In the context of acute or chronic kidney failure, renal function may diminish to a point at which it is no longer able to adequately support life. When this happens, renal replacement therapy is indicated. Renal replacement therapy refers to dialysis and/or kidney transplantationKidney TransplantationThe transference of a kidney from one human or animal to another.Organ Transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment. HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome and peritoneal dialysis (PDPDParkinson's disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome versus inside the body for PDPDParkinson's disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease).
Dialysis is a form of renal replacement therapy (RRT) that is used to perform the blood-filtering role of the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy when the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy are not functioning.
The conditions generally include:
AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury
CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
Types:
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome
Peritoneal dialysis
Indications for dialysis in acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury
Acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury is sometimes so severe that dialysis is needed as a life-support measure while waiting for possible renal recovery.
Dialysis is a temporizing measure that is used with the hope that the patient will recover enough renal function to allow dialysis to be discontinued permanently.
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury do not recover renal function and require long-term RRT.
Indications:
Signs of uremiaUremiaA clinical syndrome associated with the retention of renal waste products or uremic toxins in the blood. It is usually the result of renal insufficiency. Most uremic toxins are end products of protein or nitrogen catabolism, such as urea or creatinine. Severe uremia can lead to multiple organ dysfunctions with a constellation of symptoms.Acute Kidney Injury
Severe hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Severe metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
LithiumLithiumAn element in the alkali metals family. It has the atomic symbol li, atomic number 3, and atomic weight [6. 938; 6. 997]. Salts of lithium are used in treating bipolar disorder.Ebstein’s Anomaly
Toxic alcohols (ethylene glycolEthylene glycolA colorless, odorless, viscous dihydroxy alcohol. It has a sweet taste, but is poisonous if ingested. Ethylene glycol is the most important glycol commercially available and is manufactured on a large scale in the United States. It is used as an antifreeze and coolant, in hydraulic fluids, and in the manufacture of low-freezing dynamites and resins.Nephrolithiasis, methanolMethanolA colorless, flammable liquid used in the manufacture of formaldehyde and acetic acid, in chemical synthesis, antifreeze, and as a solvent. Ingestion of methanol is toxic and may cause blindness.Metabolic Acidosis)
Indications for dialysis in chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
Chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease is often progressive, such that patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will reach end-stage renal disease (ESRD) and then require dialysis or kidney transplantationKidney TransplantationThe transference of a kidney from one human or animal to another.Organ Transplantation.
The decision to start chronic dialysis is individualized based on uremic symptoms and lab results.
Consensus statements from Kidney Disease: Improving Global Outcomes (KDIGO) and Kidney Disease Outcomes QualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement Initiative (KDOQI) help guide these decisions, considering the following factors:
GFRGFRThe volume of water filtered out of plasma through glomerular capillary walls into Bowman’s capsules per unit of time. It is considered to be equivalent to inulin clearance.Kidney Function Tests < 15 mL/min
SerositisSerositisInflammation of a serous membrane.Systemic Lupus Erythematosus (pericarditisPericarditisPericarditis is an inflammation of the pericardium, often with fluid accumulation. It can be caused by infection (often viral), myocardial infarction, drugs, malignancies, metabolic disorders, autoimmune disorders, or trauma. Acute, subacute, and chronic forms exist. Pericarditis/pleuritisPleuritisPleuritis, also known as pleurisy, is an inflammation of the visceral and parietal layers of the pleural membranes of the lungs. The condition can be primary or secondary and results in sudden, sharp, and intense chest pain on inhalation and exhalation.Pleuritis)
Electrolyte abnormalities (primarily hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia) that are uncontrollable with medications
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension that is uncontrollable with medications
Principles
Dialysis, which depends on the principles of diffusion and ultrafiltration through a semipermeable membrane, can be administered through two distinct mechanisms:
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome: The semipermeable membrane is the synthetic dialysis filter.
Peritoneal dialysis (PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease): The semipermeable membrane is the patient’s peritoneal membrane.
Definitions:
Semipermeable membrane:
A membrane that is permeable to some, but not all, solutes
Permeability may be determined by size and/or charge of the solutes.
Necessary for the concept of concentration gradients
Diffusion: movement of solutes across a semipermeable membrane from areas of high concentration to areas of low concentration
Ultrafiltration:
Movement of water across a semipermeable membrane
In dialysis, this occurs with water moving from a place of higher pressure (the blood) to a place of lower pressure (the dialysate).
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome is a procedure by which waste products and excess water are removed from a patient’s blood. This is done by directly removing blood from the patient’s circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment, passing it through the dialysis filter, and then returning it directly back into the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment. Apparatus needed:
Dialyzer or dialysis filter
Dialysate (dialysis solution)
Tubing for transport of blood and dialysate
Machine that powers and monitors the filtration
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome access
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome cannot be performed without an adequately functioning access point.
Permanent access points (i.e., arteriovenous fistulaArteriovenous fistulaAn abnormal direct communication between an artery and a vein without passing through the capillaries. An a-v fistula usually leads to the formation of a dilated sac-like connection, arteriovenous aneurysm. The locations and size of the shunts determine the degree of effects on the cardiovascular functions such as blood pressure and heart rate.Vascular Surgery)
Large bore (usually 11–13 French) allows for the faster flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure rates needed for dialysis.
Can be nontunneled or tunneled (underneath the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions)
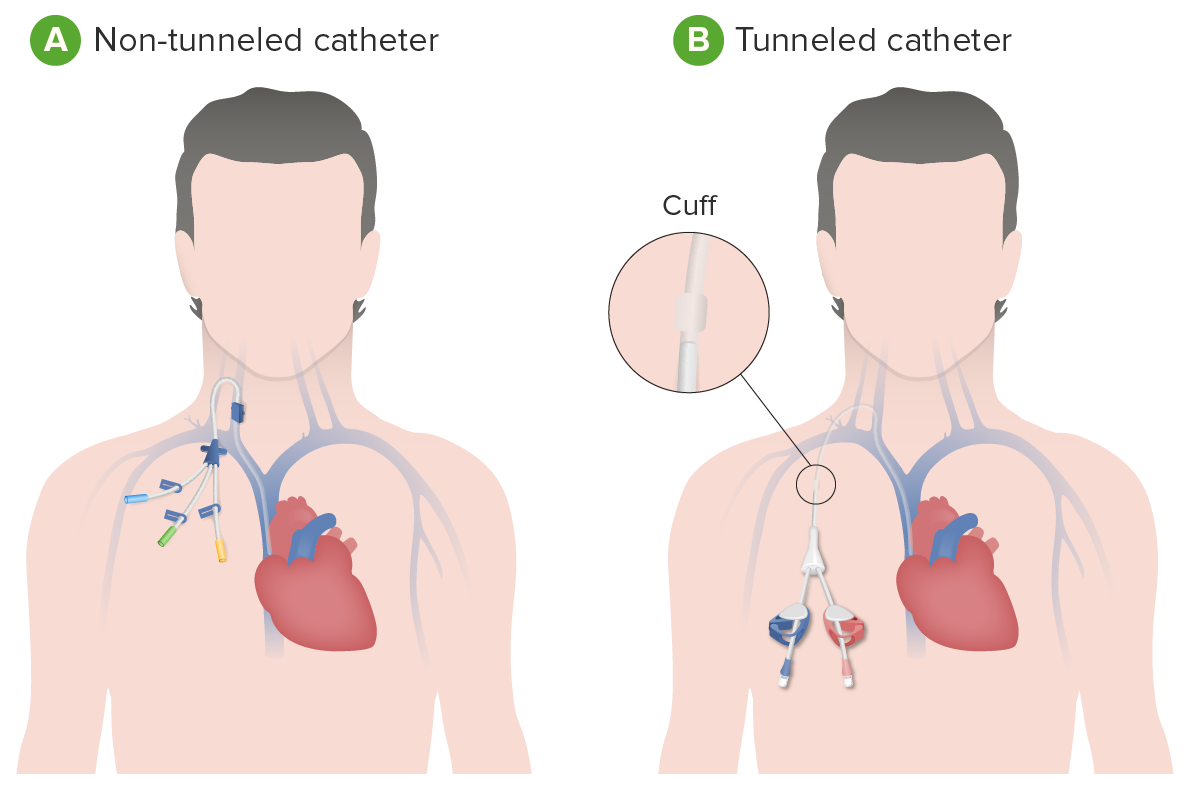
Nontunneled dialysis catheters:
Commonly referred to as “Quinton catheters” or “temporary dialysis catheters”
Most commonly placed in hospital settings for AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury
Secured to the patient only with sutures and surgical dressing
Intended to stay in place for only a period of days:
High risk of infection over time
Significant bleeding risk if inadvertently dislodged
Patient may not be discharged from the hospital with this type of catheter.
Tunneled dialysis catheters (TDC):
Also known as “Hickman catheters” or “permacaths”
Notconsidered permanent access
Used for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who need chronic dialysis started urgently (serving as a “bridge”), but do not yet have a permanent access (i.e., arteriovenous fistulaArteriovenous fistulaAn abnormal direct communication between an artery and a vein without passing through the capillaries. An a-v fistula usually leads to the formation of a dilated sac-like connection, arteriovenous aneurysm. The locations and size of the shunts determine the degree of effects on the cardiovascular functions such as blood pressure and heart rate.Vascular Surgery)
Catheter is tunneled subcutaneously and exits the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions underneath the clavicleClavicleA bone on the ventral side of the shoulder girdle, which in humans is commonly called the collar bone.Clavicle Fracture.
Secured to patient via a “cuff”:
Synthetic material around the part of the catheter that rests underneath the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions near the exit site
FibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans develops around the cuff and surrounding subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess, holding the catheter in place and serving as a barrier to infection.
May be left in place for a period of several weeks.
Patient may be discharged from the hospital with this type of catheter.
Less risk for infection as compared with nontunneled catheters
Overall risk for infection is still significant, particularly if left in place for long periods.
Removed once permanent dialysis access is functional
Central venous catheters for dialysis: A: Nontunneled dialysis catheter B: Tunneled (underneath the skin) dialysis catheter
Image by Lecturio.
Permanent access
Permanent dialysis access points allow dialysis for the long term (i.e., years) and include arteriovenous fistulas (AVFs) and arteriovenous grafts (AVGs).
Arteriovenous fistulaArteriovenous fistulaAn abnormal direct communication between an artery and a vein without passing through the capillaries. An a-v fistula usually leads to the formation of a dilated sac-like connection, arteriovenous aneurysm. The locations and size of the shunts determine the degree of effects on the cardiovascular functions such as blood pressure and heart rate.Vascular Surgery:
Ideal type of access for chronic hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome:
Least risk of infection
Longest lasting
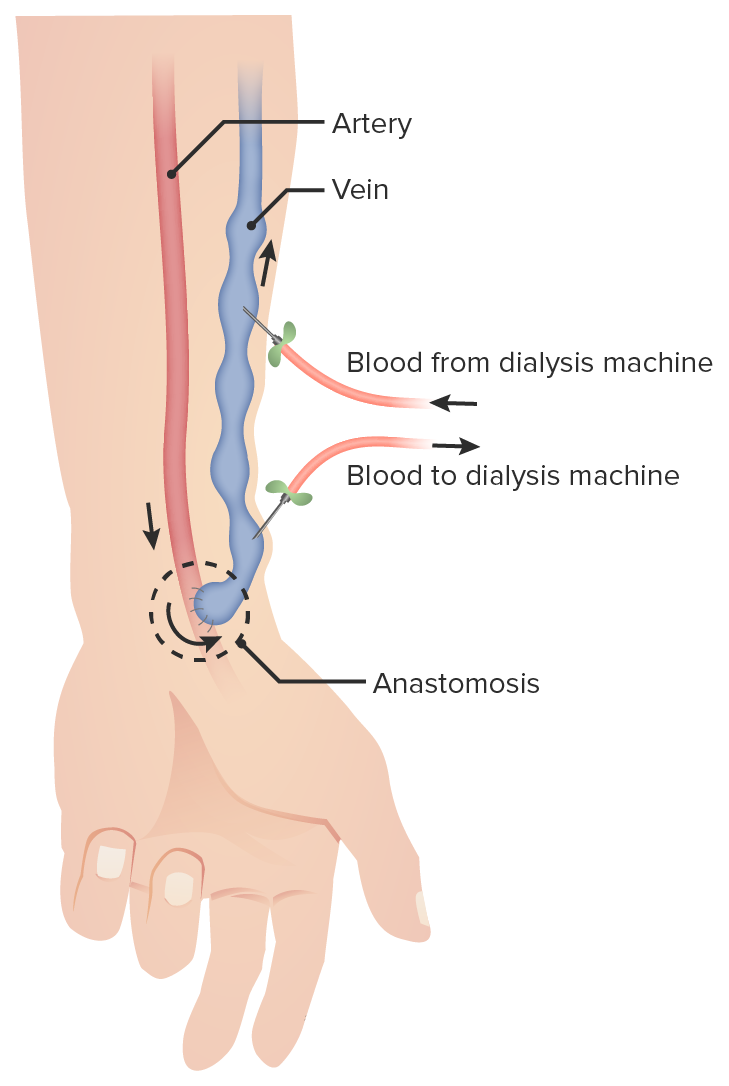
Direct surgical connection (i.e., anastomosis) of an artery and a vein, most commonly:
Radial arteryRadial ArteryThe direct continuation of the brachial trunk, originating at the bifurcation of the brachial artery opposite the neck of the radius. Its branches may be divided into three groups corresponding to the three regions in which the vessel is situated, the forearm, wrist, and hand.Forearm: Anatomy to cephalic vein
Brachial arteryBrachial ArteryThe continuation of the axillary artery; it branches into the radial and ulnar arteries.Cubital Fossa: Anatomy to cephalic vein
High pressure from the artery is transmitted directly into the vein, instead of being dispersed throughout a capillary bed.
Results in vein changing anatomically (i.e., thickening, or “arterializing”) to resemble an artery, which takes weeks to occur
This process is known as “maturation” of the fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula; AVF cannot be used during this period.
Necessary because normal veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology will either collapse or blow out under the high fluid flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure rates needed for dialysis
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with multiple failed AVFs and no other locations available for AVF
Better for chronic dialysis than TDC, but not as good as AVF
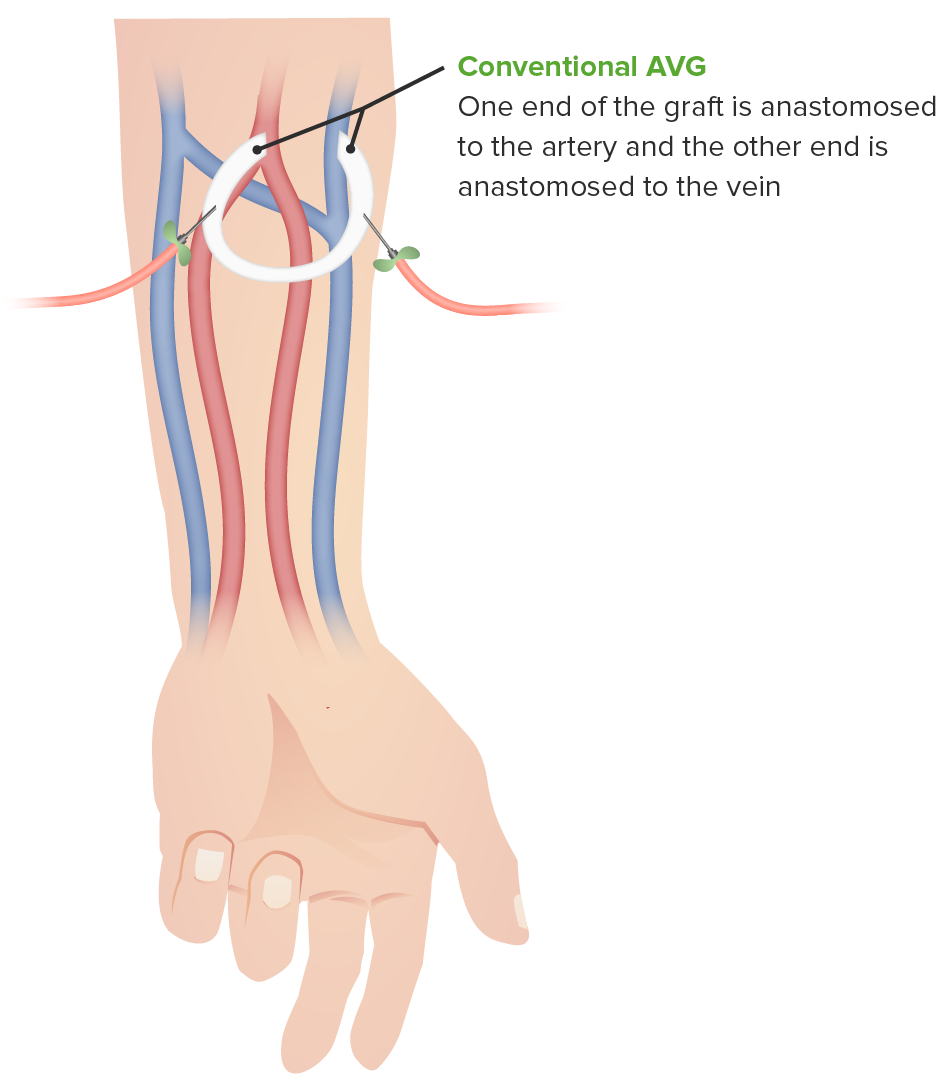
Indirect surgical connection of an artery and vein using a tube of prosthetic material
Many possible locations: forearmForearmThe forearm is the region of the upper limb between the elbow and the wrist. The term “forearm” is used in anatomy to distinguish this area from the arm, a term that is commonly used to describe the entire upper limb. The forearm consists of 2 long bones (the radius and the ulna), the interosseous membrane, and multiple arteries, nerves, and muscles. Forearm: Anatomy, upper armUpper ArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy, chest, thighThighThe thigh is the region of the lower limb found between the hip and the knee joint. There is a single bone in the thigh called the femur, which is surrounded by large muscles grouped into 3 fascial compartments. Thigh: Anatomy
Advantages compared with AVF:
Much shorter maturation period (can hypothetically be used immediately, though usually wait approximately 2 weeks before initial use)
Dialysis needles are placed directly into the synthetic graftGraftA piece of living tissue that is surgically transplantedOrgan Transplantation material.
Can be placed in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are poor candidates for AVF
Can be placed in more anatomic locations than AVFs (i.e., chest)
Disadvantages compared with AVF:
Higher risk of infection owing to synthetic material residing inside the body
Higher risk of clotting
Arteriovenous graft (AVG)
Image by Lecturio.
Arteriovenous fistula: direct surgical connection (i.e., anastomosis) of an artery and a vein
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome procedure
Two sets of tubing are connected to the patient’s dialysis access:
Connected directly to central venous catheterCentral Venous CatheterCentral venous catheters are IV lines placed into the large central veins for monitoring of central venous pressure (CVP), prolonged drug administration, or administration of parenteral nutrition. The most common sites of insertion are the internal jugular and subclavian veins. Central Venous Catheter
Two needles inserted into AVF/AVG and taped down
Azotemic blood pumped from patient into dialysis filter
Dialysis filter removes toxins primarily through diffusion:
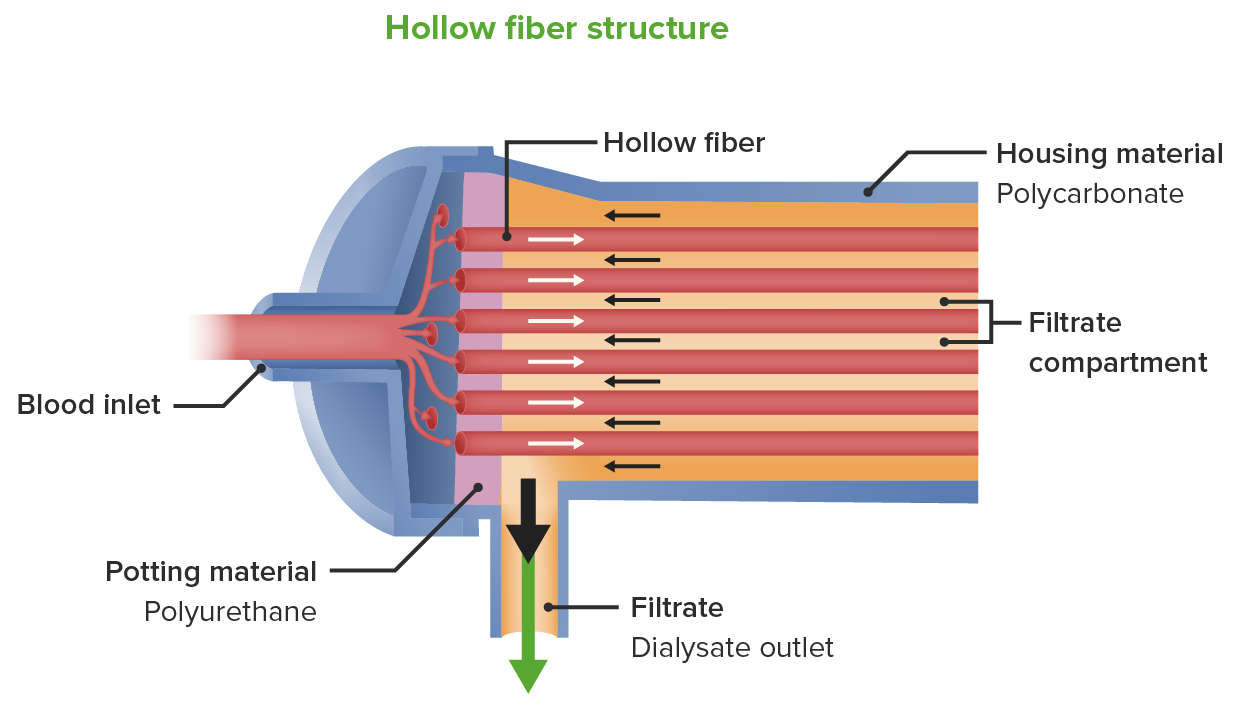
Dialysis filter is a plastic cylinder filled with thousands of tiny individual tubes composed of the filtering material.
Blood flows through the inside of the tiny tubes in one direction.
Dialysis fluid (dialysate) flows on the outside of the tiny tubes (but still within the single plastic cylinder that contains them) in the opposite direction.
The opposing directions of blood and dialysate result in maximal concentration gradients that drive the diffusion of toxins:
Known as “countercurrent” mechanism
Also results in correction of electrolyte/acid–base abnormalities via diffusion
Dialysis filter removes excess water from the blood through ultrafiltration.
Suction force is applied by the dialysis machine across the dialysis filter.
Water is pulled from the blood side into the dialysate side.
Clean blood and waste-filled dialysate exit the dialysis filter.
Clean blood is pumped back into the patient’s circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment.
Waste-filled dialysate is disposed of (including the excess water from the patient’s body that was removed during ultrafiltration).
Overall process continues until the end of the treatment session.
Chronic dialysis
3–4 hours each session
3 times a week (Monday/Wednesday/Friday or Tuesday/Thursday/Saturday)
Acute dialysis: Treatment duration and daily schedule are variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables.
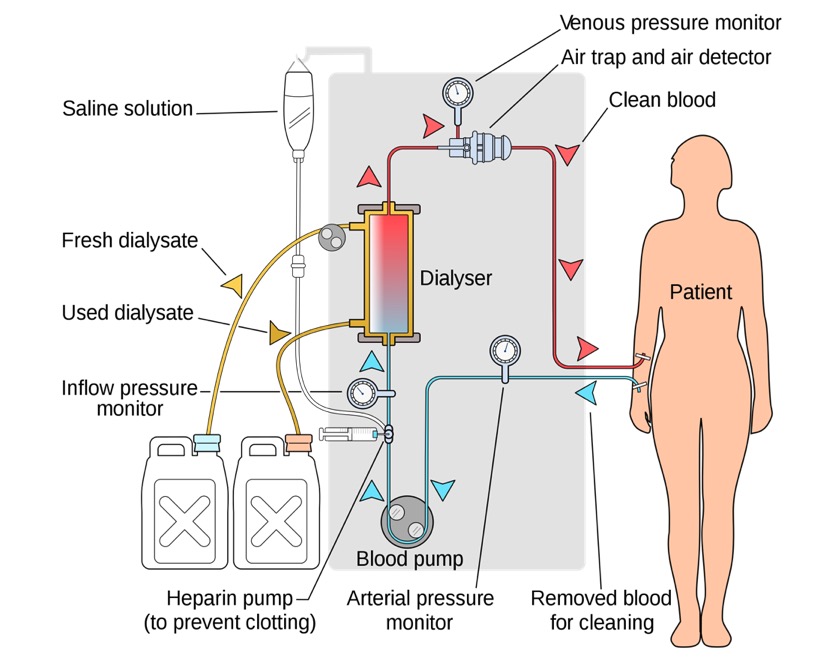
Circuit setup for hemodialysis:
Two sets of tubing are connected to the patient’s dialysis access (central venous catheter or two needles inserted into AVF/AVG). Blue tubing in the illustration represents the azotemic blood. This blood is pumped from the patient into the dialysis filter, which then removes toxins primarily through diffusion. Inside the dialyzer or filter are tubes composed of the filtering material. Blood flows through the inside of the tiny tubes in one direction. Dialysis fluid, or dialysate (which enters and leaves the dialyzer via the tubing shown in yellow in the image), on the other hand, flows on the outside of the tiny tubes (but within the single plastic cylinder that contains them) in the opposite direction. The opposing directions of blood and dialysate result in maximal concentration gradients that drive the diffusion of toxins. The filter removes excess water from the blood through ultrafiltration via a suction force/pressure applied by the machine across the filter. Water is pulled from the blood side into the dialysate side. Clean blood (through the red tubing in the image) is pumped back into the patient’s circulation. Waste-filled dialysate (through the yellow tubing) exits the dialysis filter and is disposed of (including the excess water/fluid).
Image: “Hemodialysis” by Yassine Mabret. License: CC BY 3.0
Schematic of hemodialysis filter/dialyzer showing the blood (coming into the filter) flowing in the direction opposite to that of the dialysate: The process of filtering fluid (from the blood to the dialysate) is ultrafiltration. Pressure is generated by the dialysis machine, and the transmembrane pressure between the blood (high pressure) to the dialysate (low pressure) allows fluid to be removed. Toxins are also removed from the azotemic blood. Toxins from the blood move across the dialysis membrane by the process of diffusion.
Image by Lecturio.
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome prescription
The nephrologist may control many variables within the dialysis procedure:
Blood is prone to clotting as it travels through the plastic tubing and dialysis membrane.
When cloting occurs, the treatment must be stopped and reset, which limits the overall treatment time and effectiveness.
IV heparin is often used to help prevent this clotting of the dialysis circuit.
Electrolyte composition of the dialysate:
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia can be set between 0 and 4 mEq/L.
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia can be set between 130 and 145 mEq/L.
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes can be set between 2.5 and 3.5 mEq/L.
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes can be set between 30 and 40 mEq/L.
Speed of blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure and dialysate flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure:
Dialysate flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure ranges from 500 to 800 mL/min.
Peritoneal dialysis achieves the same net result as hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome (the removal of toxins and excess water); however, the process is completely different.
Instead of removing blood from the patient, filtering it externally, and then returning it to the patient, the filtration occurs within the patient’s abdominal cavity.
The only fluid moving in and out of the patient’s body is the dialysate.
Anatomical considerations
Anatomy of the abdomen can be simply thought of as including:
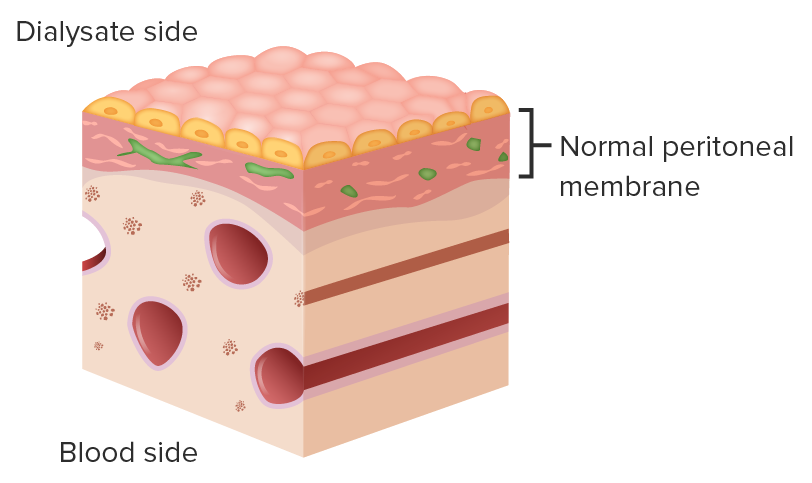
The peritoneal membrane, which lines the intraperitonealIntraperitonealPeritoneum: Anatomy space and abdominal organs, functions as the dialysis filter:
Semipermeable membrane
CapillariesCapillariesCapillaries are the primary structures in the circulatory system that allow the exchange of gas, nutrients, and other materials between the blood and the extracellular fluid (ECF). Capillaries are the smallest of the blood vessels. Because a capillary diameter is so small, only 1 RBC may pass through at a time.Capillaries: Histology on one side
Peritoneal dialysis (PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease) catheter:
Surgically inserted through the abdomen
Allows direct access for the insertion and drainage of dialysis fluid
Outside the body, the catheter extends several inches from the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.
The peritoneal membrane serves as the semipermeable membrane (between the dialysate and the blood/capillary side) and filter in PD.
Image by Lecturio.
Peritoneal dialysis access
Provides direct access to the peritoneal space via a surgically implanted catheter
Unlike hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome, there is only one basic type of PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease access: the PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease catheter:
Surgically implanted through the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Utilizes a cuff system to hold it in place, similar to TDC
Can be used immediately if urgently needed, but usually wait approximately 2 weeks after surgery
Peritoneal dialysis fluid
Not the same as is used for hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome!
The dialysate from PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease is very hypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation to the patient’s blood (the dialysate from hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome is isotonicIsotonicSolutions having the same osmotic pressure as blood serum, or another solution with which they are compared.Renal Sodium and Water Regulation).
HypertonicityHypertonicityVolume Depletion and Dehydration is the result of very high glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance concentrations.
Creates a concentration gradient for ultrafiltration
Process of Peritoneal Dialysis
Peritoneal dialysis procedure
Dialysate is inserted into the peritoneal space through the PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease catheter.
Dialysate and blood interact with the peritoneal membrane.
Toxins and water move from the blood side to the dialysate side via diffusion:
Toxin concentrations are high in the blood and zero in the dialysate.
TonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation of blood (i.e., water concentration) is lower than that of the high-tonicity dialysate.
Electrolyte/acid–base abnormalities also are corrected via diffusion.
After several hours, the two sides equilibrate and no further net transport occurs.
Equilibrated dialysate (including the toxins and excess water from the blood) is removed from the peritoneal space through the PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease catheter.
The process is repeated several times per session.
Methods of peritoneal dialysis
There are two basic methods to perform peritoneal dialysis:
Continuous ambulatory peritoneal dialysis (CAPD)
Automated peritoneal dialysis
Both methods utilize the same catheter and generally have the same clinical results, with selectionSelectionLymphocyte activation by a specific antigen thus triggering clonal expansion of lymphocytes already capable of mounting an immune response to the antigen.B cells: Types and Functions dependent on patient preference.
The primary difference is the use of a machine (called a “cycler”) in automated peritoneal dialysis to automatically pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols the dialysis fluid into and out of the body.
Continuous ambulatory peritoneal dialysis:
Does not use a machine
Gravity is used to allow dialysate to flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure into and out of the intraperitonealIntraperitonealPeritoneum: Anatomy space:
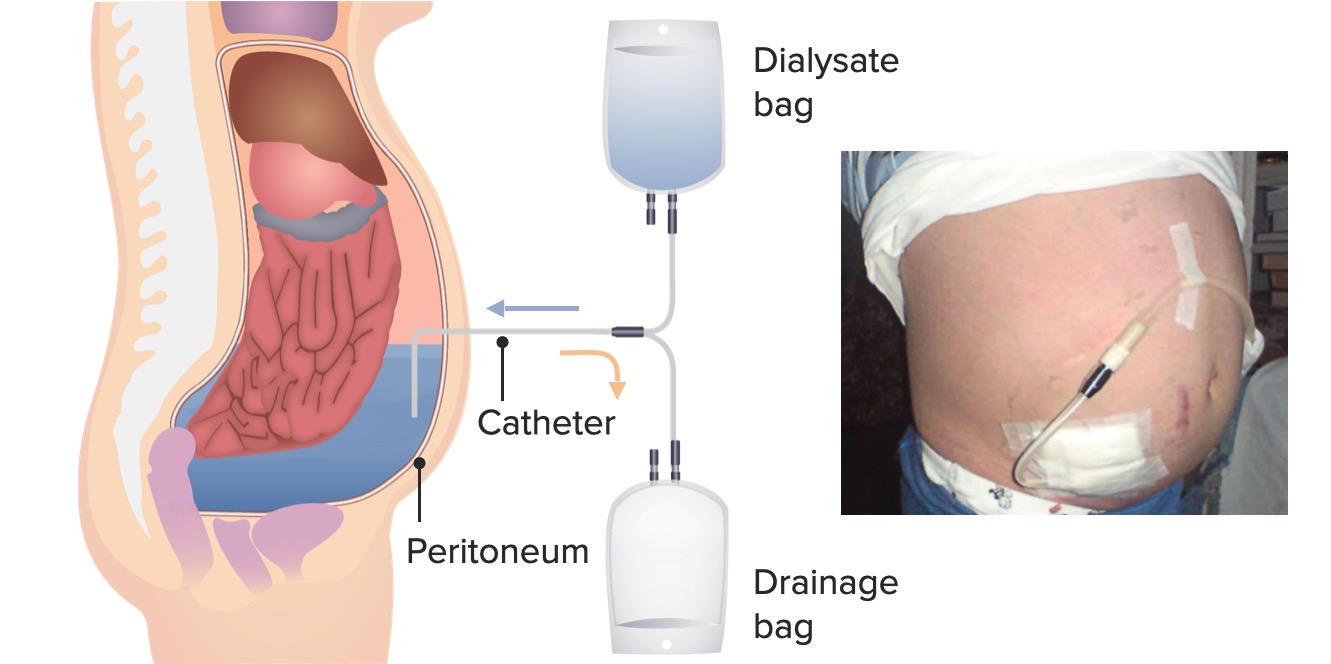
Bag of fresh dialysate is hung above the patient.
Drainage bag for spent dialysate rests below the patient.
Treatment is done throughout the day:
Patient uses sterileSterileBasic Procedures technique to connect PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease catheter tubing to dialysate bag.
Approximately 2 L of dialysate are inserted into the abdomen.
Patient can ambulate and go about their normal day while the fluid acts.
Several hours later (dwell time), the patient uses sterileSterileBasic Procedures technique to connect to the drainage bag and dialysate bag.
Patient drains the spent dialysate from the abdomen into the drainage bag.
Patient refills the abdomen with fresh dialysate (process known as an “exchange”).
Pros:
No machine needed
Patient not continuously attached to apparatus for many hours
Patient less likely to have sleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep disturbed by dialysis (treatment is during the day)
Must connect and disconnect multiple times per day, increasing the chance for touch contamination
Patient must monitor the dwell time.
Fluid that goes in and out of the abdomen must be measured; too much fluid in will be uncomfortable (net fluid removed is the ultrafiltration volume).
Continuous ambulatory peritoneal dialysis: A bag of fresh dialysate is hung above the patient and a drainage bag for spent dialysate rests below the patient. The treatment is done throughout the day, with approximately 2 L of dialysate inserted into the abdomen. The patient can ambulate and go about their normal day while the fluid acts. Several hours later (dwell time), the patient uses sterile technique to connect to the drainage bag and dialysate bag. The patient drains the spent dialysate from the abdomen into the drainage bag.
Left image by Lecturio.
Right image: “Our index patient with peritoneal dialysis catheter” by Faculty of Medicine, “Ovidius” University, 145 Tomis Blvd, Constanta 900591, Romania. License: CC BY 2.0
Automated peritoneal dialysis:
Uses a machine (cycler) to transfer fluid into and out of the peritoneal space
Treatment is done primarily at night.
Patient uses sterileSterileBasic Procedures technique to connect PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease catheter to the cycler.
Cycler is turned on, and patient goes to sleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep.
Cycler automatically pumps approximately 2 L of dialysate into the abdomen.
Dialysate dwells for several hours.
Cycler automatically pumps the spent dialysate out.
Process repeats with fresh dialysate.
When the patient wakes up, they detach from the cycler and the process is finished.
Pros:
Less work for patient, as the cycler measures fluid volumes in and out
Patient can review data (ultrafiltration volume) on the cycler after treatment.
Patient connects/disconnects only two times per session, so less chance for touch contamination.
Can function during daytime without having to stop for drain/fill procedure (i.e., exchanges)
Must be attached to cycler for 8–10 hours consecutively
May interrupt sleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep
Peritoneal dialysis prescription
Considerations:
The variables for the PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease prescription are much different from those for the hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome prescription.
After choosing between automated peritoneal dialysis and CAPD, the primary variables are:
Strength of dialysate used
Number of exchanges per session
Length of each exchange
It takes several weeks after changing the PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease prescription to determine its effect, unlike the hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome prescription, which can be monitored after each session.
Prescription contents:
Automated peritoneal dialysis versus CAPD
Number of exchanges per session (usually 4–5)
Dwell time per exchange:
4–6 hours for CAPD
1–3 hours for automated peritoneal dialysis
Dwell volume (usually approximately 2 L, but can be increased)
OsmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation is 346, 396, and 485, respectively.
ColloidColloidColloid solutions include large proteins or cells that do not readily cross capillary membranes. They remain in the ecf and do not distribute into the icf (similar to crystalloids).Intravenous Fluids
Example: Physician may instruct the patient to switch from green bag to red bag if more ultrafiltration is needed.
Other components (i.e., electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, base buffer) are standardized and not commonly manipulated.
Choice of Method
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome versus peritoneal dialysis
Studies have failed to show overall, long-term differences in outcomes (including mortalityMortalityAll deaths reported in a given population.Measures of Health Status) between hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome and peritoneal dialysis.
The decision between the two methods comes down to patient preference, based on the factors below.
Pros and consCoNSStaphylococcus of hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome
Pros:
Not work-intensive for the patient:
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship do not have to connect themselves to the dialysis machine.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship do not have to operate or monitor the dialysis machine.
Changes to dialysis prescription can be assessed for quickly.
Ultrafiltration goal can be changed every session if extra fluid weight is gained.
Time can be added to a session, if needed.
ElectrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes can be manipulated each session.
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship have long-term issues with hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome access:
Arteriovenous fistulas can fail to mature and require multiple surgeries.
Arteriovenous fistulas/arteriovenous grafts can clot and require declotting procedures.
Tunneled dialysis catheter can get infected.
Must spend considerable time in dialysis unit (approximately 9–12 hours)
Must have adequate transportation to and from the dialysis unit
Residual renal function is lost more quickly than with PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease.
Must be stricter with oral fluid restriction:
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush SyndromepatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship tend to have minimal residual urine output.
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush SyndromepatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship tend to have minimal response to oral diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication.
All fluid that the patient drinks between dialysis treatments (approximately 48 hours) must be removed during the following treatment.
Some have significant issues with adverse effects:
Can adjust life around dialysis more easily than with hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome:
Many patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship on PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease continue to work, which is less common for those on hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome.
Dialysis takes place only at night with cycler
Residual renal function is lost more slowly than with hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome.
Can be more liberal with oral fluid restriction:
With PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship tend to have significant urine output and will respond to oral diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication.
With PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship dialyze 7 days a week, with the fluid from only the previous 24 hours needing to be removed with each treatment.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must connect themselves to and disconnect themselves from the dialysis apparatus.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must always use strict sterileSterileBasic Procedures technique and avoid touch contamination.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must monitor dialysis process (dwell time, ultrafiltration).
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must make sure they do not run out of supplies.
PeritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury:
Infection of the peritoneal space
Very painful
Usually due to touch contamination during the connect/disconnect process
Treated with antibiotics that can be added to the dialysate bags
Can limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation the utility of PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease if patient is diabetic (insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin requirements will increase)
Changes to dialysis prescription take several weeks to take effect.
Kidney Disease: Improving Global Outcomes (KDIGO) Chronic Kidney Disease Work Group. (2013). KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Suppl.; 2:1–163.
National Kidney Foundation. (2015). KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. American Journal of Kidney Diseases 66(5), 884–930. https://doi.org/10.1053/j.ajkd.2015.07.015