Compartment syndrome is a surgical emergency Surgical Emergency Acute Abdomen usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation Circulation The movement of the blood as it is pumped through the cardiovascular system. ABCDE Assessment and function of the tissues within that space. Long bone fractures Bone fractures Breaks in bones. Bones: Remodeling and Healing are the most common cause, with the leg Leg The lower leg, or just "leg" in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia. Leg: Anatomy and forearm Forearm The forearm is the region of the upper limb between the elbow and the wrist. The term "forearm" is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: Anatomy compartments frequently affected. Patients Patients Individuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures. Clinician–Patient Relationship present with pain Pain An unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons. Pain: Types and Pathways out of proportion to the injury and may also have pallor, pulselessness Pulselessness Cardiac Arrest, paresthesia, poikilothermia Poikilothermia Cold to the touch. Acute Limb Ischemia, and paralysis (the 6 Ps PS Invasive Mechanical Ventilation of compartment syndrome). Diagnosis is clinical but compartment pressure measurement can be used. Management is an emergency fasciotomy. Failure to diagnose and manage the condition results in limb loss.
Last updated: Dec 15, 2025
Compartment syndrome is a condition that occurs when increased pressure in a closed muscle compartment exceeds the pressure to perfuse the compartment, resulting in muscle and nerve ischemia Ischemia A hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation. Ischemic Cell Damage.
The 6 Ps PS Invasive Mechanical Ventilation of compartment syndrome:

Leg compartments: anterior, lateral, superficial posterior, and deep posterior compartments
Image by Lecturio.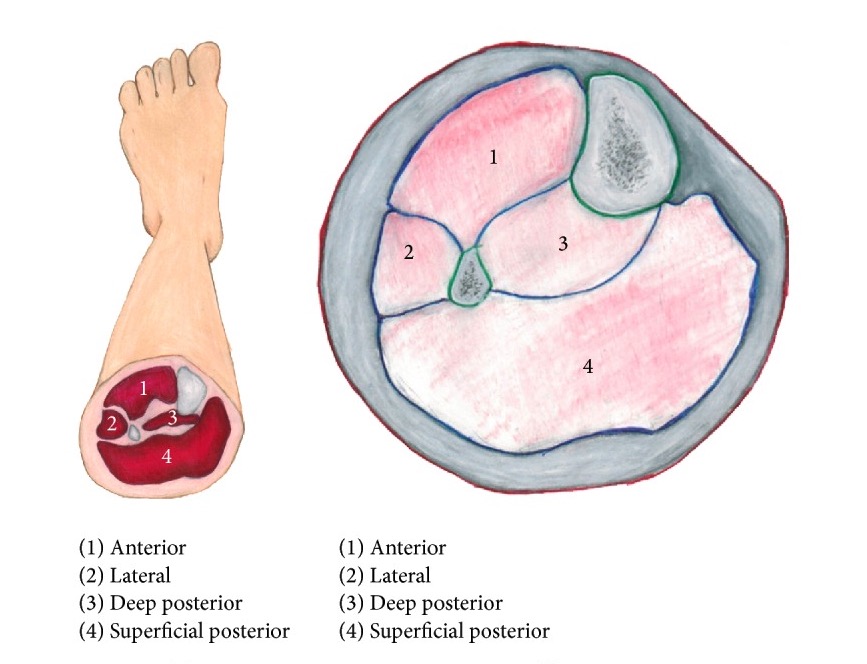
Leg compartments:
Left image: left leg showing locations of the compartments
Right image: larger view of the compartments
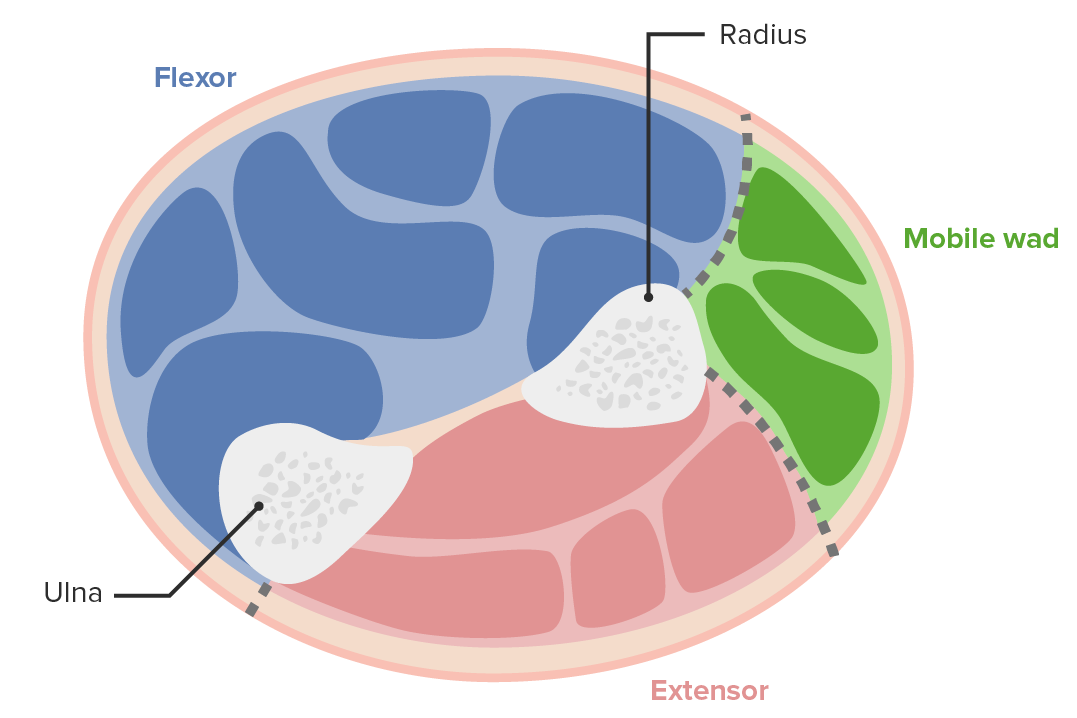
Forearm compartments: The anterior or volar compartment (contains flexor muscles) has superficial and deep components. The posterior compartment contains extensor muscles. The lateral part contains the mobile wad (brachioradialis, extensor carpi radialis brevis, and extensor carpi radialis longus).
Image by Lecturio.
Acute compartment syndrome of the forearm: Compartment syndrome occurred on the forearm of this patient secondary to intravenous (IV) infiltration with pressure from the patient identification (ID) bracelet.
* IV line site
** ID bracelet site
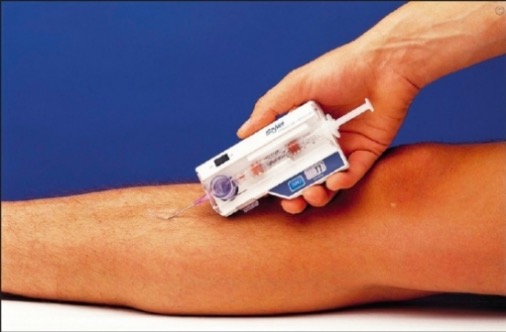
Pressure monitor
A stryker pressure monitor being used for direct compartment pressure measurement of the leg

Compartment syndrome management
Compartment syndrome occurs when the pressure within the muscle compartment increases to a level that compromises the circulation and function of the tissues. Fasciotomy is performed to decompress the involved compartments. In this image, a long incision is made in the fascia of both compartments of the lower leg to release the pressure.