-related injuries, iatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome procedures, neoplastic processes, and previous treatment with radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology and motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology deficits related to the site of the lesion and the nerves involved. Diagnosis is made based on clinical findings, imaging, and electrodiagnostic studies. Treatment is related to the underlying cause and may be medical or surgical.
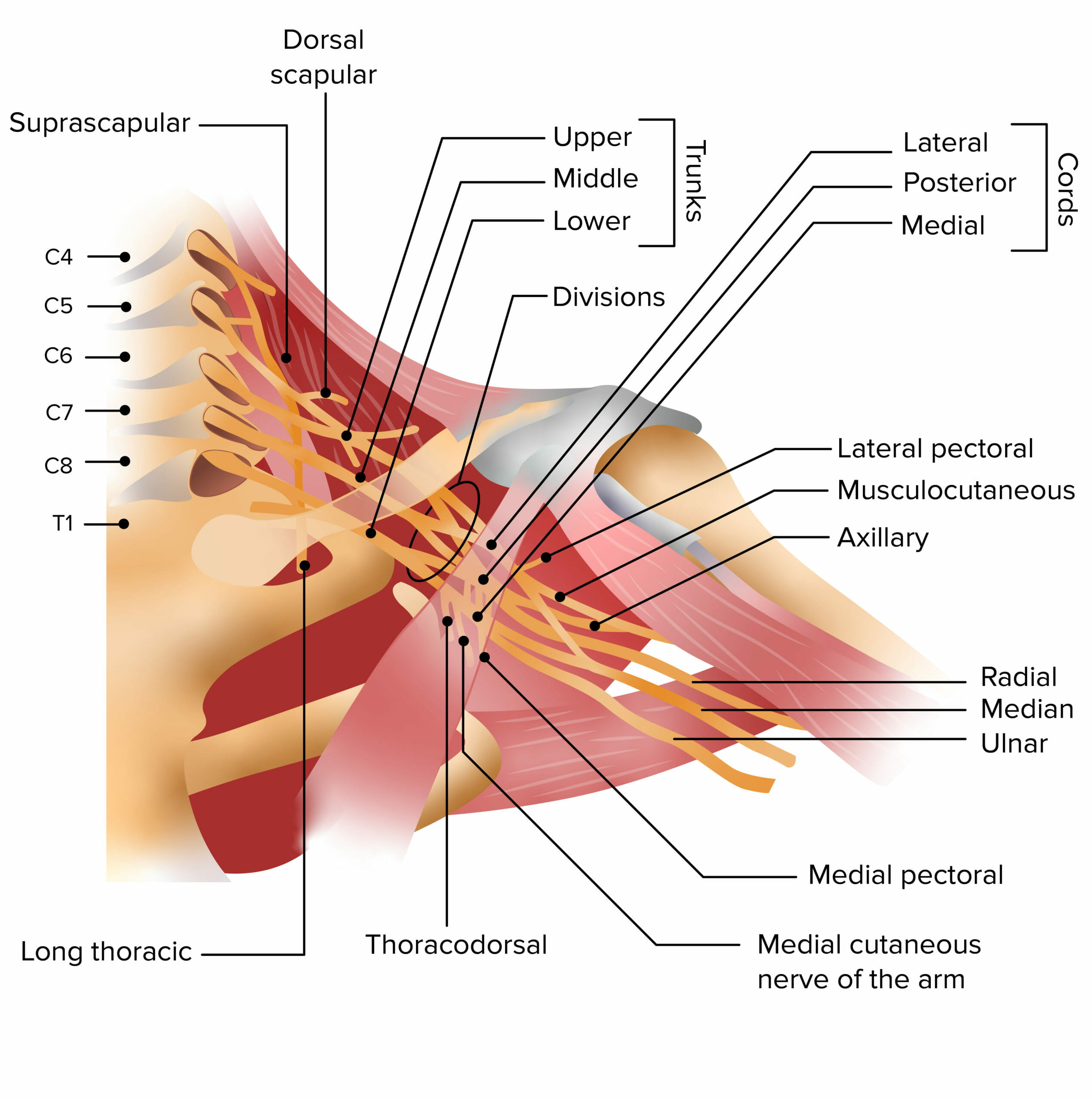
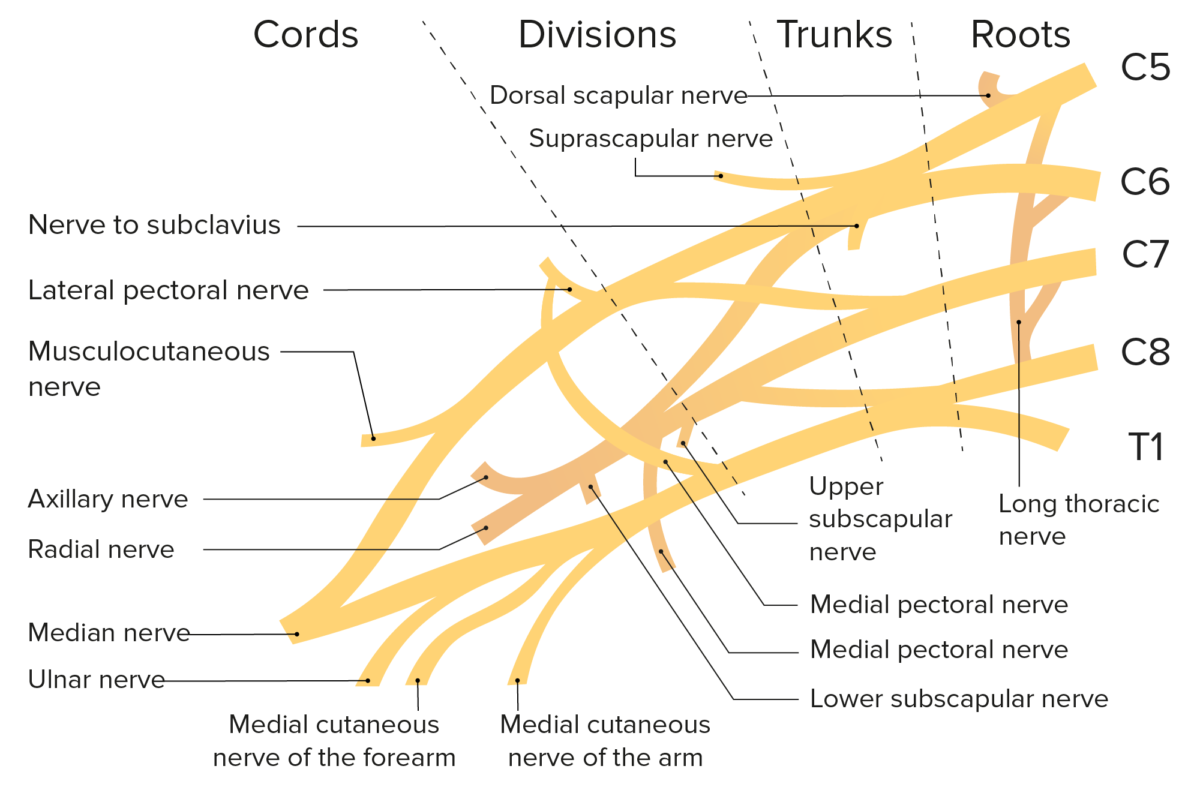
The brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region is a network of nerves from which all the motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology and sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology nerves of the upper extremity arise. It is formed by the nerve roots from C5 to T1 and divides into:
Trunks:
Upper trunk: formed by the C5 and C6 roots
Middle trunk: formed by the C7 root
Lower trunk: formed by the C8 and T1 roots
Divisions: Each trunk divides into an anterior and posterior division.
Cords, branches, and nerves:
Lateral cord branches into:
Musculocutaneous nerveMusculocutaneous NerveA major nerve of the upper extremity. The fibers of the musculocutaneous nerve originate in the lower cervical spinal cord (usually C5 to C7), travel via the lateral cord of the brachial plexus, and supply sensory and motor innervation to the upper arm, elbow, and forearm.Axilla and Brachial Plexus: Anatomy
Median nerveMedian NerveA major nerve of the upper extremity. In humans, the fibers of the median nerve originate in the lower cervical and upper thoracic spinal cord (usually C6 to T1), travel via the brachial plexus, and supply sensory and motor innervation to parts of the forearm and hand.Cubital Fossa: Anatomy
Radial nerveRadial NerveA major nerve of the upper extremity. In humans the fibers of the radial nerve originate in the lower cervical and upper thoracic spinal cord (usually C5 to T1), travel via the posterior cord of the brachial plexus, and supply motor innervation to extensor muscles of the arm and cutaneous sensory fibers to extensor regions of the arm and hand.Axilla and Brachial Plexus: Anatomy
Medial cord branches into:
Median nerveMedian NerveA major nerve of the upper extremity. In humans, the fibers of the median nerve originate in the lower cervical and upper thoracic spinal cord (usually C6 to T1), travel via the brachial plexus, and supply sensory and motor innervation to parts of the forearm and hand.Cubital Fossa: Anatomy
Ulnar nerveUlnar NerveA major nerve of the upper extremity. In humans, the fibers of the ulnar nerve originate in the lower cervical and upper thoracic spinal cord (usually C7 to T1), travel via the medial cord of the brachial plexus, and supply sensory and motor innervation to parts of the hand and forearm.Axilla and Brachial Plexus: Anatomy
Medial cutaneous nerves of the armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy and forearmForearmThe forearm is the region of the upper limb between the elbow and the wrist. The term “forearm” is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: Anatomy
Brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region syndromes are rare:
Occur in 0.4% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with cancer
Occur in 2% to 5% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship exposed to radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of idiopathicIdiopathicDermatomyositis brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy or brachial amyotrophy is 2–3 per 100,000.
The incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency ratio for traumatic injuries is 2:1, men to women.
Classification
Based on the location of the injury
Supraclavicular preganglionic:
Associated with avulsion of nerve roots
Usually results in permanent motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology and sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology deficits
Denervation of neck musclesNeck musclesThe muscles of the neck can be divided into 3 groups: anterior, lateral, and posterior neck muscles. Each of the groups is subdivided according to function and the precise location of the muscles.Muscles of the Neck: Anatomy is common.
Supraclavicular postganglionic:
Often due to traction injuries
Nerve roots remain intact.
Infraclavicular: involves individual branches of the plexus
Pathogenesis
The brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region can be injured by several mechanisms:
Nerve traction:
Also known as stretch injury (as seen in delivery of infants)
Occurs from sudden severe pull or tension of the nerves
IschemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage resulting from occlusion of small intraneural vessels due to:
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Metabolic abnormalities
Direct nerve invasion by cancer cells
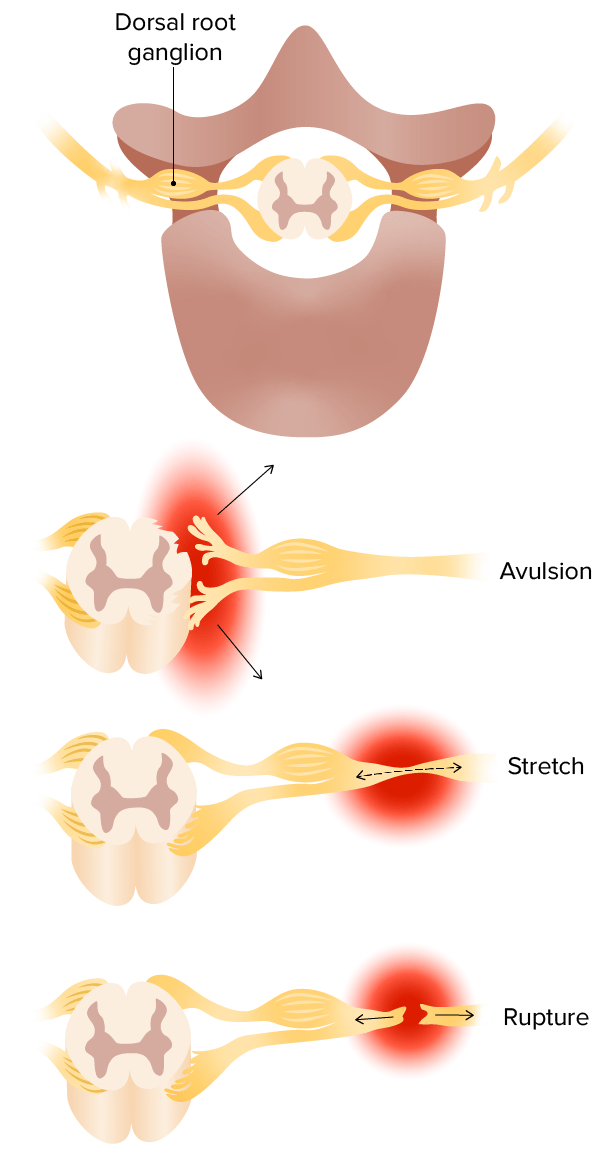
Mechanisms of brachial plexus injury:
Top: Avulsion injuries pull the rootlets out of the spinal cord.
Middle: Stretch injuries attenuate the nerve.
Bottom: Ruptures lead to complete discontinuity of the nerve.
Clinical symptom onset may vary from acute to insidious, with shoulder or upper armUpper ArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: AnatomypainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways described as “electric shock-like” or a burning sensation.
Traumatic plexopathies
Trauma from injuries:
Open: knife or gunshot woundsGunshot woundsDisruption of structural continuity of the body as a result of the discharge of firearms.Penetrating Chest Injury, animal bites
Closed: motorcycle/automobile accidents, falls from a height, hematomas
Manifestations correlate to the nerve(s) affected by the injury.
Trauma from sports injuries: burner (also called stinger)
Caused by downward traction of the shoulder, involving the upper trunk of the brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region
Most often due to tackling
Manifests as transient numbness, paresthesiasParesthesiasSubjective cutaneous sensations (e.g., cold, warmth, tingling, pressure, etc.) that are experienced spontaneously in the absence of stimulation.Posterior Cord Syndrome, or weakness in the armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy
Usually brief and self-limited; occasionally, recovery may take days to weeks
Backpack palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies (also known as rucksack paralysis or cadet palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies):
Affects the upper trunk (C5–C6)
Presents after wearing a backpack or similar apparatus
Usually painless, due to stretch or compressionCompressionBlunt Chest Trauma of the nerve fibersNerve FibersSlender processes of neurons, including the axons and their glial envelopes (myelin sheath). Nerve fibers conduct nerve impulses to and from the central nervous system.Nervous System: Histology
Weakness in extensionExtensionExamination of the Upper Limbs of the forearmForearmThe forearm is the region of the upper limb between the elbow and the wrist. The term “forearm” is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: Anatomy, wrist, and fingers
Some sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology loss in the same distribution
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship recover fully in a few months.
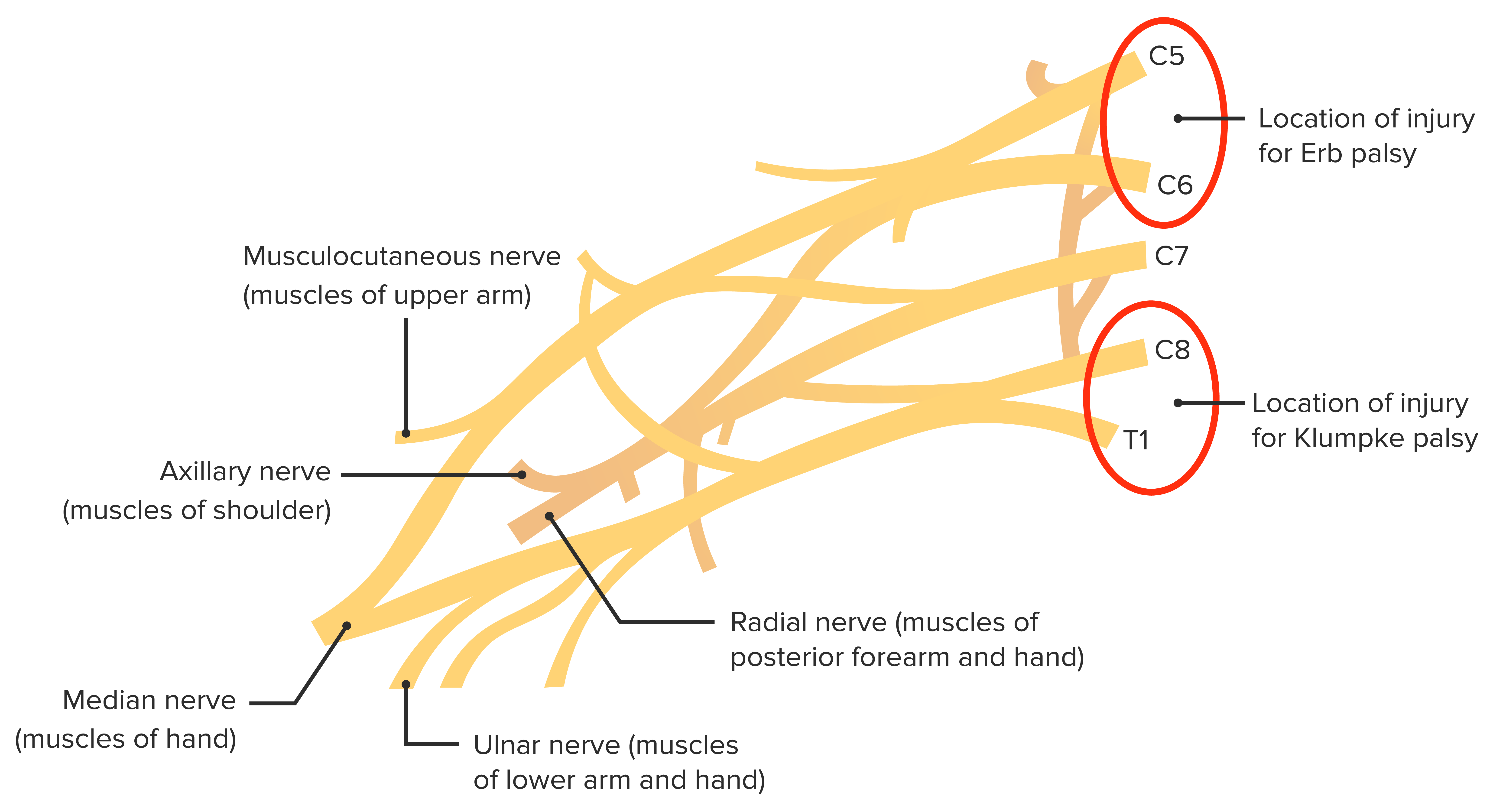
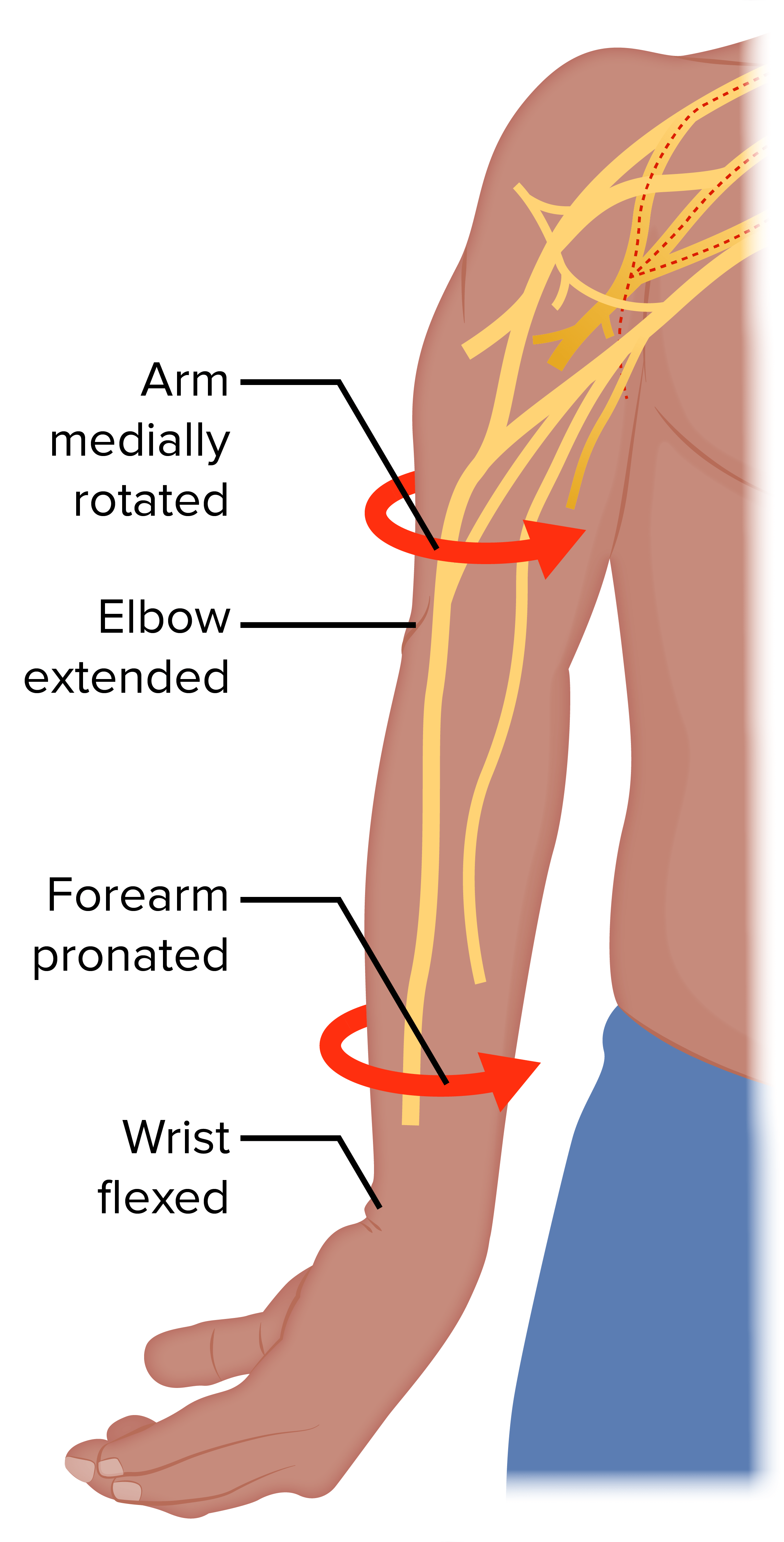
Obstetric brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region palsies:
More common than Klumpke palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Affects C5 and C6 nerve roots
DeformityDeformityExamination of the Upper Limbs: armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy hanging by the side, adducted, and medially rotated
Klumpke palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies:
Inflammatory disorder of the brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region
Also known as Parsonage-Turner syndromeParsonage-Turner SyndromeMononeuropathy and Plexopathy or idiopathicIdiopathicDermatomyositis brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy
May affect both children and adults
Sudden onset of shoulder/upper armUpper ArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: AnatomypainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways → progressive weakness and atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Hereditary brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance
Characterized by painful, recurrent brachial plexopathies
Features: short stature, hypotelorism, unusual skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions folds, creases on the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Rare
Neoplastic brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Presents with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the shoulder/axillaAxillaThe axilla is a pyramid-shaped space located between the upper thorax and the arm. The axilla has a base, an apex, and 4 walls (anterior, medial, lateral, posterior). The base of the pyramid is made up of the axillary skin. The apex is the axillary inlet, located between the 1st rib, superior border of the scapula, and clavicle. Axilla and Brachial Plexus: Anatomy
Types:
Primary: due to neurogenic tumors (e.g., schwannomas, neurofibromas)
Paraneoplastic: due to demyelinating injury from antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against the myelin sheath, associated with Hodgkin lymphomaLymphomaA general term for various neoplastic diseases of the lymphoid tissue.Imaging of the Mediastinum
C8 or T1 nerve root involvement:
Seen with Pancoast tumors (usually non–small cell lung carcinoma (NSCLC))
SympatheticneuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology run through the brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region over the lung apex.
Clinical symptoms: Horner syndromeHorner syndromeHorner syndrome is a condition resulting from an interruption of the sympathetic innervation of the eyes. The syndrome is usually idiopathic but can be directly caused by head and neck trauma, cerebrovascular disease, or a tumor of the CNS. Horner Syndrome (ptosisPtosisCranial Nerve Palsies, miosisMiosisPupil: Physiology and Abnormalities, and anhidrosis) due to an interruption of the cervical sympathetic chain supply to the eye
Radiation-induced brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
May not present until months or years after radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Due to direct axonal damage, demyelinationDemyelinationMultiple Sclerosis, microvascular infarction, and fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans
Thoracic outletThoracic OutletThoracic Outlet Syndrome syndrome (TOSTOSThoracic outlet syndrome (TOS) is a broad term used for a spectrum of syndromes related to the general region of the thoracic outlet, which involves the compression or irritation of elements of the brachial plexus, subclavian artery, or subclavian vein.Thoracic Outlet Syndrome):
Due to compressionCompressionBlunt Chest Trauma of blood vessels and nerves as they pass between the clavicleClavicleA bone on the ventral side of the shoulder girdle, which in humans is commonly called the collar bone.Clavicle Fracture and the 1st rib
Causes:
Accidents
Repetitive-use type of occupational injuries
Anatomic variants
HypertrophyHypertrophyGeneral increase in bulk of a part or organ due to cell enlargement and accumulation of fluids and secretions, not due to tumor formation, nor to an increase in the number of cells (hyperplasia).Cellular Adaptation of the scalene or pectoralis minor muscle in weight lifters and athletes
Symptoms vary but may include:
Muscle weakness
Numbness
Ischemic changes
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema of the upper extremities
Diabetes-related brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Not as common as lumbosacral plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy
May be mononeuropathies of the ulnar and median nerves
IatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome plexopathies:
Classic postoperative paresisParesisA general term referring to a mild to moderate degree of muscular weakness, occasionally used as a synonym for paralysis (severe or complete loss of motor function). In the older literature, paresis often referred specifically to paretic neurosyphilis. ‘general paresis’ and ‘general paralysis’ may still carry that connotation. Bilateral lower extremity paresis is referred to as paraparesis.Spinal Disk Herniation:
Caused by traction or pressure during surgery
Presents with painless weakness and paresthesia
Recovery is rapid and complete.
Post-median sternotomySternotomyMaking an incision in the sternum.Cardiac SurgeryplexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Occurs after open-heart surgery
Caused by injury to the anterior ramus C8
Presents with handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy weakness, paresthesia, and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the C8 dermatomeDermatomeSpinal Disk Herniation
Anesthetic block plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Occurs after regional infraclavicular brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region blockade
Due to trauma from the infusion needle, hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception formation, or neurotoxicity from the local anesthetic
Medial brachial fascial compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome:
Occurs after puncture of the axillary or brachial arteryBrachial ArteryThe continuation of the axillary artery; it branches into the radial and ulnar arteries.Cubital Fossa: Anatomy during procedures such as arteriography or axillary regional anesthetic blocks
Expanding hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception causes nerve compressionCompressionBlunt Chest Trauma of the median or ulnar nerves most commonly.
Characteristics of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology changes, weakness, and muscle atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Infection, activity, or injury associated with the onset
Change in symptoms with a change in head, neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess, or armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy position
Change in functionality of the armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy
MalignancyMalignancyHemothorax, radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma, chemotherapyChemotherapyOsteosarcoma
Demyelinating disordersDemyelinating disordersConditions characterized by loss or dysfunction of myelin in the brain, spinal cord, or optic nerves secondary to autoimmune mediated processes. This may take the form of a humoral or cellular immune response directed toward myelin or oligodendroglia associated autoantigens.Posterior Cord Syndrome
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Previous brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy
Details of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care and delivery in neonatal patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship (e.g., stretching/traction)
Physical examination
Visual inspectionInspectionDermatologic Examination for skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions changes:
Surgical scars or wounds
Muscle atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
PalpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination of the muscles of the shoulder and armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy
Range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs (ROM) of the cervical spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy and upper extremity
PupilPupilThe pupil is the space within the eye that permits light to project onto the retina. Anatomically located in front of the lens, the pupil’s size is controlled by the surrounding iris. The pupil provides insight into the function of the central and autonomic nervous systems. Pupil: Physiology and Abnormalities exam for possible Horner syndromeHorner syndromeHorner syndrome is a condition resulting from an interruption of the sympathetic innervation of the eyes. The syndrome is usually idiopathic but can be directly caused by head and neck trauma, cerebrovascular disease, or a tumor of the CNS. Horner Syndrome
Neurological exam:
MotorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology strength
Neonatal patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship: Clinical diagnosis is made when armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy weakness at birth fits a distribution consistent with a brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic Region injury.
Imaging and tests
Cervical spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: AnatomyX-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests for bony abnormalities
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests if concern for lung malignancyMalignancyHemothorax
Ultrasound may distinguish preganglionic from postganglionic traumatic lesions noninvasively.
ElectromyographyElectromyographyRecording of the changes in electric potential of muscle by means of surface or needle electrodes.Becker Muscular Dystrophy (EMG)/nerve conduction studies:
Assesses for axonal damage in motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology nerves
Gives information regarding other diagnoses (e.g., nerve entrapment syndromes)
SensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology nerve conduction studies are more sensitive to axonal loss than motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology nerve studies.
Management
Acute traumatic injuries may lead to plexopathies that are self-limited within a few months. Specific treatments for nontraumatic plexopathies include PT and medications.
Traumatic plexopathies
Some situations may require emergent surgical intervention.
Nonemergency surgery: indicated if no improvement after 3–4 months
Types of procedures:
Neurolysis
Nerve grafts
Nerve transfers
Tendon and muscle transfers
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas: improved function noted in approximately 60% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship after surgical intervention
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Analgesics
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas:
Recovery is slow over 1–3 years.
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may have persistent disabilityDisabilityDetermination of the degree of a physical, mental, or emotional handicap. The diagnosis is applied to legal qualification for benefits and income under disability insurance and to eligibility for social security and workman’s compensation benefits.ABCDE Assessment.
Hereditary brachial plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Analgesics
PT
Neoplastic plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy (RT) to reduce painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Analgesics
Radiation-induced plexopathyPlexopathyNeuropathy is a nerve pathology presenting with sensory, motor, or autonomic impairment secondary to dysfunction of the affected nerve. The peripheral nerves are derived from several plexuses, with the brachial and lumbosacral plexuses supplying the major innervation to the extremities. Mononeuropathy (affecting a single nerve) and plexopathy (affecting the plexus) can occur from trauma, compression, and systemic diseases. Mononeuropathy and Plexopathy:
Gabapentinoids (inhibit neurotransmissionNeurotransmissionThe communication from a neuron to a target (neuron, muscle, or secretory cell) across a synapse. In chemical synaptic transmission, the presynaptic neuron releases a neurotransmitter that diffuses across the synaptic cleft and binds to specific synaptic receptors, activating them. The activated receptors modulate specific ion channels and/or second-messenger systems in the postsynaptic cell. In electrical synaptic transmission, electrical signals are communicated as an ionic current flow across electrical synapses.Synapses and Neurotransmission)
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Tricyclic antidepressantsTricyclic antidepressantsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants (TCAsTCAsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants)
TOSTOSThoracic outlet syndrome (TOS) is a broad term used for a spectrum of syndromes related to the general region of the thoracic outlet, which involves the compression or irritation of elements of the brachial plexus, subclavian artery, or subclavian vein.Thoracic Outlet Syndrome:
Conservative measures:
Weight reduction
Analgesics
Strengthening program
Surgery:
True neurogenic TOSTOSThoracic outlet syndrome (TOS) is a broad term used for a spectrum of syndromes related to the general region of the thoracic outlet, which involves the compression or irritation of elements of the brachial plexus, subclavian artery, or subclavian vein.Thoracic Outlet Syndrome → surgical release of the fibrous bandFibrous bandMeckel’s Diverticulum or resection of the rudimentary cervical rib
Vascular TOSTOSThoracic outlet syndrome (TOS) is a broad term used for a spectrum of syndromes related to the general region of the thoracic outlet, which involves the compression or irritation of elements of the brachial plexus, subclavian artery, or subclavian vein.Thoracic Outlet Syndrome → decompressive surgery
IatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome plexopathies:
Conservative management
Surgical decompression
Neonatal brachial plexusBrachial PlexusThe large network of nerve fibers which distributes the innervation of the upper extremity. The brachial plexus extends from the neck into the axilla. In humans, the nerves of the plexus usually originate from the lower cervical and the first thoracic spinal cord segments (c5-c8 and T1), but variations are not uncommon.Peripheral Nerve Injuries in the Cervicothoracic RegionpalsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies:
PT to promote muscle strengthening
Surgery indications include:
Pan-plexopathy and preganglionic nerve root lesion
Complete nerve disruption and nerve root avulsions
Incomplete functional recovery
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism injection: may be helpful for contracturesContracturesProlonged shortening of the muscle or other soft tissue around a joint, preventing movement of the joint.Wound Healing/muscle imbalances
Psychosocial support for ongoing disabilityDisabilityDetermination of the degree of a physical, mental, or emotional handicap. The diagnosis is applied to legal qualification for benefits and income under disability insurance and to eligibility for social security and workman’s compensation benefits.ABCDE Assessment in childhood
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas:
Spontaneous recovery occurs over 1–3 months in most cases.
More favorable prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas if early clinical improvement in a few weeks
Good prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas with normal or near-normal strength in elbow flexionFlexionExamination of the Upper Limbs, shoulder external rotationExternal RotationExamination of the Upper Limbs, and forearmForearmThe forearm is the region of the upper limb between the elbow and the wrist. The term “forearm” is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: AnatomysupinationSupinationApplies to movements of the forearm in turning the palm forward or upward. When referring to the foot, a combination of adduction and inversion movements of the foot.Examination of the Upper Limbs by 3 months of age
Differential Diagnosis
Cervical radiculopathyCervical RadiculopathySpinal Disk Herniation: refers to painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and neurologic symptoms in the upper extremities due to injury or inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the cervical spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy nerve roots. The causes of cervical radiculopathyCervical RadiculopathySpinal Disk Herniation include cervical disk herniationHerniationOmphalocele, infection, tumorTumorInflammation infiltration, and demyelinationDemyelinationMultiple Sclerosis. The clinical features vary depending on the location and degree of cervical nerve root involvement. Diagnosis is made based on clinical exam, MRI, and electrodiagnostic studies. Treatment can be conservative with PT and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control, or with surgical decompression if there’s no improvement.
Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome (GBSGBSAn acute inflammatory autoimmune neuritis caused by t cell- mediated cellular immune response directed towards peripheral myelin. Demyelination occurs in peripheral nerves and nerve roots. The process is often preceded by a viral or bacterial infection, surgery, immunization, lymphoma, or exposure to toxins. Common clinical manifestations include progressive weakness, loss of sensation, and loss of deep tendon reflexes. Weakness of respiratory muscles and autonomic dysfunction may occur.Polyneuropathy): refers to a family of immune-mediated polyneuropathiesPolyneuropathiesDiseases of multiple peripheral nerves simultaneously. Polyneuropathies usually are characterized by symmetrical, bilateral distal motor and sensory impairment with a graded increase in severity distally. The pathological processes affecting peripheral nerves include degeneration of the axon, myelin or both. The various forms of polyneuropathy are categorized by the type of nerve affected (e.g., sensory, motor, or autonomic), by the distribution of nerve injury (e.g., distal vs. Proximal), by nerve component primarily affected (e.g., demyelinating vs. axonal), by etiology, or by pattern of inheritance.Mononeuropathy and Plexopathy that occur after infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., Campylobacter jejuniCampylobacter jejuniA species of bacteria that resemble small tightly coiled spirals. Its organisms are known to cause abortion in sheep and fever and enteritis in man and may be associated with enteric diseases of calves, lambs, and other animals.Campylobacter). Typical GBSGBSAn acute inflammatory autoimmune neuritis caused by t cell- mediated cellular immune response directed towards peripheral myelin. Demyelination occurs in peripheral nerves and nerve roots. The process is often preceded by a viral or bacterial infection, surgery, immunization, lymphoma, or exposure to toxins. Common clinical manifestations include progressive weakness, loss of sensation, and loss of deep tendon reflexes. Weakness of respiratory muscles and autonomic dysfunction may occur.Polyneuropathy is characterized by acute monophasic neuromuscular paralysisAcute Monophasic Neuromuscular ParalysisGuillain-Barré Syndrome, which is symmetric and ascending and may progress to respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure requiring prolonged hospitalizationProlonged HospitalizationSurgical Infections. Management is mostly supportive and may require either plasma exchangePlasma exchangeRemoval of plasma and replacement with various fluids, e.g., fresh frozen plasma, plasma protein fractions (ppf), albumin preparations, dextran solutions, saline. Used in treatment of autoimmune diseases, immune complex diseases, diseases of excess plasma factors, and other conditions.Thrombotic Thrombocytopenic Purpura or IV immunoglobulinIv ImmunoglobulinDermatomyositis (IVIGIVIGDermatomyositis).
Multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor (MSMSMultiple sclerosis (MS) is a chronic inflammatory autoimmune disease that leads to demyelination of the nerves in the CNS. Young women are more predominantly affected by this most common demyelinating condition.Multiple Sclerosis): chronic inflammatory autoimmune disease leading to demyelinationDemyelinationMultiple Sclerosis of the CNS. The etiology is uncertain, but both genetic and environmental factors are believed to play a role. Diagnosis is made by MRI as well as CSF examination. Management involves corticosteroidsCorticosteroidsChorioretinitis for acute exacerbations and disease-modifying agents to reduce exacerbations and slow the progression of the disease.
Spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy injury: associated with complete or incomplete syndromes due to vertebral fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures, disk herniationHerniationOmphalocele, or, in some cases, arterial occlusion/ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage. The cardinal sign is a discrete injury level, above which neurologic function is intact, and below which it is absent or markedly diminished. Diagnosis is by clinical exam and MRI. Management depends on the cause of the spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy syndrome and involves long-term symptomatic care and rehabilitation.
References
Ho, K. K. F., Guazzo, L., & Muller, J. (2023). Neurogenic thoracic outlet syndrome: When to consider the diagnosis and current management options. Australian Journal of General Practice, 52(9), 627–632. https://doi.org/10.31128/AJGP-09-22-6571
Dorhout Mees, S. M., Van Faals, N. L., & Van Alfen, N. (2020). Backpack palsy and other brachial plexus neuropathies in the military population. Journal of the Peripheral Nervous System, 25(1), 27–31.https://doi.org/10.1111/jns.12363
Upadhyaya, V, & Upadhyaya, DN. (2019). Current status of magnetic resonance neurography in evaluating patients with brachial plexopathy. Neurology India. 67(Supplement), S118–S124. https://doi.org/10.4103/0028-3886.250730
Warade, AC, Jha, AK, Pattankar, S, & Desai, K. (2019). Radiation-induced brachial plexus neuropathy: A review. Neurology India. 67(Supplement), S47–S52. https://doi.org/10.4103/0028-3886.250704
Create your free account or log in to continue reading!