Labor is the normal physiologic process defined as uterine contractions resulting in dilatation and effacement of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, which culminates in expulsion of the fetus and the products of conception. Labor has 3 stages: the 1st stage starts with the onset of regularRegularInsulin contractions, the 2nd stage starts with full cervical dilation, and the 3rd stage starts immediately after fetal delivery and ends with delivery of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity. The primary factors required for labor to progress normally are the three PsPSInvasive Mechanical Ventilation: power (uterine contractions), passenger (the fetus), and passage (the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 "hip" bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy). Labor may become abnormally protracted and require augmentation, usually with oxytocin, to prevent maternal and fetal complications.
Labor is defined as regularRegularInsulin uterine contractions that cause cervical dilation and effacement, leading to delivery of the fetus and the products of conception. Characteristics of normal labor include:
Gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care: occurs at 37–42 weeks of gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care (full-term)
Onset: spontaneous (as opposed to induced)
Progression: spontaneous, without complications
There are subtle differences in normal labor between primiparous and multiparous women (reviewed below).
Primiparous: a woman’s 1st delivery
Multiparous: a woman with prior deliveries
Monitoring progress of labor
Labor progress is followed by serial cervical exams to assess dilation, effacement, and fetal station.
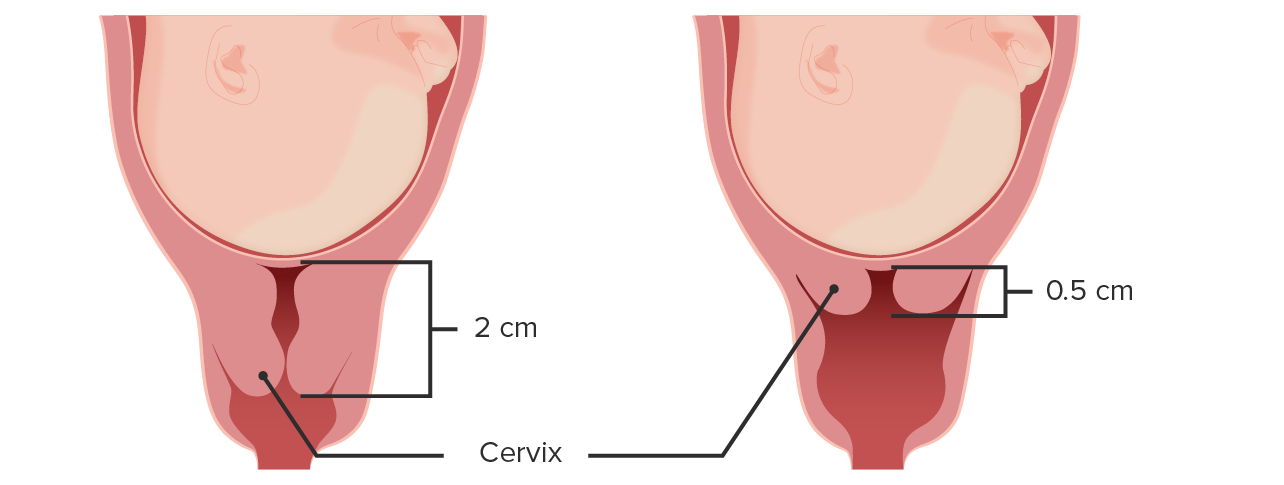
CervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy starts at > 2 cm → effaces to paper thin (full effacement)
Reported as a percentage of progress
Full effacement: 100% effaced
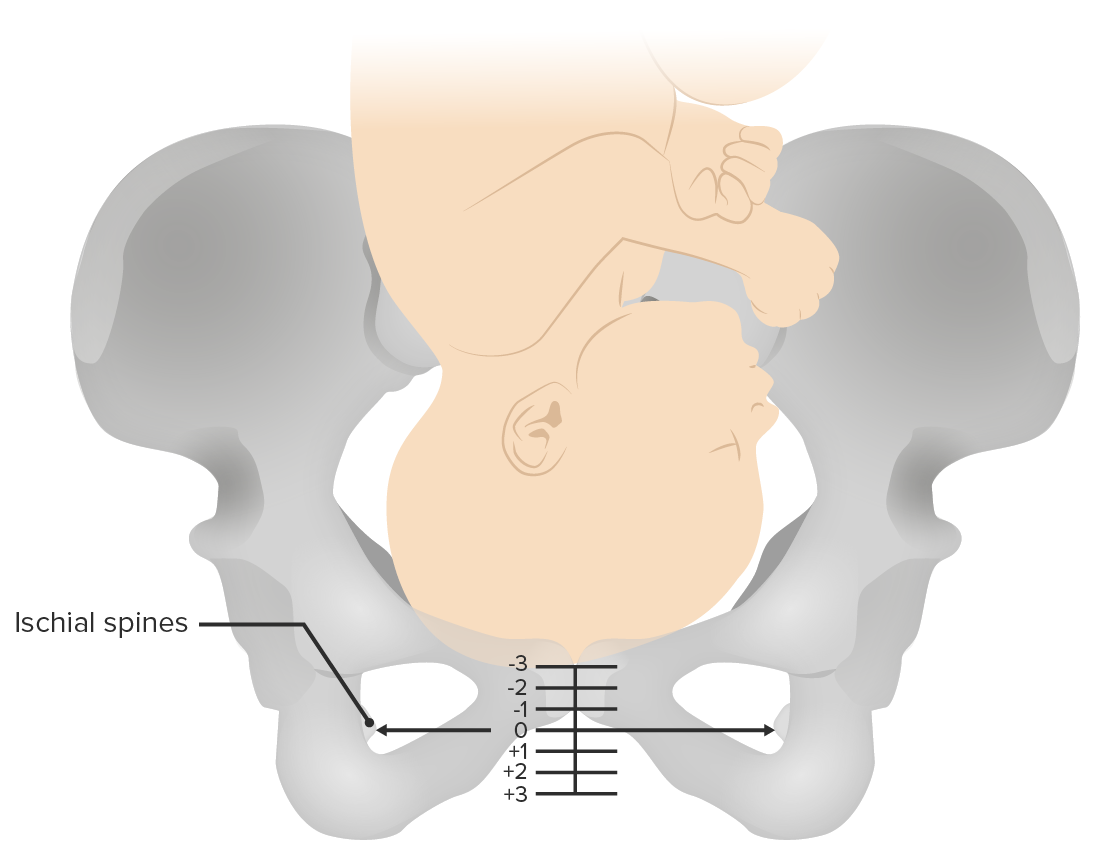
Fetal station:
How high (or low) the presenting fetal part is compared to the maternal ischial spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy
Reported in centimeters:
Positive numbers denote a lower fetal station, closer to the vaginal introitus
Negative numbers denote a fetal station higher in the pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Fetal head at the introitus: +3–5 cm
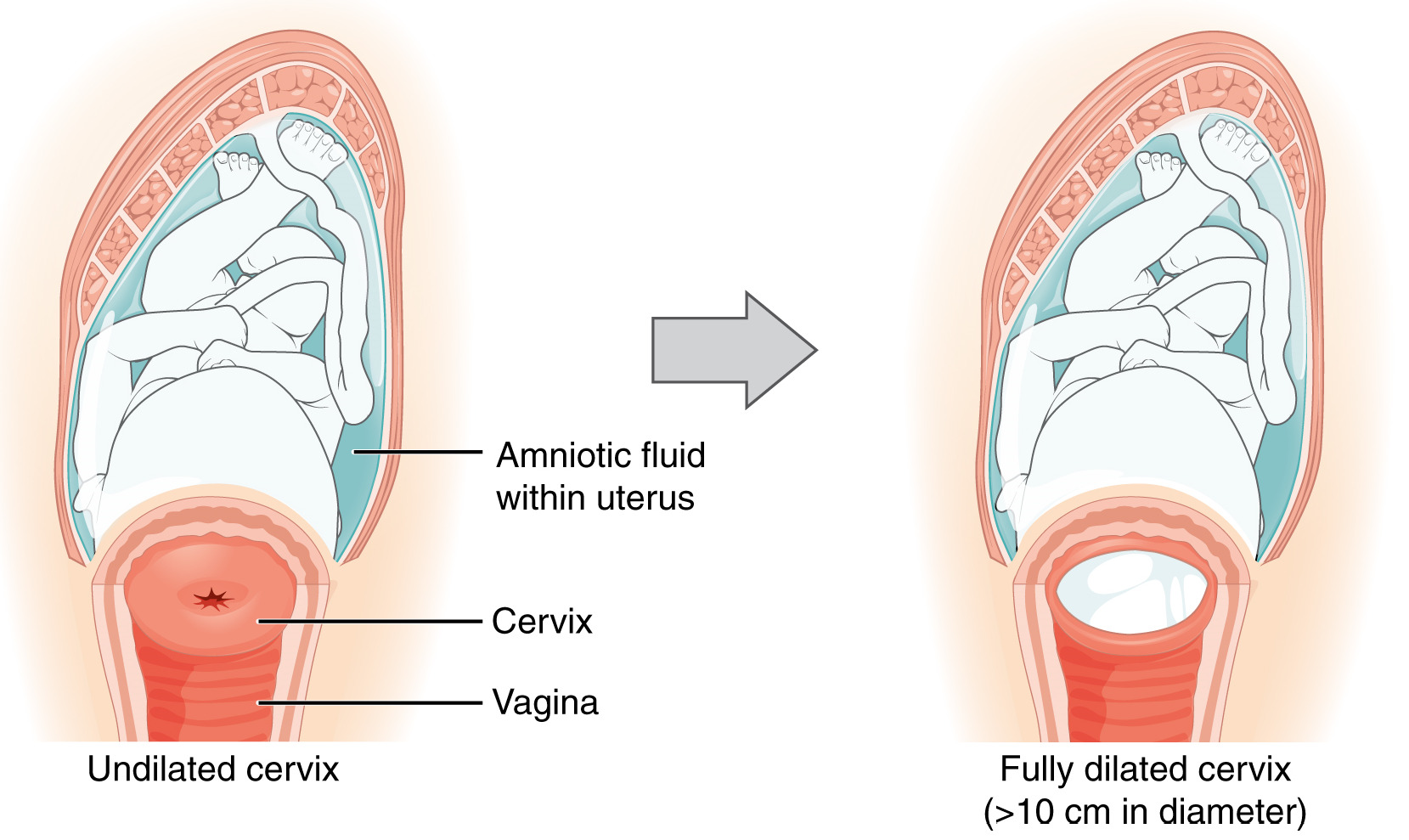
Cervical changes during the first stage of labor: At the onset of the labor, the cervix is usually undilated. The first stage ends when the cervix is fully dilated (10 cm).
Image: “2920 Stages of Childbirth-02” by OpenStax College. License: CC BY 4.0, cropped by Lecturio.
Fetal station:
The distance of the presenting fetal part from the maternal ischial spines is measured in centimeters. Negative numbers denote a higher fetal station, while positive numbers denote a lower fetal station as the fetus descends in the birth canal.
Image by Lecturio.
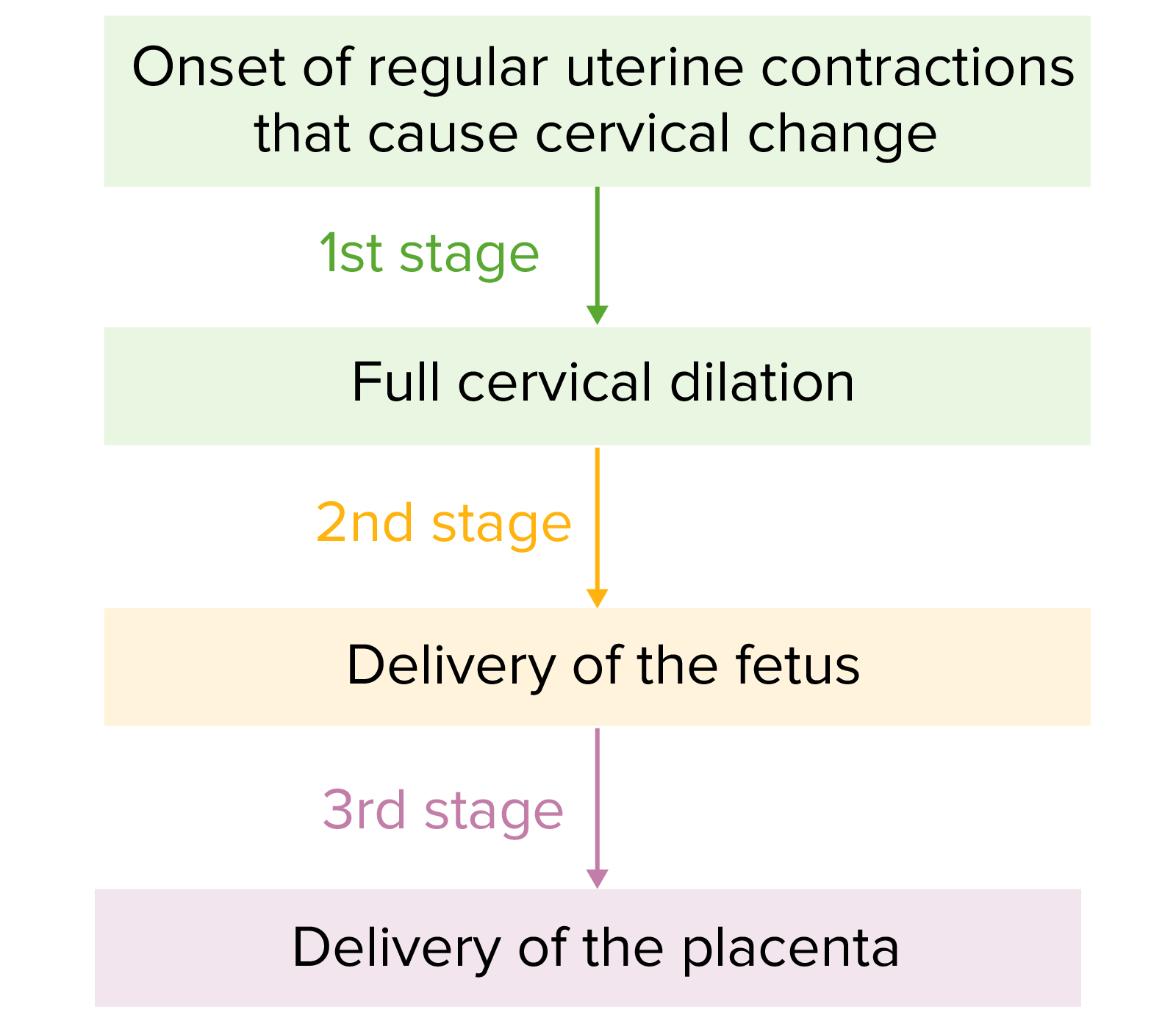
Stages of labor
There are 3 stages of labor:
The 1st stage:
Begins with the onset of regularRegularInsulin uterine contractions that cause cervical change
Ends with full cervical dilation (10 cm)
The 2nd stage:
Begins when the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy reaches full dilation (10 cm)
Ends with delivery of the fetus
The 3rd stage:
Begins immediately after delivery of the fetus
Ends with delivery of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity
For labor to progress normally, there needs to be adequate power from uterine contractions, the fetus needs to tolerate the contractions, and the fetus needs to fit through the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy. These requirements are referred to as the 3 PsPSInvasive Mechanical Ventilation: Power, Passenger, and Passage.
Power: Uterine contractions
Contractions must be powerful enough to dilate the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy and expel the fetus
Can be measured by:
External pressure transducerTransducerA device placed on the patient’s body to visualize a targetUltrasound (Sonography) (tocometry): measures frequency and strength of contractions relative to each other
Internal uterine pressure catheter (IUPC): measures frequency and numerical strength of contractions in Montevideo units (MVUs)
Montevideo units: the strength of all contractions are summated within a 10-minute period:
“Adequate power” to effect delivery: ≥ 200 MVUs in 10 minutes
“Inadequate power” is a cause of abnormal labor progress.
Passenger: Fetus
Multiple characteristics of the fetus are required in order to safely deliver vaginally. The fetal head must ultimately be flexed and directly aligned with the maternal spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy in order to fit through the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy.
Presentation: based on the “presenting part” of the fetus at the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy:
Vertex: head down
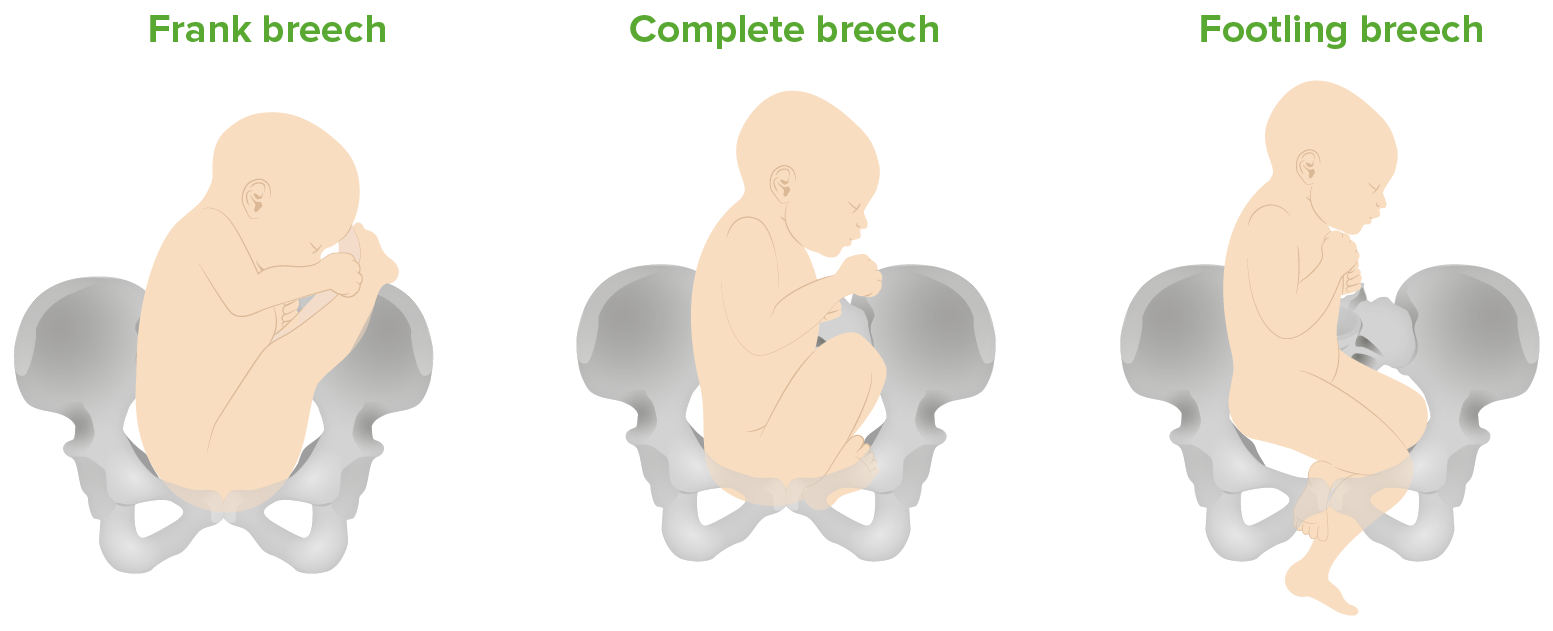
Breech:
Frank breech: bottom down, legs extended
Complete breech: bottom down, legs flexed
Footling breech: feet down
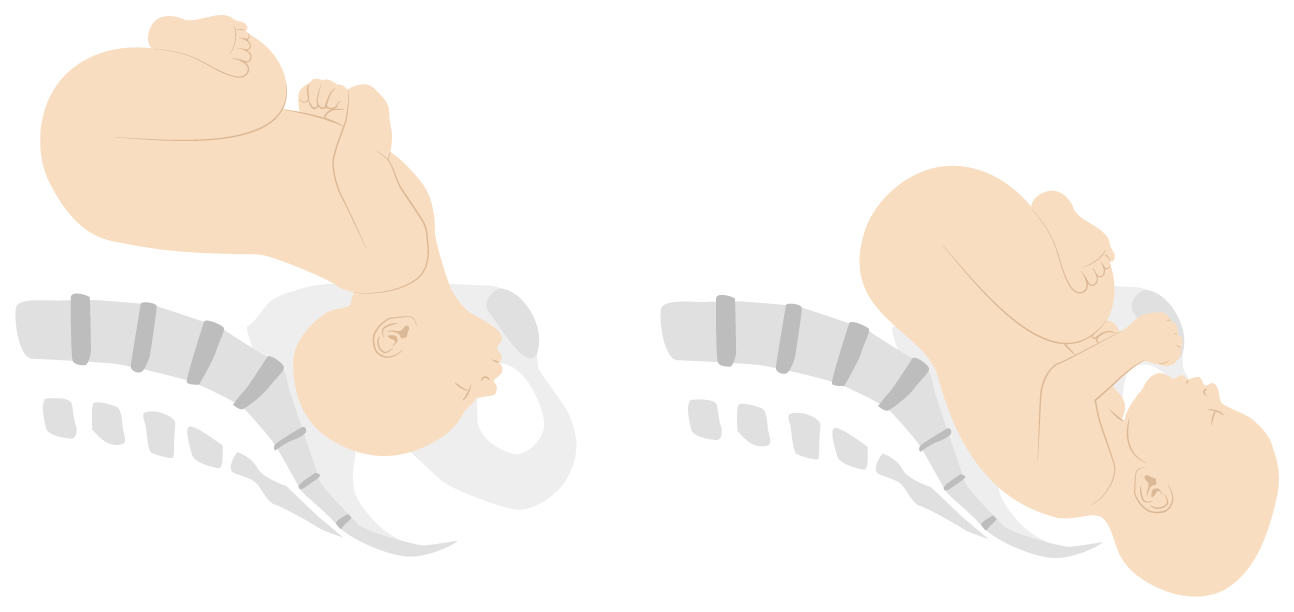
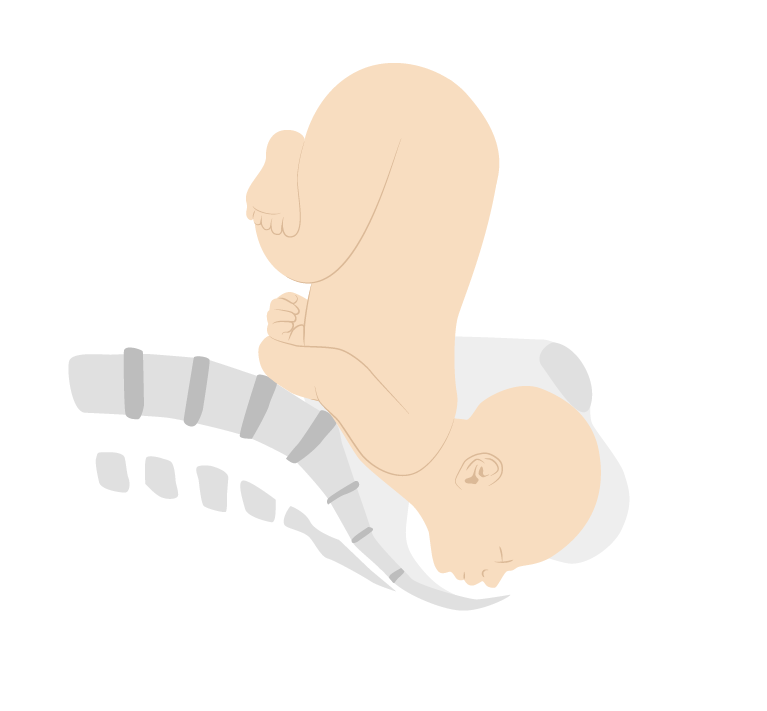
Face:
Mentum anterior (MA): chinChinThe anatomical frontal portion of the mandible, also known as the mentum, that contains the line of fusion of the two separate halves of the mandible (symphysis menti). This line of fusion divides inferiorly to enclose a triangular area called the mental protuberance. On each side, inferior to the second premolar tooth, is the mental foramen for the passage of blood vessels and a nerve.Melasma is anterior, face can flex → compatible with vaginal delivery
Mentum posterior (MP): chinChinThe anatomical frontal portion of the mandible, also known as the mentum, that contains the line of fusion of the two separate halves of the mandible (symphysis menti). This line of fusion divides inferiorly to enclose a triangular area called the mental protuberance. On each side, inferior to the second premolar tooth, is the mental foramen for the passage of blood vessels and a nerve.Melasma is posterior, face cannot flex, incompatible with vaginal delivery
Remember: “MA can, PA can’t” for vaginal deliveries
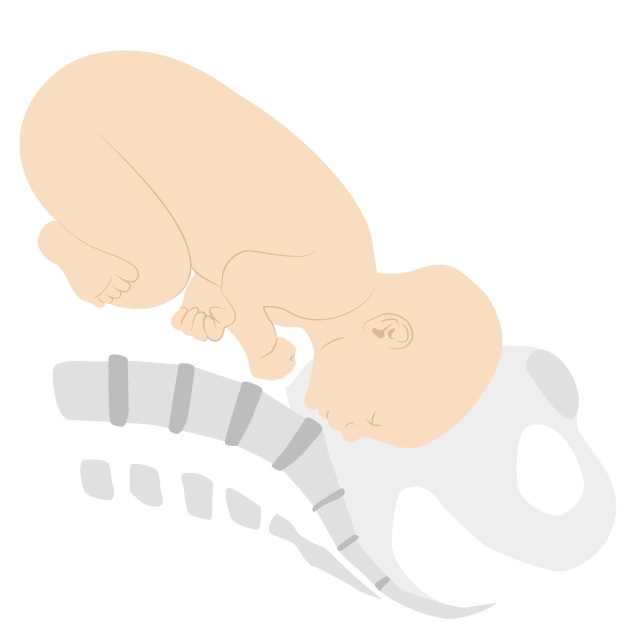
Brow: foreheadForeheadThe part of the face above the eyes.Melasma down, large diameter, incompatible with vaginal delivery
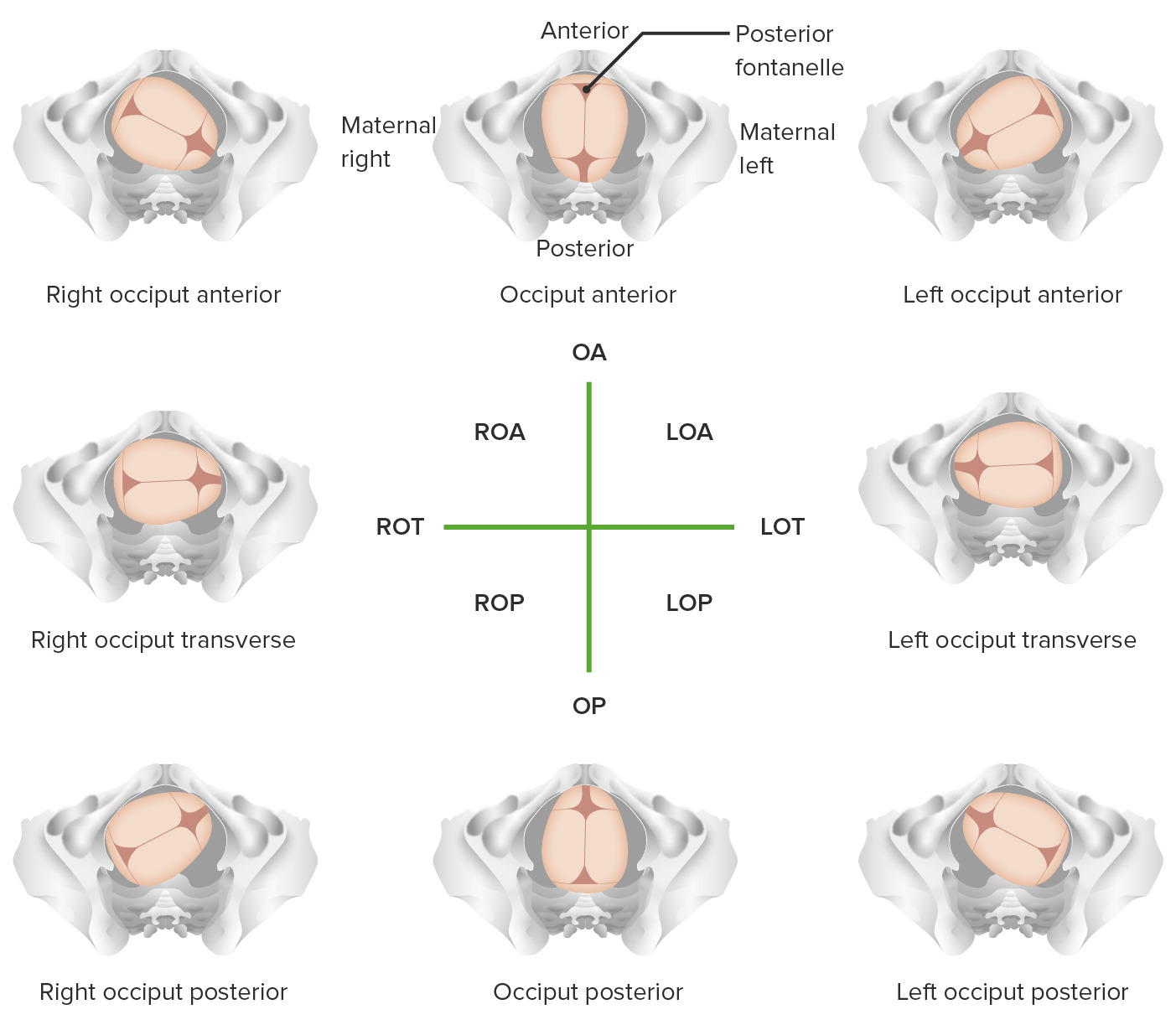
Positions:orientationOrientationAwareness of oneself in relation to time, place and person.Psychiatric Assessment of the fetal head in relation to the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy in vertex presentations:
Occiput anterior (OAOAOsteoarthritis (OA) is the most common form of arthritis, and is due to cartilage destruction and changes of the subchondral bone. The risk of developing this disorder increases with age, obesity, and repetitive joint use or trauma. Patients develop gradual joint pain, stiffness lasting < 30 minutes, and decreased range of motion.Osteoarthritis): fetus is facing maternal spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy; easiest for delivery
Occiput posterior (OP): fetus is facing maternal bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess; more challenging
Occiput transverse (OT): fetal head is sideways (facing a maternal hip)
The fetal head will not fit under the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types in this position.
Fetal toleranceTolerancePharmacokinetics and Pharmacodynamics of labor: infant must tolerate the relative ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage that occurs during uterine contractions without becoming acidotic
Normal size infant: infant must fit through maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Number of infants:
Singletons and twins are candidates for a trial of labor
Surviving triplets and higher-order multiples should be delivered via cesarean
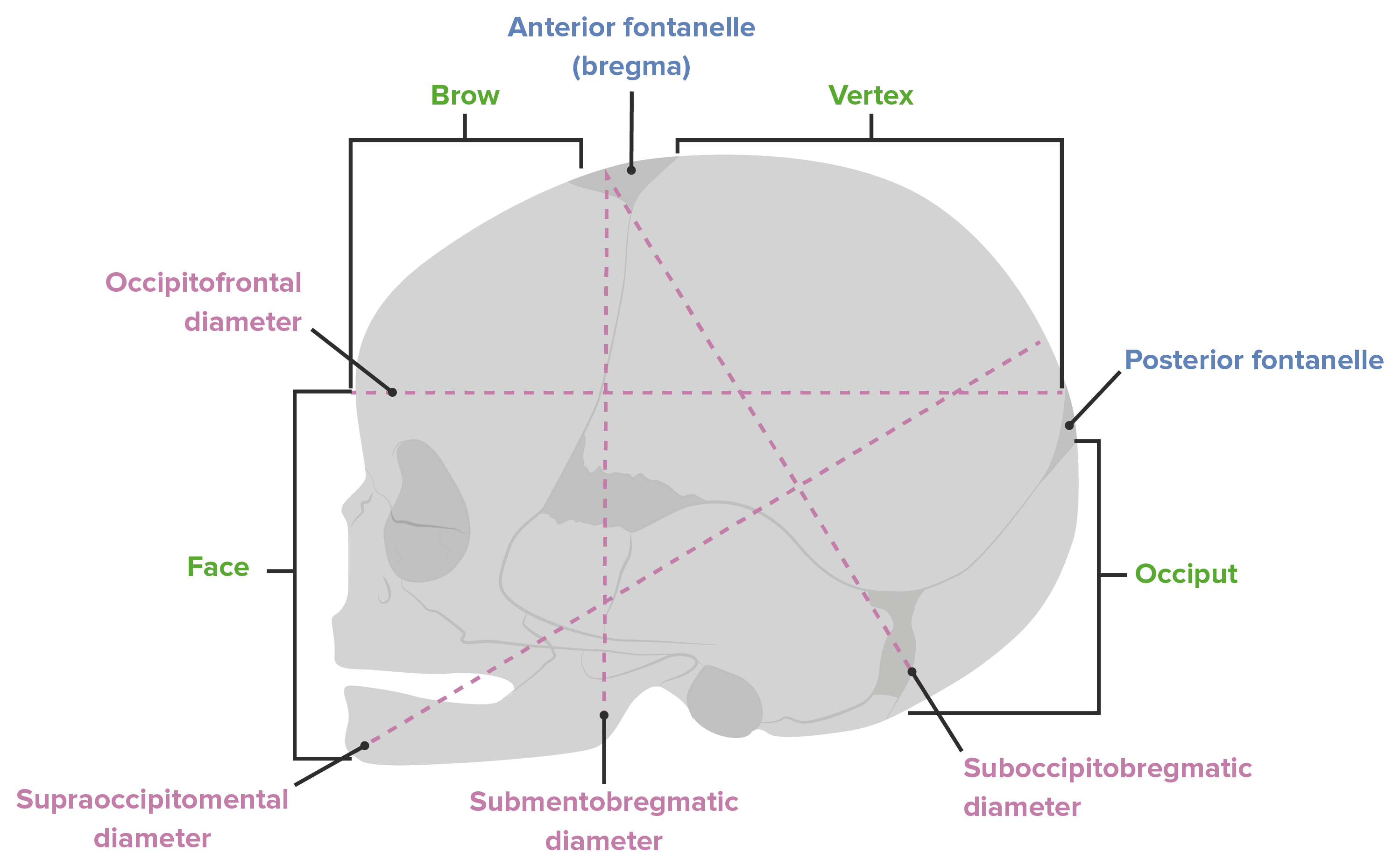
Diameters of the fetal head:
Vertex presentation: suboccipitobregmatic diameter of approximately 9.5 cm
Vertex presentation with deflexed head: occipitofrontal diameter of approximately 11.5 cm
Brow presentation: supraoccipitomental diameter of approximately 13 cm
Face presentation: submentobregmatic diameter of approximately 9.5 cm
Face presentations. Mentum anterior positions are able to flex and allow passage of the fetal head, however mentum posterior positions are unable to flex and thus cannot be delivered vaginally.
Overview of different vertex positions LOA: left occiput anterior LOP: left occiput posterior LOT: left occiput transverse OA occiput anterior OP: occiput posterior ROA: right occiput anterior ROP: right occiput posterior ROT:
right occiput transverse
Passage: PelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
The maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy must be large enough to accommodate the fetus. The pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy is assessed as “adequate” or “inadequate” for a trial of labor on the initial exam.
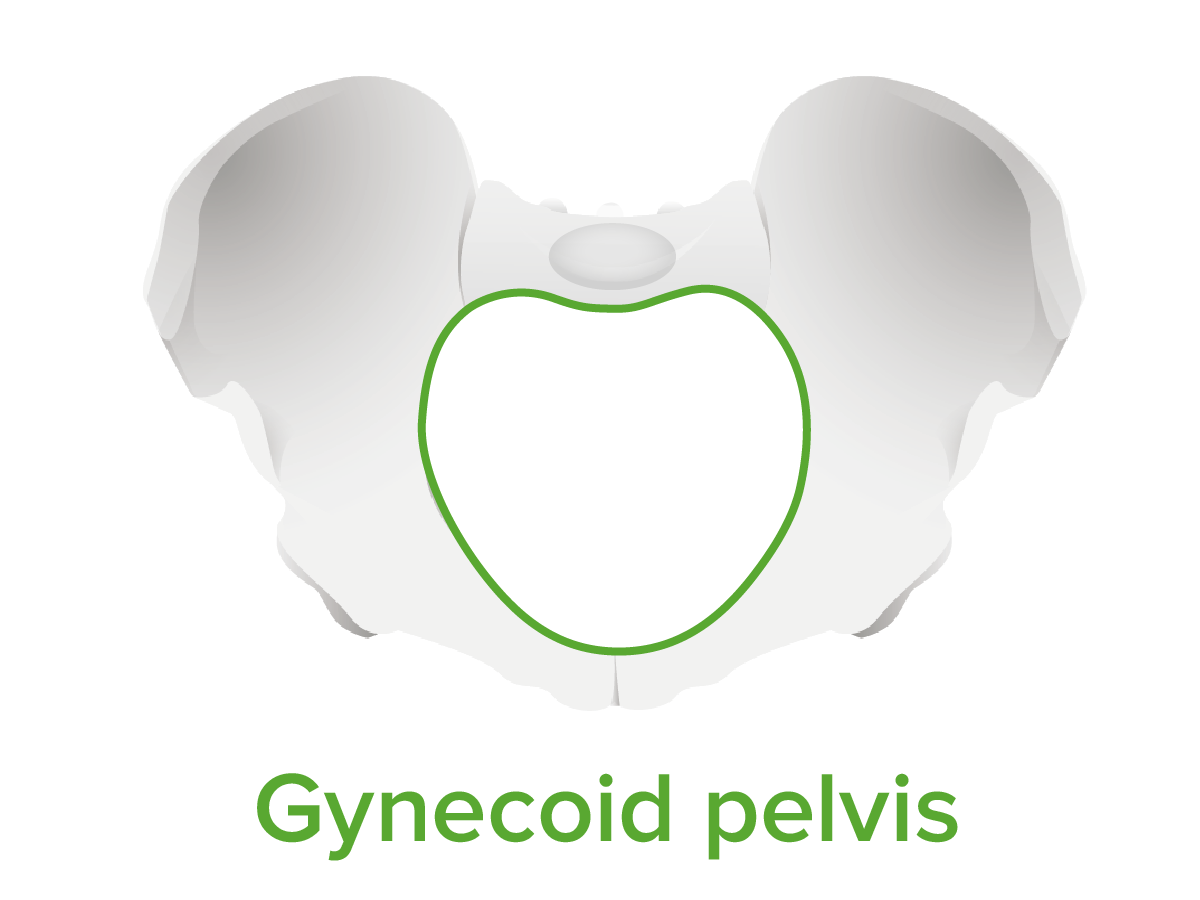
PelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy shapes: classified based on the shape of the pelvic inletPelvic inletPelvis: Anatomy:
Gynecoid: round and most spacious → most easily allows the fetal head to rotate to OAOAOsteoarthritis (OA) is the most common form of arthritis, and is due to cartilage destruction and changes of the subchondral bone. The risk of developing this disorder increases with age, obesity, and repetitive joint use or trauma. Patients develop gradual joint pain, stiffness lasting < 30 minutes, and decreased range of motion.Osteoarthritis
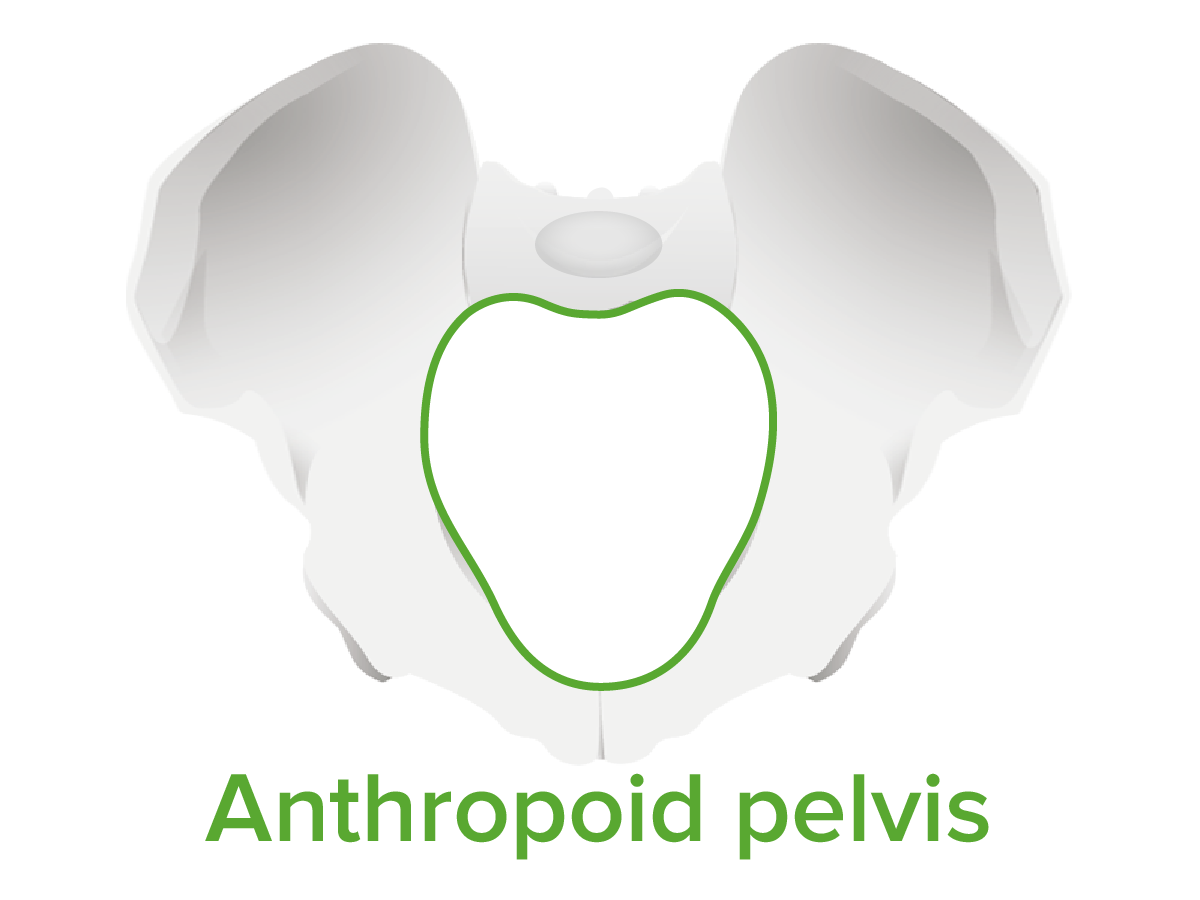
Anthropoid: longer anteroposterior diameter and narrow → more commonly causes the head to rotate to OP
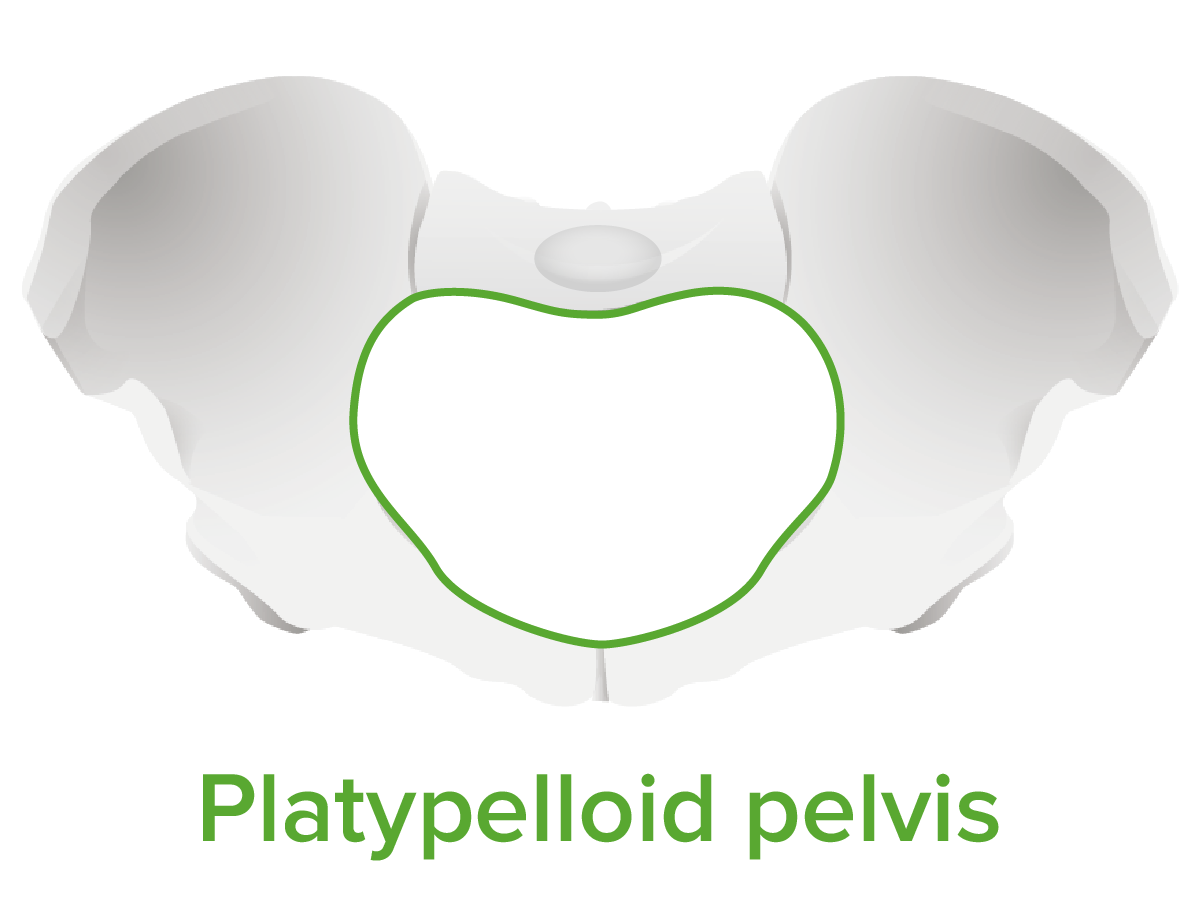
Platypelloid: wider and narrow → more commonly causes the head to stay OT
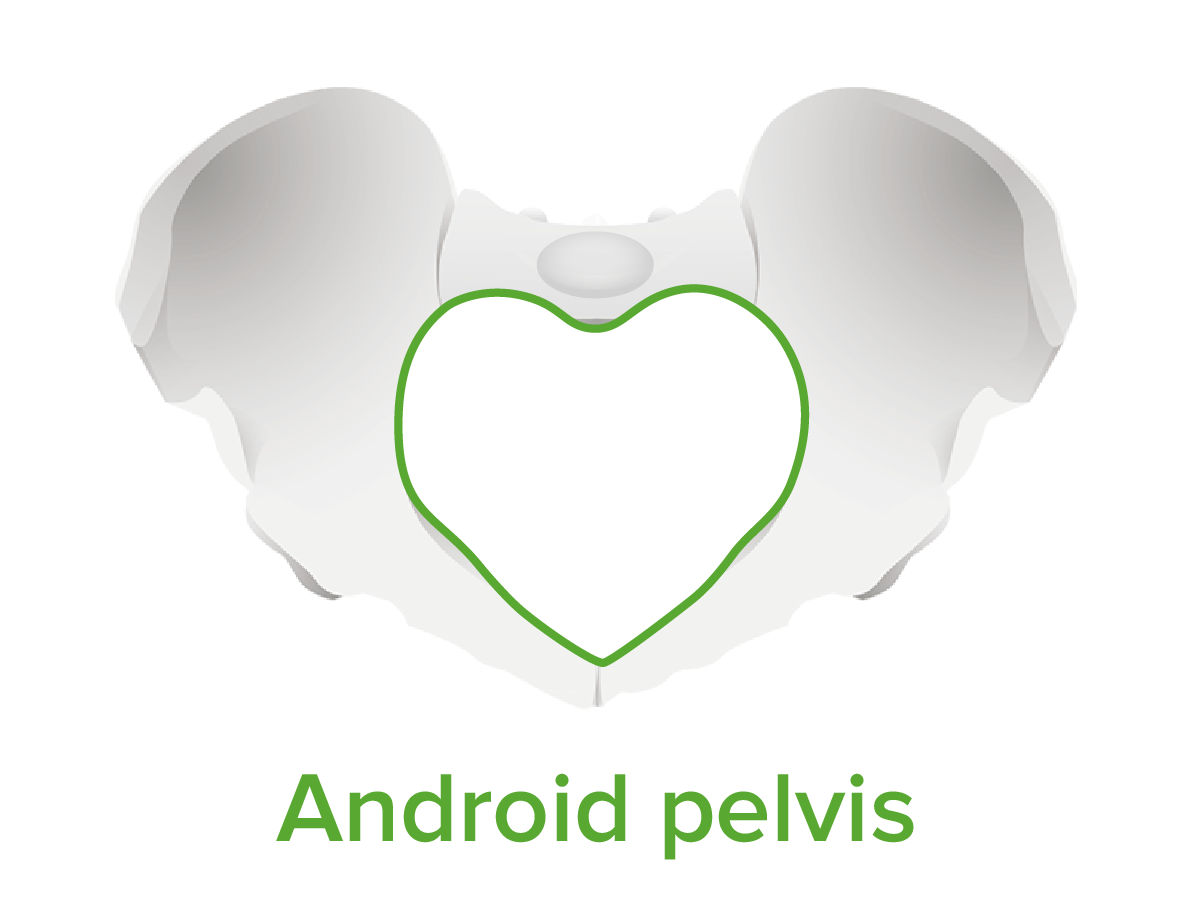
Android: heart shaped → fetal head may have difficulty engaging
Clinical relevance of pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy shape:
Difficult to determine on exam
No shape is a contraindication for a trial of labor.
Gynecoid is the easiest for vaginal delivery
Android and platypelloid are the most difficult for vaginal delivery
May contribute to abnormal labor patterns
Gynecoid pelvis:
The female pelvis is classified based on the shape of the pelvic inlet. The gynecoid pelvis is ideal for delivery, due to its round, spacious shape.
Image by Lecturio.
Anthropoid pelvis:
The female pelvis is classified based on the shape of the pelvic inlet. The anthropoid pelvis has a longer anterior-posterior length.
Image by Lecturio.
Platypelloid pelvis:
The female pelvis is classified based on the shape of the pelvic inlet. The platypelloid pelvis is wide and narrow.
Image by Lecturio.
Android pelvis:
The female pelvis is classified based on the shape of the pelvic inlet. The android pelvis has a heart-shaped inlet.
Starts with the onset of regularRegularInsulin contractions that result in:
Cervical change (dilation and effacement)
Descent of the fetus
Ends with full cervical dilation (10 cm)
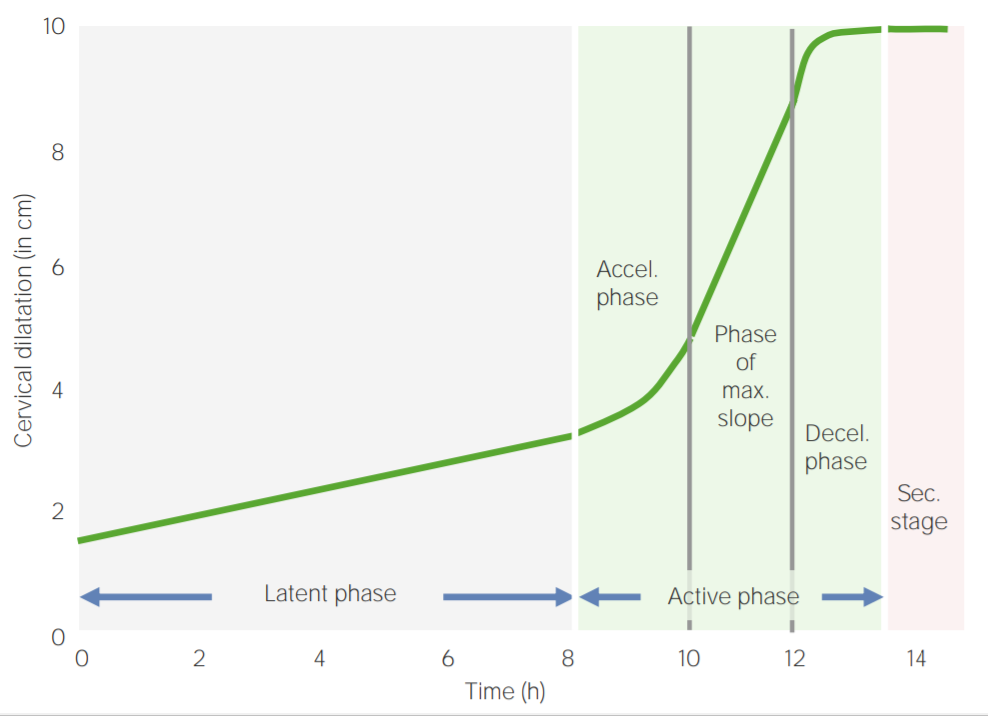
Divided into latent and active phases
Divisions and typical timing of the 1st stage of labor: Accel.: acceleration
Decel.: deceleration Max: maximum
Image by Lecturio.
Latent phase
In the late 3rd trimester, irregular contractions and runs of nonpersistent regularRegularInsulin contractions are common. The latent phase is the establishment of true labor, with regularRegularInsulin persistent contractions that will continue through delivery.
Dilation: 0 to 4–6 cm
Effacement:variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Primiparous: cervical effacement usually occurs before significant dilation
Multiparous: dilation usually precedes significant effacement
AnesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts is generally notrequired.
Typical duration:
Primiparous: < 20 hours
Multiparous: < 14 hours
Active phase
The active phase is a time of more rapid cervical change leading up to delivery.
Dilation: 6–10 cm
Primiparous: 1.2 cm/hour
Multiparous: 1.5 cm/hour
Effacement: continues to 100%
Station: progressive descent to at least the ischial spines (0 station)
AnesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts is often requested.
Table: Length of the 1st stage of labor
Primiparous
Multiparous
Latent labor
Lasts < 20 hours
Lasts < 14 hours
Active labor
1.2 cm/hour
1.5 cm/hour
Latent phase: onset of contractions until 4–6 cm cervical dilation
Active phase: begins at 4‒6 cm dilation and lasts until the cervix is fully dilated at 10 cm
Labor management
General management:
Continuous care and emotional support to the mother
Ambulation in low-riskwomen
Adequate hydration
Maternal assessment:
Labor progression: serial cervical exams
Contraction adequacy: Assess strength and frequency via palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination and/or monitoring.
Vital signs
Urine output
Fetal assessment:
Intermittent auscultation of the fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology (lowest-risk women only)
Continuous cardiotocography (majority of women)
Includes women with any medical painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways management
Includes most women with any medical or obstetric complications
Abnormalities in the 1st stage of labor
Table: Diagnosis and management of abnormalities in the 1st stage of labor
CervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy is ≥ 6 cm and
Dilating < 1 cm over 2 hours
Oxytocin
Amniotomy (if membranes are not already ruptured)
Active phase arrest
CervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy is ≥ 6 cm with ruptured membranes and:
No cervical change for ≥ 4 hours despite adequate contractions or
No cervical change for ≥ 6 hours of oxytocin administration if contractions are inadequate
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery (CD)
Table: Etiologies and management of abnormalities in the first stage of labor
Etiology
Management
Power
Inadequate power: < 200 MVUs measured with an IUPC
Pitocin: to ↑ contraction strength
Passenger
Abnormal presentation:
Breech
Face
Brow
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery recommended for:
Breech
Brow
Face: mentum posterior
Observation:
Face: mentum anterior
Abnormal position:
Occiput posterior
Occiput transverse
Observation
Attempt manual rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays
Fetal intolerance to labor / fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology abnormalities
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
PelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Cephalopelvic disproportion: fetal head does not fit through the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
MVU: Montevideo unit
IUPC: Internal uterine pressure catheter
The 2nd Stage of Labor
The 2nd stage of labor begins with complete dilatation of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy and ends with delivery of the infant.
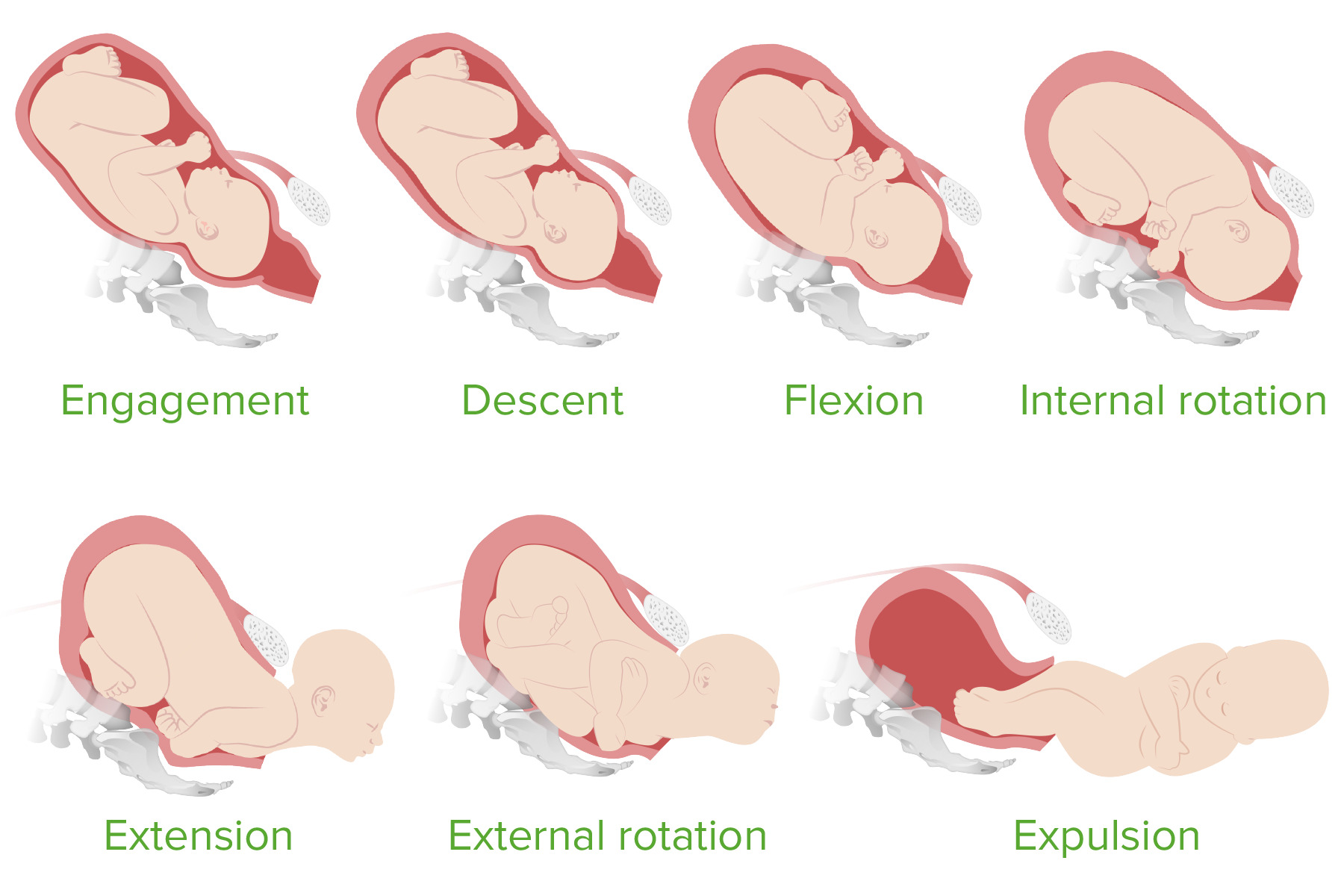
The cardinal movements of labor
The cardinal movements of labor describe the movements a fetus goes through as it moves through the maternal pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy. These movements align the largest parts of the infant with the largest diameter through the pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy (the anteroposterior diameter between the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and the sacrumSacrumFive fused vertebrae forming a triangle-shaped structure at the back of the pelvis. It articulates superiorly with the lumbar vertebrae, inferiorly with the coccyx, and anteriorly with the ilium of the pelvis. The sacrum strengthens and stabilizes the pelvis.Vertebral Column: Anatomy).
Fetal head is in an OT position: looking sideways, with the fetal head aligned with the fetal spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy
Descent: downward passage of the fetal head through the pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Passive flexionFlexionExamination of the Upper Limbs of the fetal head (fetal chinChinThe anatomical frontal portion of the mandible, also known as the mentum, that contains the line of fusion of the two separate halves of the mandible (symphysis menti). This line of fusion divides inferiorly to enclose a triangular area called the mental protuberance. On each side, inferior to the second premolar tooth, is the mental foramen for the passage of blood vessels and a nerve.Melasma touches the fetal chest) as the head is pushed against maternal bony structures
Allows the narrowest diameter of the head to present
RotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of the fetal head to an anteroposterior direction
This rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays turns the fetal head relative to its own spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy.
Example: The fetal head is now looking down, while the fetal body is still mostly facing to the side.
This prepares the fetal head to move under the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types in the next step
ExtensionExtensionExamination of the Upper Limbs: fetal head extends (chinChinThe anatomical frontal portion of the mandible, also known as the mentum, that contains the line of fusion of the two separate halves of the mandible (symphysis menti). This line of fusion divides inferiorly to enclose a triangular area called the mental protuberance. On each side, inferior to the second premolar tooth, is the mental foramen for the passage of blood vessels and a nerve.Melasma lifts off the chest) as it moves under the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and appears through the vaginal opening
Head rotates back to transverse to align with the fetal spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy again.
Allows delivery of the shoulders beneath the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types
Expulsion:
Delivery of the rest of the fetal body, which has a smaller diameter than the fetal head and shoulders
Usually rapid
The cardinal movements of labor
Image by Lecturio.
Normal parameters
Evaluated with the descentof the fetal head (station).
Normal duration of the 2nd stage depends on:
Primiparous versus multiparous
Epidural versus no epidural
Infant should be making continuous downward progress throughout the 2nd stage.
Table: Normal parameters for the 2nd stage of labor
Primiparous
Multiparous
With an epidural
4 hours
3 hours
Without an epidural
3 hours
2 hours
Management
Continue to monitor mother and infant as in the 1st stage of labor, but more frequently for:
Vital signs
Urine output
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
Fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology (FHR) and uterine contractions:
Cardiotocography (FHR tracing), or
Intermittent auscultation with palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination of contractions
Discourage lying flat → woman should have a hip roll under 1 side to keep the baby off the inferior vena cavaInferior vena cavaThe venous trunk which receives blood from the lower extremities and from the pelvic and abdominal organs.Mediastinum and Great Vessels: Anatomy
Push/bear downwith each contraction
Table: Abnormalities and management in 2nd stage of labor
Abnormality
Definition
Management
Protracted 2nd stage
Pushing duration >3 hours in nulliparous or >2 hours in multiparous individuals (individualized; can extend if progress documented)
Observation: considered if fetal and maternal status are reassuring
Operative vaginal deliveryOperative Vaginal DeliveryOperative vaginal delivery is the use of obstetric forceps or a vacuum extractor to effect delivery of a fetus.Complications during Childbirth with midforceps if head is engaged and leading point ≤ +2 station
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery if < +2 station
Arrested 2nd stage
No descent for ≥ 2 hours
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
Shoulder dystociaShoulder DystociaObstetric complication during obstetric delivery in which exit of the fetus is delayed due to physical obstruction involving fetal shoulder(s).Complications during Childbirth
Fetal head delivers, but shoulder remains lodged under the pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types → obstetric emergency: fetus not getting oxygen during this time
Flex maternal legs
Suprapubic pressure: attempting to dislodge the anterior fetal shoulder
Delivery of the posterior armArmThe arm, or “upper arm” in common usage, is the region of the upper limb that extends from the shoulder to the elbow joint and connects inferiorly to the forearm through the cubital fossa. It is divided into 2 fascial compartments (anterior and posterior).Arm: Anatomy
Rotational maneuvers: attempt to rotate the fetal shoulder to allow delivery
The 3rd stage of labor starts immediately after delivery of the baby and ends with complete expulsion of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity.
Clinical presentation
Signs that the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is ready to deliver include:
Lengthening of the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Gush of blood
UterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy becomes hard and globular
Management
Active management:
Gentle downward traction on the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity with countertraction on the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy (to avoid uterine inversion)
IM or IV injection of oxytocin
Passive management:
Observation until spontaneous placental delivery occurs
Associated with higher rates of postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Normal parameters:
< 30 minutes
Typically takes 5–10 minutes
Prolonged 3rd stage of labor
Diagnosis: 3rd stage > 30 minutes
Etiology:
Abnormal placentation (e.g., placenta accretaPlacenta AccretaAbnormal placentation in which all or parts of the placenta are attached directly to the myometrium due to a complete or partial absence of decidua. It is associated with postpartum hemorrhage because of the failure of placental separation.Placental Abnormalities)
Separated but trapped placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity due to rapid contraction of the lower uterine segment
Management:
Manual uterine exploration
Uterine relaxants (if lower uterine segment is preventing expulsion)
Surgical exploration
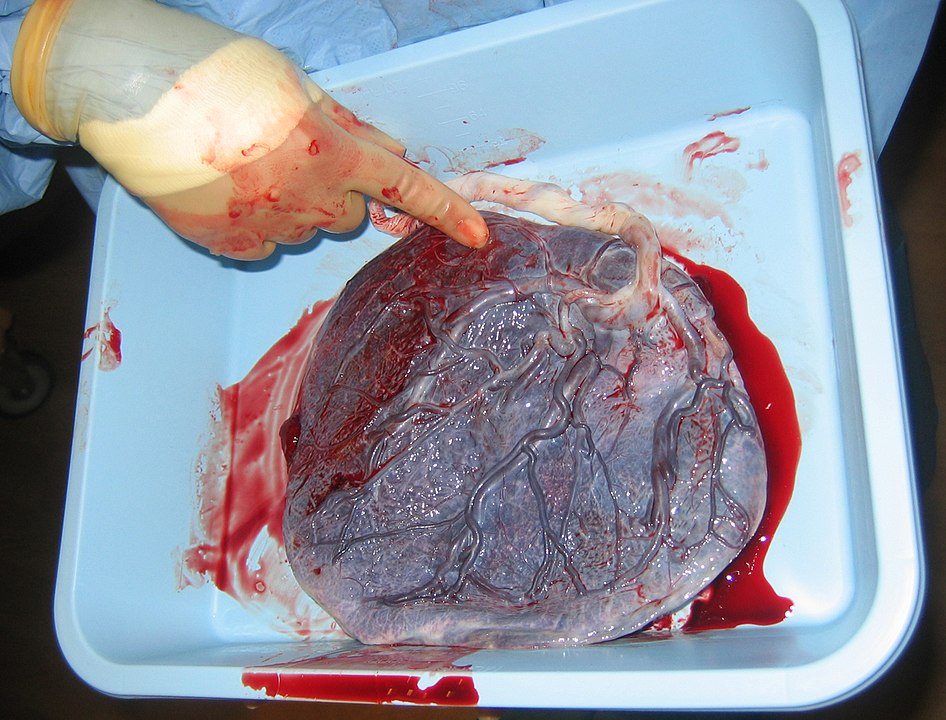
Human placenta shown a few minutes after birth:
The side shown faces the baby with the umbilical cord top right. The unseen side connects to the uterine wall.
False labor (also known asBraxton-Hicks contractionsBraxton-Hicks contractionsIrregular contractions that do not cause cervical change and become more noticeable as the pregnancy progresses Pregnancy: Diagnosis, Physiology, and Care):irregular uterine contractions or runs of regularRegularInsulin contractions without cervical changes. These contractions do not increase in intensity or duration, and they are common and normal in the 3rd trimester. Women should be reassured and counseled about hydration, as dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration was found to be associated with false labor.
Prelabor rupture of membrane: the rupture of membranes (chorionChorionThe outermost extraembryonic membrane surrounding the developing embryo. In reptiles and birds, it adheres to the shell and allows exchange of gases between the egg and its environment. In mammals, the chorion evolves into the fetal contribution of the placenta.Placenta, Umbilical Cord, and Amniotic Cavity and amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity) before the onset of labor. Women usually present with a “gush of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity” from the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy followed by a continuous dribble. InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease frequently develop after the membranes have been ruptured for a prolonged period (> 18 hours). SterileSterileBasic Proceduresspeculum examinationSpeculum ExaminationDiagnostic Procedures in Gynecology is done to visualize the presence of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity pooling within the posterior vaginal fornixFornixVagina, Vulva, and Pelvic Floor: Anatomy. Prelabor rupture of membrane may precipitate labor, but it is not considered to be labor in and of itself.