Mallory-Weiss syndrome (MWS) is bleeding from longitudinal mucosal lacerations (tears) in the distal esophagus and proximal stomach caused by a sudden rise in intraluminal esophageal pressure with forceful or recurrent vomiting. Hematemesis is due to bleeding from submucosal blood vessels and is self-limited in 80%–90% of patients. Diagnosis is made by taking a history and performing upper GI endoscopy. Treatment includes gastric acid suppression, endoscopic intervention, and angiotherapy if there is active bleeding. Blood transfusions and surgery are not usually required.
2–5 times more common in men than women, and is rare in children
History of heavy alcohol use in 40%–80% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
In women of childbearing age, the most common cause is hyperemesis gravidarum.
Accounts for approximately 5%–10% of upper gastrointestinal bleedingGastrointestinal bleedingGastrointestinal bleeding (GIB) is a symptom of multiple diseases within the gastrointestinal (GI) tract. Gastrointestinal bleeding is designated as upper or lower based on the etiology’s location to the ligament of Treitz. Depending on the location of the bleeding, the patient may present with hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (fresh blood in stools). Gastrointestinal Bleeding
Risk factors[1,4,6]
Alcohol use disorderAlcohol use disorderAlcohol is one of the most commonly used addictive substances in the world. Alcohol use disorder (AUD) is defined as pathologic consumption of alcohol leading to impaired daily functioning. Acute alcohol intoxication presents with impairment in speech and motor functions and can be managed in most cases with supportive care. Alcohol Use Disorder: 40%–80% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
May coexist with esophageal varices.
Any event provoking a sudden rise in pressure at the gastroesophageal junctionGastroesophageal junctionThe area covering the terminal portion of esophagus and the beginning of stomach at the cardiac orifice.Esophagus: Anatomy (GEJ):
Forceful or recurrent retching, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Hiccupping or violent coughing spasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy
Blunt abdominal trauma
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship have no risk factors.
There is conflicting evidence regarding hiatal herniaHiatal herniaStomach herniation located at or near the diaphragmatic opening for the esophagus, the esophageal hiatus.Congenital Diaphragmatic Hernias as a risk factor; a large study in 2017 showed no correlationCorrelationDetermination of whether or not two variables are correlated. This means to study whether an increase or decrease in one variable corresponds to an increase or decrease in the other variable.Causality, Validity, and Reliability.[8]
Pathogenesis[1,6]
Exact pathogenesis is incompletely understood but involves well-described mechanical forces.
Rapid increase in intra-abdominal pressure and intragastric pressure → exceeds lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy pressure → gastric contents are released into the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy → autonomic reflexes cause the upper esophageal sphincterUpper esophageal sphincterThe structure at the pharyngoesophageal junction consisting chiefly of the cricopharyngeus muscle. It normally occludes the lumen of the esophagus, except during swallowing.Esophagus: Anatomy (UES) to relax → vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and mucosal stress
Possible pathogenetic mechanisms:
Longitudinal esophageal tears may result from very high intra-abdominal pressures alone or combined with the failure of the UES to relax
Increased thoracic and esophageal intraluminal pressure may be transmitted from the abdomen, or transient prolapse of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy into the distal esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy may contribute to localized shearing.
Tears involving the submucosal blood vessels result in bleeding.
Acute-onset hematemesisHematemesisVomiting of blood that is either fresh bright red, or older ‘coffee-ground’ in character. It generally indicates bleeding of the upper gastrointestinal tract.Mallory-Weiss Syndrome (Mallory-Weiss Tear) after retching, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, or coughing
Epigastric or back painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
There are currently no specific guidelines for the diagnosis and management of MWSMWSMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear) in the United States or the United Kingdom. The following information is based on the typical evaluation and management for upper GI bleeding.
Clinical history of vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and hematemesisHematemesisVomiting of blood that is either fresh bright red, or older ‘coffee-ground’ in character. It generally indicates bleeding of the upper gastrointestinal tract.Mallory-Weiss Syndrome (Mallory-Weiss Tear) (with historical features of retching, alcohol use)
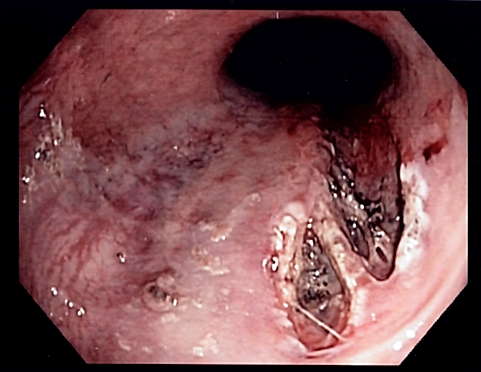
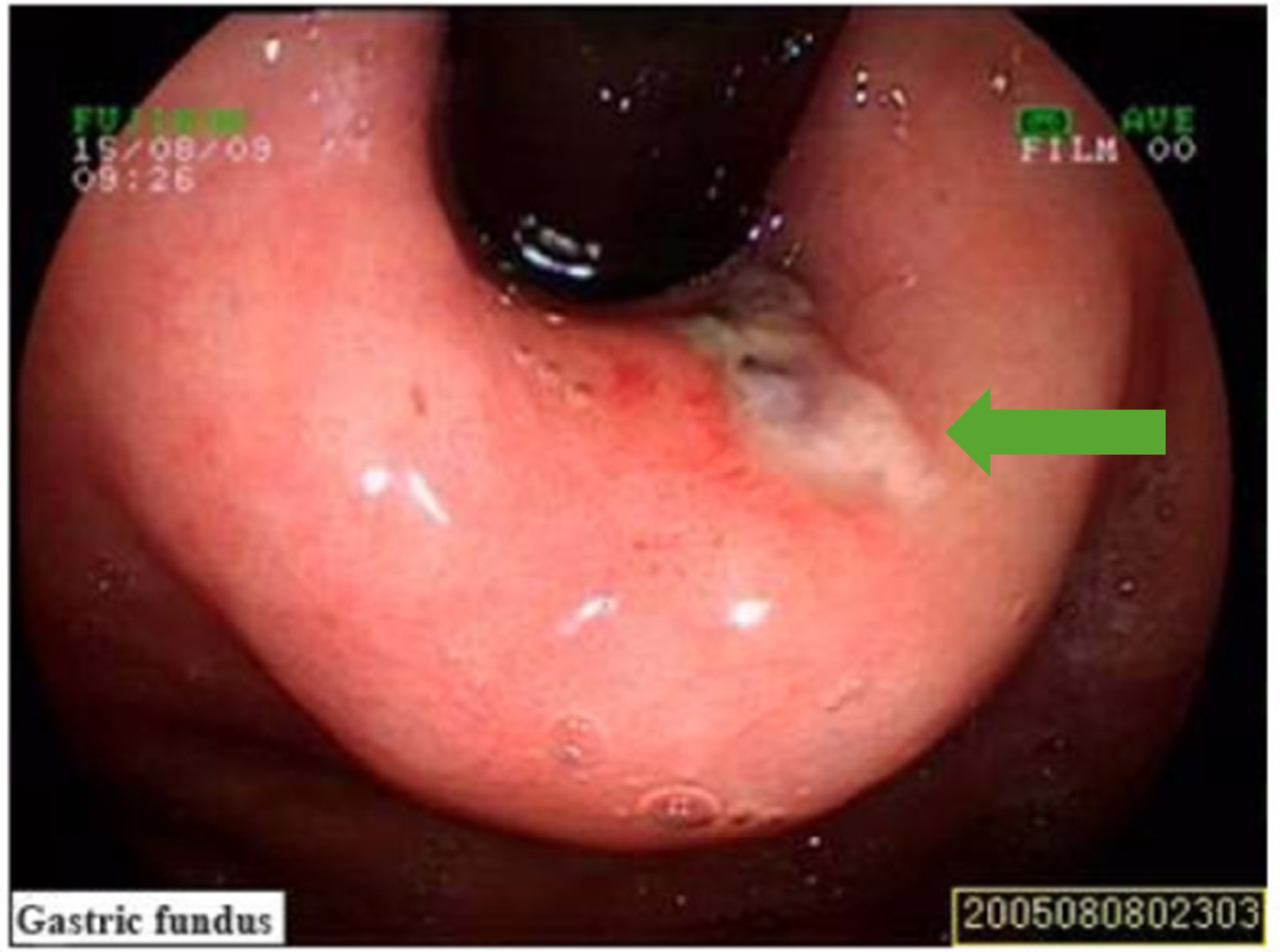
Definitive diagnosis is with upper GI endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD):
Mallory-Weiss tear (green arrow) as visualized on esophagogastroduodenoscopy (EGD)
Image: “Mallory-Weiss syndrome” by Zhao Y, Wang L, Si J. License: CC BY 3.0, edited by Lecturio.
Supporting workup[6,7]
CBC:
Assess baseline hemoglobin and hematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia at time of presentation (useful when there is trending anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types during the hospital stay).
Evaluate for thrombocytopeniaThrombocytopeniaThrombocytopenia occurs when the platelet count is < 150,000 per microliter. The normal range for platelets is usually 150,000-450,000/µL of whole blood. Thrombocytopenia can be a result of decreased production, increased destruction, or splenic sequestration of platelets. Patients are often asymptomatic until platelet counts are < 50,000/µL. Thrombocytopenia.
Coagulation studiesCoagulation studiesCoagulation studies are a group of hematologic laboratory studies that reflect the function of blood vessels, platelets, and coagulation factors, which all interact with one another to achieve hemostasis. Coagulation studies are usually ordered to evaluate patients with bleeding or hypercoagulation disorders.Coagulation Studies → assess for coagulopathy
Blood type and screen → in case transfusion is needed
Troponin → often measured to assess for myocardial ischemiaMyocardial ischemiaA disorder of cardiac function caused by insufficient blood flow to the muscle tissue of the heart. The decreased blood flow may be due to narrowing of the coronary arteries (coronary artery disease), to obstruction by a thrombus (coronary thrombosis), or less commonly, to diffuse narrowing of arterioles and other small vessels within the heart.Coronary Heart Disease
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) → done to assess for myocardial ischemiaMyocardial ischemiaA disorder of cardiac function caused by insufficient blood flow to the muscle tissue of the heart. The decreased blood flow may be due to narrowing of the coronary arteries (coronary artery disease), to obstruction by a thrombus (coronary thrombosis), or less commonly, to diffuse narrowing of arterioles and other small vessels within the heart.Coronary Heart Disease
Risk assessmentRisk assessmentThe qualitative or quantitative estimation of the likelihood of adverse effects that may result from exposure to specified health hazards or from the absence of beneficial influences.Preoperative Care:
Helps determine patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship‘ risk of rebleeding and mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate
Full score requires a completed endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD).
Helps assess adult patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who need urgent endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) and those who can be discharged for outpatient follow-up
Low-risk scores indicate outpatient management.
GBSGBSAn acute inflammatory autoimmune neuritis caused by t cell- mediated cellular immune response directed towards peripheral myelin. Demyelination occurs in peripheral nerves and nerve roots. The process is often preceded by a viral or bacterial infection, surgery, immunization, lymphoma, or exposure to toxins. Common clinical manifestations include progressive weakness, loss of sensation, and loss of deep tendon reflexes. Weakness of respiratory muscles and autonomic dysfunction may occur.Polyneuropathy score of ≥2 indicates high risk, thus admission and an esophagogastroduodenoscopy within 24 hours are recommended.
Management guidelines may vary depending on practice location. The following information is based on US and European literature and guidelines.
The initial management of any patient with upper GI bleeding requires IV fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome and stabilizing the patient hemodynamically.
Acute management[5,9,10]
Assess hemodynamic stability and administer IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids.
About 40%–70% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require transfusion.
Transfusion thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction may vary, depending on:[5]
Underlying cardiovascular disease and evidence of tissue hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage
Hemodynamic instability
Severity of bleeding
Symptoms of anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
Esomeprazole IV 40 mg every 12 hours initially, OR
PantoprazolePantoprazole2-pyridinylmethylsulfinylbenzimidazole proton pump inhibitor that is used in the treatment of gastroesophageal reflux and peptic ulcer.Gastric Acid Drugs IV 40 mg every 12 hours
A bolus + continuous infusion may also be considered.
Subsequent dosing depends on endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) findings.
Consider prokinetic agents prior to endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) to allow improved gastric visualization (by clearing blood/clots):[9]
ErythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides IV 250 mg over 20–30 minutes (preferred)
Suggested to give 20–90 minutes prior to endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)
Monitor for QTc prolongation
Because this is a CYP450 3A inhibitor, caution should be used with regard to drug interactions.
Alternative: metoclopramideMetoclopramideA dopamine d2 antagonist that is used as an antiemetic.Antiemetics IV 10 to 20 mg slow infusion
Consider antiemetic therapy for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with ongoing nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and/or vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) within 12 hours, if ongoing active bleeding suspected
With no active bleeding at time of endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD), manage with PPIs alone if:
No risk factors for rebleeding (e.g., portal hypertensionPortal hypertensionPortal hypertension is increased pressure in the portal venous system. This increased pressure can lead to splanchnic vasodilation, collateral blood flow through portosystemic anastomoses, and increased hydrostatic pressure. There are a number of etiologies, including cirrhosis, right-sided congestive heart failure, schistosomiasis, portal vein thrombosis, hepatitis, and Budd-Chiari syndrome. Portal Hypertension, coagulopathy)
No clinical features of severe bleeding (e.g., hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension, hematocheziaHematocheziaGastrointestinal Bleeding)
If continued active bleeding:
Endoscopic therapy with thermal coagulation, endoscopic clips, or endoscopic band ligationBand ligationMallory-Weiss Syndrome (Mallory-Weiss Tear) (with or without epinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs injection)
Arteriography with embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding if endoscopic interventions fail; vasopressin infusion used if embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding is not possible[2]
Surgery if angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery fails
Indications for hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium[5,6]
Risk factors for recurrent bleeding:
Active bleeding at time of endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)
Portal hypertensionPortal hypertensionPortal hypertension is increased pressure in the portal venous system. This increased pressure can lead to splanchnic vasodilation, collateral blood flow through portosystemic anastomoses, and increased hydrostatic pressure. There are a number of etiologies, including cirrhosis, right-sided congestive heart failure, schistosomiasis, portal vein thrombosis, hepatitis, and Budd-Chiari syndrome. Portal Hypertension
Coagulopathy
Endoscopic evidence of recent bleeding: visible vessel or adherent clot
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
Bleeding stops spontaneously in 80%–90% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship[7]
Rebleeding: ~ 7%; may be seen in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with coagulopathiesCoagulopathiesHemothorax
Mallory-Weiss tears heal rapidly in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship without portal hypertensionPortal hypertensionPortal hypertension is increased pressure in the portal venous system. This increased pressure can lead to splanchnic vasodilation, collateral blood flow through portosystemic anastomoses, and increased hydrostatic pressure. There are a number of etiologies, including cirrhosis, right-sided congestive heart failure, schistosomiasis, portal vein thrombosis, hepatitis, and Budd-Chiari syndrome. Portal Hypertension.
MortalityMortalityAll deaths reported in a given population.Measures of Health Status rate: ~ 5% in older patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with coexisting medical conditions[3]
Discharge medications[6,9]
Discharge on standard-dose PPI for 8 weeks, if no risk factors for rebleeding:
OmeprazoleOmeprazoleA 4-methoxy-3, 5-dimethylpyridyl, 5-methoxybenzimidazole derivative of timoprazole that is used in the therapy of stomach ulcers and zollinger-ellison syndrome. The drug inhibits an h(+)-k(+)-exchanging ATPase which is found in gastric parietal cells.Gastric Acid Drugs 20 mg (oral) daily, OR
Esomeprazole 20 mg daily, OR
PantoprazolePantoprazole2-pyridinylmethylsulfinylbenzimidazole proton pump inhibitor that is used in the treatment of gastroesophageal reflux and peptic ulcer.Gastric Acid Drugs 40 mg daily, OR
LansoprazoleLansoprazoleA 2, 2, 2-trifluoroethoxypyridyl derivative of timoprazole that is used in the therapy of stomach ulcers and zollinger-ellison syndrome. The drug inhibits h(+)-k(+)-exchanging ATPase which is found in gastric parietal cells. Lansoprazole is a racemic mixture of (r)- and (s)-isomers.Gastric Acid Drugs 30 mg daily
Differential Diagnosis
Boerhaave syndromeBoerhaave SyndromeEsophageal Perforation: perforated esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy resulting from a full-thickness tear, which requires immediate surgery to lessen the risk of mediastinitisMediastinitisMediastinitis refers to an infection or inflammation involving the mediastinum (a region in the thoracic cavity containing the heart, thymus gland, portions of the esophagus, and trachea). Acute mediastinitis can be caused by bacterial infection due to direct contamination, hematogenous or lymphatic spread, or extension of infection from nearby structures. Mediastinitis and sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock. The pathogenic mechanism is identical to that of MWSMWSMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear) (sudden increased intraluminal esophageal pressure due to forceful vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia or retching). Symptoms may include subcutaneous emphysemaSubcutaneous emphysemaPresence of air or gas in the subcutaneous tissues of the body.Mallory-Weiss Syndrome (Mallory-Weiss Tear) with crepitusCrepitusOsteoarthritis on examination, pneumomediastinumPneumomediastinumMediastinitis, odynophagiaOdynophagiaEpiglottitis, and dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea.
Esophageal varices: may present with a life-threatening GI bleed. Occurs secondary to portal hypertensionPortal hypertensionPortal hypertension is increased pressure in the portal venous system. This increased pressure can lead to splanchnic vasodilation, collateral blood flow through portosystemic anastomoses, and increased hydrostatic pressure. There are a number of etiologies, including cirrhosis, right-sided congestive heart failure, schistosomiasis, portal vein thrombosis, hepatitis, and Budd-Chiari syndrome. Portal Hypertension, usually caused by cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis. May coexist with MWSMWSMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear).
Billing and Coding
Diagnosis Codes:
This code is used to diagnose Mallory-Weiss syndromeMallory-Weiss SyndromeMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear), which is a longitudinal tear in the mucous membraneMucous membraneAn epithelium with mucus-secreting cells, such as goblet cells. It forms the lining of many body cavities, such as the digestive tract, the respiratory tract, and the reproductive tract. Mucosa, rich in blood and lymph vessels, comprises an inner epithelium, a middle layer (lamina propria) of loose connective tissue, and an outer layer (muscularis mucosae) of smooth muscle cells that separates the mucosa from submucosa.Barrett Esophagus of the esophagogastric junctionEsophagogastric junctionThe area covering the terminal portion of esophagus and the beginning of stomach at the cardiac orifice.Esophagus: Anatomy, typically caused by forceful retching or vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia.
Coding System
Code
Description
ICD-10-CM
K22.6
Gastro-esophageal laceration-hemorrhage syndrome
SNOMED CT
235650000
Mallory-Weiss syndromeMallory-Weiss SyndromeMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear) (disorder)
Evaluation & Workup:
This CPT code is for an upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) (EGD), which is the definitive diagnostic procedure. It allows for direct visualization of the tear and assessment for active bleeding.
Coding System
Code
Description
CPT
43235
Upper gastrointestinal endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD), including esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy, stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, and either the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy and/or jejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy as appropriate; diagnostic
Procedures/Interventions:
This code is used when therapeutic intervention is required during endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) to stop active bleeding from the tear, such as the application of hemoclips or thermal coagulation.
Coding System
Code
Description
CPT
43255
Upper gastrointestinal endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)…; with control of bleeding (eg, injection, bipolarBipolarNervous System: Histology cautery, unipolarUnipolarNervous System: Histology cautery, laser, heater probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography), stapler, plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products coagulator)
Medications:
This code is for proton pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols inhibitors (PPIs) like omeprazoleOmeprazoleA 4-methoxy-3, 5-dimethylpyridyl, 5-methoxybenzimidazole derivative of timoprazole that is used in the therapy of stomach ulcers and zollinger-ellison syndrome. The drug inhibits an h(+)-k(+)-exchanging ATPase which is found in gastric parietal cells.Gastric Acid Drugs, which are used to reduce stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy acid and promote healing of the tear after bleeding has been controlled.
Coding System
Code
Description
RxNorm
7646
OmeprazoleOmeprazoleA 4-methoxy-3, 5-dimethylpyridyl, 5-methoxybenzimidazole derivative of timoprazole that is used in the therapy of stomach ulcers and zollinger-ellison syndrome. The drug inhibits an h(+)-k(+)-exchanging ATPase which is found in gastric parietal cells.Gastric Acid Drugs (ingredient)
ATC
A02BC01
OmeprazoleOmeprazoleA 4-methoxy-3, 5-dimethylpyridyl, 5-methoxybenzimidazole derivative of timoprazole that is used in the therapy of stomach ulcers and zollinger-ellison syndrome. The drug inhibits an h(+)-k(+)-exchanging ATPase which is found in gastric parietal cells.Gastric Acid Drugs
References
Falk, G. W. & Katzka, D. A. (2019). Diseases of the esophagus. Chapter 129 of Crow, M.K., et al. (Eds.), Goldman-Cecil Medicine, 26th ed., vol 1, pp. 860–870.
Alrashidi, I., Kim, T.H., Shin, J.H., Alreshidi, M., Park, M., & Jang, E.B. (2021). Efficacy and safety of transcatheter arterial embolization for active arterial esophageal bleeding: a single-center experience. Diagnostic and Interventional Radiology 27(4):519–523. doi: 10.5152/dir.2021.20253
Ljubičić, N., Budimir, I., et al. (2014). Mortality in high-risk patients with bleeding Mallory-Weiss syndrome is similar to that of peptic ulcer bleeding: results of a prospective database study. Scandinavian Journal of Gastroenterology 49(4):458–464. doi: 10.3109/00365521.2013.846404
Kortas, D.Y., Haas, L.S., et al. (2001). Mallory-Weiss tear: predisposing factors and predictors of a complicated course. American Journal of Gastroenterology 96(10):2863–2965. https://pubmed.ncbi.nlm.nih.gov/11693318/
Barkun, A.N., Bardou, M., et al. (2010). International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Annals of internal medicine, 152(2), 101-13. doi: 10.7326/0003-4819-152-2-201001190-00009