Subarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. The most classic symptom is a sudden-onset (thunderclap) headache along with neck stiffness, vomiting, a decreased level of consciousness, and seizure. As with any stroke, focal neurologic deficits are commonly present, and rapid neurologic deterioration may ensue without prompt diagnosis and intervention. An SAH should be suspected in any person presenting with thunderclap headache and neurologic symptoms, and the diagnosis can be confirmed with neuroimaging or lumbar puncture (LP). Treatment consists of reversal of anticoagulation, control of blood pressure, and neurosurgical intervention to contain the bleed and/or relieve elevated intracranial pressure (ICP). Even with prompt neurosurgical intervention, SAH carries a high mortality rate.
SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is a type of cerebrovascular accidentCerebrovascular accidentAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke (stroke) resulting from intracranial hemorrhageIntracranial hemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most sahs originate from a saccular aneurysm in the circle of willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use.Subarachnoid Hemorrhage into the subarachnoid spaceSubarachnoid spaceThe space between the arachnoid membrane and pia mater, filled with cerebrospinal fluid. It contains large blood vessels that supply the brain and spinal cord.Subarachnoid Hemorrhage.
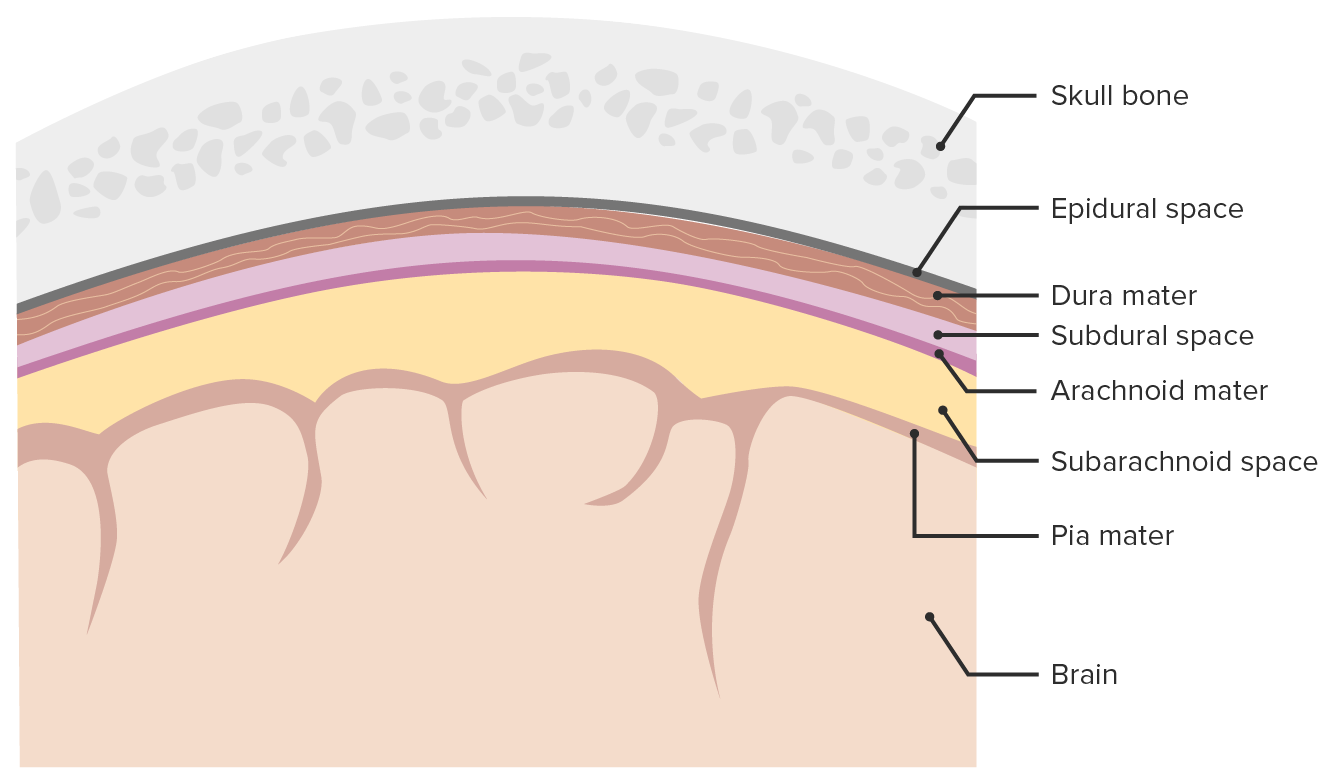
Subarachnoid spaceSubarachnoid spaceThe space between the arachnoid membrane and pia mater, filled with cerebrospinal fluid. It contains large blood vessels that supply the brain and spinal cord.Subarachnoid Hemorrhage: area between the arachnoid materArachnoid materA delicate membrane enveloping the brain and spinal cord. It lies between the pia mater and the dura mater. It is separated from the pia mater by the subarachnoid cavity which is filled with cerebrospinal fluid.Meninges: Anatomy and the pia materPia materThe innermost layer of the three meninges covering the brain and spinal cord. It is the fine vascular membrane that lies under the arachnoid and the dura mater.Meninges: Anatomy layers of the meningesMeningesThe brain and the spinal cord are enveloped by 3 overlapping layers of connective tissue called the meninges. The layers are, from the most external layer to the most internal layer, the dura mater, arachnoid mater, and pia mater. Between these layers are 3 potential spaces called the epidural, subdural, and subarachnoid spaces. Meninges: Anatomy surrounding the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Meninges and meningeal spaces: The image depicts the 3 layers (dura mater, arachnoid mater, pia mater) surrounding the brain and spinal cord. The meninges serve as mechanical protection of the CNS. They also support the cerebral and spinal blood vessels and allow for passage of the CSF. The subarachnoid space is filled with CSF.
Image by Lecturio.
Epidemiology[2]
Hemorrhagic strokes:
Account for 15%–20% of cerebrovascular accidents
50% of spontaneous hemorrhagic strokes are due to SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
Ruptured saccular aneurysmsSaccular aneurysmsBrain Aneurysms are the most common cause of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
Most aneurysms, especially small ones, do not rupture.
15%–20% percent of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage cases are non-aneurysmal.
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
Global incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage: 6–10 cases/100,000 person-years
GeneticsGeneticsGenetics is the study of genes and their functions and behaviors.Basic Terms of Genetics, increased incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency seen in:
Autosomal dominant polycystic kidney diseaseAutosomal dominant polycystic kidney diseasePolycystic kidney disease (PKD) is an inherited genetic disorder leading to the development of numerous fluid-filled cysts in the kidneys. The 2 main types of PKD are autosomal dominant polycystic kidney disease (ADPKD), which is often diagnosed in adulthood, and autosomal recessive polycystic kidney disease (ARPKD), which is often diagnosed antenatally or shortly after birth. Autosomal dominant polycystic kidney disease (ADPKD) (ADPKDADPKDPolycystic kidney disease (PKD) is an inherited genetic disorder leading to the development of numerous fluid-filled cysts in the kidneys. The 2 main types of PKD are autosomal dominant polycystic kidney disease (ADPKD), which is often diagnosed in adulthood, and autosomal recessive polycystic kidney disease (ARPKD), which is often diagnosed antenatally or shortly after birth. Autosomal dominant polycystic kidney disease (ADPKD))
Ehlers-Danlos syndromeEhlers-Danlos syndromeEhlers-Danlos syndrome (EDS) is a heterogeneous group of inherited connective tissue disorders that are characterized by hyperextensible skin, hypermobile joints, and fragility of the skin and connective tissue. Ehlers-Danlos Syndrome (EDS) type IV
Up to fivefold increased risk in 1st-degree relatives
Familial cerebral aneurysms rupture more frequently than nonfamilial aneurysms
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
Stimulant use:
CocaineCocaineAn alkaloid ester extracted from the leaves of plants including coca. It is a local anesthetic and vasoconstrictor and is clinically used for that purpose, particularly in the eye, ear, nose, and throat. It also has powerful central nervous system effects similar to the amphetamines and is a drug of abuse. Cocaine, like amphetamines, acts by multiple mechanisms on brain catecholaminergic neurons; the mechanism of its reinforcing effects is thought to involve inhibition of dopamine uptake.Local Anesthetics
Amphetamine/methamphetamineMethamphetamineA central nervous system stimulant and sympathomimetic with actions and uses similar to dextroamphetamine. The smokable form is a drug of abuse and is referred to as crank, crystal, crystal meth, ice, and speed.Stimulants
SympathomimeticsSympathomimeticsSympathomimetic drugs, also known as adrenergic agonists, mimic the action of the stimulators (î±, β, or dopamine receptors) of the sympathetic autonomic nervous system. Sympathomimetic drugs are classified based on the type of receptors the drugs act on (some agents act on several receptors but 1 is predominate).Sympathomimetic Drugs:
Cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Alcohol use disorderAlcohol use disorderAlcohol is one of the most commonly used addictive substances in the world. Alcohol use disorder (AUD) is defined as pathologic consumption of alcohol leading to impaired daily functioning. Acute alcohol intoxication presents with impairment in speech and motor functions and can be managed in most cases with supportive care. Alcohol Use Disorder
EstrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy deficiency (increased incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency observed in women > 50 years of age)
Increased incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency observed in multiparousMultiparousA woman with prior deliveriesNormal and Abnormal Labor females
Causes[2,7,8]
Trauma
Ruptured aneurysms
Saccular aneurysmsSaccular aneurysmsBrain Aneurysms (“berry aneurysmsBerry aneurysmsBrain Aneurysms,” round shape) are the most common cause of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
Fusiform aneurysms (dilatation of the entire vessel wall for a short distance)and mycotic aneurysms (bacterial, fungal, or viral infection of the vessel wall) are also possible.
Arteriovenous malformationsArteriovenous malformationsCongenital vascular anomalies in the brain characterized by direct communication between an artery and a vein without passing through the capillaries. The locations and size of the shunts determine the symptoms including headaches; seizures; stroke; intracranial hemorrhages; mass effect; and vascular steal effect.Intracerebral Hemorrhage (AVMs)
Arterial dissections
VasculitisVasculitisInflammation of any one of the blood vessels, including the arteries; veins; and rest of the vasculature system in the body.Systemic Lupus Erythematosus
Vascular amyloid deposition
Pituitary apoplexyPituitary apoplexyThe sudden loss of blood supply to the pituitary gland, leading to tissue necrosis and loss of function (panhypopituitarism). The most common cause is hemorrhage or infarction of a pituitary adenoma. It can also result from acute hemorrhage into sella turcica due to head trauma; intracranial hypertension; or other acute effects of central nervous system hemorrhage. Clinical signs include severe headache; hypotension; bilateral visual disturbances; unconsciousness; and coma.Hypopituitarism
Illicit stimulant use
Pathophysiology
Given that saccular aneurysmSaccular AneurysmSubarachnoid Hemorrhage is the most common etiology of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage, this section will focus on the pathogenesis of saccular aneurysmSaccular AneurysmSubarachnoid Hemorrhage rupture. Events that occur after the rupture itself are common to other etiologies of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
Protrusions from intracranial arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology
Thin-walled
Tunica mediaTunica mediaThe middle layer of blood vessel walls, composed principally of thin, cylindrical, smooth muscle cells and elastic tissue. It accounts for the bulk of the wall of most arteries. The smooth muscle cells are arranged in circular layers around the vessel, and the thickness of the coat varies with the size of the vessel.Arteries: Histology may be absent or thin.
Most commonly located in the circle of WillisCircle of WillisA polygonal anastomosis at the base of the brain formed by the internal carotid, proximal parts of the anterior, middle, and posterior cerebral arteries, the anterior communicating artery and the posterior communicating arteries.Subarachnoid Hemorrhage
Located in the anterior circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment > posterior circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment
Sites of bifurcation are the most vulnerable.
Episodes of acute instability or growth spurts develop over a short time in response to abnormal vascular shear forces:
Stabilization may occur with hardening due to collagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology deposition.
Intimal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation
Infiltration with T cellsT cellsLymphocytes responsible for cell-mediated immunity. Two types have been identified – cytotoxic (t-lymphocytes, cytotoxic) and helper T-lymphocytes (t-lymphocytes, helper-inducer). They are formed when lymphocytes circulate through the thymus gland and differentiate to thymocytes. When exposed to an antigen, they divide rapidly and produce large numbers of new T cells sensitized to that antigen.T cells: Types and Functions and macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation
Thin layer of thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus
Presence of odontogenic bacterial DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure (possible role of dental/periodontal infection remains an area of active investigation; not yet established as a major pathologic feature)
Risk factors for rupture[2,7]
AneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms size (diameter) > 7 mm → ↑ risk of aneurysmal ruptureAneurysmal ruptureThe tearing or bursting of the weakened wall of the aneurysmal sac, usually heralded by sudden worsening pain. The great danger of a ruptured aneurysm is the large amount of blood spilling into the surrounding tissues and cavities, causing hemorrhagic shock.Thoracic Aortic Aneurysms:
Larger aneurysms are more likely to grow than smaller aneurysms.
The rate of rupture risk is proportional to the diameter of the aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms.
AneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms growth:
Aneurysmal growth increases the diameter of the lesion.
Rapid growth outpaces the ability for collagen-mediated stabilization.
AneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms site:
The risk of rupture varies based on the parent vessel giving rise to the aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms.
Posterior circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment > anterior circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment > cavernous carotid artery
Uncontrolled hypertensionUncontrolled hypertensionAlthough hypertension is defined as a blood pressure of > 130/80 mm Hg, individuals can present with comorbidities of severe asymptomatic or “uncontrolled” hypertension (≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic) that carries with it a significant risk of morbidity and mortality. Uncontrolled Hypertension
Rupture can also occur with nonstrenuous activity.
Clinical sequelae of rupture[2,7]
Leakage of blood into the CSF:
Leads to increased intracranial pressureIntracranial PressureIdiopathic Intracranial Hypertension (ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP))
Sentinel bleed:
A warning leak preceding the major hemorrhage by days to weeks (seen in 10–43% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
May last only seconds but with a high incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of rebleeding
HydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage/increased ICPIncreased ICPExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage:
Blockage of CSF flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure and/or reabsorption caused by buildup of blood products and or/adhesions
Continued leakage of blood into the subarachnoid spaceSubarachnoid spaceThe space between the arachnoid membrane and pia mater, filled with cerebrospinal fluid. It contains large blood vessels that supply the brain and spinal cord.Subarachnoid Hemorrhage compounds the problem.
Endothelial dysfunction from the site of rupture causes local hyperemia and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation.
Cerebral vasospasm:
Seen in days 4 to 14 after hemorrhage
Release of inflammatory mediators from injured vessels, oxidative stressOxidative stressA disturbance in the prooxidant-antioxidant balance in favor of the former, leading to potential damage. Indicators of oxidative stress include damaged DNA bases, protein oxidation products, and lipid peroxidation products.Cell Injury and Death, decreased nitric oxideNitric OxideA free radical gas produced endogenously by a variety of mammalian cells, synthesized from arginine by nitric oxide synthase. Nitric oxide is one of the endothelium-dependent relaxing factors released by the vascular endothelium and mediates vasodilation. It also inhibits platelet aggregation, induces disaggregation of aggregated platelets, and inhibits platelet adhesion to the vascular endothelium. Nitric oxide activates cytosolic guanylate cyclase and thus elevates intracellular levels of cyclic gmp.Pulmonary Hypertension Drugs may cause local vasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure.
Vasospasm causes local hypoperfusion, worsening the ischemic insult.
The classic presenting symptom of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is a thunderclap headacheThunderclap HeadacheSubarachnoid Hemorrhage. There are other presenting symptoms as well.
Often (10%–40%) preceded by less severe prodromal headaches (“sentinel headaches”)
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess location/description is inconsistent among SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage sufferers.
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess presentation: not always severe but usually accompanied by nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia[14]
Often presents hours after the onset of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma is uncommon, but degree of encephalopathyEncephalopathyHyper-IgM Syndrome is a major determinant of prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas.
Sudden death occurs in > 20% of affected individuals before presenting to medical attentionAttentionFocusing on certain aspects of current experience to the exclusion of others. It is the act of heeding or taking notice or concentrating.Psychiatric Assessment.
Seizure:[11,17]
In approximately 10%–20% of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage cases
Generally occur in the first 24 hours
Associated with poor outcome
Seen in association with middle cerebral and anterior communicating artery aneurysms
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia[6,17]
Sentinel hemorrhage:[6,17]
A “warning leak” occurring prior to major hemorrhage
Symptoms (milder headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia) take place around 2–8 weeks before the SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
May be a precipitating event for aneurysmal ruptureAneurysmal ruptureThe tearing or bursting of the weakened wall of the aneurysmal sac, usually heralded by sudden worsening pain. The great danger of a ruptured aneurysm is the large amount of blood spilling into the surrounding tissues and cavities, causing hemorrhagic shock.Thoracic Aortic Aneurysms
May be a reactive phenomenon to intracerebral events
Associated with increased ICPIncreased ICPExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage as opposed to true retinal involvement
Associated with poor outcome
Oculomotor nerveOculomotor nerveThe 3D cranial nerve. The oculomotor nerve sends motor fibers to the levator muscles of the eyelid and to the superior rectus, inferior rectus, and inferior oblique muscles of the eye. It also sends parasympathetic efferents (via the ciliary ganglion) to the muscles controlling pupillary constriction and accommodation. The motor fibers originate in the oculomotor nuclei of the midbrain.The 12 Cranial Nerves: Overview and Functions (CN III) palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies[6]
Often presents as a unilateral pupillary defect
Due to CN III compressionCompressionBlunt Chest Trauma from aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms of the posterior communicating artery or superior cerebellar arterySuperior cerebellar arteryCerebrovascular System: Anatomy (located near CN III exit site from the brainstem)
SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage can manifest with a wide variety of neurologic findings.
Findings depend on the size and location of the hemorrhage.
Cushing triad[19]
Due to raised ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP)
BradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias
Diagnosis
Any thunderclap headacheThunderclap HeadacheSubarachnoid Hemorrhage presenting with or without neurologic symptoms/signs or altered mental statusAltered Mental StatusSepsis in Children should be emergently evaluated with neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Noncontrast CT is readily available at most acute care hospitals and is the initial test of choice.
If the person is unstable, rapidly deteriorating, or displaying signs of raised ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), do not wait for diagnostic confirmation before stabilizing the patient and commencing neuroprotective measures.
Clinical decision tool used to evaluate suspected SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage with emergent noncontrast CT of the head (Ottawa SAH calculator)
The presence of any of the following features is an indication for emergent CT:
NeckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar AbscesspainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways or stiffness
Cornerstone of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage diagnosis
Sensitivity of up to 100%:
If performed within 6 hours of presentation (sensitivity drops to 86% if performed after 6 hours)[15]
If reviewed by qualified neuroradiologist
Should include cuts through the base of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Locations of blood in SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage:
An LP should be performed promptly (despite negative CT if clinical suspicion of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is high).[10,12,15]
Whenever possible, the sample should be collected at least 12 hours after the event.
The sample should be protected from light (wrapped in foil or placed in a thick brown envelopeEnvelopeBilayer lipid membrane acquired by viral particles during viral morphogenesis. Although the lipids of the viral envelope are host derived, various virus-encoded integral membrane proteins, i.e. Viral envelope proteins are incorporated there.Virology outside the specimen back) to prevent degradation of bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism.
Avoid vacuum tube transport systems (to prevent hemolysis of RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology during transport).
Studies should include:[12,15]
Opening pressure
Cell counts:
RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology
RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology release oxyhemoglobin as they break down.
SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is ruled out when:[15,20]
After SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is established, angiographic studies should be performed to identify the hemorrhagic source:
Digital subtraction angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery (DSA): preferred method, allows for intervention to be performed simultaneously with identificationIdentificationDefense Mechanisms of the source
CTACTAA non-invasive method that uses a ct scanner for capturing images of blood vessels and tissues. A contrast material is injected, which helps produce detailed images that aid in diagnosing vascular diseases.Pulmonary Function Tests and MRAMRAImaging of the Heart and Great Vessels: noninvasive alternatives
Once the bleeding source is identified, clinical decisions about appropriateness of intervention are undertaken.
Severity assessment[14,15,21]
Several scalesScalesDry or greasy masses of keratin that represent thickened stratum corneum.Secondary Skin Lesions are utilized clinically in the diagnosis and gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis of severity in SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage. The Hunt and Hess gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis system (calculator) is among the most commonly used in clinical medicine. Another system is the World Federation of Neurological Surgeons gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and MetastasisscaleScaleDermatologic Examination, which incorporates the Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma) with motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology deficits.
Other gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis systems are available.
The above scalesScalesDry or greasy masses of keratin that represent thickened stratum corneum.Secondary Skin Lesions, which are commonly used, have notable intraobserver and interobserver variability.
No single scaleScaleDermatologic Examination has been found to be optimal in determining prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas and in helping to guide management.
Choice of system depends on the individual and/or institution; it is important, however, to consider other important factors that determine prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas, including:
Age
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
Size of bleed on CT scan
AneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms location and size
Other cranial areas affected by hemorrhage
Time of admission
Table: Hunt and Hess gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis system
Asymptomatic or mild headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess and slight nuchal rigidityNuchal RigidityMeningitis
1
2
Severe headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, stiff neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess, no neurologic deficit except cranial nerve (CN) palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Stuporous, moderate or severe hemiparesisHemiparesisThe term hemiparesis refers to mild to moderate weakness involving one side of the body.Epidural Hemorrhage
42
5
ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma, decerebrate posturingDecerebrate posturingA condition characterized by abnormal posturing of the limbs that is associated with injury to the brainstem. This may occur as a clinical manifestation or induced experimentally in animals. The extensor reflexes are exaggerated leading to rigid extension of the limbs accompanied by hyperreflexia and opisthotonus. This condition is usually caused by lesions which occur in the region of the brainstem that lies between the red nuclei and the vestibular nuclei. In contrast, decorticate rigidity is characterized by flexion of the elbows and wrists with extension of the legs and feet. The causative lesion for this condition is located above the red nuclei and usually consists of diffuse cerebral damage.Increased Intracranial Pressure (ICP), moribund appearance
77
Table: World Federation of Neurological Surgeons gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and MetastasisscaleScaleDermatologic Examination
Grade
Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination score
Additional tests that may help guide diagnosis and management include:
CBC
Coagulation studiesCoagulation studiesCoagulation studies are a group of hematologic laboratory studies that reflect the function of blood vessels, platelets, and coagulation factors, which all interact with one another to achieve hemostasis. Coagulation studies are usually ordered to evaluate patients with bleeding or hypercoagulation disorders.Coagulation Studies (PTT, PT/INR)
Creatinine
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG)
The following are potential complications of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage:[17,18,22]
Rebleeding:
Risk up to 14% in the first 24 hours
Maximum risk within 1st 6 hours
Associated with poor outcomes
Factors that increase rebleeding:
Longer wait until aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms treatment
Loss of consciousness on initial presentation (HHHHHereditary hemochromatosis (HH) is an autosomal recessive disorder most often associated with hfe gene mutations. Patients have increased iron intestinal absorption and iron deposition in several organs, such as the liver, heart, skin, and pancreas. The clinical presentation includes the triad of cirrhosis, diabetes, and skin bronzing.Hereditary Hemochromatosis grade III–V or WFNS grade IV–V)
Sentinel headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Large aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms size
High systolic blood pressure
Acute hydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage
Vasospasm leading to delayed cerebral ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage:
Most frequent 7–10 days after initial event
Can lead to ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke
HydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage:
Can be seen within hours of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage or a later complication (chronic)
Occurs from obstruction of blood products and/or reduced absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of CSF
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: may be due to cerebral salt wasting or SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever: most common medical complication
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
AnemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
Cardiopulmonary events
Management
Management may vary depending on practice location. The following information is based on US and UK literature and guidelines. Treatment may be guided by specialist consultation (e.g., neurosurgeryNeurosurgeryNeurosurgery is a specialized field focused on the surgical management of pathologies of the brain, spine, spinal cord, and peripheral nerves. General neurosurgery includes cases of trauma and emergencies. There are a number of specialized neurosurgical practices, including oncologic neurosurgery, spinal neurosurgery, and pediatric neurosurgery. Neurosurgery).
Elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP)
Address any trauma-related conditions:
Administer blood products in blood loss anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
Treat seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures (see below for details)
Keep on nothing-by-mouth status in anticipationAnticipationThe apparent tendency of certain diseases to appear at earlier age of onset and with increasing severity in successive generations.Huntington Disease of possible surgery
Discontinue/reverse anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants:
ProthrombinProthrombinA plasma protein that is the inactive precursor of thrombin. It is converted to thrombin by a prothrombin activator complex consisting of factor Xa, factor V, phospholipid, and calcium ions.Hemostasis complex concentrate (PCC) and vitamin KVitamin KA lipid cofactor that is required for normal blood clotting. Several forms of vitamin K have been identified: vitamin K 1 (phytomenadione) derived from plants, vitamin K 2 (menaquinone) from bacteria, and synthetic naphthoquinone provitamins, vitamin K 3 (menadione). Vitamin k 3 provitamins, after being alkylated in vivo, exhibit the antifibrinolytic activity of vitamin k. Green leafy vegetables, liver, cheese, butter, and egg yolk are good sources of vitamin k.Fat-soluble Vitamins and their Deficiencies, if on warfarinWarfarinAn anticoagulant that acts by inhibiting the synthesis of vitamin K-dependent coagulation factors. Warfarin is indicated for the prophylaxis and/or treatment of venous thrombosis and its extension, pulmonary embolism, and atrial fibrillation with embolization. It is also used as an adjunct in the prophylaxis of systemic embolism after myocardial infarction. Warfarin is also used as a rodenticide.Anticoagulants
Once stabilized, consider transfer to an appropriate facility:
Neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus
Availability of specialists:
Neurosurgeons
Endovascular specialists
Neuroprotective measures[11,13,15,16]
Prevention of delayed cerebral ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage:
Delayed cerebral ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage (DCI) is a major cause of death and is associated with vasospasm.
As stated, vasospasm most frequently is observed 7–10 days after aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms rupture, with resolution noted after 21 days.[17]
Although there is no clear evidence that vasospasm is reduced by nimodipineNimodipineSubarachnoid Hemorrhage, administration of this drug has been shown to improve neurologic outcomes.
Administer to patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
Start as early as possible (< 96 hours after diagnosis)
Recommended dose is 60 mg orally every 4 hours.
IV preparations are not FDA-approved: if oral route is compromised, the contents of the nimodipineNimodipineSubarachnoid HemorrhagecapsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides can be extracted into a syringe and given via a nasogastric tubeNasogastric tubeMalnutrition in children in resource-limited countries.
Goal systolic blood pressure < 160 mm Hg (avoid dropping below 130 mm Hg)
Goal mean arterial pressureMean Arterial PressureMean arterial pressure (MAP) is the average systemic arterial pressure and is directly related to cardiac output (CO) and systemic vascular resistance (SVR). The SVR and MAP are affected by the vascular anatomy as well as a number of local and neurohumoral factors.Vascular Resistance, Flow, and Mean Arterial Pressure < 110 mm Hg
Avoid rapid drops in blood pressure.
Avoid hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension.
Avoid nitratesNitratesNitrates are a class of medications that cause systemic vasodilation (veins > arteries) by smooth muscle relaxation. Nitrates are primarily indicated for the treatment of angina, where preferential venodilation causes pooling of blood, decreased preload, and ultimately decreased myocardial O2 demand.Nitrates, as these may elevate ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP).
Drug options for hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension:[23]
LabetalolLabetalolA salicylamide derivative that is a non-cardioselective blocker of beta-adrenergic receptors and alpha-1 adrenergic receptors.Subarachnoid Hemorrhage
IV injection: 10–20 mg over 2 minutes; followed by 20–80 mg every 10 minutes until SBPSBPAscites is < 160 mm Hg or mean arterial pressureMean Arterial PressureMean arterial pressure (MAP) is the average systemic arterial pressure and is directly related to cardiac output (CO) and systemic vascular resistance (SVR). The SVR and MAP are affected by the vascular anatomy as well as a number of local and neurohumoral factors.Vascular Resistance, Flow, and Mean Arterial Pressure is < 100 mm Hg
IV infusion: 0.5–2 mg/min until a satisfactory response is achieved, then discontinue.
NicardipineNicardipineA potent calcium channel blockader with marked vasodilator action. It has antihypertensive properties and is effective in the treatment of angina and coronary spasms without showing cardiodepressant effects. It has also been used in the treatment of asthma and enhances the action of specific antineoplastic agents.Class 4 Antiarrhythmic Drugs (Calcium Channel Blockers)
IV infusion: 3–5 mg/hr for 15 minutes, increased by 2.5 mg/hr every 15 minutes, adjusted to response.
Maximum rate: 15 mg/hr
Reduce dose gradually once target blood pressure is achieved.
Short-course tranexamic acidTranexamic acidAntifibrinolytic hemostatic used in severe hemorrhage.Hemophilia:[17,22]
A possible consideration is a 24- to 72-hour course of IV tranexamic acidTranexamic acidAntifibrinolytic hemostatic used in severe hemorrhage.Hemophilia if endovascular coilingEndovascular CoilingSubarachnoid Hemorrhage or neurosurgical clipping is suitable but cannot be carried out within 24 hours.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may benefit if early aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms treatment cannot be performed but risks are still uncertain.
May reduce rebleeding risk but has not been proven to improve clinical outcomes.
PhenytoinPhenytoinAn anticonvulsant that is used to treat a wide variety of seizures. The mechanism of therapeutic action is not clear, although several cellular actions have been described including effects on ion channels, active transport, and general membrane stabilization. Phenytoin has been proposed for several other therapeutic uses, but its use has been limited by its many adverse effects and interactions with other drugs.First-Generation Anticonvulsant Drugs has been associated with poor outcomes.[22]
May be continued for months after initial insult (in those at risk for delayed seizure, e.g., intracerebral hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception, prior seizure)[17]
Management of increased ICPIncreased ICPExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage:
Head elevation to 30 degrees
IV mannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics:
Administer 0.25–1 g/kg over 30–60 minutes.
Repeat every 6–8 hours, as needed.
Short-term, controlled hyperventilationHyperventilationA pulmonary ventilation rate faster than is metabolically necessary for the exchange of gases. It is the result of an increased frequency of breathing, an increased tidal volume, or a combination of both. It causes an excess intake of oxygen and the blowing off of carbon dioxide.Respiratory Alkalosis
AnalgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts and antiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics:
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia can raise ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP).
Remember to take into account the sedating effect of opiatesOpiatesOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates.Opioid Analgesics when conducting neurologic assessments.
Neurosurgical and endovascular intervention[11,17,22]
Consult neurosurgeryNeurosurgeryNeurosurgery is a specialized field focused on the surgical management of pathologies of the brain, spine, spinal cord, and peripheral nerves. General neurosurgery includes cases of trauma and emergencies. There are a number of specialized neurosurgical practices, including oncologic neurosurgery, spinal neurosurgery, and pediatric neurosurgery. Neurosurgery and/or endovascular interventionist as soon as a SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage is suspected! The goal is to stop the bleeding, prevent rebleeding, and manage ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) to prevent secondary ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage. Possible interventions include:
May be indicated to relieve ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) in cases of intracerebral hemorrhageIntracerebral HemorrhageIntracerebral hemorrhage (ICH) refers to a spontaneous or traumatic bleed into the brain parenchyma and is the 2nd-most common cause of cerebrovascular accidents (CVAs), commonly known as stroke, after ischemic CVAs. Intracerebral Hemorrhage
May be indicated to relieve ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) in cases of severe cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Cerebrovascular imaging is recommended immediately after aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms repair.
Monitoring and additional management[11,13,25]
Monitoring should be performed in an ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus by specially trained staff equipped to continuously and simultaneously address the following:
Hemodynamic instability:[17]
May require central lines, arterial lines, ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitor
IV fluid infusions (usually normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids) for maintenance of euvolemiaEuvolemiaVolume Depletion and Dehydration
Avoid large amounts of hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation fluids.
Avoid significant volume contraction.
Closely monitor fluid input and output.
Neurologic deterioration:
Focused neurologic exam every 2 hours by qualified ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus nurse
Emergent CT for any acute deterioration
Transcranial DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography) can be used to monitor for vasospasm (arterial narrowing or change in blood velocity).[17]
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever:
Increases cerebral metabolic rate[24]
Antipyretics and cooling measures as indicated to achieve normothermia[17]
ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP):
VentriculostomyVentriculostomySurgical creation of an opening in a cerebral ventricle.Neurosurgery: Intracranial line placed by neurosurgical staff to monitor ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP).
VentriculostomyVentriculostomySurgical creation of an opening in a cerebral ventricle.Neurosurgery also allows for drainage of CSF to reduce ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP).
Electrolyte imbalance:
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia is especially common in this setting.
IV fluid choice and drip rate may be adjusted to maintain eunatremia.
HyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus is associated with poor outcomes, so the following are recommended:
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance monitoring
Maintenance of euglycemia with insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin protocol
When hydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage is present:[11]
Acute hydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage is usually managed by external ventricular drainage or lumbar drainage.
Chronic hydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage is usually managed with a ventricular shunt.
Deep vein thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus (DVTDVTDeep vein thrombosis (DVT) usually occurs in the deep veins of the lower extremities. The affected veins include the femoral, popliteal, iliofemoral, and pelvic veins. Proximal DVT is more likely to cause a pulmonary embolism (PE) and is generally considered more serious. Deep Vein Thrombosis)/pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism (PE) prophylaxisProphylaxisCephalosporins:
Mechanical means are preferred.
AnticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants are generally avoided until definitive repair has been undertaken.
Follow-up[5,9,11]
Care plan:
Develop and document a personalized care plan, including details of follow-up care.
Give a copy to the patient (or family/caregivers).
Include details of whom to contact at the specialist center for ongoing advice and support.
NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant:
Consider follow-up neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant for people with an aneurysmal SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
The frequency of follow-up imaging is based on:
Type and outcome of any neurosurgical or endovascular intervention
Presence of non-culprit aneurysms: A multidisciplinary team including a neuroradiologist and a neurosurgeon should evaluate options for these.
Estimated risk of rebleeding
Risk of planned/subsequent interventions
Patient’s preference
Ongoing measures:
Encourage smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation and direct to support resources/groups.
Do not withhold solely on the basis of SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage if the culprit aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms has been secured by coiling or clipping.
Balance harm of not taking medication with risk of future SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage.
May be due to chronic hydrocephalusHydrocephalusExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage if the person has features of raised ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP).
ScreeningScreeningPreoperative Care: It is reasonable to offer screeningScreeningPreoperative Care (neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant) to 1st-degree relatives of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage for saccular aneurysmsSaccular aneurysmsBrain Aneurysms.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[5]
Survivors may have significant morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status:
Increased incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of cardiovascular events
Neurologic, cognitive, and memoryMemoryComplex mental function having four distinct phases: (1) memorizing or learning, (2) retention, (3) recall, and (4) recognition. Clinically, it is usually subdivided into immediate, recent, and remote memory.Psychiatric Assessment deficits are common.
SleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep disorders and mood disorders are common.
Persistent seizure disorder is common.
AnosmiaAnosmiaComplete or severe loss of the subjective sense of smell. Loss of smell may be caused by many factors such as a cold, allergy, olfactory nerve diseases, viral respiratory tract infections (e.g., COVID-19), aging and various neurological disorders (e.g., Alzheimer disease).Cranial Nerve Palsies is common.
Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke: an ischemic infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage of the cerebral parenchyma caused by occlusion of a cerebral artery by atherosclerotic lesions or cardioembolic emboli. Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke presents with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/level of consciousness that depends on the size and location of the infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage. Diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management includes initial stabilization, possible cerebrovascular intervention, addressing identifiable underlying etiologies (severe hypertensionSevere hypertensionA confirmed blood pressure ≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic.Uncontrolled Hypertension, embolus), and management of cardiovascular risk factors.
Other hemorrhagic cerebral conditions: carotid/cerebral artery dissection, epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage, intraparenchymal hemorrhage, and subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage are other hemorrhagic manifestations of the cerebral vasculature that can present with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/level of consciousness. Diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management depends on the hemorrhagic etiology and includes initial stabilization, neurosurgical/endovascular consultation, management of ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), and monitoring in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus.
Hypertensive encephalopathyEncephalopathyHyper-IgM Syndrome: neurologic deficit and/or altered mental statusAltered Mental StatusSepsis in Children/level of consciousness that presents in the setting of severe hypertensionSevere hypertensionA confirmed blood pressure ≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic.Uncontrolled Hypertension. Diagnosis is based on the presence of elevated blood pressure and neurologic signs/symptoms. NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant is useful to rule out ischemic or hemorrhagic cerebrovascular accidentCerebrovascular accidentAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke. Management centers around careful acute lowering of the blood pressure and long-term blood pressure management.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose a subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage (SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage), which is bleeding into the subarachnoid spaceSubarachnoid spaceThe space between the arachnoid membrane and pia mater, filled with cerebrospinal fluid. It contains large blood vessels that supply the brain and spinal cord.Subarachnoid Hemorrhage. The codes are highly specific to the location and cause, most commonly a ruptured cerebral aneurysmCerebral aneurysmBrain aneurysms, also known as intracranial or cerebral aneurysms, are dilations of the arteries along points of weakness in the brain. The majority of the aneurysms are berry (saccular) in nature and located within the anterior circulation of the circle of Willis.Brain Aneurysms.
Coding System
Code
Description
ICD-10-CM
I60.7
Nontraumatic subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage from unspecified intracranial artery
ICD-10-CM
I60.2
Nontraumatic subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage from anterior communicating artery
Evaluation & Workup:
A non-contrast head CT is the first step. If negative but suspicion is high, a lumbar punctureLumbar PunctureFebrile Infant is performed to check for blood in the CSF. A CT angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery is then used to find the source of the bleed.
Coding System
Code
Description
CPT
70450
Computed tomography, head or brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification; without contrast material
CPT
62270
Spinal puncture, lumbar, diagnostic
CPT
70496
Computed tomography angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery, head, with contrast material(s)
Procedures/Interventions:
These codes are for the procedures used to secure a ruptured aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms and prevent re-bleeding: endovascular coilingEndovascular CoilingSubarachnoid Hemorrhage or neurosurgical clipping.
Coding System
Code
Description
CPT
61624
Transcatheter permanent occlusion or embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding (eg, for tumorTumorInflammation destruction, to achieve hemostasisHemostasisHemostasis refers to the innate, stepwise body processes that occur following vessel injury, resulting in clot formation and cessation of bleeding. Hemostasis occurs in 2 phases, namely, primary and secondary. Primary hemostasis involves forming a plug that stops the bleeding temporarily. Secondary hemostasis involves the activation of the coagulation cascade.Hemostasis, to occlude a vascular malformation), percutaneous, any method; central nervous systemCentral nervous systemThe main information-processing organs of the nervous system, consisting of the brain, spinal cord, and meninges.Nervous System: Anatomy, Structure, and Classification (intracranial, spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy)
CPT
61700
Surgery of aneurysmAneurysmAn aneurysm is a bulging, weakened area of a blood vessel that causes an abnormal widening of its diameter > 1.5 times the size of the native vessel. Aneurysms occur more often in arteries than in veins and are at risk of dissection and rupture, which can be life-threatening. Thoracic Aortic Aneurysms, intracranial; carotid circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment
Hacein-Bey, L, Provenzale, JM. (2011). Current imaging assessment and treatment of intracranial aneurysms. AJR. American journal of roentgenology, 196(1):32–44. https://doi.org/10.2214/AJR.10.5329
Carley, S, Harrison, M. (2004). Timing of lumbar puncture in suspected subarachnoid haemorrhage. Emergency Medicine Journal 22(2). https://emj.bmj.com/content/22/2/121.2
National Institute for Health and Care Excellence (2022). Subarachnoid haemorrhage caused by ruptured aneurysm: diagnosis and management. Retrieved Jul 26, 2026, from https://www.nice.org.uk/guidance/ng228
Cruickshank, A., Auld, P., Beetham, R., Burrows, G., Egner, W., Holbrook, I., Keir, G., Lewis, E., Patel, D., Watson, I., White, P., & UK NEQAS Specialist Advisory Group for External Quality Assurance of CSF Proteins and Biochemistry (2008). Revised national guidelines for analysis of cerebrospinal fluid for bilirubin in suspected subarachnoid haemorrhage. Annals of clinical biochemistry, 45(Pt 3), 238–244. https://doi.org/10.1258/acb.2008.007257
Marcolini, E, Hine, J. (2019). Approach to the diagnosis and management of subarachnoid hemorrhage. Western Journal of Emergency Medicine 20(2):203–211
Muehlschlegel, S. (2018). Subarachnoid hemorrhage. Lifelong Learning in Neurology 24(6):1623–1657
Connolly, E, Rabinstein, A, et al. (2012). Guidelines for the management of aneurysmal subarachnoid hemorrhage. Stroke 43(6):1711–1737.
Linn, F, Rinkel, G, et al. (2000). The notion of “warning leaks” in subarachnoid haemorrhage: are such patients in fact admitted with a rebleed? Journal of Neurology, Neurosurgery & Psychiatry 68:332–336.
Fodstad, H, Kelly, P, et al.(2006). History of the cushing reflex. Neurosurgery 59(5):1132–1137.
Perry, JJ, Alyahya B, Sivilotti ML, et al. (2015). Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ 350:h568. https://doi.org/10.1136/bmj.h568
Rosen, DS, Macdonald, RL. (2005). Subarachnoid hemorrhage grading scales: a systematic review. Neurocritical Care 2(2):110–118. https://doi.org/10.1385/NCC:2:2:110
Maher, M, Schweizer, TA, Macdonald, RL. (2020). Treatment of spontaneous subarachnoid hemorrhage: guidelines and gaps. Stroke 51(4):1326–1332. https://doi.org/10.1161/STROKEAHA.119.025997
Peacock, WF, 4th, Hilleman, DE, Levy, PD, Rhoney, DH, Varon, J. (2012). A systematic review of nicardipine vs labetalol for the management of hypertensive crises. American Journal of Emergency Medicine 30(6):981–993. https://doi.org/10.1016/j.ajem.2011.06.040
Busija, DW, Leffler, CW, Pourcyrous, M. (1988). Hyperthermia increases cerebral metabolic rate and blood flow in neonatal pigs. American Journal of Physiology 255(2 Pt 2):H343–H346. https://doi.org/10.1152/ajpheart.1988.255.2.H343
Greenberg, SM, et al. (2022). 2022 guideline for the management of patients with spontaneous intracerebral hemorrhage: A guideline from the American Heart Association/American Stroke Association. Stroke, 53:e282-e361. https://www.ahajournals.org/doi/full/10.1161/STR.0000000000000407
Create your free account or log in to continue reading!