In the pediatric population, imaging often plays a critical diagnostic role, especially in diagnosing congenital anomalies. In children, CT scans are avoided if at all possible due to the high risk of radiation exposure. In addition, both CT and (especially) MRI require children to hold still for significant periods of time and often require sedation to complete the study. For these reasons, plain radiography (often with contrast), fluoroscopy, and ultrasound are the imaging modalities of choice for most suspected cases involving GI pathology. Some conditions that can be diagnosed using imaging include hypertrophic pyloric stenosis, necrotizing enterocolitis, midgut malrotation with or without volvulus, intestinal atresia intussusception, appendicitis, Hirschsprung disease, mesenteric lymphadenitis, and obstructions of the biliary tree.
Several additional issues must be considered during pediatric imaging, including:
Limiting/avoiding radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma exposure as much as possible → CT scans are avoided
Can the individual hold still for the image without sedation? → MRI scans are usually avoided/not needed, especially in young children
Best imaging modalities:
Ultrasound
Plain radiography
FluoroscopyFluoroscopyProduction of an image when x-rays strike a fluorescent screen.X-rays
Preparatory steps prior to image analysis
Prior to the interpretation of any image, the physician should take certain preparatory steps. The same systematic approach should always be followed:
Confirm the name, date, and time on all images.
Obtain the individual’s medical history and physical examination findings.
Confirm the appropriate exam and technique for the desired pathology.
Compare any available images of the same area previously taken using the same modality.
Right or left marker on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
In the US, standard exam views place a marker (dot) to the right side of the subject.
For CT/MRI: On axialAxialComputed Tomography (CT) view, the image is sliced and viewed from inferior to superior (as if you are looking from the subject’s feet up).
Radiography/Fluoroscopy
Indications
Abdominal distension
Abnormal bowel movements (chronic constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).)
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
History of ingested foreign object
Suspected (or potential) bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis or perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Palpable massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Trauma
Verification of correct placement of IVs, lines, and tubes
Advantages
Low cost
Relatively low radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma dose
Can be acquired with the subject supine or upright (upright is better for evaluating bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis and free air)
No rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of shoulders or hips; the following should be symmetric:
Pedicles of the spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy
RibsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy
Iliac crests
Obturator foramen
Board should be against the back.
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests beams in the anterior → posterior direction through the subject
For lateral decubitus images:
The subject should be lying on their side.
The board should be against the subject’s back (held up by an assistant).
Usually left lateral decubitus (i.e., left side down on table) allows better visualization of free air.
Field of view:
Image should be centered in the midline at the level of the iliac crests.
Superiorly: Include at least up to the full diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy.
Inferiorly: inferior pubic rami
Laterally: lateral edges of the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Images should always be interpreted using a systematic approach.
Follow the steps in the introduction (e.g., confirm subject’s name, medical history, image orientationOrientationAwareness of oneself in relation to time, place and person.Psychiatric Assessment, and correct study for the suspected pathology).
Assess adequacy of the image:
RotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays: Is the subject rotated?
PenetrationPenetrationX-rays is the degree to which the radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma has passed through the body, resulting in a darker or lighter image:
Underpenetration: not enough X-raysX-raysX-rays are high-energy particles of electromagnetic radiation used in the medical field for the generation of anatomical images. X-rays are projected through the body of a patient and onto a film, and this technique is called conventional or projectional radiography. X-rays have passed through → unable to differentiate different dense structures → film appears white and features are less apparent
Overpenetration: too many X-raysX-raysX-rays are high-energy particles of electromagnetic radiation used in the medical field for the generation of anatomical images. X-rays are projected through the body of a patient and onto a film, and this technique is called conventional or projectional radiography. X-rays have passed through → film appears dark and features are less apparent
Look for solid organ silhouettesSolid Organ SilhouettesImaging of the Urinary System (liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy, kidney).
Evaluate soft tissues for abnormal calcifications (stones, masses in pediatrics).
Look at lung basesBasesUsually a hydroxide of lithium, sodium, potassium, rubidium or cesium, but also the carbonates of these metals, ammonia, and the amines.Acid-Base Balance for evidence of consolidationConsolidationPulmonary Function Tests, effusion, and pneumothoraces.
Evaluate osseous structures (vertebral bodyVertebral bodyMain portion of the vertebra which bears majority of the weight.Vertebral Column: Anatomy height, iliac bones, femurs).
Look at tubes and lines.
If an abnormality is noted → use patterns for differential diagnoses
Should not distend the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy by > 3 cm
Should be uniform throughout the abdomen
Organs:
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy region visible under the right hemidiaphragm should be uniform with no free air.
StomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy are visible with air in the lumen under the left hemidiaphragm.
Renal outlines, if visible, should be in the right and left upper quadrants.
Fat planes: along the periphery
Lung basesBasesUsually a hydroxide of lithium, sodium, potassium, rubidium or cesium, but also the carbonates of these metals, ammonia, and the amines.Acid-Base Balance:
Should be clear with minimal lung markings
Costophrenic angles should be sharp.
Bones:
Pedicles should be present and symmetric bilaterally.
Vertebral bodyVertebral bodyMain portion of the vertebra which bears majority of the weight.Vertebral Column: Anatomy heights should gradually enlarge as they move inferiorly.
Radiographic/fluoroscopic images are acquired while swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility barium contrast.
Esophagram:
Focuses primarily on the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Allows assessment of esophageal function and anatomy of the lumen
Indicated in the evaluation of eating/drinking/swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility difficulties and gastric reflux
Upper GI radiography:
Includes evaluation of the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy, stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, and duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Helpful in diagnosing malrotation, volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus, and/or duodenal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS)
Images are taken at different time points (minutes to hours) following oral contrast → contrast is followed all the way through the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy into the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Usually (though not always) follows an upper GI study
Allows assessment of strictures, obstructions, masses, and position of the intestines
Normal findings:
Normal movement of contrast in peristaltic waves down the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy, into the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, and into the small intestines
No reflux
No narrowing/strictures
Normal position of the organs
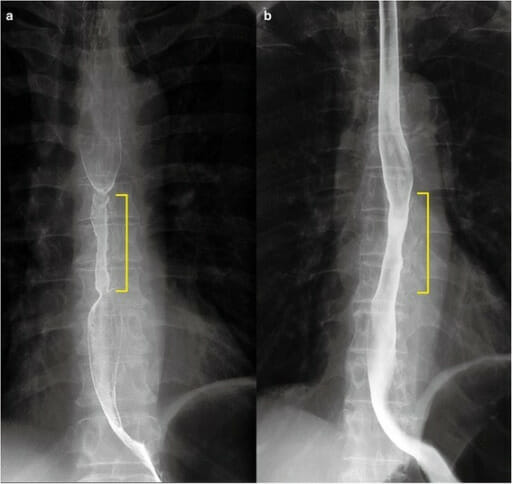
Barium esophagram showing a subtle midesophageal narrowing (yellow marker)
Image: “Barium esophagram 1 month after endoscopic submucosal dissection.” By Department of Gastroenterology, Keiyukai Daini Hospital. License: CC BY 4.0
Contrast enema
Radiographic/fluoroscopic images are taken while the contrast is injected into the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy via an enema tube.
Allows assessment of lower GI anatomy
Contrast may be barium or a water-soluble agent.
May be indicated for the evaluation of:
Chronic constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation or diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease
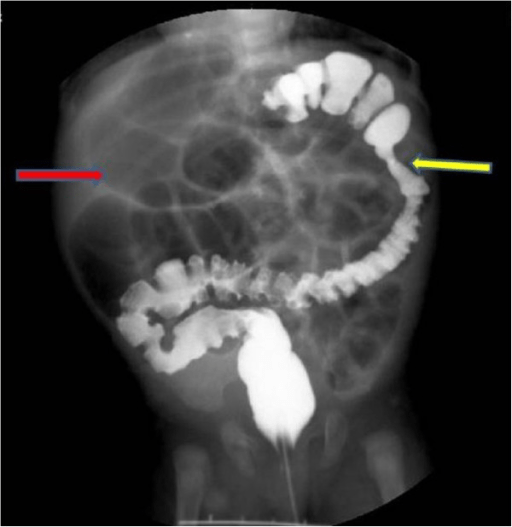
A barium enema study demonstrating colonic atresia: A 2-month-old girl exhibits delayed meconium passage, abdominal distension, and vomiting starting 10 days after birth. Barium enema reveals atresia at the splenic side of the colon (yellow arrow) and distension of the ileum (red arrow).
Image: “Case 3” by Pediatric Surgery Department of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China. License: CC BY 2.0
Sitz marker test to determine colonic transit time
Capsules with a number of small radiopaqueRadiopaqueAn object of high density that blocks X-rays (looks white)X-rays markers are swallowed → radiography performed 3‒5 days later
Allows assessment of bowel motilityMotilityThe motor activity of the gastrointestinal tract.Gastrointestinal Motility and colonic transit
Indicated for the evaluation of chronic constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Normal findings: All markers should be cleared by 5 days.
Ultrasound
Indications
Evaluate for suspected/potential conditions:
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
Hypertrophic pylorusPylorusThe region between the sharp indentation at the lower third of the stomach (incisura angularis) and the junction of the pylorus with the duodenum. Pyloric antral glands contain mucus-secreting cells and gastrin-secreting endocrine cells (g cells).Stomach: Anatomy
For neonates with abnormalities noted on prenatal ultrasonography
Known congenital disease with predisposition for certain complications
Advantages
Low cost
No radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma exposure
Widespread availability
Rapid
Disadvantages
Poor resolution
Narrow field of view
Subject must hold still during image acquisition.
Technician dependent
Exam technique
Positioning:
Depends on the area of concern, but usually supine
The organ of interest should be most superficial to the probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography) without other organs/bowel between the area of interest and the ultrasound probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography).
Maximize contact between the subject’s skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and ultrasound probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography).
Depth:
Determines the field of view
Should include the entire area of concern without excessive deeper areas
Gain:
Determines echogenicity characteristics of the tissue
Solid organ parenchyma should have midrange signal echogenicity.
DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography): assesses velocity and direction of blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure in an area
Interpretation and evaluation
Follow the steps in the introduction (e.g., confirming the subject’s name, medical history, image orientationOrientationAwareness of oneself in relation to time, place and person.Psychiatric Assessment, the correct study for the suspected pathology).
Assess adequacy of the image:
Is the depth and gain appropriate to fully assess the area of concern?
Is the entire area of concern imaged in the proper views for full assessment?
Analyze images:
Take measurements of all relevant structures and compare them with standard reference ranges, for example:
“Fresh” blood: more hyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) signals
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types/calcifications: very hyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) (white)
Should be heterogeneous due to the presence of muscle, fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis, and fat
No fluid collection
Arteries and veinsArteries And VeinsACES and RUSH: Resuscitation Ultrasound Protocols should have appropriate directional flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure.
Ultrasound is theimaging study of choice in suspected cases:
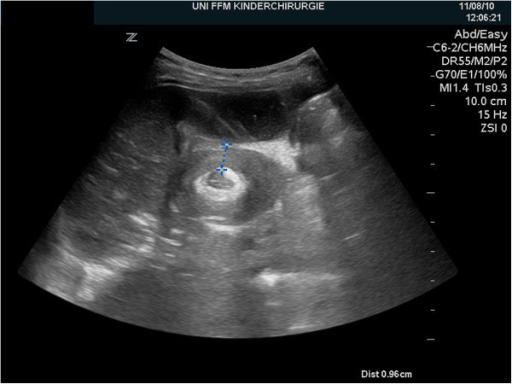
Pyloric thickness > 4 mm
Target signTarget signPseudomembranous Colitis or donut sign: classic cross-sectional appearance of the pylorusPylorusThe region between the sharp indentation at the lower third of the stomach (incisura angularis) and the junction of the pylorus with the duodenum. Pyloric antral glands contain mucus-secreting cells and gastrin-secreting endocrine cells (g cells).Stomach: Anatomy in the shape of a target or donut
Elongated pyloric canal
Upper GI seriesUpper Gi SeriesImaging of the Intestines: only ordered if the exam and ultrasound are nondiagnostic, or if there are other symptoms suggesting more distal obstruction
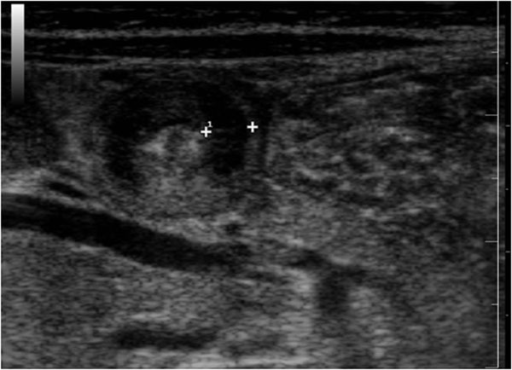
Ultrasound features of hypertrophic pyloric stenosis: The image shows a cross-section of the pylorus demonstrating the “target sign” (also referred to as the “donut sign”). The calipers mark the thickened musculature, with an inner echogenic ring representing the mucosa.
Image: “Ultrasound features of hypertrophic pyloric stenosis” by Second University of Naples, Department of Clinical and Experimental Internistic. License: CC BY 2.0
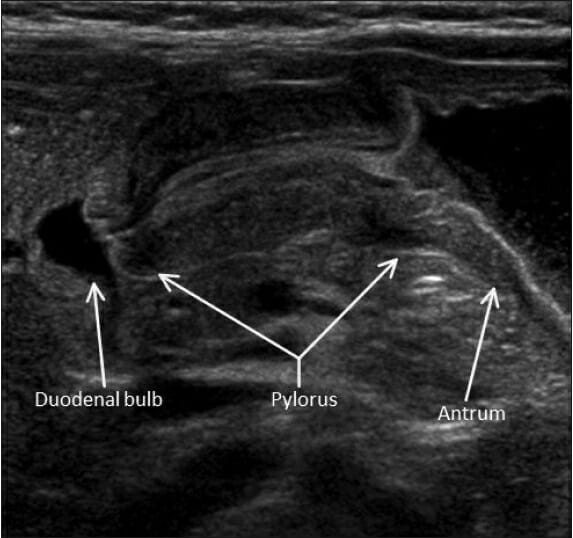
Ultrasound image demonstrating a longitudinal view of the pylorus in a case of hypertrophic pyloric stenosis: Thickening of the pyloric musculature and elongation of the canal is noted.
Image: “Hypertrophic pyloric stenosis” by Herliczek TW. License: CC BY 4.0
Necrotizing enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis (NECNECNecrotizing enterocolitis (NEC) is an intestinal inflammatory process that can lead to mucosal injury and necrosis. The condition is multifactorial, with underlying risk factors that include prematurity and formula feeding. The clinical presentation varies in severity from feeding intolerance, acute findings on abdominal exam, and systemic symptoms. Necrotizing Enterocolitis)
Necrotizing enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis is a relatively common neonatal GI emergency due to infection by gas-forming organisms, which results in ischemic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of the intestinal mucosaIntestinal MucosaLining of the intestines, consisting of an inner epithelium, a middle lamina propria, and an outer muscularis mucosae. In the small intestine, the mucosa is characterized by a series of folds and abundance of absorptive cells (enterocytes) with microvilli.Small Intestine: Anatomy. Infants typically present with a sudden change in feeding toleranceTolerancePharmacokinetics and Pharmacodynamics and abdominal distension in the 1st or 2nd weeks of life.
Plain radiography (imaging modality of choice)findings:
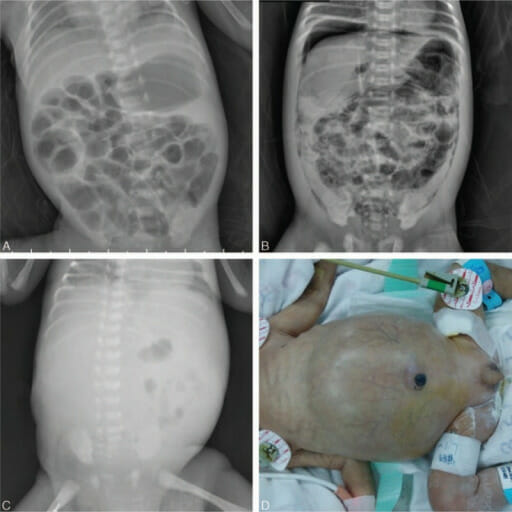
Pneumatosis intestinalisPneumatosis intestinalisA condition characterized by the presence of multiple gas-filled cysts in the intestinal wall, the submucosa and/or subserosa of the intestine. The majority of the cysts are found in the jejunum and the ileum.Necrotizing Enterocolitis:
Pathognomonic for NECNECNecrotizing enterocolitis (NEC) is an intestinal inflammatory process that can lead to mucosal injury and necrosis. The condition is multifactorial, with underlying risk factors that include prematurity and formula feeding. The clinical presentation varies in severity from feeding intolerance, acute findings on abdominal exam, and systemic symptoms. Necrotizing Enterocolitis
Presence of gas within the intestinal wall itself
Appears as a linear or bubbly pattern
Dilated and thickened bowel loops
Fixed dilated loops and absence of intestinal gas (gasless abdomen)
PneumoperitoneumPneumoperitoneumA condition with trapped gas or air in the peritoneal cavity, usually secondary to perforation of the internal organs such as the lung and the gastrointestinal tract, or to recent surgery. Pneumoperitoneum may be purposely introduced to aid radiological examination.Perforated Viscus and/or portal venous gasPortal Venous GasImaging of the Intestines → indicates bowel necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage and perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Ultrasound is used as a 2nd-line test:
Bowel wall thickening
HyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) foci within bowel walls → represents intramural gas
Free fluid (especially with echogenic debris) → suggests perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Note: Barium enemas are contraindicated in NECNECNecrotizing enterocolitis (NEC) is an intestinal inflammatory process that can lead to mucosal injury and necrosis. The condition is multifactorial, with underlying risk factors that include prematurity and formula feeding. The clinical presentation varies in severity from feeding intolerance, acute findings on abdominal exam, and systemic symptoms. Necrotizing Enterocolitis as they may cause bowel perforationBowel perforationPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall.Perforated Viscus.
Necrotizing enterocolitis (NEC) on radiography (A) Subtle portal venous gas with pneumatosis intestinalis (B) Pneumoperitoneum under the right hemidiaphragm and pneumatosis intestinalis (C) Paucity of gas in the abdomen (D) Neonate with a distended abdomen
Image: “Radiographic findings of necrotizing enterocolitis” by Qingfeng Sheng, MD, PhD, Zhibao Lv, MD, Weijue Xu, MD, Jiangbin Liu, MD, Yibo Wu, MD, Jingyi Shi, MD, and Zhengjun Xi, MD. License: CC BY 4.0
MidgutMidgutDevelopment of the Abdominal Organs malrotation and volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
MidgutMidgutDevelopment of the Abdominal Organs malrotation is the abnormal position and fixation of the intestine due to abnormal gut tube rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays during fetal development:
Anatomy varies based on the different rotational abnormalities during development.
Abnormal positioning of the duodenojejunal junction:
Normal anatomy: lies to the left of the midline
Anatomy in malrotation: most commonly to the right of the midline
Anatomy in malrotation: most commonly ends up in the right mid-upper abdomen, fixated to the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen and potentially obstructing the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Predisposes to volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus:
Twisting of the intestines around its mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy, resulting in bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis
Better at diagnosing volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus than malrotation
Findings include:
Abnormal position of the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy and/or superior mesenteric vein
Whirlpool signWhirlpool signTwisting of the superior mesenteric vein and the mesentery around the superior mesenteric artery.Intestinal Malrotation on DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography): caused by vessels twisting around the base of the mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy in volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
Dilated duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (indicates obstruction)
Plain radiography:
Rarely helps with diagnosis, but should be ordered to exclude intestinal perforationIntestinal perforationPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall.Perforated Viscus and pneumoperitoneumPneumoperitoneumA condition with trapped gas or air in the peritoneal cavity, usually secondary to perforation of the internal organs such as the lung and the gastrointestinal tract, or to recent surgery. Pneumoperitoneum may be purposely introduced to aid radiological examination.Perforated Viscus
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus may show dilated loops of bowel and air fluid levelsAir Fluid LevelsImaging of the Intestines, indicating obstruction.
Finding that is diagnostic of malrotation/volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus: directly visualizing the abnormal duodenal position by passing a nasogastric tubeNasogastric tubeMalnutrition in children in resource-limited countries through the area
Upper GI contrast series:
Gold standard for the definitive diagnosis of both malrotation and volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
Obtained if ultrasound findings are equivocal (or negative) but malrotation/volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus is still suspected
Malrotation findings: DuodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy stays to the right of the spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy.
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus:
Corkscrew appearance of the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy and jejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy
Anteroposterior fluoroscopic image after positive enteric contrast administration demonstrates a “corkscrew” appearance of the duodenum, which does not cross the leftward aspect of the spine (dashed line). This finding is suggestive of malrotation and midgut volvulus.
Image: “Upper gastrointestinal study (UGI) demonstrating intestinal malrotation and volvulus with abnormal position of the duodenal-jejunal junction to the right of the spine” by Pediatric Department, Shaare Zedek Medical Center, P.O. Box 3235, 9103102, Jerusalem, Israel. License: CC BY 4.0
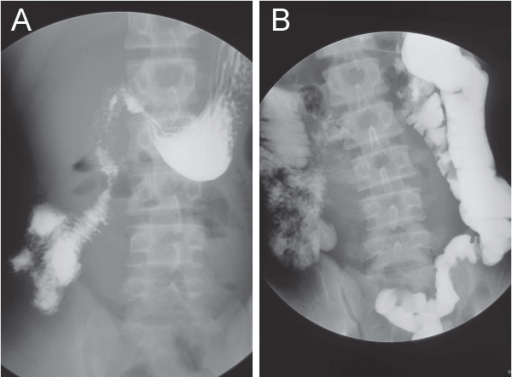
(A) Upper GI series with barium contrast shows that the duodenum remains isolated to the right hemiabdomen without crossing the midline, consistent with malrotation.
(B) Small bowel follow-through shows that the cecum is located in the left lower quadrant.
Image: “Gastrointestinal contrast studies” by Department of Emergency, Disaster and Critical Care Medicine, Hyogo College of Medicine. License: CC BY 2.0
Intestinal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS)is a condition in which a portion of intestine fails to canalize during development, resulting in bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis in newborns. Approximately ½ of all cases constitute duodenal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS). Infants present with vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and abdominal distension. Surgery is the definitive treatment.
Plain radiography:
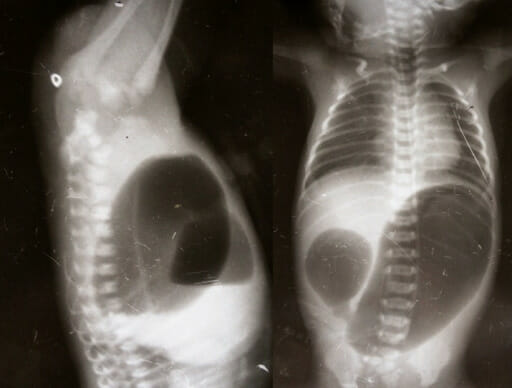
Double bubble sign:
2 “bubbles” of air are seen representing dilation of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and proximal duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy.
PneumoperitoneumPneumoperitoneumA condition with trapped gas or air in the peritoneal cavity, usually secondary to perforation of the internal organs such as the lung and the gastrointestinal tract, or to recent surgery. Pneumoperitoneum may be purposely introduced to aid radiological examination.Perforated Viscus may be seen → represents intestinal perforationIntestinal perforationPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall.Perforated Viscus
Differentiates intestinal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS) from obstruction due to malrotation with volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
Contrast enema:
Obtained if the above studies fail to diagnose the cause of obstruction
Differentiates colonic atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS) from obstruction due to Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease
Radiograph showing the double bubble sign in an infant with duodenal atresia
Image: “Invertogram showing high ARM and AP view showing duodenal atresia” by Manoj Saha, Department of Pediatric Surgery, Gauhati Medical College. License: CC BY 3.0
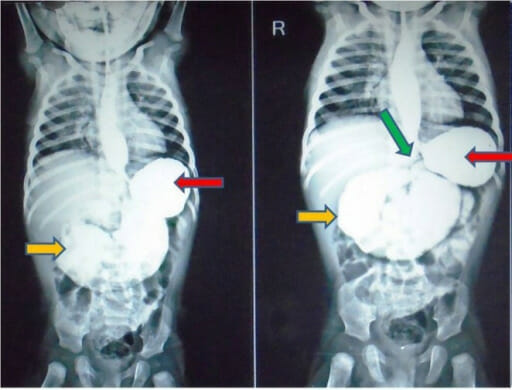
Upper GI contrast study taken at 5 and 15 minutes showing a dilated stomach (red arrows) and marked distension of the duodenum (yellow arrows) all the way to the duodenojejunal junction (green arrow). The findings suggest jejunal atresia. Gastroesophageal reflux is also noted in the esophagus, but the rest of the distal bowel appears normal.
Image: “Upper gastrointestinal contrast study” by Rahul Gupta, Praveen Mathur, Sharanabasappa Gubbi, Pradeep Kumar Gupta, Ramendra Shukla, and Anu Bhandari. License: CC BY 3.0
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception: telescoping of a proximal segment of bowel into an adjacent distal segment, most often in the ileocolic region. IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception is the most common abdominal emergency in children < 2 years of age, which presents with the “classic triad” of sudden onset crampy abdominal painAbdominal PainAcute Abdomen, a palpable sausage-shaped massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast, and currant jelly stools.
Ultrasound:
Often the diagnostic test of choice
Excellent sensitivity, specificity, and negative predictive valueNegative predictive valueThe NPV is the percentage of people with a negative test result who are actually disease free, among all people with a negative result regardless of whether or not they have the disease.Epidemiological Values of Diagnostic Tests (NPVNPVThe NPV is the percentage of people with a negative test result who are actually disease free, among all people with a negative result regardless of whether or not they have the disease.Epidemiological Values of Diagnostic Tests) when performed by an experienced sonographer
Can detect the pathologic lead points that may have caused the intussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
Key finding is a “target” sign (most often in the RLQ):
Also called a bull’s eye or coiled spring sign
Represents layers of intestine within the intestine
↓ Perfusion on color DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography) → indicates ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
Plain radiography:
Nondiagnostic for intussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception itself
Should be ordered to exclude perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis and for screeningScreeningPreoperative Care of other pathologies
Possible findings:
CrescentCrescentRapidly Progressive Glomerulonephritis (meniscus) sign:soft tissueSoft TissueSoft Tissue Abscess density (intussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception) projecting into the gas of the large bowel
Signs of small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis: distended loops of bowel with absent colonic gas
Management:
In stable individuals, intussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception is usually managed with nonoperative reduction (e.g., an air enema) delivered under fluoroscopic or sonographic guidance.
Surgery is indicated for:
Unstable individuals
Cases complicated by intestinal perforationIntestinal perforationPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall.Perforated Viscus or peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
Unsuccessful nonoperative reduction
Ultrasonography of the right abdomen shows the typical ultrasonographic “target” sign of ileocolic intussusception.
Image: “Ultrasonography of the right upper abdominal quadrant” by Department of Pediatric Surgery and Pediatric Urology, Johann Wolfgang Goethe University of Frankfurt. License: CC BY 4.0
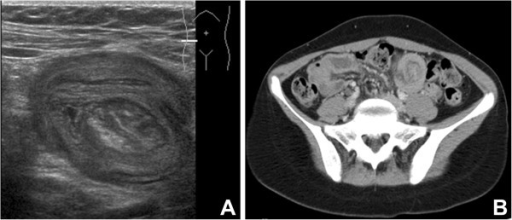
Ultrasound (A) and CT (B) radiographic evidence of intussusception (A) Ultrasound showing the appearance of bowel within a bowel, consistent with intussusception (B) Axial CT with IV contrast showing intussusception in the left lower quadrant
Image: “Radiographic evidences of the suspected intussusception” by Pediatric Surgery Unit, DMCP, Hôpital de l’Enfance, CHUV, Lausanne, Switzerland. License: CC BY 2.0
Abdominal radiograph after air enema demonstrates a “crescent” (meniscus) sign demonstrating intussusception.
Image: “Abdominal radiograph after subsequent air enema” by Jaclyn Otero, Molly R. Posa, and Maria N. Kelly. License: CC BY 4.0
MeconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the NeonateileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Obstruction of the terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy by abnormally thick and sticky meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate. MeconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the NeonateileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction is often seen in neonates with cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans and Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease. Affected neonates usually present with vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, failure to pass meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate within 12‒24 hours, and abdominal distension.
Plain radiography: to rule out perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis and other abnormalities
Contrast enema:
Diagnostic and therapeutic
Small caliber colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy due to disuse
MeconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate pellets can be seen in the terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy.
Often releases the plug (otherwise, surgery is required)
Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease
Also known as congenital aganglionic megacolonMegacolonMegacolon is a severe, abnormal dilatation of the colon, and is classified as acute or chronic. There are many etiologies of megacolon, including neuropathic and dysmotility conditions, severe infections, ischemia, and inflammatory bowel disease.Megacolon, Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease is characterized by the absence of nerve cells in the distal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy, resulting in failure of the affected segment to relax, leading to functional obstruction. Affected neonates present with bilious emesis, abdominal distension, and failure to pass meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate. Associated enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis is common.
Plain radiography:
Dilated proximal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy with collapsed distal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy/rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Rules out perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Normal films donot exclude the diagnosis.
Contrast enema is thebest radiologic test:
Pathognomonic finding: presence of a transition zone between the distended normal proximal bowel and narrow aganglionic distal segments
The site of the transition zone depends on the extent of intestinal involvement, but is usually in the rectosigmoid area.
May be absent: Normal films donot exclude the diagnosis.
MeconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate plugs may be seen as multiple filling defectsFilling DefectsImaging of the Intestines within the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy.
Other diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests:
Definitive diagnosis requires a rectal biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma, which should be obtained prior to surgery.
Abdominal anteroposterior radiograph of a neonate with Hirschsprung disease showing air-filled distended loops of the large intestine: No part of the descending or sigmoid colon can be identified.
Image: “Abdominal plain X-ray shows a generalized distention of the loops of the large intestine” by Nusrat et al. License: CC BY 4.0
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis is the inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy, which characteristically presents with periumbilical painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways migrating to the RLQ with guarding, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, and feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever. In children, the diagnosis is usually clinical with/without the use of ultrasound. Management is usually surgical.
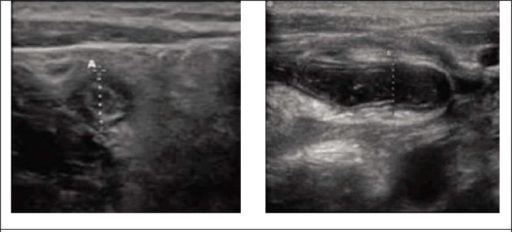
Ultrasonography:AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis cannot be reliably excluded unless the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy is definitively seen.
Can consider CT and/or MRI if the ultrasound is nondiagnostic. Findings are similar to those from ultrasound, although CT/MRI have higher sensitivity/specificity.
Sonographic views in appendicitis: axial (left) and transverse (right). The overall diameter between the calipers is shown.
Image: “Sonographic views of appendix.” by Ebrahim Karimi, Mohammad Aminianfar, Keivan Zarafshani, and Arash Safaie. License: CC BY 3.0
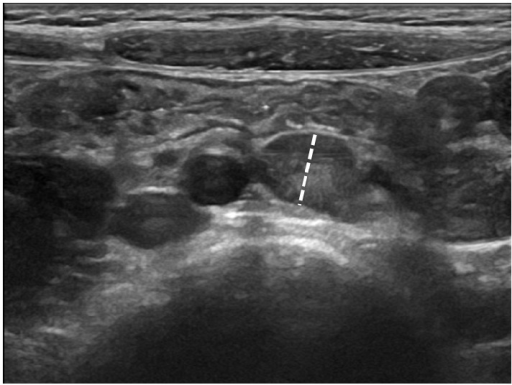
Mesenteric lymphadenitisLymphadenitisInflammation of the lymph nodes.Peritonsillar Abscess refers to inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation in the mesenteric lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy (usually in the RLQ) that often occurs when the enteric immune systemImmune systemThe body’s defense mechanism against foreign organisms or substances and deviant native cells. It includes the humoral immune response and the cell-mediated response and consists of a complex of interrelated cellular, molecular, and genetic components.Primary Lymphatic Organs reacts strongly to an infection (e.g., viral infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, Yersinia enterocoliticaYersinia enterocoliticaA species of the genus yersinia, isolated from both man and animal. It is a frequent cause of bacterial gastroenteritis in children.Yersinia spp./Yersiniosis infection). Stretching of the lymphLymphThe interstitial fluid that is in the lymphatic system.Secondary Lymphatic Organs node capsules can result in painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways similar to that experienced in appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis; however, mesenteric lymphadenitisLymphadenitisInflammation of the lymph nodes.Peritonsillar Abscess is self-limitingSelf-LimitingMeningitis in Children.
Ultrasound of the right lower quadrant showing prominent mesenteric lymph nodes measuring up to 9 mm, suggestive of mesenteric lymphadenitis
Image: “Abdominal ultrasound showing large hypoechoic mesenteric lymph nodes in a 6-year-old girl with acute nonspecific mesenteric lymphadenitis” by Rossana Helbling, Elisa Conficconi, Marina Wyttenbach, Cecilia Benetti, Giacomo D. Simonetti, Mario G. Bianchetti, Flurim Hamitaga, Sebastiano A.G. Lava, Emilio F. Fossali, and Gregorio P. Milani. License: CC BY 4.0
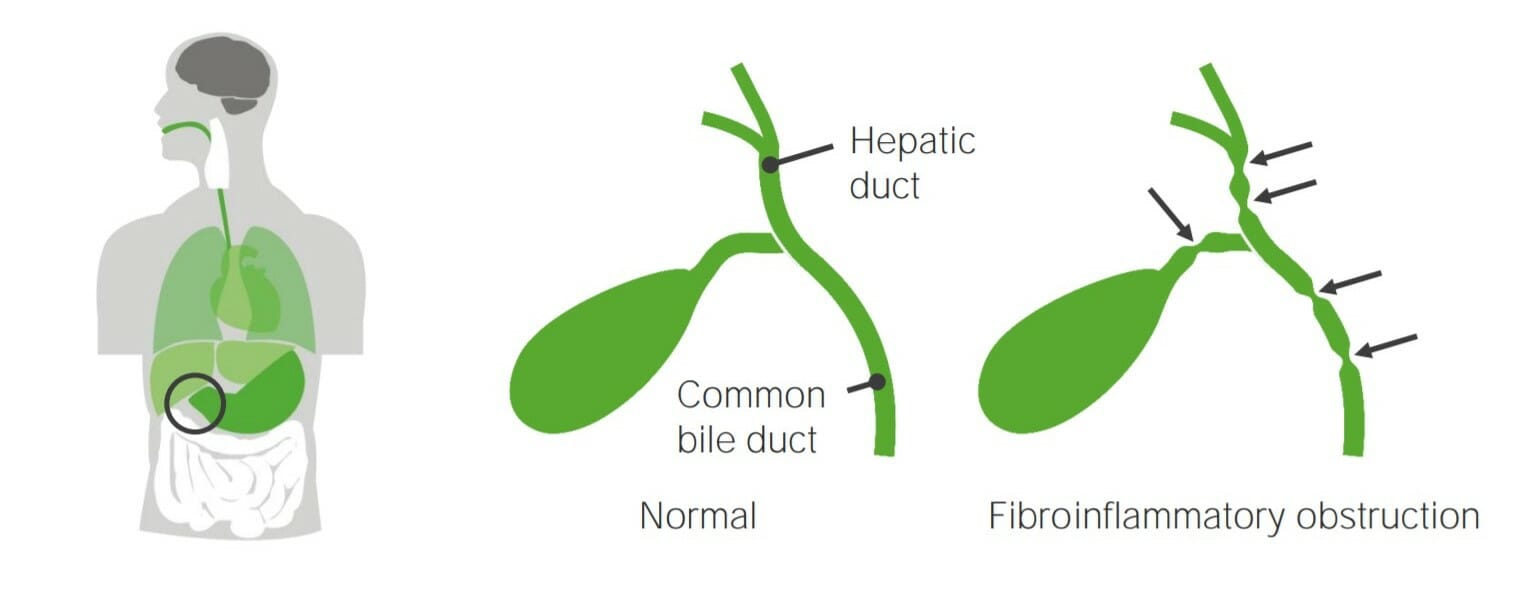
Obstructive biliary tractBiliary tractBile is secreted by hepatocytes into thin channels called canaliculi. These canaliculi lead into slightly larger interlobular bile ductules, which are part of the portal triads at the “corners” of hepatic lobules. The bile leaves the liver via the right and left hepatic ducts, which join together to form the common hepatic duct. Gallbladder and Biliary Tract: Anatomy disorders
Two significant biliary tractBiliary tractBile is secreted by hepatocytes into thin channels called canaliculi. These canaliculi lead into slightly larger interlobular bile ductules, which are part of the portal triads at the “corners” of hepatic lobules. The bile leaves the liver via the right and left hepatic ducts, which join together to form the common hepatic duct. Gallbladder and Biliary Tract: Anatomy disorders that can cause obstruction include biliary atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS) and choledochal cystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change. Both present with obstructive jaundiceObstructive jaundiceHepatocellular Carcinoma (HCC) and Liver Metastases and acholic stools. Treatment is surgical.
Choledochal cystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change: congenital anomalies of the bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct cyst that cause abnormal enlargement and obstruction of the intrahepatic and/or extrahepatic bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy ducts
Absence or irregular shape of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
Findings of choledochal cystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change: hypoechoicHypoechoicA structure that produces a low-amplitude echo (darker grays)Ultrasound (Sonography) masses seen
Also used to exclude other causes of cholestasis (e.g., gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis)
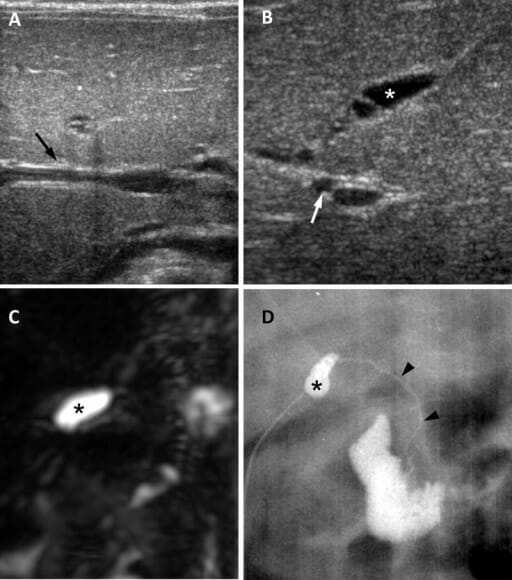
Biliary atresia in a 65-day-old girl: (A) Ultrasound in the transverse plane shows a negative triangular cord sign (arrow). (B) Ultrasound image in the oblique subcostal plane shows an atretic gallbladder measuring 0.8 cm (asterisk) and enlarged hepatic artery measuring 1.5 mm (arrow). (C) A 3D MRCP shows no visible extrahepatic biliary tree and the presence of a small gallbladder (asterisk). (D) Surgical cholangiography shows a small gallbladder (asterisk) and a patent but extremely hypoplastic common bile duct.
Image: “Biliary atresia in a 65-day-old girl” by Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine. License: CC BY 4.0