Basic surgical intervention in the thoracic cavity has the primary goal of alleviating any malady that mechanically affects the function of the heart and lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy, which can be secondary to underlying pathologies or, most commonly, trauma. Interventions such as tube thoracostomyThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Hemothorax and thoracentesis are performed to evacuate fluid, blood, or air that is occupying the thoracic cavity in order to restore thoracic negative pressure. When direct intervention to the heart and mediastinumMediastinumThe mediastinum is the thoracic area between the 2 pleural cavities. The mediastinum contains vital structures of the circulatory, respiratory, digestive, and nervous systems including the heart and esophagus, and major thoracic vessels.Mediastinum and Great Vessels: Anatomy is required, an emergency thoracotomy is performed. Once the immediate mechanical problems are addressed, more advanced reparative surgery involving heart, lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy, or mediastinal structures can then be performed as necessary.
It is important to review the anatomy of the chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy in order to more easily avoid the important vascular and nervous components as well as to locate the appropriate entry points during surgical interventions.
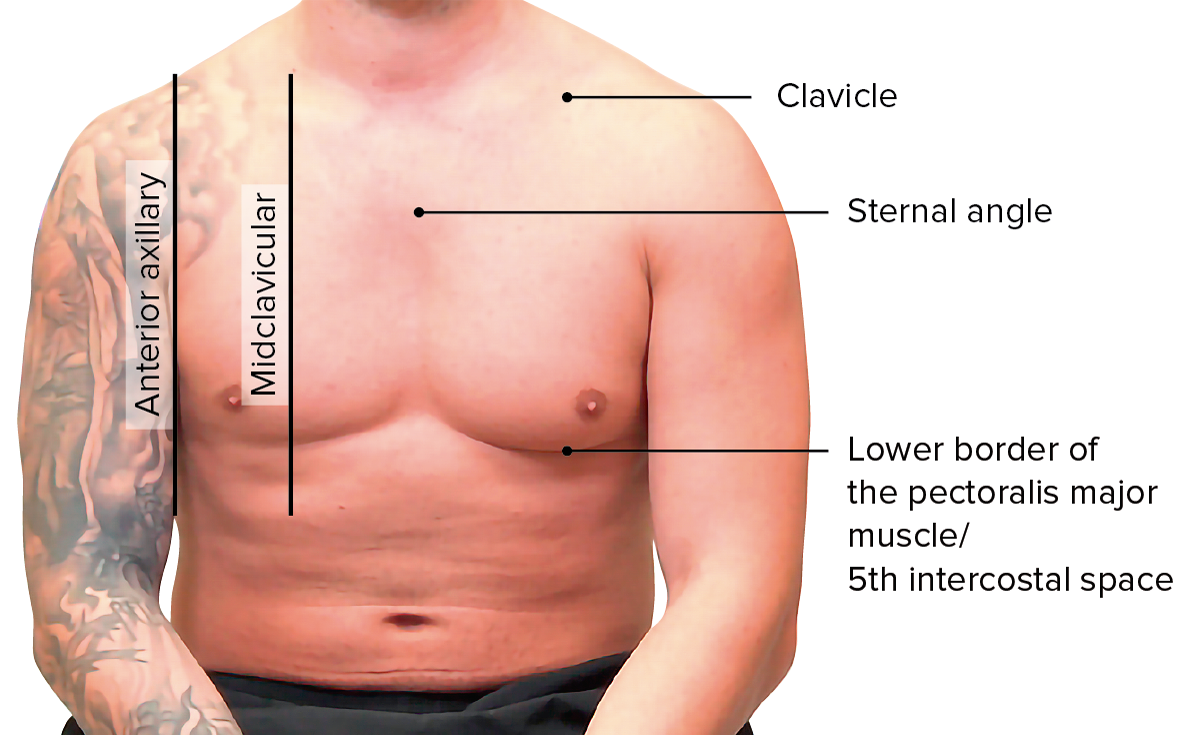
Surface anatomy landmarks
ClavicleClavicleA bone on the ventral side of the shoulder girdle, which in humans is commonly called the collar bone.Clavicle Fracture
Lower border of the pectoralis major muscle/inframammary fold (5th intercostal space)
Surface anatomy landmarks of the thorax to keep in mind for chest tube placement
Image by Lecturio.
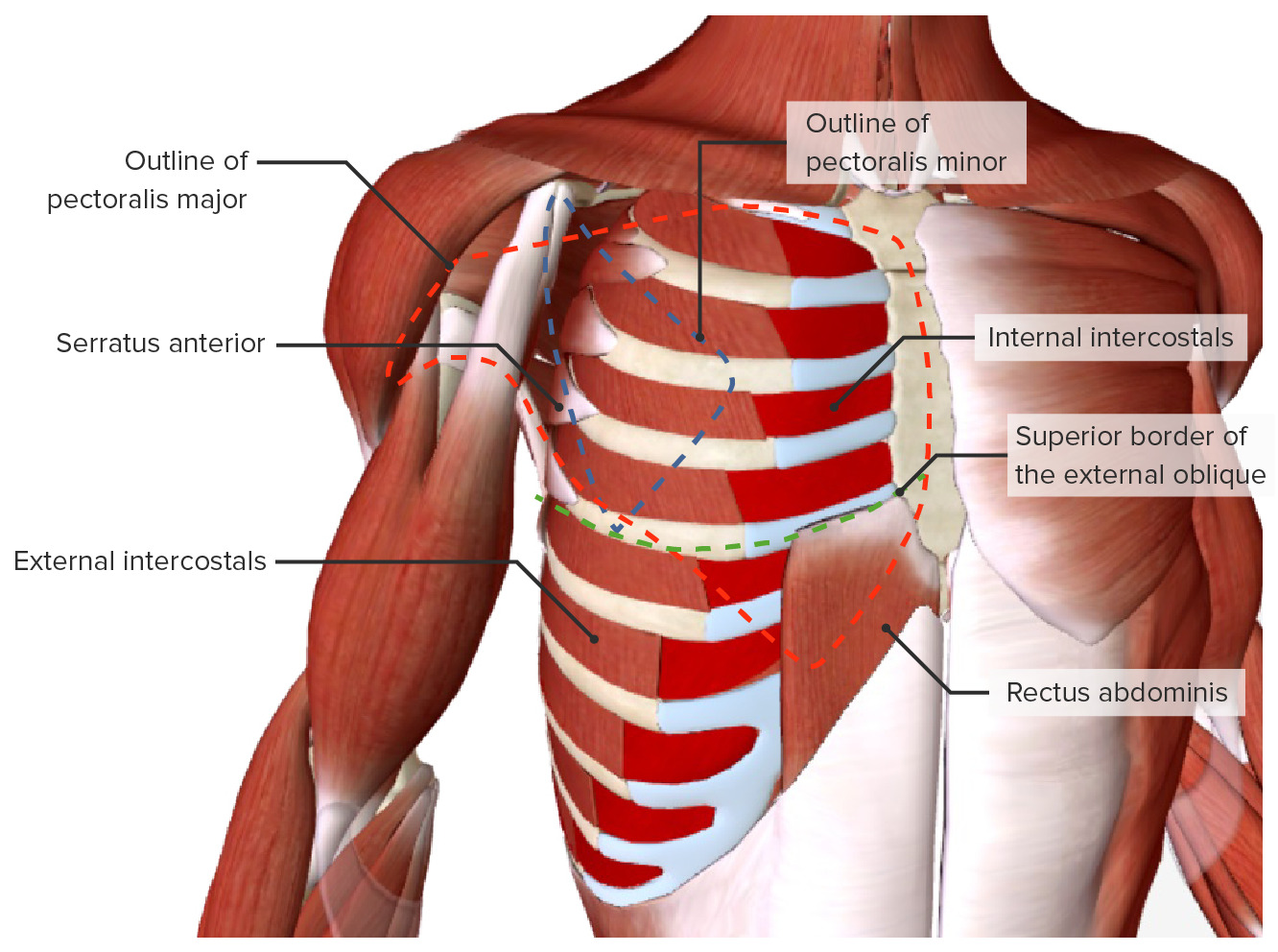
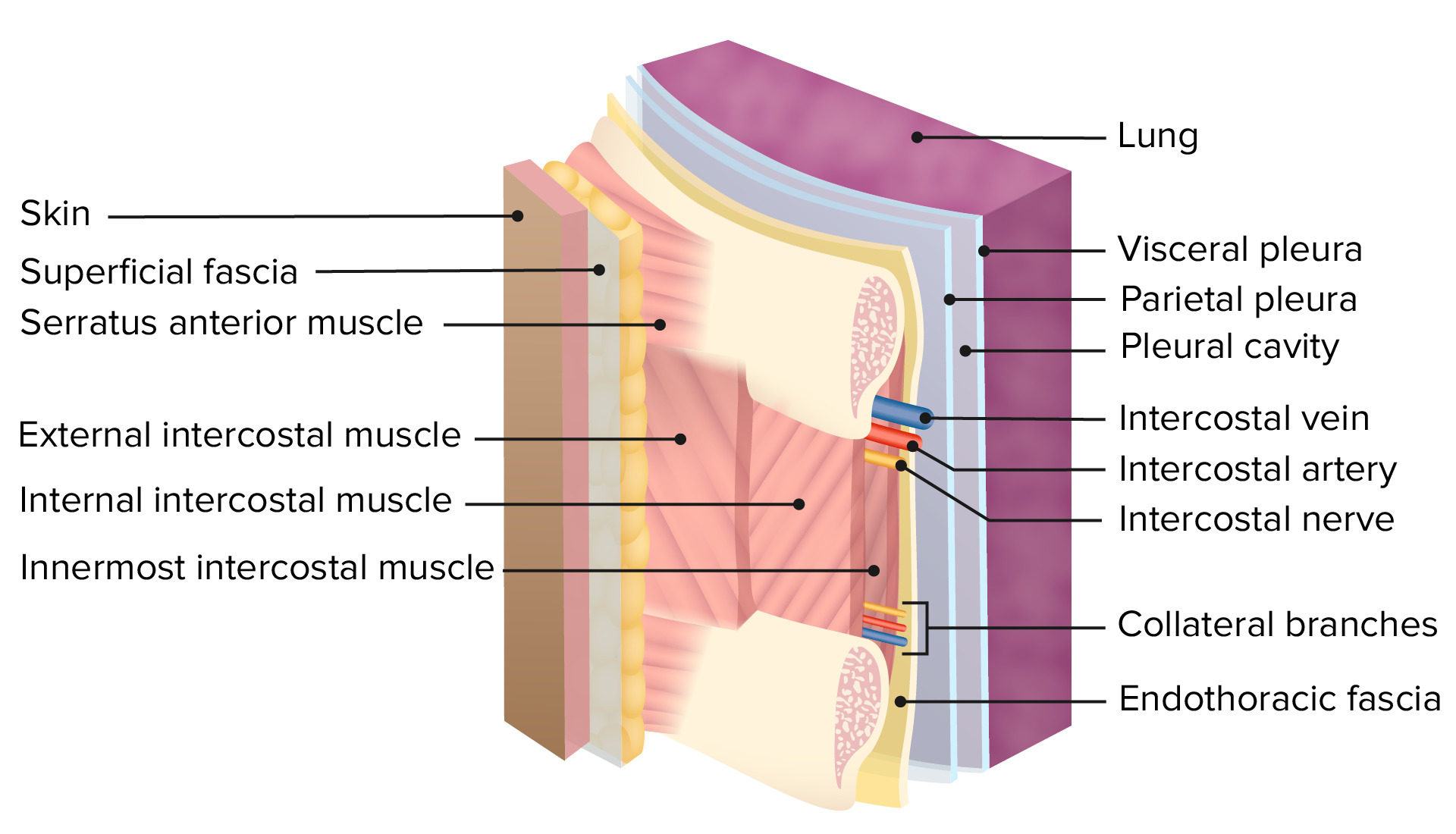
Layers of the chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
Subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess
Intercostal musclesIntercostal MusclesRespiratory muscles that arise from the lower border of one rib and insert into the upper border of the adjoining rib, and contract during inspiration or respiration.Chest Wall: Anatomy:
Neurovasculature of the chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy
Blood supply:
Intercostal arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology: branches of the aortaAortaThe main trunk of the systemic arteries.Mediastinum and Great Vessels: Anatomy and internal mammary artery that anastomose
Internal mammary artery
Venous drainage:
Intercostal veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology
Chest tube placementChest tube placementSurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Pleural Effusion, or tube thoracostomyThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Hemothorax, is an invasive procedure that consists of inserting a large-bore tube into the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy to provide continuous drainage of pleural fluid and/or air.
Indications
PneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Hemopneumothorax
Thoracic empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation
There are no contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation for the placement of a chest tube. However, insertion must be done with caution in the following cases:
Underlying coagulopathy or low platelet count
Antiplatelet therapy and anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants
Procedure
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests has to be carefully reviewed to determine the best approach and location.
Patient can be placed in the supine or in the lateral decubitus position.
The armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy is placed over or behind the head.
The site of insertion is usually at the anterior axillary line in the 4th or 5th intercostal space, but can be adjusted:
Can be placed more posteriorly for pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
A more precise localization with radiologic guidance may be required for complex loculated air or fluid collections.
A 2-cm incision is made in the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.
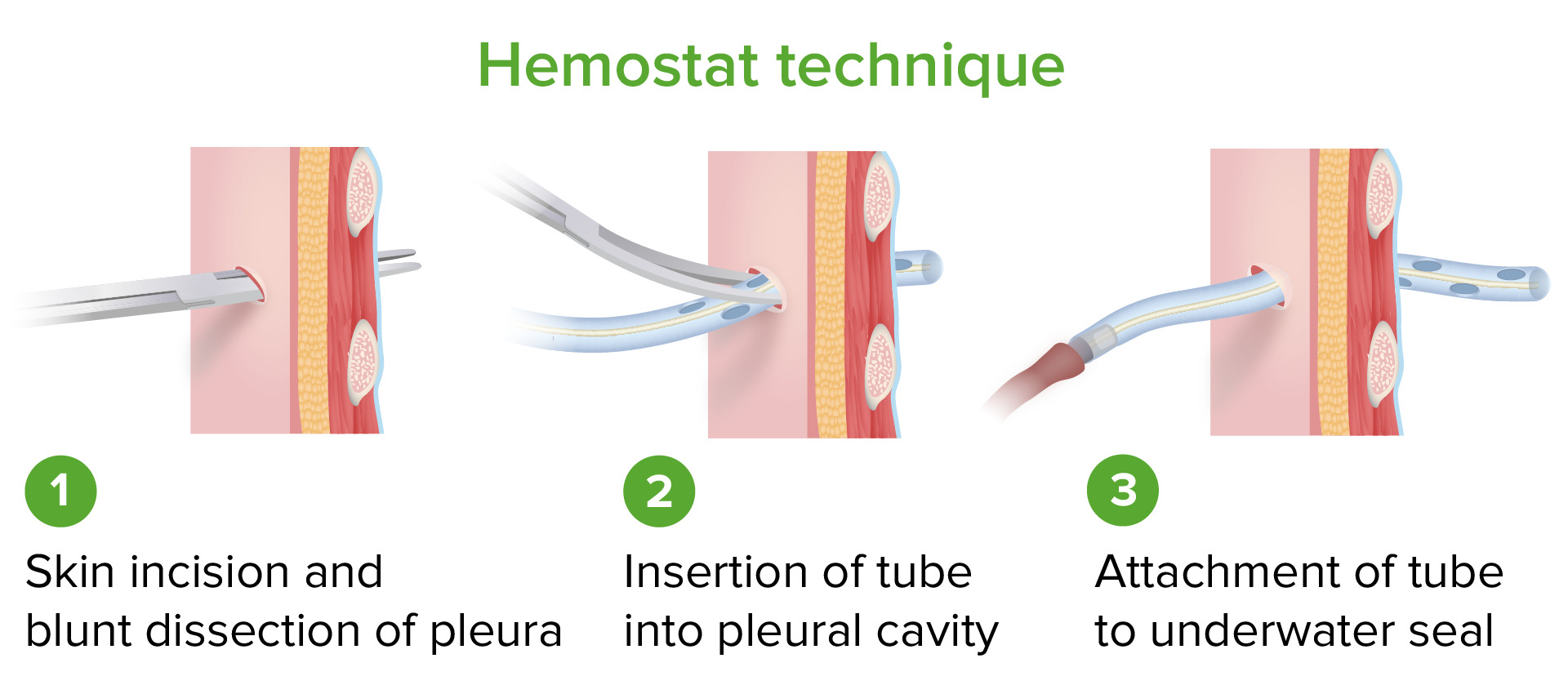
A Kelly clamp is used to make a tunnel through the incision and intercostal musclesIntercostal MusclesRespiratory muscles that arise from the lower border of one rib and insert into the upper border of the adjoining rib, and contract during inspiration or respiration.Chest Wall: Anatomy into the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy.
A finger is used to make sure the lung is away from the incision site.
The chest tube is inserted starting from its perforated end in a superior–posterior–medial direction. This step can be aided with a Kelly clamp.
The tube is connected to a drainage system (Pleur-Evac) and secured to the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions with a purse-string suture.
A chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is obtained to ensure adequate placement.
Steps of the hemostat technique for chest tube placement
Image by Lecturio.
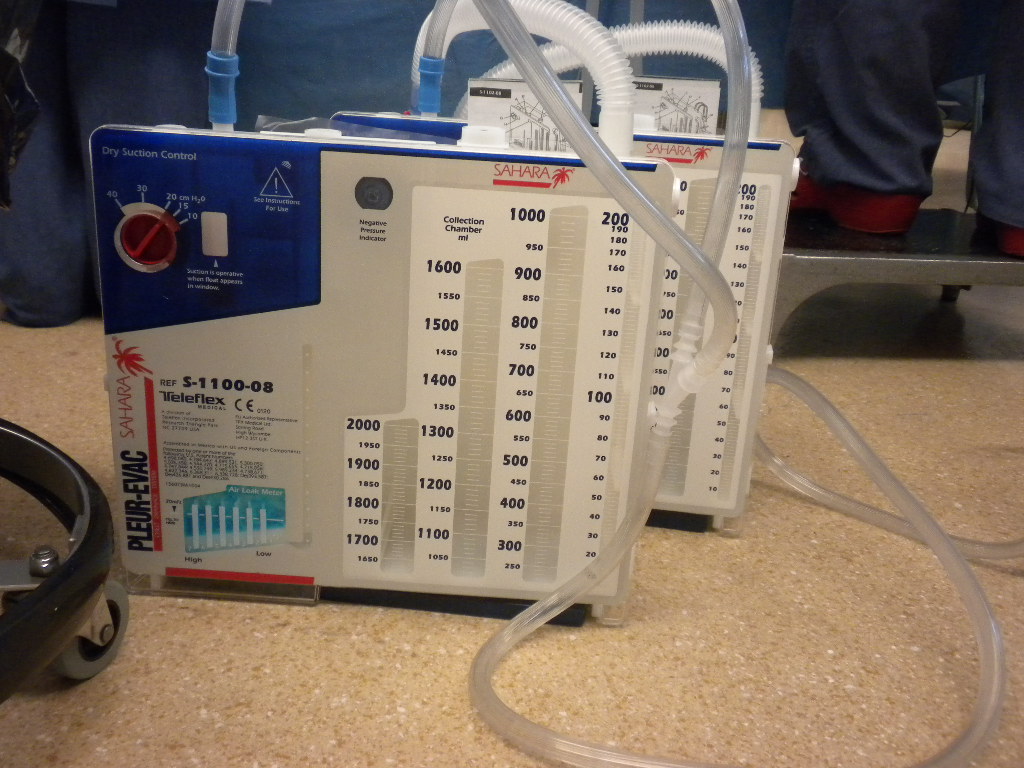
Chest tube suction apparatus (Pleur-Evac)
Image: “Drainage Canisters – Pleur-Evac Sahara” by Bentplate84. License: CC BY-SA 3.0
Complications
Injury to the lung parenchyma: can present as a persistent air leak
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis of the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy and/or abdominal viscera:
If the insertion site is too low
Can result in liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy (on the right) or spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy (on the left) injury with intra-abdominal hemorrhage
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis of the heart:
From left tube thoracostomyThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Hemothorax
Will get rapid blood return in tube
Injury to the intercostal vessels:
Can happen if the chest tube is inserted close to the lower costal margin, where intercostal vessels lie
Can present as intrathoracic and/or insertion site bleeding
Reexpansion pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema:
Rare
Can happen if a large pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion (> 1.5 L) is evacuated too quickly
Presents as acute onset of respiratory distress/cough/frothy sputum
Thoracentesis
Definition
Thoracentesis is an invasive procedure that consists of inserting a catheter into the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis to evacuate pleural fluid for diagnostic and/or therapeutic reasons.
Indications
Thoracentesis may be required in any condition that presents with pleural effusions that compromise breathing, such as:
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
EmpyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
AtelectasisAtelectasisAtelectasis is the partial or complete collapse of a part of the lung. Atelectasis is almost always a secondary phenomenon from conditions causing bronchial obstruction, external compression, surfactant deficiency, or scarring. Atelectasis
Pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism
Hepatic hydrothoraxHydrothoraxA collection of watery fluid in the pleural cavity.Edema
HypoalbuminemiaHypoalbuminemiaA condition in which albumin level in blood (serum albumin) is below the normal range. Hypoalbuminemia may be due to decreased hepatic albumin synthesis, increased albumin catabolism, altered albumin distribution, or albumin loss through the urine (albuminuria).Nephrotic Syndrome in Children
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
UremiaUremiaA clinical syndrome associated with the retention of renal waste products or uremic toxins in the blood. It is usually the result of renal insufficiency. Most uremic toxins are end products of protein or nitrogen catabolism, such as urea or creatinine. Severe uremia can lead to multiple organ dysfunctions with a constellation of symptoms.Acute Kidney Injury
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation
There are no absolute contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to thoracentesis. However, caution is advised with the following:
Coagulopathy
Use of antiplatelet agentsAntiplatelet agentsAntiplatelet agents are medications that inhibit platelet aggregation, a critical step in the formation of the initial platelet plug. Abnormal, or inappropriate, platelet aggregation is a key step in the pathophysiology of arterial ischemic events. The primary categories of antiplatelet agents include aspirin, ADP inhibitors, phosphodiesterase/adenosine uptake inhibitors, and glycoprotein IIb/IIIa inhibitors. Antiplatelet Drugs and anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants
Recent surgery on the ipsilateral thoracic cavity
Metastatic cancer
Factors predictive of difficult thoracentesis:
Use of positive-pressure ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing (i.e., mechanical, continuous positive airwayAirwayABCDE Assessment pressure (CPAPCPAPA technique of respiratory therapy, in either spontaneously breathing or mechanically ventilated patients, in which airway pressure is maintained above atmospheric pressure throughout the respiratory cycle by pressurization of the ventilatory circuit.Noninvasive Ventilation))
Chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: AnatomycellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis
Loculated pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
Procedure
Preoperative preparation:
Perform a full physical examination with special emphasis on chest percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination.
Preprocedure images need to be carefully reviewed:
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
Chest CT scan
Withhold anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants before the procedure.
The patient should be sitting, leaning forward, and resting the elbows on a table. In patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are not able to sit up, the head of the bed is elevated 30 degrees.
Ultrasonography can be performed to guide the procedure.
When ultrasonography is not available, one of the following sites is located and marked:
5th–7th intercostal space in the posterior scapular line
Dullness to percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination indicates a site of greater fluid accumulation, ideal for puncture.
A 22-gauge needle is used to enter the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis while applying negative pressure.
Entrance is confirmed by the aspiration of free-flowing fluid.
Bubbles in the syringe may indicate lung puncture.
A thoracentesis needle catheter is prepared, including a 3-way stopcock, syringe, and tube leading to a collection bag.
The thoracentesis needle catheter is inserted into the superior margin of the lower rib while maintaining negative pressure.
An initial 30–60 mL of fluid is collected for laboratory analysis (e.g., Gram stainGram stainKlebsiella, culture, chemistry, cell count).
The remaining fluid is drained into the collecting bag until 1 of the following occurs:
Fluid stops draining spontaneously.
The patient starts coughing or reports chest discomfort.
A total of 1–1.5 L of fluid is drained.
When drainage is complete, the patient is instructed to hold their breath and then exhale while the catheter is withdrawn.
Postprocedure chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is obtained to rule out pneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax.
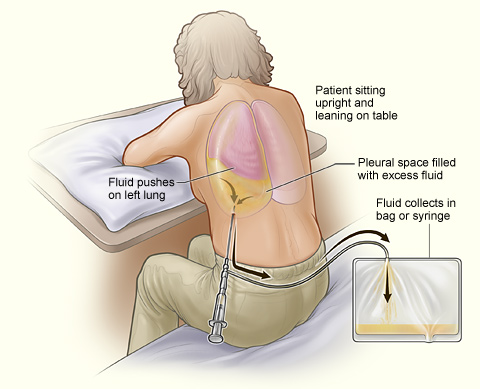
Thoracentesis on a left hemithorax
Image: “Thoracentesis” by National Heart, Lung and Blood Institute. License: Public Domain
Complications
Reexpansion pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema
PneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception at the injection site
Intra-abdominal puncture, with liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy or spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy injury
Pleural infection and empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia
Pleural fluid analysis
Transudative effusions (caused by changes in hydrostatic or oncotic pressureOncotic PressureEdema or pleural permeability):
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: AnatomycirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
Severe hypoalbuminemiaHypoalbuminemiaA condition in which albumin level in blood (serum albumin) is below the normal range. Hypoalbuminemia may be due to decreased hepatic albumin synthesis, increased albumin catabolism, altered albumin distribution, or albumin loss through the urine (albuminuria).Nephrotic Syndrome in Children
Nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome
Exudative effusions (altered formation and absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of pleural fluid):
Infection (e.g., empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia due to bacterial pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
Trauma
Pulmonary infarction
Pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism
Light’s criteria (for diagnosis of exudative effusions):
Pleural fluid LDHLDHOsteosarcoma > 2⁄3 the normal upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation for serum
Other findings associated with exudative effusions:
Color/appearance:purulent, bloody, milky, black, presence of particles
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance < 3.4 mmol/L
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance < 7.3
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption > 110 U/L
Emergency, or resuscitative, thoracotomy is an invasive procedure that consists of making a large incision in the left hemithorax to attain access to the heart and other mediastinal structures, including the thoracic aortaAortaThe main trunk of the systemic arteries.Mediastinum and Great Vessels: Anatomy, to control bleeding and quickly repair life-threatening injuries.
Therapeutic goals
ResuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome of agonic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with penetrating cardiothoracic injuries
Evacuation of cardiac tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis (especially in penetrating trauma)
Direct cardiac massage
Direct repair of cardiac injuries
Control of massive intrathoracic hemorrhage
Clamping of the descending thoracic aortaAortaThe main trunk of the systemic arteries.Mediastinum and Great Vessels: Anatomy for maintenance of perfusion to the heart and brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Prevention of air embolismAir embolismBlocking of a blood vessel by air bubbles that enter the circulatory system, usually after trauma; surgical procedures, or changes in atmospheric pressure.Nonthrombotic Embolism
Indications
Cardiac arrestCardiac arrestCardiac arrest is the sudden, complete cessation of cardiac output with hemodynamic collapse. Patients present as pulseless, unresponsive, and apneic. Rhythms associated with cardiac arrest are ventricular fibrillation/tachycardia, asystole, or pulseless electrical activity. Cardiac Arrest following penetrating or blunt chest traumaBlunt chest traumaBlunt chest trauma is a non-penetrating traumatic injury to the thoracic cavity. Thoracic traumatic injuries are classified according to the mechanism of injury as blunt or penetrating injuries. Different structures can be injured including the chest wall (ribs, sternum), lungs, heart, major blood vessels, and the esophagus.Blunt Chest Trauma with signs of life
Cardiac tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis with profound shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock in a patient who is unresponsive to volume expansion and unlikely to survive until proper surgery can be performed
Blunt or penetrating trauma to the chest or abdomen with profound shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock in a patient who is unresponsive to volume expansion and unlikely to survive until proper surgery can be performed
Massive chest or abdominal bleedingAbdominal BleedingPenetrating Abdominal Injury with profound shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock (> 1500 mL of blood obtained via chest tube)
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation
Traumatic cardiac arrestTraumatic cardiac arrestA sudden cardiac arrhythmia (e.g., ventricular fibrillation) caused by a blunt, non-penetrating impact to the precordial region of chest wall. Commotio cordis often results in sudden death without prompt cardiopulmonary defibrillation.Blunt Chest Trauma with no signs of life in the prehospital setting (e.g., asystoleAsystoleNo discernible electrical activity, flatline on electrocardiogram (P waves and QRS complexes are not present).Cardiac Arrest, prolonged lack of pulse)
Patient who is immediately responsive to volume expansion or decompression of tension pneumothoraxTension PneumothoraxPneumothorax
Penetrating or blunt thoracic injury with > 15 minutes of CPRCPRThe artificial substitution of heart and lung action as indicated for heart arrest resulting from electric shock, drowning, respiratory arrest, or other causes. The two major components of cardiopulmonary resuscitation are artificial ventilation and closed-chest cardiac massage.Cardiac Arrest and no signs of life
Procedure
Preoperative preparation:
Perform bedside FAST, if available:
Cardiac tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax
Intra-abdominal hemorrhage
The patient should be intubated and ventilated.
The site of the incision is washed with a skin-sterilizing solution and covered with sterileSterileBasic Procedures drapes.
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG)
Technique:
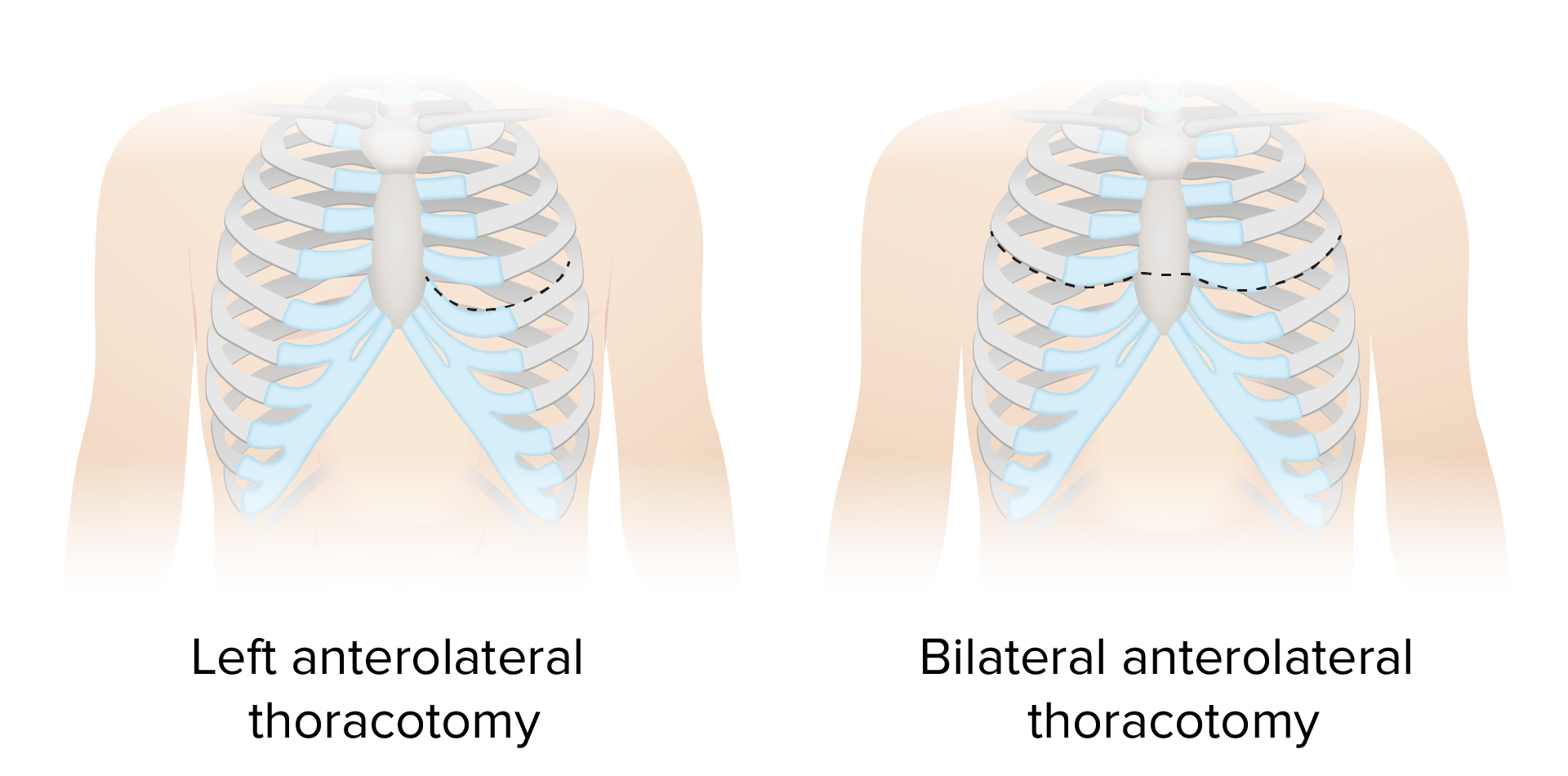
The usual approach in an emergency is through left thoracotomy. Thoracotomy is a last-resort potentially lifesaving procedure that needs to be performed quickly.
The 4th or 5th intercostal space is identified (reference point: the nippleNippleThe conic organs which usually give outlet to milk from the mammary glands.Examination of the Breast in men, the inframammary fold in women).
An incision is made going from the lateral border of the left sternocostal junction to the posterior axillary line (anterolateral thoracotomy), exposing the intercostal musclesIntercostal MusclesRespiratory muscles that arise from the lower border of one rib and insert into the upper border of the adjoining rib, and contract during inspiration or respiration.Chest Wall: Anatomy.
The incision should follow the curvature of the ribsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy.
The inferior border of the superior rib should be avoided to prevent damaging the intercostal neurovascular bundle.
The intercostal musclesIntercostal MusclesRespiratory muscles that arise from the lower border of one rib and insert into the upper border of the adjoining rib, and contract during inspiration or respiration.Chest Wall: Anatomy are transected from the sternumSternumA long, narrow, and flat bone commonly known as breastbone occurring in the midsection of the anterior thoracic segment or chest region, which stabilizes the rib cage and serves as the point of origin for several muscles that move the arms, head, and neck.Chest Wall: Anatomy to the posterior axillary line, to gain access to the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis.
The ribsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy are spread with the fingers in order to insert and be separated further by the rib spreader (Finochietto retractor).
The left lung is displaced superiorly, and the pericardiumPericardiumA conical fibroserous sac surrounding the heart and the roots of the great vessels (aorta; venae cavae; pulmonary artery). Pericardium consists of two sacs: the outer fibrous pericardium and the inner serous pericardium. The latter consists of an outer parietal layer facing the fibrous pericardium, and an inner visceral layer (epicardium) resting next to the heart, and a pericardial cavity between these two layers.Heart: Anatomy is inspected for tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis or lacerations.
To relieve tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis:
The pericardiumPericardiumA conical fibroserous sac surrounding the heart and the roots of the great vessels (aorta; venae cavae; pulmonary artery). Pericardium consists of two sacs: the outer fibrous pericardium and the inner serous pericardium. The latter consists of an outer parietal layer facing the fibrous pericardium, and an inner visceral layer (epicardium) resting next to the heart, and a pericardial cavity between these two layers.Heart: Anatomy is grasped using forcepsForcepsSurgical Instruments and Sutures and opened from the apex toward the base (pericardiotomy).
Clotted blood is manually removed and liquid blood is suctioned.
To perform direct cardiac massage:
With the wrists together, the physician gently compresses the heart in a clapping motion from the apex toward the base.
If ventricular fibrillationVentricular fibrillationVentricular fibrillation (VF or V-fib) is a type of ventricular tachyarrhythmia (> 300/min) often preceded by ventricular tachycardia. In this arrhythmia, the ventricle beats rapidly and sporadically. The ventricular contraction is uncoordinated, leading to a decrease in cardiac output and immediate hemodynamic collapse. Ventricular Fibrillation (V-fib) is felt, defibrillationDefibrillationVentricular Fibrillation (V-fib) with internal paddles is performed.
To control myocardial lacerationLacerationTorn, ragged, mangled wounds.Blunt Chest Trauma: with surgical staples, mattress sutures, or a Foley catheter (a balloon is inflated within the cardiac cavity with normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids)
To clamp the aorta in cases of nonresponse to fluid resuscitation:
The pleuraPleuraThe pleura is a serous membrane that lines the walls of the thoracic cavity and the surface of the lungs. This structure of mesodermal origin covers both lungs, the mediastinum, the thoracic surface of the diaphragm, and the inner part of the thoracic cage. The pleura is divided into a visceral pleura and parietal pleura. Pleura: Anatomy and fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis are dissected to expose the aortaAortaThe main trunk of the systemic arteries.Mediastinum and Great Vessels: Anatomy.
A nasogastric tubeNasogastric tubeMalnutrition in children in resource-limited countries is inserted to identify the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy.
A vascular clamp, aortic compressionCompressionBlunt Chest Trauma device, or the physician’s handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy is used to clamp/put pressure on the aortaAortaThe main trunk of the systemic arteries.Mediastinum and Great Vessels: Anatomy against the spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy.
The rest of the cavity is checked for uncontrolled sources of bleeding and other life-threatening injuries.
If the injury is located on the right hemithorax, the thoracotomy is expanded by transecting the sternumSternumA long, narrow, and flat bone commonly known as breastbone occurring in the midsection of the anterior thoracic segment or chest region, which stabilizes the rib cage and serves as the point of origin for several muscles that move the arms, head, and neck.Chest Wall: Anatomy (clamshell thoracotomy).
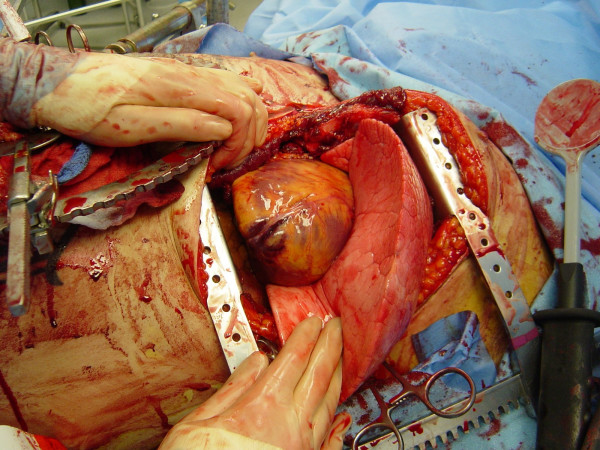
A left emergency thoracotomy performed through the 4th or 5th intercostal space. The heart and left lung are readily visualized. Note the Finochietto retractor and the defibrillation paddle on the right-hand side of the picture.
Image: “Figure 2” by Cothren, C.C., et al. License: CC BY 2.0
Postoperative carePostoperative careAfter any procedure performed in the operating room, all patients must undergo close observation at least in the recovery room. After larger procedures and for patients who require hospitalization, observation must continue on the surgical ward. The primary intent of this practice is the early detection of postoperative complications. Postoperative Care:
It is still under debate whether one should close the chest completely or perform a temporary closure.
Transfer to the OR for definitive management.
After definitive management, transfer to the ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus for continued resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
The most important determinant of survival is the location and magnitude of the injuries.
Reported survival of up to 70% following emergency thoracotomy in penetrating trauma
The survival rate is much poorer for blunt trauma.
Survival is related to the length of CPRCPRThe artificial substitution of heart and lung action as indicated for heart arrest resulting from electric shock, drowning, respiratory arrest, or other causes. The two major components of cardiopulmonary resuscitation are artificial ventilation and closed-chest cardiac massage.Cardiac Arrest, with > 15 minutes equated with poor survival.
Direct cardiac massage may result in better cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics and cerebral perfusionCerebral PerfusionSyncope.
A 5th of survivors suffer significant neurologic injury.
Clinical Relevance
Indicates for tube thoracostomyThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Hemothorax:
PneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax: accumulation of air within the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis between the parietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: Anatomy and visceral pleuraVisceral pleuraPleura: Anatomy, which can be open (with communicationCommunicationThe exchange or transmission of ideas, attitudes, or beliefs between individuals or groups.Decision-making Capacity and Legal Competence to the outside) or under tension (without an opening in the chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy and ongoing air leak from the injured lung parenchyma)
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion: accumulation of fluid within the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis, which can be a transudateTransudateTransudates are fluids that pass through a membrane or squeeze through tissue or into the extracellular space of tissues. Transudates are thin and watery and contain few cells or proteins.Pleural Effusion or an exudateExudateExudates are fluids, cells, or other cellular substances that are slowly discharged from blood vessels usually from inflamed tissues.Pleural Effusion according to Light’s criteria, depending on the result of the cytochemical analysis
HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax: accumulation of blood within the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis due to profuse bleeding, usually seen in the context of trauma to the chest
Hemopneumothorax: accumulation of both blood and air within the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy, also frequently seen in the context of trauma to the chest: The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship must be careful at the time of decompression, since the pressurized air may propel blood through the incision.
Thoracic empyemaEmpyemaPresence of pus in a hollow organ or body cavity.Pneumonia: accumulation of purulent material (pus) within the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy, seen in the context of infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease of the lower respiratory tract (i.e., pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
ChylothoraxChylothoraxThe presence of chyle in the thoracic cavity.Pleural Effusion: accumulation of chyle within the pleural cavityPleural cavityPaired but separate cavity within the thoracic cavity. It consists of the space between the parietal and visceral pleura and normally contains a capillary layer of serous fluid that lubricates the pleural surfaces.Pleura: Anatomy after injury to the thoracic ductThoracic DuctThe largest lymphatic vessel that passes through the chest and drains into the subclavian vein.Lymphatic Drainage System: Anatomy
Indication for thoracentesis:
Pleural effusions: the accumulation of fluid within the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis, which, according to cytochemical analysis (Light’s criteria), can be classified as a transudateTransudateTransudates are fluids that pass through a membrane or squeeze through tissue or into the extracellular space of tissues. Transudates are thin and watery and contain few cells or proteins.Pleural Effusion or exudateExudateExudates are fluids, cells, or other cellular substances that are slowly discharged from blood vessels usually from inflamed tissues.Pleural Effusion
Indication for emergency thoracotomy:
Cardiac tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis: restriction in cardiac filling due to the excessive accumulation of fluid within the pericardial cavityPericardial cavityHeart: Anatomy that leads to decreased cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics and serious systemic consequences (hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension and shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock)
Massive hemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax: drainage of > 1500 mL of blood via tube thoracostomyThoracostomySurgical procedure involving the creation of an opening (stoma) into the chest cavity for drainage; used in the treatment of pleural effusion; pneumothorax; hemothorax; and empyema.Hemothorax or bleeding of > 200 mL per hour for at least 2 hours: HemothoraxHemothoraxA hemothorax is a collection of blood in the pleural cavity. Hemothorax most commonly occurs due to damage to the intercostal arteries or from a lung laceration following chest trauma. Hemothorax can also occur as a complication of disease, or hemothorax may be spontaneous or iatrogenic. Hemothorax itself is the accumulation of blood within the pleural spacePleural spaceThe thin serous membrane enveloping the lungs (lung) and lining the thoracic cavity. Pleura consist of two layers, the inner visceral pleura lying next to the pulmonary parenchyma and the outer parietal pleura. Between the two layers is the pleural cavity which contains a thin film of liquid.Pleuritis.
Massive hemorrhage with witnessed or impending cardiac arrestCardiac arrestCardiac arrest is the sudden, complete cessation of cardiac output with hemodynamic collapse. Patients present as pulseless, unresponsive, and apneic. Rhythms associated with cardiac arrest are ventricular fibrillation/tachycardia, asystole, or pulseless electrical activity. Cardiac Arrest: The descending aortaDescending aortaMediastinum and Great Vessels: Anatomy can be clamped to control the hemorrhage and temporarily restore the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment to the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification and heart. Survival in this situation is rare, and there is significant morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status related to spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy and kidney ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage.
Cothren, C. C., Moore, E. E. (2006). Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World Journal of Emergency Surgery 1(4). https://doi.org/10.1186/1749-7922-1-4
Create your free account or log in to continue reading!