Cluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Autonomic symptoms typically manifest as ocular and nasal phenomena (e.g., ptosis, miosis, nasal congestion, rhinorrhea) on the same side as the headache. Men are more commonly affected by cluster headaches than women. The diagnosis is clinical and often easy to establish owing to the distinct features of the presenting headache. The 1st-line treatment involves administration of oxygen by nasal cannula and/or abortive therapy using a triptan. Preventive strategies (e.g., glucocorticoids, verapamil) are crucial, as cluster headache is a chronic condition associated with significant morbidity and a high rate of suicide.
Cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches are named based on their tendency to occur in clusters lasting from weeks to months, and interrupted by periods of remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches. The defining features include:
Cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess belongs to 2 distinct classification schemes: primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorders and trigeminal autonomic cephalgias (TACsTACsPrimary headache disorders that show symptoms caused by the activation of the autonomic nervous system of the trigeminal nerve. These autonomic features include redness and tearing of the eye, nasal congestion or discharge, facial sweating and other symptoms. Most subgroups show unilateral cranial pain.Cluster Headaches).
Primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorders:
MigraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine HeadacheheadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Tension headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Trigeminal autonomic cephalgias:
Common features:
Suspected similar pathophysiology
Clinical presentation: trigeminal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways + autonomic activation
Examples:
Cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess:
Most common of the TACsTACsPrimary headache disorders that show symptoms caused by the activation of the autonomic nervous system of the trigeminal nerve. These autonomic features include redness and tearing of the eye, nasal congestion or discharge, facial sweating and other symptoms. Most subgroups show unilateral cranial pain.Cluster Headaches
Has the longest duration of a single attack of the TACsTACsPrimary headache disorders that show symptoms caused by the activation of the autonomic nervous system of the trigeminal nerve. These autonomic features include redness and tearing of the eye, nasal congestion or discharge, facial sweating and other symptoms. Most subgroups show unilateral cranial pain.Cluster Headaches (15 minutes to 3 hours)
The lowest frequency in a given day of the TACsTACsPrimary headache disorders that show symptoms caused by the activation of the autonomic nervous system of the trigeminal nerve. These autonomic features include redness and tearing of the eye, nasal congestion or discharge, facial sweating and other symptoms. Most subgroups show unilateral cranial pain.Cluster Headaches (≤ 8 per day)
Paroxysmal hemicrania
Hemicrania continua
Short-lasting unilateral neuralgiform headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess with conjunctival injection and tearing (SUNCT)
Short-lasting unilateral neuralgiform headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess with cranial autonomic symptomsAutonomic SymptomsCluster Headaches (SUNA)
Epidemiology[1]
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency: < 1%
Strong association with cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Strong association with suicideSuicideSuicide is one of the leading causes of death worldwide. Patients with chronic medical conditions or psychiatric disorders are at increased risk of suicidal ideation, attempt, and/or completion. The patient assessment of suicide risk is very important as it may help to prevent a serious suicide attempt, which may result in death. Suicide attempts and successful suicideSuicideSuicide is one of the leading causes of death worldwide. Patients with chronic medical conditions or psychiatric disorders are at increased risk of suicidal ideation, attempt, and/or completion. The patient assessment of suicide risk is very important as it may help to prevent a serious suicide attempt, which may result in death. Suicide
The pathophysiology of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess is multifactorial and the precise mechanisms are poorly understood. The prevailing theories of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways mechanisms are outlined below.[3,4]
Trigeminal-autonomic reflex activation
Trigeminal nociceptive afferents have a direct connection to cranial autonomic fibers:
Between the trigeminal ganglionTrigeminal ganglionThe semilunar-shaped ganglion containing the cells of origin of most of the sensory fibers of the trigeminal nerve. It is situated within the dural cleft on the cerebral surface of the petrous portion of the temporal bone and gives off the ophthalmic, maxillary, and part of the mandibular nerves.Trigeminal Neuralgia and sphenopalatine ganglion
Between the trigeminocervical complex and higher brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification pain-processing centers
Some degree of autonomic outflow in response to stimulation of trigeminal nociceptive stimulation is normal, for example:
Stimulus: being slapped in the face
Autonomic response: ipsilateral lacrimation, local hyperemia/subcutaneous edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
In cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, the reflex is centralized, intrinsically triggered, and pathologically tethered to hypothalamic clocklike functions.
Trigeminal-autonomic reflex activation and hypothalamic activation mechanisms are interdependent.
Hypothalamic activation
Features of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess suggest the involvement of the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus, which has direct connections to the trigeminal system. Factors suggesting hypothalamic involvement include:
Circadian periodicity of attacks with predictable regularity of attack intervals
Associated hypothalamic hormonal irregularities:
Low testosteroneTestosteroneA potent androgenic steroid and major product secreted by the leydig cells of the testis. Its production is stimulated by luteinizing hormone from the pituitary gland. In turn, testosterone exerts feedback control of the pituitary LH and FSH secretion. Depending on the tissues, testosterone can be further converted to dihydrotestosterone or estradiol.Androgens and Antiandrogens levels
Abnormal pituitary-thyroid axis feedback loop
Functional imaging during attacks shows posterior hypothalamic activity.
Hypothalamic neuropeptides are known to play a role in trigeminal nociceptionNociceptionSensing of noxious mechanical, thermal or chemical stimuli by nociceptors. It is the sensory component of visceral and tissue pain (nociceptive pain).Pain: Types and Pathways.
Clinical Presentation
There is an overlap in the presenting symptoms and signs of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess and other primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess syndromes, as well as that of other TACsTACsPrimary headache disorders that show symptoms caused by the activation of the autonomic nervous system of the trigeminal nerve. These autonomic features include redness and tearing of the eye, nasal congestion or discharge, facial sweating and other symptoms. Most subgroups show unilateral cranial pain.Cluster Headaches. The distinguishing features are presented below.[1]
Autonomic manifestations accompanying painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the trigeminal (V1) distribution are typical of cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches.
Physical examination may be entirely normal unless the affected individual is experiencing an attack acutely.
History/physical exam[6–8,10,11]
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess features:
Always unilateral
Location:
Orbital
Supraorbital
Temporal
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways characteristics:
Affected individuals tend to become restless during attacks; common behaviors include:
Pacing
Rocking to and fro
Fidgeting
Frequency: up to 8 attacks per day
Duration: 15–180 minutes per attack
Timing: Attacks often occur overnight, causing sleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep disturbance.
Injected conjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy
Eyelid edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
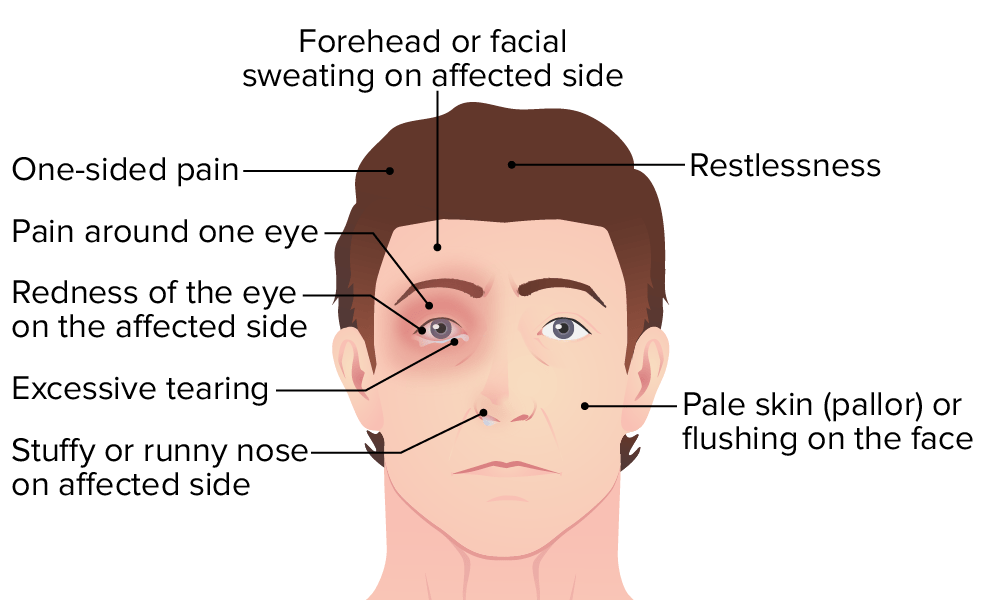
Illustration showing the symptoms of cluster headache
Image by Lecturio.
Subtypes of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess[8]
Episodic:
Most common subtype
RegularRegularInsulin daily headaches for days up to several weeks (6–12 on average)
Intermittent periods of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain AbscessremissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches (up to 12 months)
No associated periods of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain AbscessremissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches (or brief, < 3 months)
≥ 12 months without remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches for ≥ 3 months required for diagnosis
May arise as a primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorder or as a progression from episodic cluster headacheEpisodic Cluster HeadacheCluster Headaches
Secondary causes of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess meet the criteria for cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess but are caused by an associated underlying structural brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification lesion.
Diagnosis is clinical. A full diagnostic workup for headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess should be performed as well as ruling out red flag symptoms. Consider an MRI to rule out secondary causes of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess.[1] Laboratory evaluation is indicated only if an underlying condition is suspected and should be tailored to the specific suspected cause.[1]
Temporal, orbital, and/or supraorbital location of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Duration ≥ 15, but ≤ 180 minutes if left untreated
Plus ≥ 1 of the following symptoms ipsilateral to the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways:
Injected conjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy
Eyelid edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Restlessness or agitationAgitationA feeling of restlessness associated with increased motor activity. This may occur as a manifestation of nervous system drug toxicity or other conditions.St. Louis Encephalitis Virus
Frequency: every 2 days, up to 8 times per day
Not better accounted for by another headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess diagnosis
Meets the criteria stated above plus the following criteria:
Headaches occur in clusters.
≥ 2 clusters lasting ≥ 7 days, but ≤ 1 year if left untreated
Clusters separated by headache-free periods of remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches lasting ≥ 3 months
Meets the criteria stated above plus the following criteria:
Absence of remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches, OR
Remissions lasting ≤ 3 months during ≥ 1-year period
Imaging[12]
NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant is indicated at the initial evaluation of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess:
Rule out the secondary causes of headaches.
Evaluate for pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types abnormalities, which are found in 4% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches.
Repeat imaging is indicated only in the following cases:
Red-flag headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess symptoms:[12]
Subacute head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma
Related to exertion or sexual activity
Positional
Known or suspected cancer
Immunosuppression
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Age ≥ 50 years
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess characteristics have changed or no longer classify as any of the primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorders.
Imaging modalities:
MRI of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification with and without contrast is the test of choice[12].
CT is faster for triage of suspected acute intracranial hemorrhageIntracranial hemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most sahs originate from a saccular aneurysm in the circle of willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use.Subarachnoid Hemorrhage.
Management
While abortive therapy may successfully terminate an isolated attack, preventive therapy is the mainstay of cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess management. Preventive strategies should be started at the onset of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess episodes. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should typically be referred to specialists.[5–7,9,11]
Home oxygen use requires a strict fire-risk assessment.
Immediate onset of action
Well tolerated and effective (approximately 60% have a significant response)
TriptansTriptansTriptans and ergot alkaloids are agents used mainly for the management of acute migraines. The therapeutic effect is induced by binding to serotonin receptors, which causes reduced vasoactive neuropeptide release, pain conduction, and intracranial vasoconstriction.Triptans and Ergot Alkaloids:[5–7]
Routes of administration:
Subcutaneous:
May be administered at home (self-injection) or in the office
Rapid onset of action
Intranasal spray:
For individuals who cannot tolerate or cannot self-administer injections
Slower onset of action, but more convenient
To be administered contralateral to the side of the headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess (to prevent poor absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption due to nasal congestion)
Oral
Timing: should be administered as soon as the headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess begins
1st-line (best data regarding effectiveness):[5,7]
SumatriptanSumatriptanA serotonin agonist that acts selectively at 5ht1 receptors. It is used in the treatment of migraine disorders.Triptans and Ergot Alkaloids 6 mg subcutaneously
SumatriptanSumatriptanA serotonin agonist that acts selectively at 5ht1 receptors. It is used in the treatment of migraine disorders.Triptans and Ergot Alkaloids 20 mg intranasally
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to triptansTriptansTriptans and ergot alkaloids are agents used mainly for the management of acute migraines. The therapeutic effect is induced by binding to serotonin receptors, which causes reduced vasoactive neuropeptide release, pain conduction, and intracranial vasoconstriction.Triptans and Ergot Alkaloids:[6]
Cardiovascular disease: stroke, peripheral vascular disease, and severe hypertensionSevere hypertensionA confirmed blood pressure ≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic.Uncontrolled Hypertension
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Adverse effects:[6]
Medication-overuse headaches
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
ParesthesiasParesthesiasSubjective cutaneous sensations (e.g., cold, warmth, tingling, pressure, etc.) that are experienced spontaneously in the absence of stimulation.Posterior Cord Syndrome
Other options:[5,6]
Additional options with less evidence, but noted to “probably” be effective, include:
10% LidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics 1 mL intranasally
OctreotideOctreotideA potent, long-acting synthetic somatostatin octapeptide analog that inhibits secretion of growth hormone and is used to treat hormone-secreting tumors; diabetes mellitus; hypotension, orthostatic; hyperinsulinism; hypergastrinemia; and small bowel fistula.Antidiarrheal Drugs 100 µg subcutaneously
Prevention/treatment of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess and toxicityToxicityDosage Calculation caused by abortive medication overuse
Regimen:
Begin with the onset of a cluster attack → goal is to reduce the frequency of individual episodes during a cluster attack
Continue for up to 4 weeks after a cluster attack has subsided (duration is guided by patient experience)
Dosing range: 240‒960 mg daily in divided doses (2 or 3 doses daily depending on whether tablets are sustained- or regular-release)
Begin with 240 mg total daily dose (e.g., 80 mg 3 times a day) and increase by 80 mg every 2 weeks according to response
Once the cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess bout is over, slowly stop the medication.
At the onset of the next cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess bout, immediately start at the known effective dose, provided that the baseline ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) is normal.[7]
Slow onset of action
Side effects:
1 in 5 patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship develop cardiac arrhythmia, bradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias or PR intervalPR intervalElectrocardiogram (ECG) lengthening
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) recommended prior to commencement, 10 days following dose increment and every 6 months once a stable dose is achieved.
Other less serious side effects include constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation and pedal edemaPedal EdemaRocky Mountain Spotted Fever.
Oral agents are typically used as an adjunct with verapamilVerapamilA calcium channel blocker that is a class IV anti-arrhythmia agent.Pulmonary Hypertension Drugs as a “transition therapy” while waiting for preventive options to take effect
May be used alone for infrequent episodic bouts
Oral options:[5,6]
PrednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants 60–80 mg once daily for 2–4 days (then tapered)
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 20 mg every other day
To avoid cumulative effects of systemic steroid use
Unilateral greater occipitalOccipitalPart of the back and base of the cranium that encloses the foramen magnum.Skull: Anatomy nerve block: e.g., methylprednisoloneMethylprednisoloneA prednisolone derivative with similar anti-inflammatory action.Immunosuppressants 80 mg with 2 mL of 2% lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics. Lasts 4 weeks and can be repeated in 3 months.
Suboccipital injections: agents and regimens vary (e.g., cortivazol 3.75 mg ipsilateral to the headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, performed 3 times 2–3 days apart.)
LithiumLithiumAn element in the alkali metals family. It has the atomic symbol li, atomic number 3, and atomic weight [6. 938; 6. 997]. Salts of lithium are used in treating bipolar disorder.Ebstein’s Anomaly:
TopiramateTopiramateA sulfamate-substituted fructose analog that was originally identified as a hypoglycemic agent. It is used for the treatment of epilepsy and migraine disorders, and may also promote weight loss.Second-Generation Anticonvulsant Drugs:
Extensive side effects: cognitive and mood effects, teratogenicity, nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis, impact on contraceptive efficacy
Dose: Start at 25 mg/day and titrate upward in 25-mg increments up to a recommended dose of 100–200 mg/day in 2 divided doses.
Galcanezumab:
Monoclonal antibody against calcitoninCalcitoninA peptide hormone that lowers calcium concentration in the blood. In humans, it is released by thyroid cells and acts to decrease the formation and absorptive activity of osteoclasts. Its role in regulating plasma calcium is much greater in children and in certain diseases than in normal adults.Other Antiresorptive Drugs gene-related peptide (CGRPCGRPA 37-amino acid peptide derived from the calcitonin gene. It occurs as a result of alternative processing of mRNA from the calcitonin gene. The neuropeptide is widely distributed in the brain, gut, perivascular nerves, and other tissue. The peptide produces multiple biological effects and has both circulatory and neurotransmitter modes of action. In particular, it is a potent endogenous vasodilator.Gastrointestinal Neural and Hormonal Signaling) ligand (CGRPCGRPA 37-amino acid peptide derived from the calcitonin gene. It occurs as a result of alternative processing of mRNA from the calcitonin gene. The neuropeptide is widely distributed in the brain, gut, perivascular nerves, and other tissue. The peptide produces multiple biological effects and has both circulatory and neurotransmitter modes of action. In particular, it is a potent endogenous vasodilator.Gastrointestinal Neural and Hormonal Signaling elevated in cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches)
Modestly effective
Reserved for individuals refractory to the above preventive therapies
FDA approved in 2019 but not included in American HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess Society Guidelines
Neuromodulation:[5,7]
Indicated in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship in whom oral preventive therapies were ineffective or contraindicated
Most commonly used techniques:
Noninvasive vagus nerveVagus nerveThe 10th cranial nerve. The vagus is a mixed nerve which contains somatic afferents (from skin in back of the ear and the external auditory meatus), visceral afferents (from the pharynx, larynx, thorax, and abdomen), parasympathetic efferents (to the thorax and abdomen), and efferents to striated muscle (of the larynx and pharynx).Pharynx: Anatomy stimulation[7]
Instructions: three 2-minute stimulations using a hand-held device, 2 times a day on the ipsilateral side over the cervical branch of the vagus nerveVagus nerveThe 10th cranial nerve. The vagus is a mixed nerve which contains somatic afferents (from skin in back of the ear and the external auditory meatus), visceral afferents (from the pharynx, larynx, thorax, and abdomen), parasympathetic efferents (to the thorax and abdomen), and efferents to striated muscle (of the larynx and pharynx).Pharynx: Anatomy
Effective for terminating acute attacks and can be used as a preventive treatment
Sphenopalatine ganglion stimulation:[5,7]
Microstimulator surgically implanted into pterygopalatine fossaPterygopalatine fossaA small space in the skull between the maxilla and the sphenoid bone, medial to the pterygomaxillary fissure, and connecting to the nasal cavity via the sphenopalatine foramen.Skull: Anatomy
Patient activates the stimulator via a hand-held device placed near the ipsilateral cheek
Has a preventive effect in ⅓ of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship; if already in place as a preventive treatment, may be helpful in aborting acute attack
Risks include sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology disturbance and postoperative complicationsPostoperative ComplicationsPathologic processes that affect patients after a surgical procedure. They may or may not be related to the disease for which the surgery was done, and they may or may not be direct results of the surgery.Postoperative Care.[7]
Not readily available
Behavioral approaches and lifestyle modifications:
Lifestyle modifications:
Avoidance of triggers (alcohol, strong smells)
RegularRegularInsulinsleepSleepA readily reversible suspension of sensorimotor interaction with the environment, usually associated with recumbency and immobility.Physiology of Sleep
Exercise
Stopping smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Paroxysmal hemicrania: a rare form of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess and TAC with substantial similarity to cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess in terms of intensity, location, and presence of autonomic symptomsAutonomic SymptomsCluster Headaches. Attacks occur 5–40 times per day and last 2–30 minutes. The diagnosis is clinical. Paroxysmal hemicrania is responsive to the NSAIDNSAIDNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs)indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs), which is useful both in diagnosis and treatment. Other NSAIDsNSAIDSPrimary vs Secondary Headaches, calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes channel blockers, and corticosteroidsCorticosteroidsChorioretinitis are also effective.
Hemicrania continua: a TAC with substantial similarity to cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess in terms of location and presence of autonomic symptomsAutonomic SymptomsCluster Headaches. Hemicrania continua is distinguished by a milder intensity but a longer, continuous headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess duration of several hours. There may be periodic exacerbations of severe intensity, but the underlying moderate headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess does not abate without treatment. The diagnosis is clinical. Hemicrania continua is responsive to the NSAIDNSAIDNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs)indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs), which is useful both in diagnosis and treatment.
SUNCT and SUNA: rare forms of TAC similar to cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess in painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways location but may also be retroorbital and rarely in other trigeminal and nontrigeminal areas. Attacks of prolonged stabbing painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways (1–5 minutes) may occur in isolation or in groups with a total duration of up to 10 minutes. The attacks are often associated with triggers, but may also be spontaneous. Oxygen and indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs) are ineffective in SUNCT and SUNA, but IV lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics may be effective.
Primary stabbing headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess: while not classified as a TAC,primary stabbing headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess does have some overlapping clinical features. PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways attacks are brief (< 1 second), sharp and stabbing, and unilateral, but are not accompanied by autonomic symptomsAutonomic SymptomsCluster Headaches. Attacks may be isolated or can occur at irregular intervals with several hours or even days between episodes. Diagnosis is clinical. The attacks usually subside with the administration of indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs).
Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia: a rare neuralgiform headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess entity that manifests in the temporal, orbital, or supraorbital area(s) with extreme sudden burning or shock-like face painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia may mimic a TAC as it may manifest in any of the trigeminal areas. Attacks generally last < 5 seconds, are unilateral, and not accompanied by autonomic symptomsAutonomic SymptomsCluster Headaches. Management includes drugs such as anticonvulsants (e.g., carbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs) and tricyclic antidepressantsTricyclic antidepressantsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants, and surgery. Typical analgesics and opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics have not been proven effective to treat trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia.
MigraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine HeadacheheadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess: a type of primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess that is severe and generally described as unilateral and throbbing. MigraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine Headache headaches are associated with neurological symptoms such as nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and/or light and sound sensitivity. Attacks last between 4 and 72 hours and are more common in women. Individuals may experience an auraAuraReversible neurological phenomena that often precede or coincide with headache onset.Migraine Headache, such as a visual phenomenon, or experience tinglingTinglingPosterior Cord Syndrome on the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions or difficulty speaking before headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess onset. Diagnosis is clinical and based on the typical symptoms. Migraines do not generally present with autonomic symptomsAutonomic SymptomsCluster Headaches, but there is a distinct subset that does. Management includes avoiding loud noises and light, and treatment with simple analgesicsSimple AnalgesicsPrimary vs Secondary Headaches and/or triptansTriptansTriptans and ergot alkaloids are agents used mainly for the management of acute migraines. The therapeutic effect is induced by binding to serotonin receptors, which causes reduced vasoactive neuropeptide release, pain conduction, and intracranial vasoconstriction.Triptans and Ergot Alkaloids.
Medication-overuse headacheMedication-Overuse HeadachePrimary vs Secondary Headaches: also called rebound headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess. A type of secondary headacheSecondary headacheConditions with headache symptom that can be attributed to a variety of causes including brain vascular disorders; wounds and injuries; infection; drug use or its withdrawal.Primary vs Secondary Headaches in individuals who have frequent or daily headaches despite, or because of, the regularRegularInsulin use of medications to relieve headaches. Medication-overuse headacheMedication-Overuse HeadachePrimary vs Secondary Headaches is usually preceded by an episodic primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorder that has been treated with excessive amounts of abortive medications, especially drug combinations containing caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants and codeineCodeineAn opioid analgesic related to morphine but with less potent analgesic properties and mild sedative effects. It also acts centrally to suppress cough.Opioid Analgesics. Treatment consists of establishing an effective preventive regimen so that the offending abortive agent(s) can be weaned or discontinued.
Sinus headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess: a headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess that occurs in the setting of acute or chronic sinusitisSinusitisSinusitis refers to inflammation of the mucosal lining of the paranasal sinuses. The condition usually occurs concurrently with inflammation of the nasal mucosa (rhinitis), a condition known as rhinosinusitis. Acute sinusitis is due to an upper respiratory infection caused by a viral, bacterial, or fungal agent. Sinusitis. The painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is typically described as constant and deep around the cheeksCheeksThe part of the face that is below the eye and to the side of the nose and mouth.Melasma, foreheadForeheadThe part of the face above the eyes.Melasma, or bridge of the noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal). Sinus headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess is associated with symptoms including a runny noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal), swellingSwellingInflammation or tearing of the eyes, and feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever. Management includes decongestants, antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines in the case of allergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction, and antibiotics in the presence of a bacterial infection.
Billing and Coding
Diagnosis Codes:
Cluster headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess is a severe primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorder coded based on its pattern, either episodic (with periods of remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches) or chronic (without remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches).
These codes represent acute and preventive therapies. High-flow oxygen and injectable sumatriptanSumatriptanA serotonin agonist that acts selectively at 5ht1 receptors. It is used in the treatment of migraine disorders.Triptans and Ergot Alkaloids are first-line for aborting an acute attack. VerapamilVerapamilA calcium channel blocker that is a class IV anti-arrhythmia agent.Pulmonary Hypertension Drugs is the primary medication for prevention.
SumatriptanSumatriptanA serotonin agonist that acts selectively at 5ht1 receptors. It is used in the treatment of migraine disorders.Triptans and Ergot Alkaloids (ingredient)
May, A. (2022). Pathophysiology of the trigeminal autonomic cephalgias. UpToDate. Retrieved October 5, 2022, from https://www.uptodate.com/contents/pathophysiology-of-the-trigeminal-autonomic-cephalalgias
Robbins, M. S., Starling, A. J., Pringsheim, T. M., Becker, W. J., Schwedt, T. J. (2016). Treatment of cluster headache: the American Headache Society evidence-based guidelines: headache. Headache, 56(7), 1093–1106. https://doi.org/10.https://doi.org/10.1111/head.128661111/head.12866
May, A., Leone, M., Áfra, J., Linde, M., Sándor, P. S., Evers, S., Goadsby, P. J. (2006). EFNS guidelines on the treatment of cluster headache and other trigeminal-autonomic cephalalgias. European Journal of Neurology, 13(10), 1066–1077. https://doi.org/10.1111/j.1468-1331.2006.01566.x
Headache Classification Committee of the International Headache Society. (2018). The international classification of headache disorders, 3rd edition. Cephalalgia, 38(1), 1‒211. doi: 10.1177/0333102417738202
Steiner, T. J., Jensen, R., Katsarava, Z., Linde, M., MacGregor, E. A., Osipova, V., Paemeleire, K., Olesen, J., Peters, M., Martelletti, P. (2019). Aids to management of headache disorders in primary care (2nd edition). Journal of Headache and Pain, 20(1), 57. https://doi.org/10.1186/s10194-018-0899-2
Expert Panel on Neurologic Imaging, Whitehead, M. T., Cardenas, A. M., Corey, A. S., Policeni, B., Burns, J., Chakraborty, S., Crowley, R. W., Jabbour, P., Ledbetter, L. N., Lee, R. K., Pannell, J. S., Pollock, J. M., Powers, W. J., Setzen, G., Shih, R. Y., Subramaniam, R. M., Utukuri, P. S., Bykowski, J. (2019). ACR Appropriateness Criteria® Headache. Journal of the American College of Radiology, 16(11S), S364–S377. https://doi.org/10.1016/j.jacr.2019.05.030
Create your free account or log in to continue reading!