Cervical cancer is the 3rd most common gynecologic cancer. More than 90% of cervical cancer cases are associated with high-risk human papillomavirus (hrHPV), which is transmitted by sexual contact. Cervical cancer can be prevented by early detection and treatment of precancerous lesions caused by hrHPV. The methods of detection are cervical cytology and HPV testing. Guidelines vary on when to start screening, with various US societies recommending that screening start between 21 and 25 years of age, while the World Health Organization (WHO) suggests waiting until age 30, especially in resource-limited settings.Guidelines also vary on the preferred method of testing, though HPV testing (with or without cytology) is universally preferred starting at age 30. Since the screening program was initiated, there has been a 75% decline in the incidence of and mortality from cervical cancer.
Cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer[6,12]
Cancer of the uterine cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy
Major histologic types:
Squamous cell carcinomaSquamous cell carcinomaCutaneous squamous cell carcinoma (cSCC) is caused by malignant proliferation of atypical keratinocytes. This condition is the 2nd most common skin malignancy and usually affects sun-exposed areas of fair-skinned patients. The cancer presents as a firm, erythematous, keratotic plaque or papule. Squamous Cell Carcinoma (SCC): approximately 75% of cervical cancers
Adenocarcinoma: up to 20%
Adenosquamous carcinoma: 3 to 5%
Associated with human papillomavirusHuman papillomavirusHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) (HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV)):
Detected in 99.7% of cervical cancers
Subtypes HPV 16HPV 16A type of alphapapillomavirus usually associated with genital warts; and laryngeal neoplasms.Papillomavirus (HPV) and 18 found in > 70% of cervical cancers[6]
Epidemiology[1,6,12]
More than 80% of new cases worldwide are from less developed countries.
Worldwide:
2020 estimates:
> 660,000 diagnosed with cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer
> 350,000 died due to cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer
Most common cause of cancer in 23 developing countries, primarily in sub-Saharan Africa, South America, and Southeast AsiaASIASpinal Cord Injuries
In the United States:
14,000 new cases of invasive cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer are diagnosed annually.
Mean age at diagnosis: 50 years
3rd most common gynecologic cancer diagnosed
18th most common cause of cancer death overall
Risk factors[12]
HPV-related:
Early onset of sexual activity
Multiple sexual partners
Multiparity ≥ 3 full-term births
Early age (< 20 years of age) at 1st birth
History of vulvar or vaginal squamous intraepithelial neoplasia or cancer
Immunosuppression
Human immunodeficiencyImmunodeficiencyChédiak-Higashi SyndromevirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology (HIVHIVAnti-HIV Drugs) infection
Co-infection with other sexually transmitted diseases (e.g., Chlamydia trachomatisChlamydia trachomatisType species of Chlamydia causing a variety of ocular and urogenital diseases.Chlamydia, herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology)
Non-HPV related:
Low socioeconomic status
non-Hispanic Black race due to health disparities and access to care
Use of oral contraceptives
Cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases (associated with squamous cell carcinomaSquamous cell carcinomaCutaneous squamous cell carcinoma (cSCC) is caused by malignant proliferation of atypical keratinocytes. This condition is the 2nd most common skin malignancy and usually affects sun-exposed areas of fair-skinned patients. The cancer presents as a firm, erythematous, keratotic plaque or papule. Squamous Cell Carcinoma (SCC))
Women 21‒65 years of age (or 25–65 where primary HPV testingHPV testingCervical Cancer Screening is used) are at risk for cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer due to potential exposure to high-risk human papillomavirusHuman papillomavirusHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) (hrHPV) through sexual intercourse.
A 75% decline in the incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency and mortalityMortalityAll deaths reported in a given population.Measures of Health Status of cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer occurred in the past 50 years due to screeningScreeningPreoperative Care.
Most cases of cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer are found in women who have not been adequately screened.
Cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer usually does not cause symptoms.
Cancerous and precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesions are rare before the age of 21.
The progression from hrHPV infection → precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesions (cervical intraepithelial neoplasia (CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer)) → invasive cancer takes many years
Many precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesions and HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV)infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease will regress.
May lead to more harm from psychological distress and unnecessary procedures
Most are nucleic acid amplificationNucleic acid amplificationLaboratory techniques that involve the in-vitro synthesis of many copies of DNA or RNA from one original template.Septic Arthritis tests (NAATs)[1,6]
Tests vary as to which subtypes they can detect, though all detect the 14 most common oncogenic types, including 16 and 18.
GenotypingGenotypingMethods used to determine individuals’ specific alleles or snps (single nucleotide polymorphisms).Polymerase Chain Reaction (PCR) refers to testing for an individual type, typically 16 and 18, +/– 45.
Patient collects own sample by inserting soft swab into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy (in a healthcare setting)
For individuals who cannot or do not undergo clinician-collected cervical sampling; provider needs to order the test.
Cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening:[1,13]
Ectocervical and endocervical cells are collected to evaluate the transformation zoneTransformation zoneDiagnostic Procedures in Gynecology (area at risk for cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer).
Conventional Papanicolaou (Pap) smear: Ectocervical spatula is smeared and the brush rolled onto a slide, with fixative applied immediately
Liquid-based thin layer cytology: Collection device is placed and swirled in the liquid fixative solution, which is then processed by the laboratory.
Liquid-based cytology has largely replaced conventional Pap smears in U.S. clinical practice.
A co-test (HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) test combined with a Pap test): co-testing (every 5 years) remains an acceptable strategy for ages 30–65, though many guidelines now prefer primary HPV testingHPV testingCervical Cancer Screening alone (due to higher sensitivity and similar long-term protection).
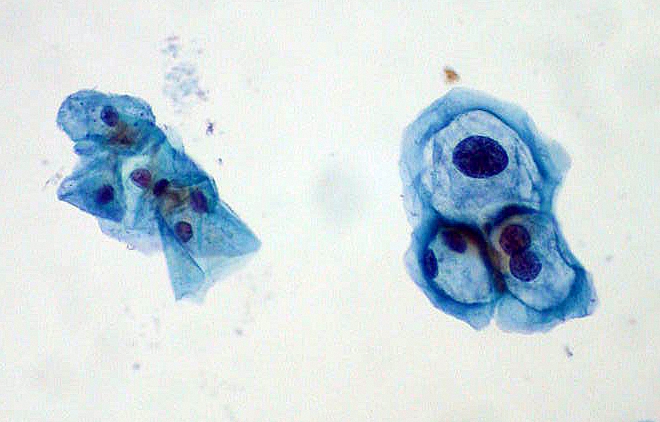
Slide image from a Pap smear for cervical cancer screening: Normal squamous cells are on the left; HPV-infected cells with mild dysplasia are on the right.
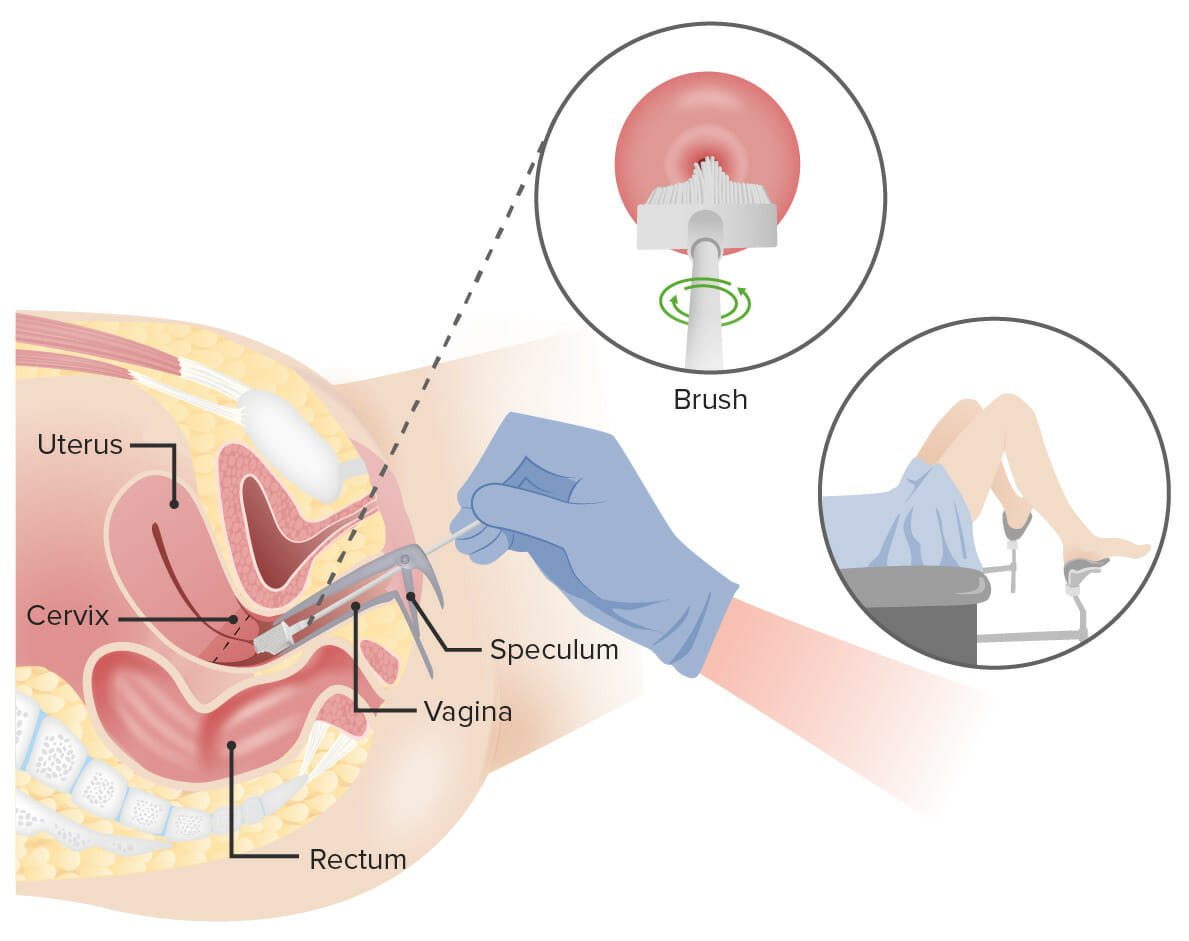
Pap test: A speculum is inserted into the vagina to widen it. Then, a broom (shown here) or an endocervical brush and spatula is/are inserted into the vagina to collect cells from the cervix. The cells are checked under a microscope for signs of disease.
Image by Lecturio.
Cervical Cancer Screening for Average-Risk Individuals
The following recommendations are for average-risk individuals.[1-7] This group includes individuals who are fully vaccinated against HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV).
United States Preventive Services Task Force (USPSTF)[1]recommendations (which are endorsed by the American Society for ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening and Cervical Pathology (ASCCP),[4,5] the American College of Obstetricians and Gynecologists (ACOG),[7] and the Society of Gynecologic Oncology[7]):
Cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening alone every 3 years
Differences from the American Cancer Society (ACS) recommendations:[7]
Access to primary screeningScreeningPreoperative Care with hrHPV testing alone is still frequently unavailable in the US.
Raising the initial age of screeningScreeningPreoperative Care to 25 (as ACS did) is under consideration.
Concern exists that raising the initial age of screeningScreeningPreoperative Care and/or changing the preferred method of screeningScreeningPreoperative Care may exacerbate underscreening in those 25‒29 years old and health equity concerns.
Co-testing with HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) and cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening every 5 years
Cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening alone every 3 years
Low incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer in those < 24 years of age
About 70% of adolescents have received at least 1 dose of the HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV)vaccineVaccineSuspensions of killed or attenuated microorganisms (bacteria, viruses, fungi, protozoa), antigenic proteins, synthetic constructs, or other bio-molecular derivatives, administered for the prevention, amelioration, or treatment of infectious and other diseases.Vaccination.
3 consecutive negative cytology results, with the last result within the past 3 years
2 consecutive negative co-test results within the past 10 years, with the most recent test within the past 5 years
2 consecutive negative primary HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) test results within the past 10 years, with the most recent test within the past 5 years
Cervical Cancer Screening for Special Populations
High-risk individuals[1,3,6,7]
Certain conditions have a high risk for cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer, so screeningScreeningPreoperative Care must be individualized and more frequent:
ImmunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.Gastroenteritis (e.g., transplant or immunosuppressant therapy):
ASCCP: screeningScreeningPreoperative Care within one year of the onset of sexual activity, regardless of age, even if before 21.[18]
Many immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.Gastroenteritis groups continue screeningScreeningPreoperative Care beyond 65 based on health status/life expectancyLife expectancyBased on known statistical data, the number of years which any person of a given age may reasonably expected to live.Population Pyramids.
In utero exposure to diethylstilbestrolDiethylstilbestrolA synthetic nonsteroidal estrogen used in the treatment of menopausal and postmenopausal disorders. It was also used formerly as a growth promoter in animals. According to the fourth annual report on carcinogens, diethylstilbestrol has been listed as a known carcinogen.Noncontraceptive Estrogen and Progestins (last used in the 1970s, so most relevant in women born prior to 1980)
Previous treatment of a high-grade precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesion or cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer within the past 25 years
With history of subtotal hysterectomy (cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy intact; typically called a supracervical hysterectomy)
With history of cervical intraepithelial neoplasia (CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer), even after hysterectomy
History of a total hysterectomy (which includes removal of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy) for a benignBenignFibroadenoma disease
No history of a high-grade precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesion (CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer grade 2 or 3) or cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with limited access to care
A life expectancyLife expectancyBased on known statistical data, the number of years which any person of a given age may reasonably expected to live.Population Pyramids of ≥ 10 years
An informed decision-making discussion with the patient
Continued screeningScreeningPreoperative Care is recommended for at least 25 years after a precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus lesion regresses or is treated, even if screeningScreeningPreoperative Care goes past the age of 65, including situation in which:
Results (Bethesda systemBethesda systemA standardized reporting of results of PAP test, which includes the specimen adequacy, general categorization of findings, and resultsCervical Cancer Screening)[14]
The Bethesda systemBethesda systemA standardized reporting of results of PAP test, which includes the specimen adequacy, general categorization of findings, and resultsCervical Cancer Screening is a standardized reporting of results, which includes the specimen adequacy, general categorizationCategorizationTypes of Variables of findings, and results.
Specimen adequacy (critical for qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement assurance):[14]
Requires at least 5,000 well-visualized squamous cells on a liquid preparation or 8,000‒12,000 well-visualized squamous cells on a traditional Pap smearPap smearCytological preparation of cells collected from a mucosal surface and stained with Papanicolaou stain.Cervical Cancer Screening
The area of squamous metaplasiaMetaplasiaA condition in which there is a change of one adult cell type to another similar adult cell type.Cellular Adaptation between the squamocolumnar junctionSquamocolumnar junctionEsophagus: Anatomy separating squamous ectocervical cells from glandular endocervical cells
Requires at least 10 well-preserved endocervical or squamous metaplastic cells
Presence of a transformation zoneTransformation zoneDiagnostic Procedures in Gynecology component is defined as at least 10 well-preserved endocervical or squamous metaplastic cells; however, its absence does not make the specimen unsatisfactory.
Absent or minimal obscuring or interfering factors (a specimen is unsatisfactory for evaluation when > 75% of the cells are obscured); factors include:
Blood
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Some lubricants
Types of squamous cell epithelial cell abnormalities:
Negative for intraepithelial lesion or malignancyMalignancyHemothorax (NILM): no cellular evidence of neoplasia
Atypical squamous cells (ASC):
Some cells seen are not normal but do not meet the requirements to be precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus.
May be precancerousPrecancerousPathological conditions that tend eventually to become malignant.Barrett Esophagus or associated with infection, irritation, or intercourse
Categories:
ASC of undetermined significance (ASC-US): abnormal cells, but no squamous intraepithelial lesions (SIL)
ASC cannot exclude high-grade SILs (HSIL): equivocal findings (cytologic changes suggestive of HSIL but lacking definitive qualitative or quantitative criteria)
Squamous intraepithelial lesion (SIL):
Premalignant findings for invasive squamous cell carcinomaSquamous cell carcinomaCutaneous squamous cell carcinoma (cSCC) is caused by malignant proliferation of atypical keratinocytes. This condition is the 2nd most common skin malignancy and usually affects sun-exposed areas of fair-skinned patients. The cancer presents as a firm, erythematous, keratotic plaque or papule. Squamous Cell Carcinoma (SCC)
Low-grade squamous intraepithelial lesion (LSIL):
Low-grade dysplasia (manifestation of an active, often transient, HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) infection) corresponding to CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 1 (cervical intraepithelial neoplasia type 1Type 1Spinal Muscular Atrophy) histology
Moderate or high-grade dysplasia (corresponding to CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 2, CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3)
Increased risk of progression to invasive carcinoma (compared with LSIL changes)
Squamous cell carcinomaSquamous cell carcinomaCutaneous squamous cell carcinoma (cSCC) is caused by malignant proliferation of atypical keratinocytes. This condition is the 2nd most common skin malignancy and usually affects sun-exposed areas of fair-skinned patients. The cancer presents as a firm, erythematous, keratotic plaque or papule. Squamous Cell Carcinoma (SCC): cancer
Glandular cell abnormalities (categorized as endocervical, endometrial, or not otherwise specified):
Atypical endocervical, endometrial, or glandular cells (AGC): endometrial or cervical cell changes abnormal, requiring closer evaluation
AGC, favor neoplastic: show features that suggest, but are not sufficient for, a diagnosis of adenocarcinoma
Endocervical adenocarcinoma in situ (AISAISScoliosis): premalignant lesion of invasive adenocarcinoma
Adenocarcinoma: cancer
Other possible findings reported on cervical cytologyCervical cytologyA procedure in which ectocervical and endocervical cells are collected to evaluate the transformation zone (area at risk for cervical cancer).Cervical Cancer Screening reports:
Organisms:
TrichomonasTrichomonasA genus of parasitic flagellate eukaryotes distinguished by the presence of four anterior flagella, an undulating membrane, and a trailing flagellum.Nitroimidazoles vaginalis
Fungal elements (consistent with CandidaCandidaCandida is a genus of dimorphic, opportunistic fungi. Candida albicans is part of the normal human flora and is the most common cause of candidiasis. The clinical presentation varies and can include localized mucocutaneous infections (e.g., oropharyngeal, esophageal, intertriginous, and vulvovaginal candidiasis) and invasive disease (e.g., candidemia, intraabdominal abscess, pericarditis, and meningitis). Candida/Candidiasis)
Cellular changes consistent with herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology or cytomegalovirusCytomegalovirusCMV is a ubiquitous double-stranded DNA virus belonging to the Herpesviridae family. CMV infections can be transmitted in bodily fluids, such as blood, saliva, urine, semen, and breast milk. The initial infection is usually asymptomatic in the immunocompetent host, or it can present with symptoms of mononucleosis. Cytomegalovirus
Bacterial vaginosisBacterial vaginosisPolymicrobial, nonspecific vaginitis associated with positive cultures of gardnerella vaginalis and other anaerobic organisms and a decrease in lactobacilli. It remains unclear whether the initial pathogenic event is caused by the growth of anaerobes or a primary decrease in lactobacilli.Vulvovaginitis
BacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology consistent with ActinomycesActinomycesActinomyces is an anaerobic, gram-positive, branching, filamentous rod. Actinomyces israelii is the most common species involved in human disease. The organism is commonly found as part of the normal flora in the oral cavity, gastrointestinal tract, and reproductive tract. Actinomyces/Actinomycosis
Other nonneoplastic findings may be included:
Reactive cellular changes
Glandular cells status post-hysterectomy
AtrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
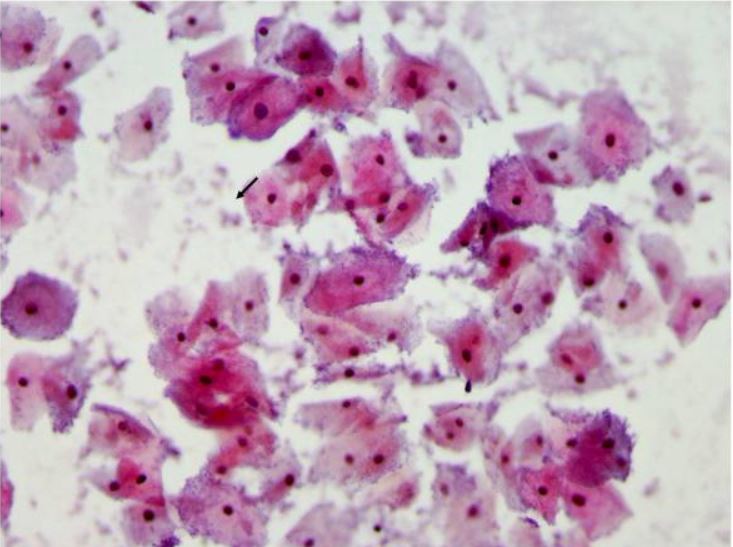
Pap smear showing bacterial vaginosis with many clue cells Clue cells are vaginal epithelial cells studded with adherent coccobacilli that are best appreciated at the edge of the cells. The bacteria are stained blue-purple by the Pap stain (arrows).
Image: “Cervical cytological changes in HIV-infected patients” by Mwakigonja AR, Torres LM, Mwakyoma HA, Kaaya EE. License: CC BY 2.0, edited by Lecturio
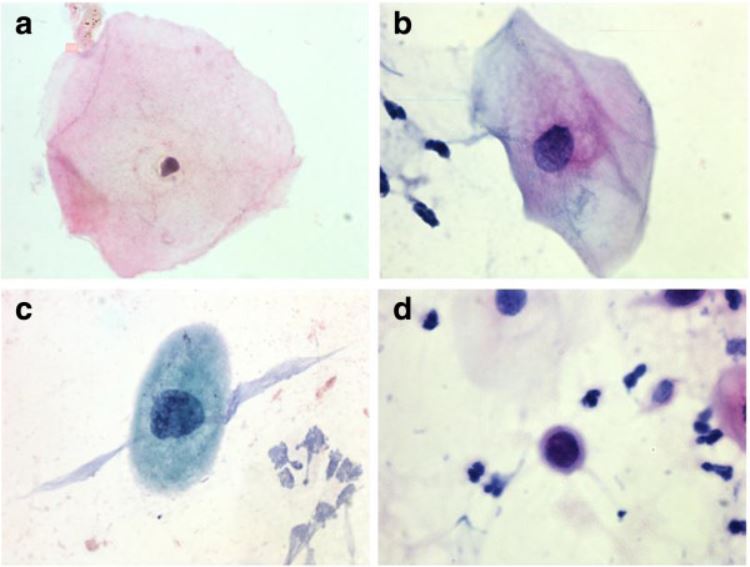
Examples of squamous cell findings during cervical cancer screening: a. Normal cell b. ASC-US c. LSIL d. HSIL
Image: “Diagnosis of cervical cells based on fractal and Euclidian geometrical measurements” by Prieto Bohórquez SE, Velásquez JO, Correa Herrera SC, Soracipa Muñoz MY. License: CC BY 2.0
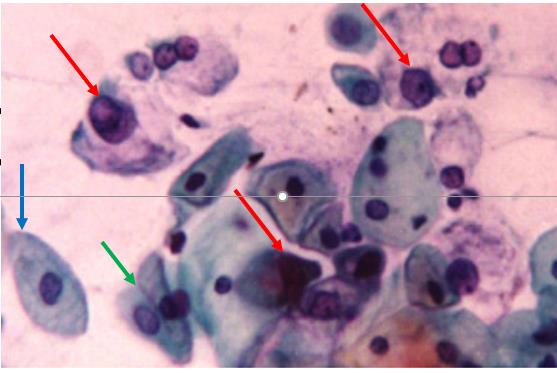
AGCUS favoring a neoplastic process, Pap stain Cervical cytology showing atypical glandular cells (red arrows), favoring a neoplastic process. The blue arrow points to a benign squamous epithelial cell, and the green arrow points to 2 benign endocervical cells.
Image: “Prevalence of cervical neoplastic lesions and Human Papilloma Virus infection” by el-All HS, Refaat A, Dandash K. License: CC BY 2.0, edited by Lecturio
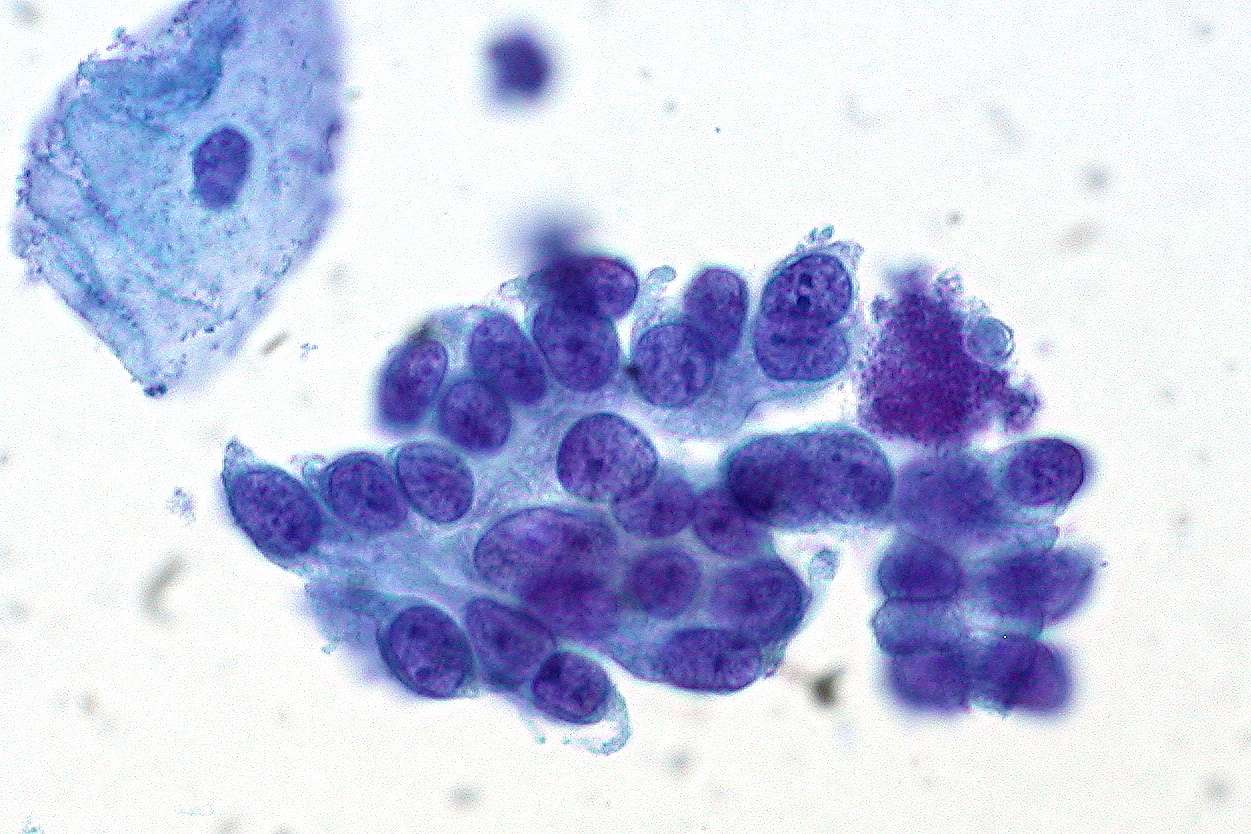
Cervical cytology showing adenocarcinoma in situ of the cervix: Note the benign squamous epithelial cell in the top left.
Image: “Adenocarcinoma in Situ of the Cervix” by Ed Uthman. License: CC BY 2.0
Management of Abnormal Results
Guidelines below reflect US recommendations. Management may vary based on country/region of practice and is affected by follow-up capabilities and resources (testing and treatment) available.
Determining risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+
Management of abnormal screeningScreeningPreoperative Care results is based on a patient’s risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ (given as a percentage) both now and in 5 years.[4,5,8]
Risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ includes:
CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3
Squamous cell carcinomaSquamous cell carcinomaCutaneous squamous cell carcinoma (cSCC) is caused by malignant proliferation of atypical keratinocytes. This condition is the 2nd most common skin malignancy and usually affects sun-exposed areas of fair-skinned patients. The cancer presents as a firm, erythematous, keratotic plaque or papule. Squamous Cell Carcinoma (SCC) or adenocarcinoma of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy
Management based on CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ risk was chosen because:
Persistent HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) infection is necessary for the development of high-grade precancer (HSIL) and cancer.
The goal of screeningScreeningPreoperative Care programs is to prevent cancer by identifying and treating precancer that is likely to progress.
Uses a combination of current screeningScreeningPreoperative Care results and past history (including unknown history)
People with the same overall levels of risk are treated the same way, regardless of the combination of results that yielded the risk level.
The same current test result may lead to different management options depending on how prior history/prior results affect the risk.
Note: This is a change from previous “results-based” guidelines, which recommended that management options be based on current test results.
Options for determining a patient’s risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+:
Use the ASCCP’s risk-based management guidelines app (paid) or web application (free, but requires registration).[4]
Look up risk level in one of the risk tables from the US National Institutes of Health[5]
Minimum requirements: prior results (includes “unknown”) and current results
Risk estimate and management tables[5]
Tables give:
The immediate/current risk of having CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+
The risk of developing CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ over the next 5 years
Current results obtained during follow-up of HPV-negative ASC-US
Current results obtained during follow-up of HPV-negative LSIL
Current results obtained during follow-up of HPV-positive NILM
Current colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening/biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma results
SurveillanceSurveillanceDevelopmental Milestones and Normal Growth following colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening/biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma results < CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 2 (no treatment):
Post-colposcopy after low-grade result (e.g., LSIL)
Post-colposcopy after high-grade result (e.g., HSIL)
Follow-up after treatment for CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 2 or CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3:
Immediate and 5-year risks after treatment
Long-term follow-up when there are 2 or 3 negative follow-up tests after treatment
Management:
Based on a patient’s risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ either:
Immediately/currently or
Developing within the next 5 years
Specific management recommendations are defined for different levels of risk.
The lower limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of each “risk level” is known as the clinical action thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction.
Choosing immediate vs. 5-year risk levels:
If the immediate risk is ≥ 4% → manage based on the immediate CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ risk level
If the immediate risk is < 4 % → manage based on the 5-year CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+
Note: ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening is a procedure in which a colposcopeColposcopeInstruments inserted into the vagina for examination of the tissues of the vagina and cervix by means of a magnifying lens.Diagnostic Procedures in Gynecology (magnifying devicemagnifying deviceInstruments inserted into the vagina for examination of the tissues of the vagina and cervix by means of a magnifying lens.Diagnostic Procedures in Gynecology) is used to enhance visualization of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, identify macroscopic abnormal areas, and guide biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
Table: Clinical action thresholds and preferred management[8]
Risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ developing within the next 5 years(clinical action thresholds)
Immediate risk of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ (clinical action thresholds)
Preferred management
4 % to < 25 %
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening recommended
25 % to < 60 %
Expedited treatment or colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening acceptable (for nonpregnant patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship ≥ 25 years of age)
≥ 60 %
Expedited treatment preferred (for nonpregnant patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship ≥ 25 years of age)
Table: Risk estimate and management – immediate and 5-year risks for CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ for abnormal screeningScreeningPreoperative Care results
History
Current HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) result
Current cytology result
CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ immediate risk (%)
CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ 5-year risk (%)
Recommended management
Unknown
HPV-negative
NILM
0.00
0.12
5 year follow-up
ASC-US
0.04
0.40
3 year follow-up
LSIL
1.1
2.0
1 year follow-up
ASC-H
3.4
3.8
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
25
27
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HPV-positive
NILM
2.1
4.8
1 year follow-up
ASC-US
4.4
7.3
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
LSIL
4.3
6.9
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
ASC-H
26
33
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HSIL+
49
53
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HPV-negative
HPV-negative
NILM
0.00
0.09
5 year follow-up
ASC-US
0.01
0.36
3 year follow-up
LSIL
0.44
0.79
1 year follow-up
ASC-H
2.8
3.3
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
14
14
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HPV-positive
NILM
0.74
2.3
1 year follow-up
ASC-US
2.0
3.8
1 year follow-up
LSIL
2.1
3.8
1 year follow-up
ASC-H
14
18
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
32
34
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
ASC-H atypical squamous cells, cannot exclude HSIL ASC-US: atypical squamous cells of undetermined significance HSIL: high-grade squamous intraepithelial lesion LSIL: low-grade squamous intraepithelial lesion NILM: no intraepithelial lesions or malignancy
Table: Risk estimate and management table:
Immediate and 5-year risks for CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ during surveillanceSurveillanceDevelopmental Milestones and Normal Growth following results that did not require immediate colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening[5]
History
Current HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) result
Current cytology result
CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ immediate risk (%)
CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 3+ 5-year risk (%)
Recommended management
HPV-negative ASC-US
HPV-negative
NILM
0.00
0.14
5 years of follow-up
ASC-US
0.06
0.78
1 year of follow-up
LSIL
2.4
3.1
1 year of follow-up
ASC-H
5.7
5.7
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
11
11
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HPV-positive
NILM
0.96
2.4
1 year of follow-up
ASC-US
2.1
6.6
1 year of follow-up
LSIL
2.6
2.6
1 year of follow-up
ASC-H
24
24
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
36
36
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HPV-negative LSIL*
HPV-negative
NILM
0.00
0.40
3 years of follow-up
ASC-US
0.00
4.0
1 year of follow-up
LSIL
0.0
4.4
1 year of follow-up
ASC-H
0.00
0.00
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
0.00
0.00
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HPV-positive
NILM
0.00
8.6
1 year of follow-up
ASC-US
5.3
6.9
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
LSIL
7.9
7.9
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
ASC-H
50
50
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
33
33
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HPV-positive NILM
HPV-negative
NILM
0.01
0.90
1 year of follow-up
ASC-US
0.35
2.6
1 year of follow-up
LSIL
2.3
2.3
1 year of follow-up
ASC-H
NA
NA
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
44
44
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
HPV-positive
NILM
4.1
7.2
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
ASC-US
5.4
9.5
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
LSIL
5.0
8.5
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
ASC-H
22
29
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HSIL+
44
50
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening or expedited treatment
*HPV-negative LSIL should be followed up with co-testing rather than primary HPV testing.
ASC-H atypical squamous cells, cannot exclude HSIL
ASC-US: atypical squamous cells of undetermined significance
HSIL: high-grade squamous intraepithelial lesion
LSIL: low-grade squamous intraepithelial lesion
NA: not applicable NILM: no intraepithelial lesions or malignancy
Special situations[4,20]
Unsatisfactory cytology:
No HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) or unknown result (any age) or HPV-negative (age ≥ 25) → repeat age-based screeningScreeningPreoperative Care in 2‒4 months
HPV-positive with unknown genotypeGenotypeThe genetic constitution of the individual, comprising the alleles present at each genetic locus.Basic Terms of Genetics (age ≥ 25) options:
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
HPV 16HPV 16A type of alphapapillomavirus usually associated with genital warts; and laryngeal neoplasms.Papillomavirus (HPV) or 18 positive (age ≥ 25) → colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
ASC-US or LSIL → repeat cytology in 1 year (preferred)
ASC-H or HSIL → colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with AGC:
Atypical endometrial cells →
Endometrial sampling PLUS
Endocervical sampling
+/-Colposcopy
All other AGC →
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening + endocervical sampling (all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Endometrial sampling only if age ≥ 35 or < 35 with abnormal uterine bleedingAbnormal Uterine BleedingAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym PALM-COEIN, with PALM representing the structural causes and COEIN indicating the non-structural causes. Abnormal Uterine Bleeding, obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity, or other conditions suggesting chronic anovulationAnovulationSuspension or cessation of ovulation in animals or humans with follicle-containing ovaries (ovarian follicle). Depending on the etiology, ovulation may be induced with appropriate therapy.Polycystic Ovarian Syndrome
For pregnant patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship:
Use the same clinical action thresholds as those for nonpregnant patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening and ectocervical biopsies can be performed during pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care.
Treatment of CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer 2 or 3 is not recommended.
If AISAISScoliosis is diagnosed → refer to a gynecologic oncologist for treatment
Contraindicated in pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care:
Expedited treatment (i.e., treatment without biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma)
Endocervical curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors (typically done with colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening)
These codes are used to document a routine visit for cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical CancerscreeningScreeningPreoperative Care in an asymptomatic patient, establishing the medical necessity for the screeningScreeningPreoperative Care tests.
Domain
Code
Description
ICD-10-CM
Z12.4
Encounter for screeningScreeningPreoperative Care for malignant neoplasm of cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy
These CPT codes represent the core procedures in cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical CancerscreeningScreeningPreoperative Care and evaluation: the Pap test to collect cervical cells, HPV testingHPV testingCervical Cancer Screening, and a colposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening with biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma to examine the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy under magnification if screeningScreeningPreoperative Care is abnormal.
Domain
Code
Description
CPT
88175
Cytopathology, cervical or vaginal (any reporting system), collected in preservative fluid, automated thin layer preparation
CPT
87624
Infectious agent detection by nucleic acid (DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure or RNARNAA polynucleotide consisting essentially of chains with a repeating backbone of phosphate and ribose units to which nitrogenous bases are attached. RNA is unique among biological macromolecules in that it can encode genetic information, serve as an abundant structural component of cells, and also possesses catalytic activity.RNA Types and Structure); Human PapillomavirusHuman papillomavirusHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV) (HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV)), high-risk types
CPT
57455
ColposcopyColposcopyThe examination, therapy or surgery of the cervix and vagina by means of a specially designed endoscope introduced vaginally.Cervical Cancer Screening of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy including upper/adjacent vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy; with biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma(s) of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy
Abnormal Findings Codes:
These codes are used to document the results of abnormal screeningScreeningPreoperative Care tests, such as Atypical Squamous Cells of Undetermined Significance (ASC-US) or the pathologic diagnosis of cervical dysplasia (CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer) from a biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
Domain
Code
Description
ICD-10-CM
R87.610
Atypical squamous cells of undetermined significance on cytologic smear of cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy (ASC-US)
ICD-10-CM
R87.612
Low grade squamous intraepithelial lesion on cytologic smear of cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy (LGSIL)
ICD-10-CM
N87.1
Moderate cervical dysplasia (CINCINAn increased tendency to acquire chromosome aberrations when various processes involved in chromosome replication, repair, or segregation are dysfunctional.Colorectal Cancer II)
ConizationConizationCervical Cancer of cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, with or without fulguration, with or without dilation and curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors, with or without repair; loop electrode excision
Fontham, E., Wolf, A., Church, T. R., Etzioni, R., Flowers, C. R., Herzig, A., Guerra, C. E., Oeffinger, K. C., Shih, Y. T., Walter, L. C., Kim, J. J., Andrews, K. S., DeSantis, C. E., Fedewa, S. A., Manassaram-Baptiste, D., Saslow, D., Wender, R. C., Smith, R. A. (2020). Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA: A Cancer Journal for Clinicians, 70(5), 321–346. https://doi.org/10.3322/caac.21628
Perkins, R. B., Guido, R. S., Castle, P. E., Chelmow, D., Einstein, M. H., Garcia, F., Huh, W. K., Kim, J. J., Moscicki, A. B., Nayar, R., Saraiya, M., Sawaya, G. F., Wentzensen, N., Schiffman, M., 2019 ASCCP Risk-Based Management Consensus Guidelines Committee. (2020). 2019 ASCCPrisk-based management consensus guidelinesfor abnormal cervical cancer screening tests and cancer precursors. Journal of Lower Genital Tract Disease, 24(2), 102–131. https://doi.org/10.1097/LGT.0000000000000525
Egemen, D., Cheung, L. C., Chen, X., Demarco, M., Perkins, R. B., Kinney, W., Poitras, N., Befano, B., Locke, A., Guido, R. S., Wiser, A. L., Gage, J. C., Katki, H. A., Wentzensen, N., Castle, P. E., Schiffman, M., Lorey, T. S. (2020). Risk estimates supporting the 2019 ASCCP risk-based management consensus guidelines. Journal of Lower Genital Tract Disease, 24(2), 132–143. https://doi.org/10.1097/LGT.0000000000000529
World Health Organization. (2021). WHOguideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention, second edition. Retrieved Feb 24, 2026, from https://www.who.int/publications/i/item/9789240030824
Moscicki, A. B., Flowers, L., Huchko, M. J., Long, M. E., MacLaughlin, K. L., Murphy, J., Spiryda, L. B., Gold, M. A. (2019). Guidelines for cervical cancer screening in immunosuppressed women without HIV infection. Journal of Lower Genital Tract Disease, 23(2), 87–101. https://doi.org/10.1097/LGT.0000000000000468
Iniesta, M. D., Schmeler, K. M., Ramirez, P. T. (2016). Tumors of the uterine cervix. In Kantarjian H.M., Wolff R. A. (Eds.), The MD Anderson Manual of Medical Oncology (3rd ed.). McGraw-Hill.