Menopause is a physiologic process in women characterized by the permanent cessation of menstruationMenstruationThe periodic shedding of the endometrium and associated menstrual bleeding in the menstrual cycle of humans and primates. Menstruation is due to the decline in circulating progesterone, and occurs at the late luteal phase when luteolysis of the corpus luteum takes place.Menstrual Cycle that occurs after the loss of ovarian activity. Menopause can only be diagnosed retrospectively, after 12 months without menstrual bleeding. During the menopausal transition, reproductive hormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types can fluctuate significantly, leading to symptoms that include hot flushesHot FlushesPrimary Ovarian Insufficiency, sleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep and mood disturbances, and vaginal dryness. In postmenopausal woman, low estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy levels contribute to an increased risk for cardiovascular disease, osteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis, and sexual dysfunctionSexual dysfunctionPhysiological disturbances in normal sexual performance in either the male or the female.Sexual Physiology due to vulvovaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation. For some women, symptoms negatively affect their qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life and treatment is warranted. Management usually involves menopausal hormone therapy (MHT), but other treatment options also exist.
Menopause is the permanent physiologic cessation of mensesMensesThe periodic shedding of the endometrium and associated menstrual bleeding in the menstrual cycle of humans and primates. Menstruation is due to the decline in circulating progesterone, and occurs at the late luteal phase when luteolysis of the corpus luteum takes place.Menstrual Cycle due to loss of ovarian activity determined retrospectively after 12 consecutive months of no menstrual bleeding and low estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy levels.
Epidemiology
Average age: 51 years
Typical range: 44–55 years of age (95% of women)
Abnormal < 40 years of age: primary ovarian insufficiencyPrimary ovarian insufficiencyCessation of ovarian function after menarche but before the age of 40, without or with ovarian follicle depletion. It is characterized by the presence of oligomenorrhea or amenorrhea, elevated gonadotropins, and low estradiol levels. It is a state of female hypergonadotropic hypogonadism. Etiologies include genetic defects, autoimmune processes, chemotherapy, radiation, and infections. The most commonly known genetic cause is the expansion of a cgg repeat to 55 to 199 copies in the 5′ untranslated region in the X-linked fmr1 gene.Primary Ovarian Insufficiency
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Reproductive history
ChemotherapyChemotherapyOsteosarcoma or pelvic radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Hysterectomy with ovarian conservation → post-surgical impairment in blood supply
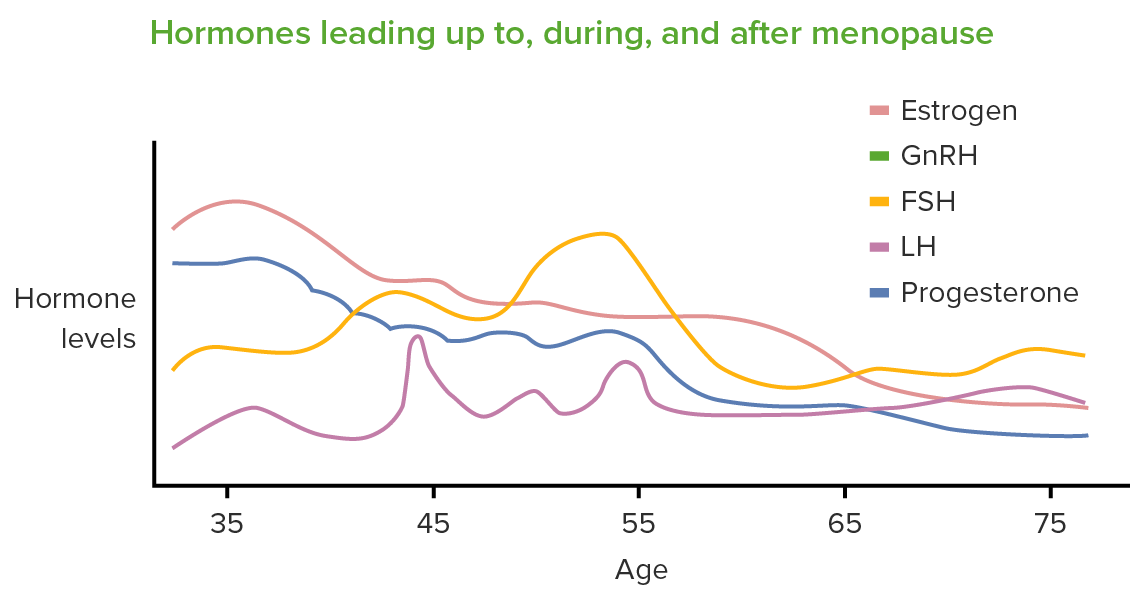
Menopause is characterized by a physiologic ↓ in oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy due to progressive atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS), ultimately leading to a chronic hypoestrogenic state in postmenopause. During the menopause transition, hormone levels fluctuate significantly.
The primary hormonal changes seen in perimenopause/menopause are a decrease in estrogen and progesterone and an increase in follicle-stimulating hormone (FSH) and luteinizing hormone (LH). GnRH: gonadotropin-releasing hormone
Image by Lecturio.
Physiology of menopause transition
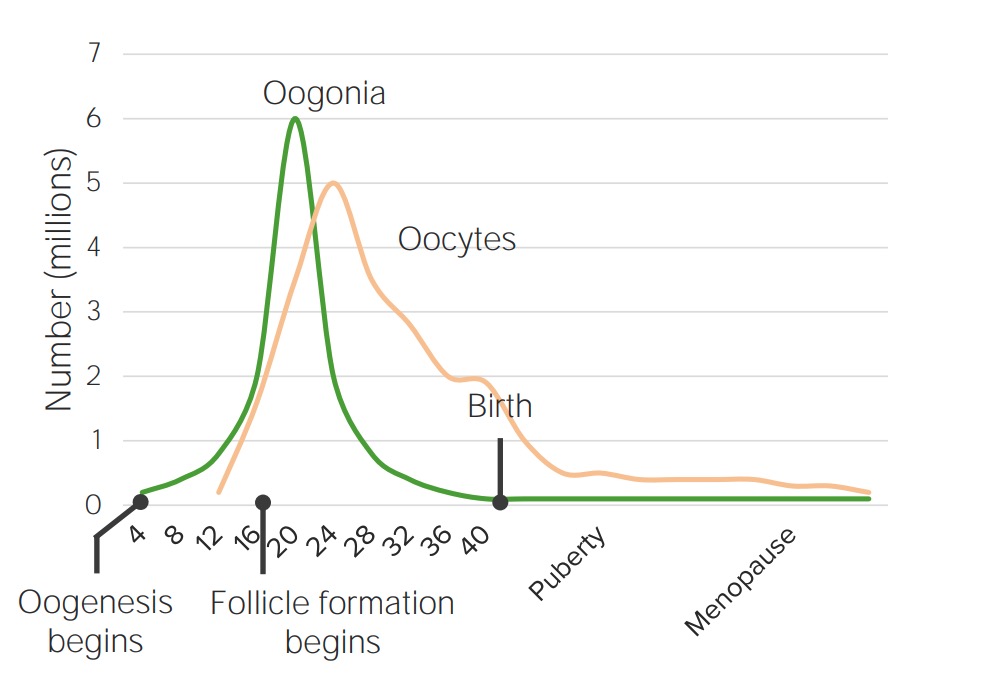
Normal oocyte counts:
At birth: 1–2 million oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy
At pubertyPubertyPuberty is a complex series of physical, psychosocial, and cognitive transitions usually experienced by adolescents (11-19 years of age). Puberty is marked by a growth in stature and the development of secondary sexual characteristics, achievement of fertility, and changes in most body systems.Puberty: 400,000 oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy
At age 30–35: 100,000 oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy
At menopause: < 1,000 oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy
Effects of estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy:
Inhibits release of FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle
Endometrial stimulation
Vaginal lubrication
Breast growth
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types growth
Modulating effects on thermoregulationThermoregulationBody temperature can be divided into external temperature, which involves the skin, and core temperature, which involves the CNS and viscera. While external temperature can be variable, the core temperature is maintained within a narrow range of 36.5-37.5ºC (97.7-99.5ºF).Body Temperature Regulation and mood
Late reproductive years/early menopause transition:
Perimenopause:
Transitional period from reproductive to non-reproductive stage
Characterized by increasing menstrual irregularity and fluctuating hormone levels
↓ OocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy → ↓ estrogens → ↓ inhibition of FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle → ↑ FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle → ↑ follicular response → ↑ estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy (mid-cycle)
Significant fluctuations in estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy throughout cycle
Severely depleted follicle supply → more anovulatory cycles
↓ OocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy → ↓ estrogens → ↓ inhibition of FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle → ↑ FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle → ↓ qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of oocytesOocytesFemale germ cells derived from oogonia and termed oocytes when they enter meiosis. The primary oocytes begin meiosis but are arrested at the diplotene state until ovulation at puberty to give rise to haploid secondary oocytes or ova (ovum).Ovaries: Anatomy are unable to respond → estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy stays ↓
Primary estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy switches from estradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins (E2) to estroneEstroneAn aromatized C18 steroid with a 3-hydroxyl group and a 17-ketone, a major mammalian estrogen. It is converted from androstenedione directly, or from testosterone via estradiol. In humans, it is produced primarily by the cyclic ovaries, placenta, and the adipose tissue of men and postmenopausal women.Noncontraceptive Estrogen and Progestins (E1E1An aromatized C18 steroid with a 3-hydroxyl group and a 17-ketone, a major mammalian estrogen. It is converted from androstenedione directly, or from testosterone via estradiol. In humans, it is produced primarily by the cyclic ovaries, placenta, and the adipose tissue of men and postmenopausal women.Noncontraceptive Estrogen and Progestins):
E2:
Primary estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy in premenopausal women
Produced in ovariesOvariesOvaries are the paired gonads of the female reproductive system that contain haploid gametes known as oocytes. The ovaries are located intraperitoneally in the pelvis, just posterior to the broad ligament, and are connected to the pelvic sidewall and to the uterus by ligaments. These organs function to secrete hormones (estrogen and progesterone) and to produce the female germ cells (oocytes).Ovaries: Anatomy
↓ Significantly at menopause
E1E1An aromatized C18 steroid with a 3-hydroxyl group and a 17-ketone, a major mammalian estrogen. It is converted from androstenedione directly, or from testosterone via estradiol. In humans, it is produced primarily by the cyclic ovaries, placenta, and the adipose tissue of men and postmenopausal women.Noncontraceptive Estrogen and Progestins:
Primary estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy in postmenopausal women
Produced primarily in adipose tissueAdipose tissueAdipose tissue is a specialized type of connective tissue that has both structural and highly complex metabolic functions, including energy storage, glucose homeostasis, and a multitude of endocrine capabilities. There are three types of adipose tissue, white adipose tissue, brown adipose tissue, and beige or “brite” adipose tissue, which is a transitional form.Adipose Tissue: Histology
Oocyte counts over lifespan of a woman:
Oogenesis is mostly completed by birth and viable oocyte counts continue to decrease through a woman’s life.
Image by Lecturio.
Other hormonal changes in perimenopause
Table: Other hormonal changes in perimenopause
Hormone
Change
Explanation
Anti-Müllerian hormone (AMHAMHA glycoprotein that causes regression of mullerian ducts. It is produced by sertoli cells of the testes. In the absence of this hormone, the mullerian ducts develop into structures of the female reproductive tract. In males, defects of this hormone result in persistent mullerian duct, a form of male pseudohermaphroditism.Primary Amenorrhea)
↓
Secreted by prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis follicles
Inhibits FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual CyclesecretionSecretionCoagulation Studies
May begin to ↓ around age 35 (earliest measurable marker) → ↑ FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle
LHLHA major gonadotropin secreted by the adenohypophysis. Luteinizing hormone regulates steroid production by the interstitial cells of the testis and the ovary. The preovulatory luteinizing hormone surge in females induces ovulation, and subsequent luteinization of the follicle. Luteinizing hormone consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle and FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle
↑
Inhibin B has an inhibitory effect on LHLHA major gonadotropin secreted by the adenohypophysis. Luteinizing hormone regulates steroid production by the interstitial cells of the testis and the ovary. The preovulatory luteinizing hormone surge in females induces ovulation, and subsequent luteinization of the follicle. Luteinizing hormone consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle and FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle, so during menopause their levels increase.
TestosteroneTestosteroneA potent androgenic steroid and major product secreted by the leydig cells of the testis. Its production is stimulated by luteinizing hormone from the pituitary gland. In turn, testosterone exerts feedback control of the pituitary LH and FSH secretion. Depending on the tissues, testosterone can be further converted to dihydrotestosterone or estradiol.Androgens and Antiandrogens
↓
Primary source of production shifts from ovariesOvariesOvaries are the paired gonads of the female reproductive system that contain haploid gametes known as oocytes. The ovaries are located intraperitoneally in the pelvis, just posterior to the broad ligament, and are connected to the pelvic sidewall and to the uterus by ligaments. These organs function to secrete hormones (estrogen and progesterone) and to produce the female germ cells (oocytes).Ovaries: Anatomy to adrenals.
HypoplasiaHypoplasiaHypoplastic Left Heart Syndrome (HLHS) of adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy leads to a 25% decrease in testosteroneTestosteroneA potent androgenic steroid and major product secreted by the leydig cells of the testis. Its production is stimulated by luteinizing hormone from the pituitary gland. In turn, testosterone exerts feedback control of the pituitary LH and FSH secretion. Depending on the tissues, testosterone can be further converted to dihydrotestosterone or estradiol.Androgens and Antiandrogens.
Clinical Presentation
The clinical symptoms of perimenopause are caused by fluctuating hormone levels in the menopause transition period. The presentation of postmenopause results from the low estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy levels that ensue after cessation of ovarian function, which persist for the remainder of a woman’s life.
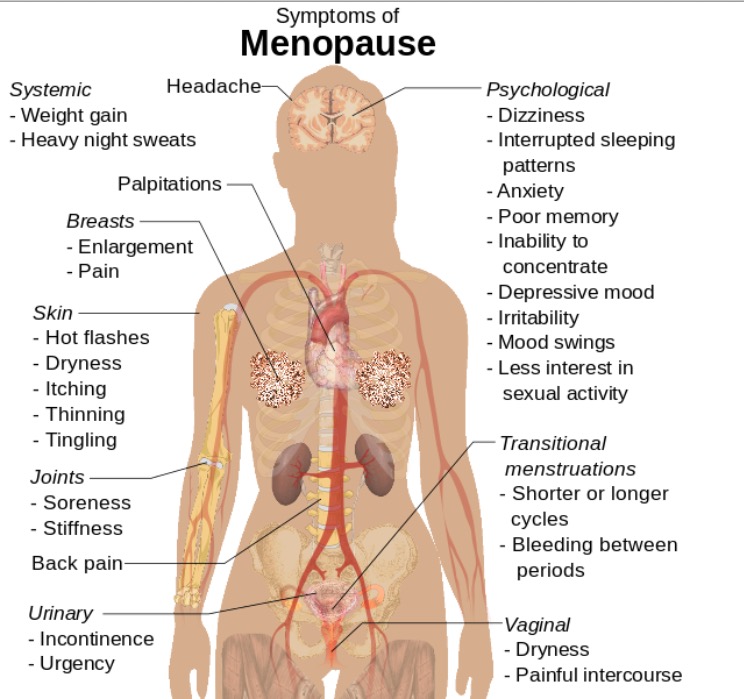
Symptoms of menopause that can also be seen in primary ovarian insufficiency
Image: “Symptoms of menopause” by Mikael Häggström. License: CC0
Symptoms associated with perimenopause
Menstrual changes:
Late reproductive years: Menstrual cycles shorten (cycles get closer).
Menopausal transition: shorter cycles → longer cycles → very irregular/sporadicSporadicSelective IgA Deficiency cycles → final menstrual period
Stress and anxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder
Symptoms related to sexual function:
Genitourinary syndrome of menopause (GSM): vulvovaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation (the physical changes of vulvaVulvaThe vulva is the external genitalia of the female and includes the mons pubis, labia majora, labia minora, clitoris, vestibule, vestibular bulb, and greater vestibular glands. Vagina, Vulva, and Pelvic Floor: Anatomy, vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, and lower urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy due to estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy deficiency)
Vaginal dryness and itching
DyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency
Symptoms and conditions associated with postmenopause
These symptoms are a result of long-term estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy deficiency:
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types loss:
OsteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis
Fragility fracturesFragility fracturesPelvic fractures are a disruption in the cortex of a pelvic bone involving iliac wing fractures, acetabular fractures, or those causing loss of integrity of the pelvic ring (the sacrum and the 2 innominate bones). Patients often present with a history of trauma or a fall, limb length discrepancy, intense pain on palpation, and mechanical instability.Pelvic Fractures
Cardiovascular disease:
Lipid profiles worsen (↑cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism).
Weight gain
↑ Risk for myocardial infarctionMyocardial infarctionMI is ischemia and death of an area of myocardial tissue due to insufficient blood flow and oxygenation, usually from thrombus formation on a ruptured atherosclerotic plaque in the epicardial arteries. Clinical presentation is most commonly with chest pain, but women and patients with diabetes may have atypical symptoms.Myocardial Infarction and thromboembolic events
Hair, muscle, and skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions changes:
Hair thins.
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions becomes drier and rougher.
Dryness/dyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency
↑ Risk of pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse
Incontinence issues
↑ Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (UTIs)
Pelvic exam: Assess vaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation in context of sexual complaints.
Routine lab evaluation not indicated:
FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle, LHLHA major gonadotropin secreted by the adenohypophysis. Luteinizing hormone regulates steroid production by the interstitial cells of the testis and the ovary. The preovulatory luteinizing hormone surge in females induces ovulation, and subsequent luteinization of the follicle. Luteinizing hormone consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle, and estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy levels fluctuate significantly and are not clinically useful in most cases.
Exception: if patient is around age of menopause with abnormal bleeding, ↑ FSHFSHA major gonadotropin secreted by the adenohypophysis. Follicle-stimulating hormone stimulates gametogenesis and the supporting cells such as the ovarian granulosa cells, the testicular sertoli cells, and leydig cells. Fsh consists of two noncovalently linked subunits, alpha and beta. Within a species, the alpha subunit is common in the three pituitary glycoprotein hormones (TSH, LH, and FSH), but the beta subunit is unique and confers its biological specificity.Menstrual Cycle may be helpful in clarifying menopausal status
Abnormal uterine bleedingAbnormal Uterine BleedingAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym PALM-COEIN, with PALM representing the structural causes and COEIN indicating the non-structural causes. Abnormal Uterine Bleeding should be evaluated:
Endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation/cancer
Leiomyomas
Polyps
AdenomyosisAdenomyosisAdenomyosis is a benign uterine condition characterized by the presence of ectopic endometrial glands and stroma within the myometrium. Adenomyosis is a common condition, affecting 20%-35% of women, and typically presents with heavy menstrual bleeding and dysmenorrhea. Adenomyosis
Ovulatory dysfunction from other causes
Management
A majority of women in perimenopause and postmenopause do not require treatment. The primary goals of management are relief of bothersome symptoms and ensuring health through appropriate screeningScreeningPreoperative Care.
Menopausal hormone therapy (MHT)
EstrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy therapy (ET):
GSM: vaginal dryness, dyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency
SelectionSelectionLymphocyte activation by a specific antigen thus triggering clonal expansion of lymphocytes already capable of mounting an immune response to the antigen.B cells: Types and Functions of route and dosing:
Give continuously.
Transdermal is usually preferred for vasomotor symptoms.
Vaginal ET is preferred when treating GSM only.
EstrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy stimulates endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development → progestin required if patient has uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy
ProgestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives:
Higher risk of adverse events than estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy therapy
Required for endometrial protection in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy
SelectionSelectionLymphocyte activation by a specific antigen thus triggering clonal expansion of lymphocytes already capable of mounting an immune response to the antigen.B cells: Types and Functions of route and dosing:
Usually oral
Give cyclically if still menstruating regularly.
Give continuously if post-menopausal.
Candidates for therapy:
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship within 10 years of menopause
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship < 60–65 years of age
Symptoms severe enough to affect qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
No contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to MHT include history of:
Hormone-sensitive breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer
High-risk endometrial cancerEndometrial CancerEndometrial carcinoma (EC) is the most common gynecologic malignancy in the developed world, and it has several histologic types. Endometrioid carcinoma (known as type 1 EC) typically develops from atypical endometrial hyperplasia, is hormonally responsive, and carries a favorable prognosis.Endometrial Hyperplasia and Endometrial Cancer
Stroke or transient ischemic attackTransient ischemic attackTransient ischemic attack (TIA) is a temporary episode of neurologic dysfunction caused by ischemia without infarction that resolves completely when blood supply is restored. Transient ischemic attack is a neurologic emergency that warrants urgent medical attention. Transient Ischemic Attack (TIA) (TIATIATransient ischemic attack (TIA) is a temporary episode of neurologic dysfunction caused by ischemia without infarction that resolves completely when blood supply is restored. Transient ischemic attack is a neurologic emergency that warrants urgent medical attention. Transient Ischemic Attack (TIA))
Acute liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
General principles:
Use lowest dose for shortest duration required to treat symptoms.
Should not be used for prevention of chronic disease
Risks and benefits beyond symptom relief:
MHT ↑ risk of:
Breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer
GallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy disease
MHT ↓ risk of:
OsteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis
Colorectal cancerColorectal cancerColorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Colorectal Cancer
Selective estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: AnatomyreceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors modulators (SERMsSERMsA structurally diverse group of compounds distinguished from estrogens by their ability to bind and activate estrogen receptors but act as either an agonist or antagonist depending on the tissue type and hormonal milieu. They are classified as either first generation because they demonstrate estrogen agonist properties in the endometrium or second generation based on their patterns of tissue specificity.Antiestrogens):
Modulate effects of estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy
Different effects (agonist vs. antagonist) in different tissue types
Common examples:
RaloxifeneRaloxifeneA second generation selective estrogen receptor modulator (SERM) used to prevent osteoporosis in postmenopausal women. It has estrogen agonist effects on bone and cholesterol metabolism but behaves as a complete estrogen antagonist on mammary gland and uterine tissue.Other Antiresorptive Drugs (agonist in boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types, antagonist in breast and uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy)
GabapentinGabapentinA cyclohexane-gamma-aminobutyric acid derivative that is used for the treatment of partial seizures; neuralgia; and restless legs syndrome.Second-Generation Anticonvulsant Drugs
ClonidineClonidineAn imidazoline sympatholytic agent that stimulates alpha-2 adrenergic receptors and central imidazoline receptors. It is commonly used in the management of hypertension.Sympathomimetic Drugs
Botanical and herbal remedies: not shown to be effective in clinical trials
Lifestyle changes:
Layer clothing.
Maintain lower ambient temperature at home.
Avoid alcohol and caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants.
Stress management
Management options for GSM
Low-dose vaginal estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy:
Most effective treatment
Doses are low enough that progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives are not required for endometrial protection.
Vaginal lubricants
Vaginal moisturizers
RegularRegularInsulin sexual activity or use of dilators
Cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening
Up to age 65/every 3 years
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus testing
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types mineral density
At age 65/every 2 years if risk factors are present
Primary ovarian insufficiencyPrimary ovarian insufficiencyCessation of ovarian function after menarche but before the age of 40, without or with ovarian follicle depletion. It is characterized by the presence of oligomenorrhea or amenorrhea, elevated gonadotropins, and low estradiol levels. It is a state of female hypergonadotropic hypogonadism. Etiologies include genetic defects, autoimmune processes, chemotherapy, radiation, and infections. The most commonly known genetic cause is the expansion of a cgg repeat to 55 to 199 copies in the 5′ untranslated region in the X-linked fmr1 gene.Primary Ovarian Insufficiency (POI): a condition characterized by impaired ovarian function in women < 40 years of age. Symptoms are identical to menopause, including amenorrheaAmenorrheaAbsence of menstruation.Congenital Malformations of the Female Reproductive System, vasomotor symptoms, and vaginal dryness. The key difference is patient age. Menopause is a natural physiologic process, while POI is pathologic, and may be caused by genetic or chromosomal anomalies, an autoimmune process, or ovarian toxins. Management is with HRTHRTHormone replacement therapy (HRT) is used to treat symptoms associated with female menopause and in combination to suppress ovulation. Risks and side effects include uterine bleeding, predisposition to cancer, breast tenderness, hyperpigmentation, migraine headaches, hypertension, bloating, and mood changes.Noncontraceptive Estrogen and Progestins, addressing fertility concerns, and counseling.
Abnormal uterine bleedingAbnormal Uterine BleedingAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym PALM-COEIN, with PALM representing the structural causes and COEIN indicating the non-structural causes. Abnormal Uterine Bleeding (AUBAUBAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym palm-coein, with palm representing the structural causes and coein indicating the non-structural causes.Abnormal Uterine Bleeding): preferred term for uterine bleeding outside normal parameters, and includes heavy and irregular bleeding. Common causes include leiomyomas, polyps, endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation or malignancyMalignancyHemothorax, coagulopathy (especially in younger women), and ovulatory dysfunction. Diagnosis usually requires endometrial biopsyEndometrial BiopsyDiagnostic Procedures in Gynecology and pelvic ultrasound. Management depends on underlying etiology. Important to exclude pathologic causes of AUBAUBAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym palm-coein, with palm representing the structural causes and coein indicating the non-structural causes.Abnormal Uterine Bleeding in perimenopausal women.