Colorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Almost all cases of CRC are adenocarcinoma, and the majority of lesions come from the malignant transformation of an adenomatous polyp. Since most CRC cases are asymptomatic, screening colonoscopy or stool tests are generally recommended in patients ≥ 45 years of age. Along with screening, diagnosis is reached by colonoscopy, which allows visualization as well as tissue sampling. Treatment is primarily surgical, with chemotherapy reserved for advanced disease.
2nd most common cause of death due to cancer in the United States
In the United States, incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency and mortalityMortalityAll deaths reported in a given population.Measures of Health Status rates have been declining.
The majority are adenocarcinomas.
Most colorectal cancers (CRCs) arise from polyps (adenomatous or serrated).
Risk factors
Age ≥ 45 (94% of new CRC cases)
Hereditary syndromes:
Familial adenomatous polyposisFamilial Adenomatous PolyposisFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis (FAPFAPFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis)
Hereditary non-polyposis colorectal cancerHereditary non-polyposis colorectal cancerLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome (HNPCCHNPCCLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome) or Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome
Peutz-Jeghers syndromePeutz-Jeghers SyndromePeutz-Jeghers syndrome (PJS) is an autosomal-dominant inherited disorder characterized by GI polyps and mucocutaneous-pigmented macules. Peutz-Jeghers syndrome is 1 of the polyposis syndromes, a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract and associated with other extracolonic features.Peutz-Jeghers Syndrome (PJSPJSPeutz-Jeghers syndrome (PJS) is an autosomal-dominant inherited disorder characterized by GI polyps and mucocutaneous-pigmented macules. Peutz-Jeghers syndrome is 1 of the polyposis syndromes, a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract and associated with other extracolonic features.Peutz-Jeghers Syndrome)
MUTYH-associated polyposis (MAP): mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in the base excision repairBase excision repairDNA Repair MechanismsgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics mutY homolog
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy pathologies:
Abdominopelvic radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Conditions with increased insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin or insulin-like growth factor (e.g., diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, acromegalyAcromegalyA condition caused by prolonged exposure to excessive human growth hormone in adults. It is characterized by bony enlargement of the face; lower jaw (prognathism); hands; feet; head; and thorax. The most common etiology is a growth hormone-secreting pituitary adenoma.Acromegaly and Gigantism, obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity)
StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus gallolyticusbacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides
Renal transplantation
Lifestyle and social factors:
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases and alcohol consumption (> 4 drinks/day)
Diet (increased fat, red and processed meat, low fiber)
Abnormal tissue outgrowths arising from the colonic mucosa and extending into the lumen
Most common lesions from which CRC arises
Morphology:
Sessile: polyp without a stalk, with growth adjacent to the massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Pedunculated: polyp with a stalk
30% of the population has polyps by the age of 50.
Types of polyps:
Inflammatory polyps (non-neoplastic)
Hamartomatous polyps (↑ CRC risk if associated with PJSPJSPeutz-Jeghers syndrome (PJS) is an autosomal-dominant inherited disorder characterized by GI polyps and mucocutaneous-pigmented macules. Peutz-Jeghers syndrome is 1 of the polyposis syndromes, a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract and associated with other extracolonic features.Peutz-Jeghers Syndrome)
Adenomas with villous features (CRC risk > 3 times that of tubular adenomas) or high-grade dysplasia
Serrated polyps/adenomas
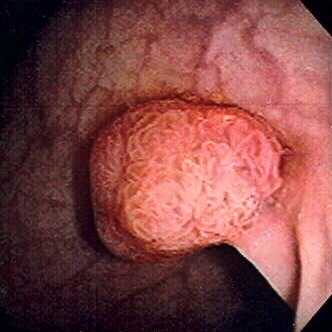
Polyp of sigmoid colon revealed by colonoscopy: The polyp is pedunculated (with a short stalk).
Image: “Colon polyp” by Dr. F.C. Turner. License: CC BY 2.5
Cancer development
Most polyps are benignBenignFibroadenoma. Malignant transformationTransformationChange brought about to an organism’s genetic composition by unidirectional transfer (transfection; transduction, genetic; conjugation, genetic, etc.) and incorporation of foreign DNA into prokaryotic or eukaryotic cells by recombination of part or all of that DNA into the cell’s genome.Bacteriology is affected by a series of mutations and environmental factors.
Mutations:
Germline mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations:
Occurs before fertilizationFertilizationTo undergo fertilization, the sperm enters the uterus, travels towards the ampulla of the fallopian tube, and encounters the oocyte. The zona pellucida (the outer layer of the oocyte) deteriorates along with the zygote, which travels towards the uterus and eventually forms a blastocyst, allowing for implantation to occur. Fertilization and First Week
Can be transmitted (from parent to offspring)
Found in the common inherited syndromes (e.g., FAPFAPFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis, Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome), which account for < 10% of CRCs
Spontaneous mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in sperm/ovum or zygoteZygoteThe fertilized ovum resulting from the fusion of a male and a female gamete.Fertilization and First Week
Parent does not have the mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations, but future offspring can inherit.
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis (adenomatous polyposis coliAdenomatous polyposis coliA polyposis syndrome due to an autosomal dominant mutation of the APC genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis) geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics:
Most CRCs begin with adenomatous polyposis coliAdenomatous polyposis coliA polyposis syndrome due to an autosomal dominant mutation of the APC genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis (APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis)geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics inactivation (either by germline or somatic mutationSomatic MutationNon-Hodgkin Lymphomas).
CRCs take 10–15 years to develop but can advance in a shorter time under certain conditions.
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis protein, encoded by APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous PolyposisgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics, promotes β-catenin degradation.
Without APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis protein:
β-catenin activates T cell factor (Tcf)–dependent transcriptionTranscriptionTranscription of genetic information is the first step in gene expression. Transcription is the process by which DNA is used as a template to make mRNA. This process is divided into 3 stages: initiation, elongation, and termination. Stages of Transcription of specific target genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure.
These genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure include MYC and cyclin D1Cyclin D1Protein encoded by the bcl-1 gene which plays a critical role in regulating the cell cycle. Overexpression of cyclin D1 is the result of bcl-1 rearrangement, a t(11; 14) translocation, and is implicated in various neoplasms.Non-Hodgkin Lymphomas (oncogenesOncogenesGenes whose gain-of-function alterations lead to neoplastic cell transformation. They include, for example, genes for activators or stimulators of cell proliferation such as growth factors, growth factor receptors, protein kinases, signal transducers, nuclear phosphoproteins, and transcription factors. A prefix of ‘v-‘ before oncogene symbols indicates oncogenes captured and transmitted by retroviruses; the prefix ‘c-‘ before the gene symbol of an oncogene indicates it is the cellular homolog (proto-oncogenes) of a v-oncogene.Carcinogenesis), which promote proliferation.
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis mutations: the initiating event for adenoma formation, but multiple genetic hits are required for CRC progression
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis
Adenomatous polyposis coliAdenomatous polyposis coliA polyposis syndrome due to an autosomal dominant mutation of the APC genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposisis an initial gene mutationGene MutationMyotonic Dystrophies.
Most adenomas and CRCs begin with APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous PolyposisgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics inactivation (either by germline or somatic mutationSomatic MutationNon-Hodgkin Lymphomas).
After the initiating event, CRCs take 10–15 years to develop (shorter time in certain conditions).
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis protein, encoded by APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous PolyposisgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics, promotes β-catenin degradation.
Without APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis protein:
β-catenin (of the WnT pathway) activates Tcf–dependent transcriptionTranscriptionTranscription of genetic information is the first step in gene expression. Transcription is the process by which DNA is used as a template to make mRNA. This process is divided into 3 stages: initiation, elongation, and termination. Stages of Transcription of specific target genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure.
These genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure include MYC and cyclin D1Cyclin D1Protein encoded by the bcl-1 gene which plays a critical role in regulating the cell cycle. Overexpression of cyclin D1 is the result of bcl-1 rearrangement, a t(11; 14) translocation, and is implicated in various neoplasms.Non-Hodgkin Lymphomas (oncogenesOncogenesGenes whose gain-of-function alterations lead to neoplastic cell transformation. They include, for example, genes for activators or stimulators of cell proliferation such as growth factors, growth factor receptors, protein kinases, signal transducers, nuclear phosphoproteins, and transcription factors. A prefix of ‘v-‘ before oncogene symbols indicates oncogenes captured and transmitted by retroviruses; the prefix ‘c-‘ before the gene symbol of an oncogene indicates it is the cellular homolog (proto-oncogenes) of a v-oncogene.Carcinogenesis), which promote proliferation.
Molecular mechanisms of tumorigenesis
Multiple genetic hits are required for CRC progression.
Accumulation of mutations and molecular events:
Accumulation of mutations and molecular events (e.g., genetic alteration, DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and StructuremethylationMethylationAddition of methyl groups. In histo-chemistry methylation is used to esterify carboxyl groups and remove sulfate groups by treating tissue sections with hot methanol in the presence of hydrochloric acid. .Glucocorticoids, overexpression) contributes to carcinogenesisCarcinogenesisThe origin, production or development of cancer through genotypic and phenotypic changes which upset the normal balance between cell proliferation and cell death. Carcinogenesis generally requires a constellation of steps, which may occur quickly or over a period of many years.Carcinogenesis.
Chromosomal instability (CIN):
Structural chromosomal aberrationschromosomal aberrationsAbnormal number or structure of chromosomes. Chromosome aberrations may result in chromosome disorders.Chromosome Testing (deletions or loss of heterozygosity)
Results in either promotion of oncogenesOncogenesGenes whose gain-of-function alterations lead to neoplastic cell transformation. They include, for example, genes for activators or stimulators of cell proliferation such as growth factors, growth factor receptors, protein kinases, signal transducers, nuclear phosphoproteins, and transcription factors. A prefix of ‘v-‘ before oncogene symbols indicates oncogenes captured and transmitted by retroviruses; the prefix ‘c-‘ before the gene symbol of an oncogene indicates it is the cellular homolog (proto-oncogenes) of a v-oncogene.Carcinogenesis or reduction of tumorTumorInflammation suppressor genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure (TSGs)
Seen in genetic alterations of APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous Polyposis
Other genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure: DCC, TP53/p53, and SMAD4 (tumorTumorInflammation suppressor genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure) or KRAS (a proto-oncogene)
85% of CRCs develop through this mechanism.
Microsatellite instability (MSI):
Also calledmutator phenotypePhenotypeThe complete genetic complement contained in the DNA of a set of chromosomes in a human. The length of the human genome is about 3 billion base pairs.Basic Terms of Genetics/mismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndrome pathway
Microsatellites: repeated,abnormal, short sequences of nucleotide basesBasesUsually a hydroxide of lithium, sodium, potassium, rubidium or cesium, but also the carbonates of these metals, ammonia, and the amines.Acid-Base Balance caused by mismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndrome deficiency
Cause: germline mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations of genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and StructureMLH1, MSH2, or PMS2 leading to dysfunctional DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structuremismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndrome (MMRMMRA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Excinucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndrome) enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes
Microsatellite accumulation: found in MSI-high (MSI-H) tumors
Biologic hallmark of Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome
CpG island methylator phenotypePhenotypeThe complete genetic complement contained in the DNA of a set of chromosomes in a human. The length of the human genome is about 3 billion base pairs.Basic Terms of Genetics (CIMP+) pathway:
DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure hypo- or hypermethylation can change geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics expression.
High methylationMethylationAddition of methyl groups. In histo-chemistry methylation is used to esterify carboxyl groups and remove sulfate groups by treating tissue sections with hot methanol in the presence of hydrochloric acid. .Glucocorticoids of CpG islands (cytosineCytosineA pyrimidine base that is a fundamental unit of nucleic acids.Nucleic Acids followed by a guanineGuanineNucleic Acids base, linked by phosphodiester bondPhosphodiester bondDNA Types and Structure) occurs in TSG.
MethylationMethylationAddition of methyl groups. In histo-chemistry methylation is used to esterify carboxyl groups and remove sulfate groups by treating tissue sections with hot methanol in the presence of hydrochloric acid. .Glucocorticoids inactivates TSG, leading to tumorTumorInflammation progression.
COX-2: overexpressed in 43% of adenomas and 86% of carcinomas
COX-2 inhibition reduces the number of intestinal polyps.
Morphologic mechanisms of tumorigenesis
Adenoma-carcinoma sequence:
Sequence followed by most CRCs
Progression: early adenoma (tubular or tubulovillous) → advanced adenoma (villous) → adenocarcinoma
Adenomatous polyps:
Develop with disrupted epithelial renewal
Replacement of surface cell lining becomes dysplastic as the adenomas increase in size.
APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous PolyposismutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations common
Associated molecular pathway(s): CIN
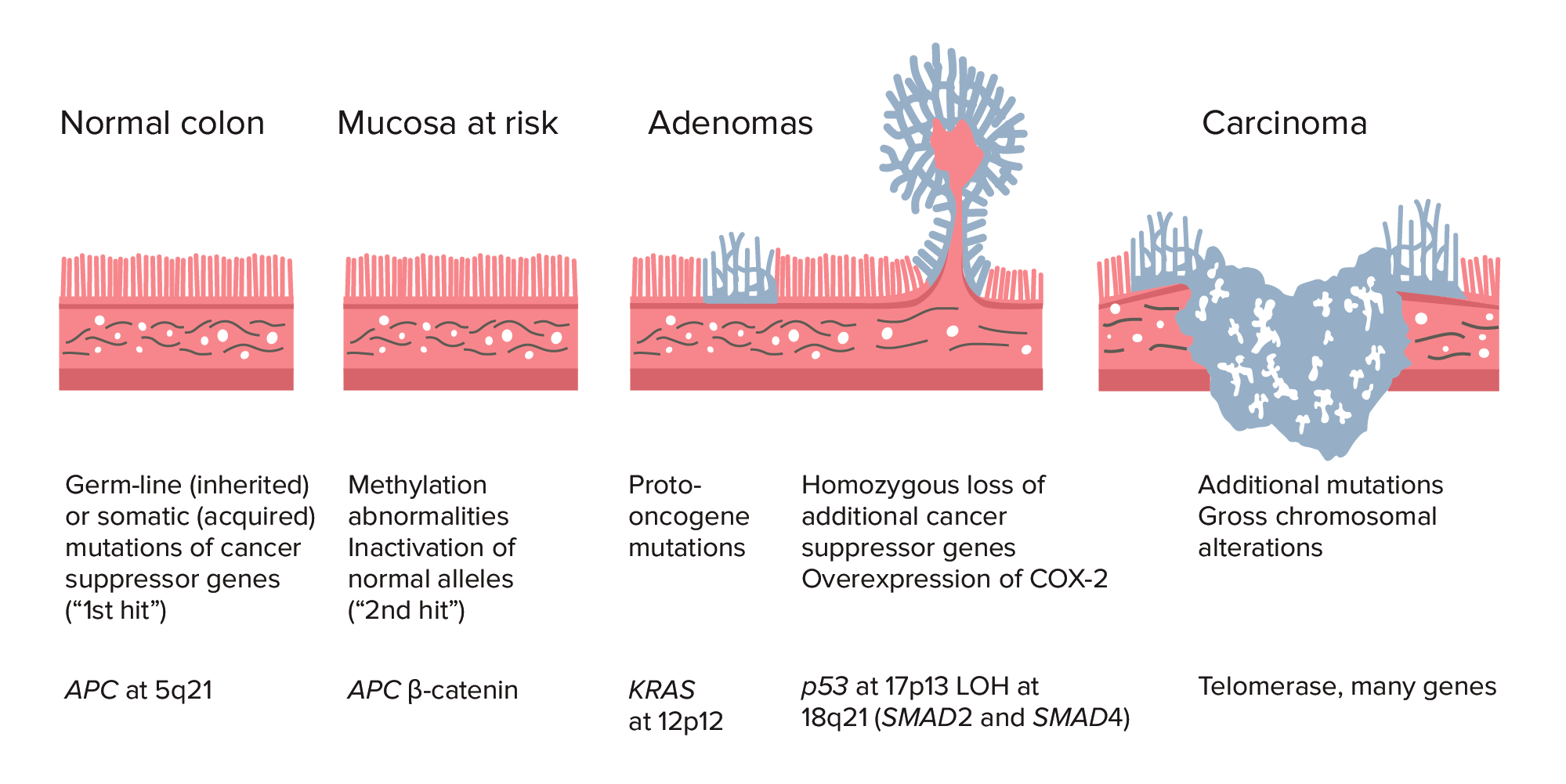
Adenoma–carcinoma sequence from normal colon to carcinoma: Colorectal cancer (CRC) formation begins with APC gene mutation (inherited or acquired) and methylation abnormalities. Other changes can include KRAS gene mutation. Late in the process, p53 deletion, loss of heterozygosity (LOH) at 18q21 (involving SMAD2 and SMAD4), with overexpression of COX-2 can contribute to further growth and progression to cancer. The accumulation of mutations, rather than the timing of occurrence, is most crucial in carcinogenesis.
BRAF oncogene activation with KRAS mutations noted
Associated molecular pathway/s:
CIMP (major mechanism that drives the serrated pathway toward CRC)
MSI
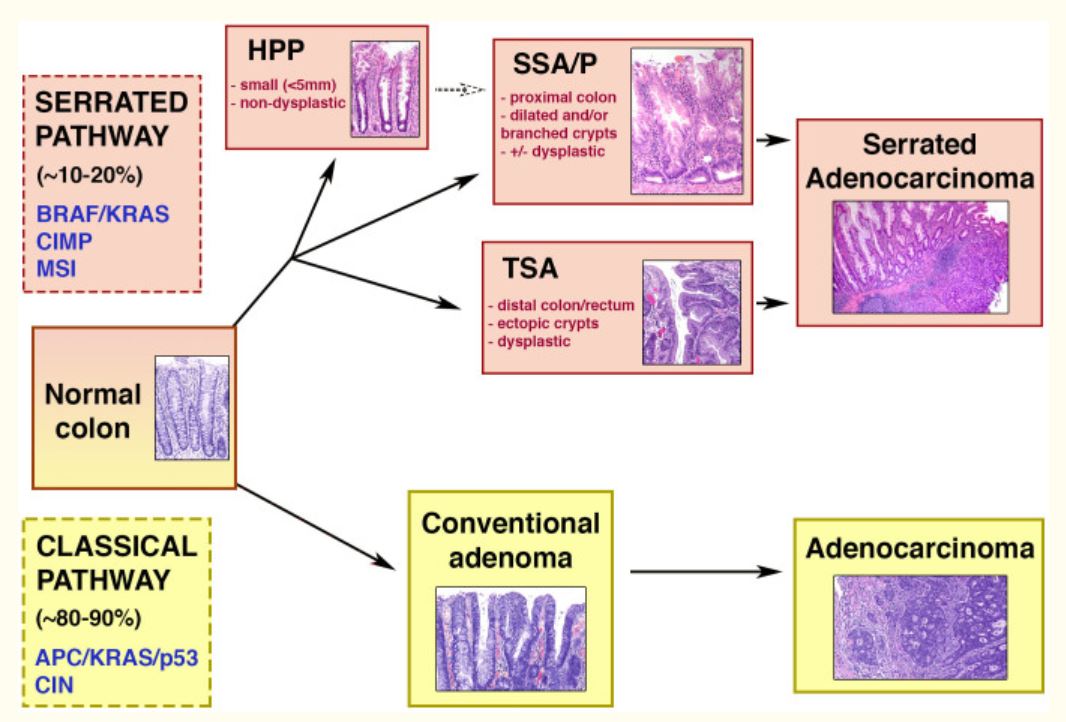
Schematic diagram of the classical (adenoma-carcinoma) and serrated pathways. Upper half: serrated pathway of colorectal carcinogenesis, occurring in 10%–20% of CRCs. The pathway is associated with the following genetic features: BRAF/KRAS mutations, MSI (microsatellite instability), and CIMP (CpG island methylator phenotype). Serrated lesions can be hyperplastic polyps (HPPs), sessile serrated adenomas/polyps (SSA/Ps), and traditional serrated adenomas (TSAs). The latter 2 are associated with dysplasia and progression to carcinoma. Lower half: adenoma-carcinoma or classical pathway, occurring in most CRCs. Among the genetic features include mutations in APC/KRAS/p53 genes and chromosomal instability (CIN). Through this sequence, adenoma becomes adenocarcinoma.
Image: “Schematic diagram of the classical (adenoma-carcinoma) and serrated pathways” by Centre for Tumor Biology, Barts Cancer Institute, Barts and the London School of Medicine and Dentistry, Queen Mary University of London, London, UK. License: CC BY 4.0
Systemic features: weakness, anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types, weight lossWeight lossDecrease in existing body weight.Bariatric Surgery
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements deficiency anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types in an elderly patient indicates colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy cancer until proven otherwise.
Dependent on location
Right-sided carcinomas
Obstructive symptoms are not common:
Stool in the area (ileocecal valveIleocecal valveThe valve, at the junction of the cecum with the colon, that guards the opening where the ileum enters the large intestine.Small Intestine: Anatomy to ascending colonAscending colonThe segment of large intestine between the cecum and the transverse colon. It passes cephalad from the cecum to the caudal surface of the right lobe of the liver where it bends sharply to the left, forming the right colic flexure.Colon, Cecum, and Appendix: Anatomy) is still liquid.
Lumen is larger (than left side).
Lesions can grow, ulcerate, and lead to occult blood loss:
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements deficiency anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types: fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, angina, palpitationsPalpitationsEbstein’s Anomaly
Changes in bowel habits (constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation alternating with loose stools)
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy (1st site for intestinal tumors): abdominal distentionAbdominal distentionMegacolon, jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice, ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites, hepatomegaly
LungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy (1st site for distal rectal tumors): cough, dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea (may be from pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion), hemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis
Visualization of lesion(s) and tissue sampling (biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma or lesion removal) can be performed.
Asymptomatic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
For the population with average risk: performed at age 45 years and above
Performed in symptomatic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Colon cancer found on colonoscopy and confirmed via biopsy
Image: “Primary tumor” by Second Department of Surgery, Wakayama Medical University, School of Medicine, 811-1 Kimiidera, Wakayama 641-8510, Japan. License: CC BY 2.0
Can be used in incomplete colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening (e.g., obstruction, tortuous colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy) or as an initial diagnostic test
ColonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening remains the gold standard.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be able to pass flatus.
Cannot perform biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma or lesion removal
PILLCam 2
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: AnatomycapsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.BacteroidesendoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD): Patient swallows a capsule-sized endoscope.
Considered in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with incomplete colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should have no obstruction.
Further imaging studies
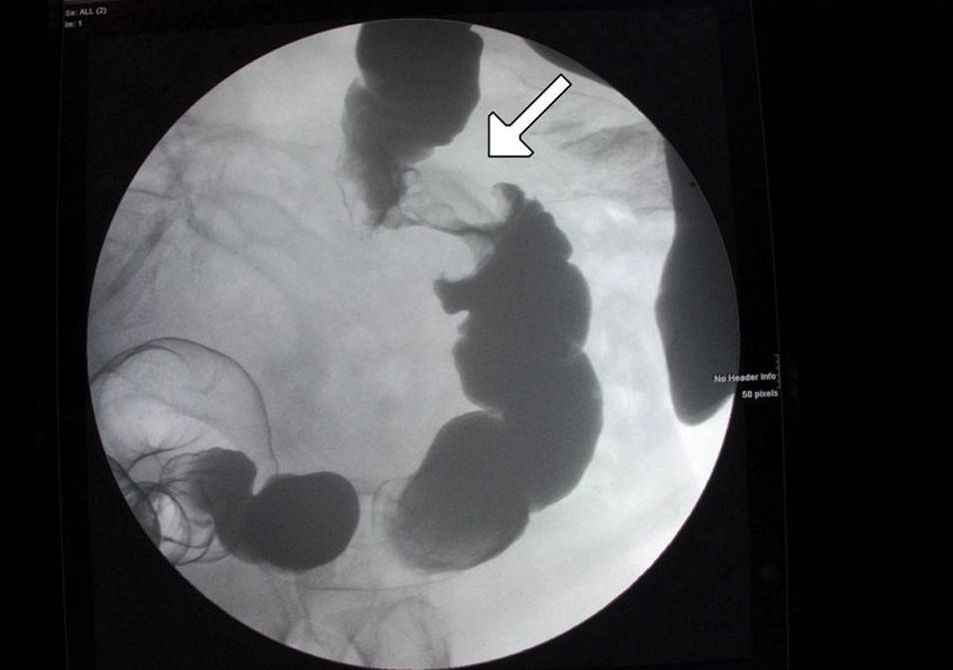
Air contrast barium enemaBarium enemaX-ray examination of lower gastrointestinal tract. Imaging is done while a barium compound (e.g., barium sulfate) fills the large intestine via the rectum as a contrast material.Diarrhea may show apple core lesion.
CT scan:
For preoperative stagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis
Detects associated complications (e.g., obstruction, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula)
Pelvic magnetic resonance imaging (MRI) or transrectal endoscopic ultrasonography (US):
For rectal cancers
For assessment of cancer depth through the rectal wall and perirectal lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy
An “apple core” lesion of the colon shown on contrast enema: This is concerning for cancer.
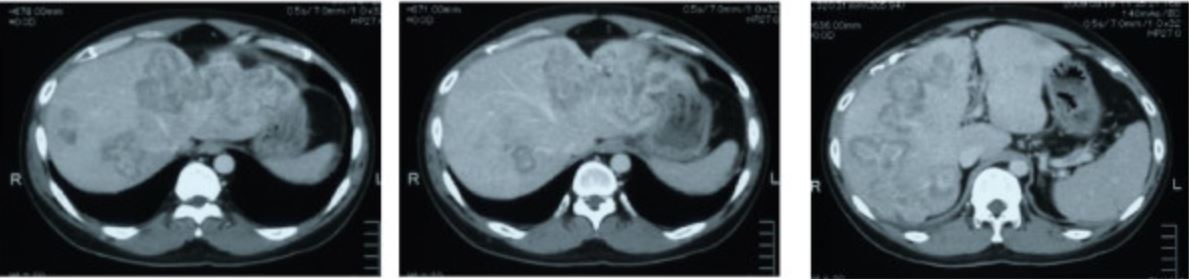
Image: “CT scan showing liver metastasis from sigmoid colon cancer” by Department of Surgery, The Jikei University Kashiwa Hospital, Kashiwashita, Kashiwa City, Japan. License: CC BY 2.0
Laboratory tests
Carcinoembryonic antigenCarcinoembryonic antigenA glycoprotein that is secreted into the luminal surface of the epithelia in the gastrointestinal tract. It is found in the feces and pancreaticobiliary secretions and is used to monitor the response to colon cancer treatment.Serum Tumor Markers (CEACEAA glycoprotein that is secreted into the luminal surface of the epithelia in the gastrointestinal tract. It is found in the feces and pancreaticobiliary secretions and is used to monitor the response to colon cancer treatment.Serum Tumor Markers):
Prognostic value: preoperative CEACEAA glycoprotein that is secreted into the luminal surface of the epithelia in the gastrointestinal tract. It is found in the feces and pancreaticobiliary secretions and is used to monitor the response to colon cancer treatment.Serum Tumor Markers > 5 ng/mL has worse prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas.
Non-normalization of values after surgery: indicative of persistent disease
Complete blood count (CBC): may show anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
Metabolic panel:
May show additional metabolic abnormalities
Elevated alkaline phosphataseAlkaline PhosphataseAn enzyme that catalyzes the conversion of an orthophosphoric monoester and water to an alcohol and orthophosphate.Osteosarcoma: most common liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy abnormality associated with liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: AnatomymetastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Staging
After establishing the diagnosis of CRC, stagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis the disease is needed for appropriate management.
Preoperative examination (e.g., ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites, lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy)
Imaging results:
CT scan (chest/abdomen/pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy)
MRI (identifies more metastatic hepatic lesions)
Transrectal endoscopic US (for rectal cancer)
EndoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) (with biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma) and lymph node biopsyLymph Node BiopsyLymphadenopathy
Tis:carcinoma in situCarcinoma in situA lesion with cytological characteristics associated with invasive carcinoma but the tumor cells are confined to the epithelium of origin, without invasion of the basement membrane.Leukoplakia (intramucosal carcinoma)
M0: no distant metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Stage I
T1: invasion into the submucosa through muscularis mucosa
M0: no distant metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Stage II
T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones: invasion through the muscularis propria and into the pericolorectal tissues
M0: no distant metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
M0: no distant metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Stage IV
Any T
Any N
M1a: metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis to 1 site or organ; no peritoneal metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
M1b:metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis to 2 or more sites; no peritoneal metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
M1c:metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis to peritoneal surface (alone or with other site metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis)
United States Preventive Services Taskforce: daily low-dose aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs) for primary prevention of CRC
Individuals should have:
No bleeding risk
At least 10 years of life expectancyLife expectancyBased on known statistical data, the number of years which any person of a given age may reasonably expected to live.Population Pyramids
Flexible sigmoidoscopySigmoidoscopyEndoscopic examination, therapy or surgery of the sigmoid flexure.Colorectal Cancer Screening every 5 years (limited to distal part of the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy)
CT colonographyCT colonographyA non-invasive imaging method that uses computed tomographic data combined with specialized imaging software to examine the colon.Colorectal Cancer Screening every 5 years
ColonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening atage 40 or 10 years earlier than the age of diagnosis of the 1st-degree relative (whichever comes first)
Treatment of choice for almost all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with resectable lesions
Can be laparoscopic or open surgery
Regional lymphLymphThe interstitial fluid that is in the lymphatic system.Secondary Lymphatic Organs node dissection (at least 12 lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy) is performed with resection (aids in determining additional adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.Vaccination therapy).
AdjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.VaccinationchemotherapyChemotherapyOsteosarcoma: given depending on stage of colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy carcinoma
Neoadjuvant chemotherapyNeoadjuvant ChemotherapyOsteosarcoma and/or radiotherapy: given for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with rectal carcinoma (T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones or higher, node-positive cancers)
FOLFOX (5-fluorouracil5-FluorouracilA pyrimidine analog that is an antineoplastic antimetabolite. It interferes with DNA synthesis by blocking the thymidylate synthetase conversion of deoxyuridylic acid to thymidylic acid.Antimetabolite Chemotherapy/5-FU5-FUA pyrimidine analog that is an antineoplastic antimetabolite. It interferes with DNA synthesis by blocking the thymidylate synthetase conversion of deoxyuridylic acid to thymidylic acid.Antimetabolite Chemotherapy + folinic acid/leucovorin + oxaliplatinOxaliplatinAn organoplatinum complex in which the platinum atom is complexed with 1, 2-diaminocyclohexane, and with an oxalate ligand which is displaced to yield active oxaliplatin derivatives. These derivatives form inter- and intra-strand DNA crosslinks that inhibit DNA replication and transcription. Oxaliplatin is an antineoplastic agent that is often administered with fluorouracil and folinic acid in the treatment of metastatic colorectal neoplasms.Alkylating Agents and Platinum) regimen
FOLFIRI (5-fluorouracil5-FluorouracilA pyrimidine analog that is an antineoplastic antimetabolite. It interferes with DNA synthesis by blocking the thymidylate synthetase conversion of deoxyuridylic acid to thymidylic acid.Antimetabolite Chemotherapy + folinic acid + irinotecanIrinotecanA semisynthetic camptothecin derivative that inhibits DNA topoisomerase I to prevent nucleic acid synthesis during s phase. It is used as an antineoplastic agent for the treatment of colorectal neoplasms and pancreatic neoplasms.Microtubule and Topoisomerase Inhibitors)
CAPOX/XELOX: oral capecitabineCapecitabineA deoxycytidine derivative and fluorouracil prodrug that is used as an antineoplastic antimetabolite in the treatment of colon cancer; breast cancer and gastric cancer.Antimetabolite Chemotherapy (Xeloda) used with oxaliplatinOxaliplatinAn organoplatinum complex in which the platinum atom is complexed with 1, 2-diaminocyclohexane, and with an oxalate ligand which is displaced to yield active oxaliplatin derivatives. These derivatives form inter- and intra-strand DNA crosslinks that inhibit DNA replication and transcription. Oxaliplatin is an antineoplastic agent that is often administered with fluorouracil and folinic acid in the treatment of metastatic colorectal neoplasms.Alkylating Agents and Platinum
The stage of CRC and molecular biology (in the case of targeted therapyTargeted TherapyTargeted therapy exerts antineoplastic activity against cancer cells by interfering with unique properties found in tumors or malignancies. The types of drugs can be small molecules, which are able to enter cells, or monoclonal antibodies, which have targets outside of or on the surface of cells. Targeted and Other Nontraditional Antineoplastic Therapy) dictate the roles of surgical and pharmacologic treatments.
Carcinoma in a polyp
Endoscopic removal or polypectomy
When invasive cancer is suspected, tattooing is done (for localization if an invasive lesion is found or if additional therapy/surgery is needed).
Factors indicating high risk for residual cancer or nodal metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis (consider radical surgery):
Poorly differentiated histology
Cancer at stalk margin
Lymphovascular invasion
T2 lesion
Invasive carcinoma in a sessile polyp
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy cancer stage I–III
Wide resection of the lesion with regional lymphadenectomy is performed.
Surgical options:
Right hemicolectomy: lesion(s) in the cecumCecumThe blind sac or outpouching area of the large intestine that is below the entrance of the small intestine. It has a worm-like extension, the vermiform appendix.Colon, Cecum, and Appendix: Anatomy and right colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy (can be extended to include transverse colonTransverse colonThe segment of large intestine between ascending colon and descending colon. It passes from the right colic flexure across the abdomen, then turns sharply at the left colonic flexure into the descending colon.Colon, Cecum, and Appendix: Anatomy)
Left hemicolectomy: lesion(s) in the splenic flexureSplenic flexureSmall Intestine: Anatomy and left colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy (can be extended to include transverse colonTransverse colonThe segment of large intestine between ascending colon and descending colon. It passes from the right colic flexure across the abdomen, then turns sharply at the left colonic flexure into the descending colon.Colon, Cecum, and Appendix: Anatomy)
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colectomy: sigmoidSigmoidA segment of the colon between the rectum and the descending colon.VolvuluscolonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Total abdominal colectomy:
Synchronous colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy cancers
FAPFAPFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis
HNPCCHNPCCLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome
Multivisceral resection with negative margins of the involved structure is recommended in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who have an invasion of the contiguous organs or adhesions with adjacent structures.
Stage I: no adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.Vaccination therapy
Stage II: controversial; those at high risk of recurrence may benefit from adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.Vaccination therapy
Stage III (node-positive disease):
Significant benefit from adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.Vaccination therapy
MSI-H tumors: do not benefit from 5-FU5-FUA pyrimidine analog that is an antineoplastic antimetabolite. It interferes with DNA synthesis by blocking the thymidylate synthetase conversion of deoxyuridylic acid to thymidylic acid.Antimetabolite Chemotherapy based chemotherapyChemotherapyOsteosarcoma
Metastatic disease or stage IV
The majority do not have a resectable (curable) disease.
Isolated liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy/lung lesions: Metastatic lesions confined to the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy or lung can be resected.
The addition of biologic agentsBiologic AgentsImmunosuppressants/targeted therapyTargeted TherapyTargeted therapy exerts antineoplastic activity against cancer cells by interfering with unique properties found in tumors or malignancies. The types of drugs can be small molecules, which are able to enter cells, or monoclonal antibodies, which have targets outside of or on the surface of cells. Targeted and Other Nontraditional Antineoplastic Therapy improves survival in suitable patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Unresectable metastatic disease:
Address the associated complication(s) (obstruction, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis).
Local ablative techniques (cryosurgery, radiofrequency coagulation, embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding, hepatic intra-arterial chemotherapyChemotherapyOsteosarcoma) or radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
In T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones or greater tumors
For minimally invasive, small (less than 3 cm), well-differentiated T1 rectal tumors: transanal excision
Most stage II–III:
Low anterior resection (LAR):
Sphincter-preserving surgery
Moderately or well-differentiated tumors within 2 cm of the anal sphincter
Poorly differentiated tumors within 5 cm of the anal sphincter
Abdominoperineal resection (APR):
Total rectal excision with a permanent colostomy
Moderately or well-differentiated tumors < 2 cm from the anal sphincter
Poorly differentiated tumors < 5 cm from the anal sphincter
Unresectable rectal cancer: palliative treatment with a diverting colostomy
Role of targeted therapyTargeted TherapyTargeted therapy exerts antineoplastic activity against cancer cells by interfering with unique properties found in tumors or malignancies. The types of drugs can be small molecules, which are able to enter cells, or monoclonal antibodies, which have targets outside of or on the surface of cells. Targeted and Other Nontraditional Antineoplastic Therapy
GeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics profiling of tumorTumorInflammation tissue: performed to find specific molecular abnormalities and determine treatment options
Anti-EGFR (epidermal growth factor receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors) (added to chemotherapyChemotherapyOsteosarcoma in stage IV tumors with specific mutations): cetuximabCetuximabA chimeric monoclonal antibody that functions as an antineoplastic agent through its binding to the epidermal growth factor receptor, where it prevents the binding and signaling action of cell growth and survival factors.Targeted and Other Nontraditional Antineoplastic Therapy, panitumumabPanitumumabRecombinant human monoclonal antibody that binds to and inhibits the function of the epidermal growth factor receptor. It is used in the treatment of egfr-expressing metastatic colorectal cancer that expresses wild-type RAS gene.Targeted and Other Nontraditional Antineoplastic Therapy
BRAF inhibitor (for metastatic CRC that progressed with prior chemotherapyChemotherapyOsteosarcoma): encorafenib
Immune checkpoint inhibitorsImmune Checkpoint InhibitorsDrugs that block negative regulator immune checkpoint proteins (e.g., PD-1 receptor and CTLA-4 antigen) thereby increasing suppressed immune activation in immunotherapies.Cancer Immunotherapy (for MSI-H or deficient mismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndrome (dMMR) CRC): pembrolizumabPembrolizumabSquamous Cell Carcinoma (SCC), nivolumabNivolumabA genetically engineered, fully humanized immunoglobulin g4 monoclonal antibody that binds to the pd-1 receptor, activating an immune response to tumor cells. It is used as monotherapy or in combination with ipilimumab for the treatment of advanced malignant melanoma. It is also used in the treatment of advanced or recurring non-small cell lung cancer; renal cell carcinoma; and Hodgkin’s lymphoma.Melanoma
Multi-targeted kinase inhibitor (for metastatic, refractory CRC after progression on standard regimens): regorafenib
Trifluridine/tipiracil (refractory CRC after progression on standard regimens)
Follow-up
Carcinoembryonic antigenCarcinoembryonic antigenA glycoprotein that is secreted into the luminal surface of the epithelia in the gastrointestinal tract. It is found in the feces and pancreaticobiliary secretions and is used to monitor the response to colon cancer treatment.Serum Tumor Markers:
Monitored for 5 years after the completion of treatment (every 6 months).
Serial values after surgery/treatment:
Elevation of CEACEAA glycoprotein that is secreted into the luminal surface of the epithelia in the gastrointestinal tract. It is found in the feces and pancreaticobiliary secretions and is used to monitor the response to colon cancer treatment.Serum Tumor Markers should be retested.
When confirmed, testing may include CT scan, positron emission tomography (PETPETAn imaging technique that combines a positron-emission tomography (PET) scanner and a ct X ray scanner. This establishes a precise anatomic localization in the same session.Nuclear Imaging), and/or colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening looking for disease recurrence.
Within a few months after surgical resection, then 1 year after surgery
Every 3–5 years thereafter
Imaging:
Annual CT scan (chest and abdomen) for at least 3 years
Annual CT scan (pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy) for rectal cancer if pelvic radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma was not given
Familial adenomatous polyposisFamilial Adenomatous PolyposisFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance
Occurs due to a mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in the APCAPCA polyposis syndrome due to an autosomal dominant mutation of the apc genes on chromosome 5. The syndrome is characterized by the development of hundreds of adenomatous polyps in the colon and rectum of affected individuals by early adulthood.Familial Adenomatous PolyposisgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics
Hundreds of colorectal adenomas develop (seen in colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening) by age 15 years.
Treatment: prophylactic colectomy (proctocolectomy or total colectomy), usually by age 20
Indications for colectomy in FAPFAPFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis:
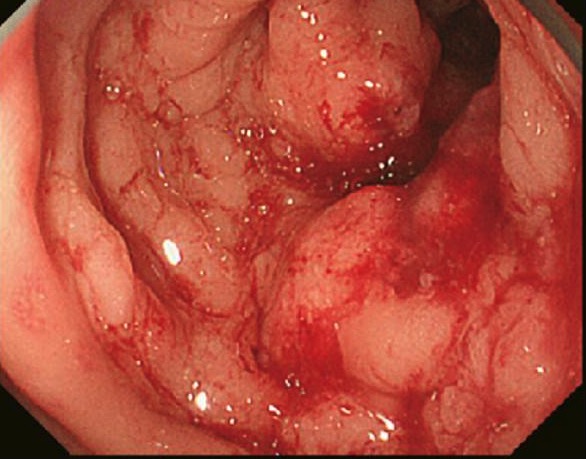
Colonic mucosa carpeted by adenomatous polyps in familial adenomatous polyposis FAP
Image: “Colonic mucosa carpeted by adenomatous polyps in familial adenomatous polyposis FAP” by Shussman N., Wexner SD. License: CC BY 3.0
Endoscopic view of established, multiple FAP adenomas
Image: “Endoscopic view of established, multiple FAP adenomas” by Bercovich D., Rozen P. License: CC BY 2.0
Hereditary non-polyposis colorectal cancerHereditary non-polyposis colorectal cancerLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome/Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance
Occurs due to mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations of 1 of the DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structuremismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndromegenesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure (MSH2, MSH6, MLH1) resulting in MSI, or the EPCAMEPCAMA cell adhesion molecule that is expressed on the membranes of nearly all epithelial cells, especially at the junctions between intestinal epithelial cells and intraepithelial lymphocytes. It also is expressed on the surface of adenocarcinoma and epithelial tumor cells. It may function in the mucosa through homophilic interactions to provide a barrier against infection. It also regulates the proliferation and differentiation of embryonic stem cells.Lynch syndromegeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics.
3or more relatives with CRC, 1 of whom must be a first-degree relative of the other 2
Involvement of 2 or more generations
At least 1 cancer must have been diagnosed < 50 years of age.
FAPFAPFamilial adenomatous polyposis (FAP) is an autosomal dominant inherited genetic disorder that presents with numerous adenomatous polyps in the colon. Familial adenomatous polyposis is the most common of the polyposis syndromes, which is a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract, associated with other extracolonic features. Familial Adenomatous Polyposis has been excluded.
Tumors verified by pathologic examination
Confirmatory test: DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure sequencing
AspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs) (may reduce risk of CRC)
Peutz-Jeghers syndromePeutz-Jeghers SyndromePeutz-Jeghers syndrome (PJS) is an autosomal-dominant inherited disorder characterized by GI polyps and mucocutaneous-pigmented macules. Peutz-Jeghers syndrome is 1 of the polyposis syndromes, a group of inherited or acquired conditions characterized by the growth of polyps in the GI tract and associated with other extracolonic features.Peutz-Jeghers Syndrome
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance
STK11mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations
Development of hamartomas of the small and large intestines
Associated withhyperpigmentationHyperpigmentationExcessive pigmentation of the skin, usually as a result of increased epidermal or dermal melanin pigmentation, hypermelanosis. Hyperpigmentation can be localized or generalized. The condition may arise from exposure to light, chemicals or other substances, or from a primary metabolic imbalance.Malassezia Fungi of the mouth, hands, and feet
Risk of developing CRC: 40%
Malignancies:
Gastrointestinal (GI) malignancies (stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy, and colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy) develop in 40%–60% of cases.
Breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer in 30%–50% of cases
Nonintestinal organs (gonadsGonadsThe gamete-producing glands, ovary or testis.Hormones: Overview and Types, pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy)
HemorrhoidsHemorrhoidsHemorrhoids are normal vascular cushions in the anal canal composed of dilated vascular tissue, smooth muscle, and connective tissue. They do not cause issues unless they are enlarged, inflamed, thrombosed, or prolapsed. Patients often present with rectal bleeding of bright red blood, or they may have pain, perianal pruritus, or a palpable mass. Hemorrhoids: also presents with blood per rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and changes in bowel habits. HemorrhoidsHemorrhoidsHemorrhoids are normal vascular cushions in the anal canal composed of dilated vascular tissue, smooth muscle, and connective tissue. They do not cause issues unless they are enlarged, inflamed, thrombosed, or prolapsed. Patients often present with rectal bleeding of bright red blood, or they may have pain, perianal pruritus, or a palpable mass. Hemorrhoids may cause rectal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and can be identified on physical exam or anoscopic exam. Bleeding per rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy in a patient > 50 years of age with hemorrhoidsHemorrhoidsHemorrhoids are normal vascular cushions in the anal canal composed of dilated vascular tissue, smooth muscle, and connective tissue. They do not cause issues unless they are enlarged, inflamed, thrombosed, or prolapsed. Patients often present with rectal bleeding of bright red blood, or they may have pain, perianal pruritus, or a palpable mass. Hemorrhoids still needs to be investigated for CRC.
Diverticular diseaseDiverticular diseaseDiverticula are protrusions of the bowel wall occurring most commonly in the colon. The condition of having diverticula (called diverticulosis) is mostly asymptomatic. These diverticula can become symptomatic, however, when associated with diseases. Diverticulitis is the inflammation of diverticula, often presenting with lower abdominal pain and changes in bowel habits.Diverticular Disease: diverticulosisDiverticulosisA pathological condition characterized by the presence of a number of colonic diverticula in the colon. Its pathogenesis is multifactorial, including colon aging, motor dysfunction, increases in intraluminal pressure, and lack of dietary fibers.Diverticular Disease is the presence of sac-like protrusions in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy.Complications include diverticular bleeding and diverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease, which also present with blood per rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and changes in bowel habits. Colonoscopic findings differentiate diverticular diseaseDiverticular diseaseDiverticula are protrusions of the bowel wall occurring most commonly in the colon. The condition of having diverticula (called diverticulosis) is mostly asymptomatic. These diverticula can become symptomatic, however, when associated with diseases. Diverticulitis is the inflammation of diverticula, often presenting with lower abdominal pain and changes in bowel habits.Diverticular Disease from CRC.
Small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: AnatomyneoplasmsNeoplasmsNew abnormal growth of tissue. Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms.Benign Bone Tumors: also present with blood in stool and obstructive symptoms. To differentiate these neoplasmsNeoplasmsNew abnormal growth of tissue. Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms.Benign Bone Tumors from CRC, upper and lower endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) may be required.
Neuroendocrine tumorsNeuroendocrine tumorsTumors whose cells possess secretory granules and originate from the neuroectoderm, i.e., the cells of the ectoblast or epiblast that program the neuroendocrine system. Common properties across most neuroendocrine tumors include ectopic hormone production (often via apud cells), the presence of tumor-associated antigens, and isozyme composition.Gastrinoma: affect the right colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy in the majority of cases. These lesions have characteristic symptoms of carcinoid syndromeCarcinoid syndromeA symptom complex associated with carcinoid tumor and characterized by attacks of severe flushing of the skin, diarrheal watery stools, bronchoconstriction, sudden drops in blood pressure, edema, and ascites. The carcinoid tumors are usually located in the gastrointestinal tract and metastasize to the liver. Symptoms are caused by tumor secretion of serotonin, prostaglandins, and other biologically active substances. Cardiac manifestations constitute carcinoid heart disease.Carcinoid Tumors and Syndrome (diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, flushing, and wheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing).
References
Chime, C., Patel, H., Kumar, K., Elwan, A., Bhandari, M., & Ihimoyan, A. (2019). Colon cancer with Streptococcus gallolyticus aortic valve endocarditis: A missing link? Case Reports in Gastrointestinal Medicine, 2019, Article 4205603. https://doi.org/10.1155/2019/4205603
American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC). (2018). Colorectal cancer TNM staging. 8th edition.
De Palma, F., D’Argenio, V., Pol, J., Kroemer, G., Chiara Maiuri, M., & Salvatore, F. (2019). The Molecular Hallmarks of the Serrated Pathway in Colorectal Cancer. Cancers (Basel) 11(7): 1017. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6678087/
Eshghifar, N., Farrokhi, N., Naji, T. & Zali, M. (2017). Tumor suppressor genes in familial adenomatous polyposis. Gastroenterol Hepatol Bed Bench. 10(1): 3–13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5346818/
Grady, W., Markowitz, S. (2015). The molecular pathogenesis of colorectal cancer and its potential application to colorectal cancer screening. Dig Dis Sci. 60(3): 762–772. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4779895/
Heidt, D., Huang, E., Minter, R. & Doherty, G. (2010). Operative Management of Rectal Tumors. Current Procedures: Surgery. McGraw-Hill.
Kumar V, Abbas A, Aster J, Robbins, S. Robbins & Cotran (Eds.). (2020). The gastrointestinal tract. Pathologic Basis of Disease (10th ed., 807-818). Elsevier, Inc.
Kwaan M.R., Stewart Sr D.B., & Dunn K (2019). Colon, rectum, and anus. In Brunicardi F, et al. (Eds), Schwartz’s Principles of Surgery, 11th ed. McGraw-Hill.