Chronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in individuals over age 40 with a history of more than 40 pack-years of cigarette smoking. Symptoms include progressive dyspnea and chronic cough. Prolonged expiration, wheezing, and/or diminished breath sounds may be noted on physical exam. The diagnosis is confirmed with pulmonary function testing. Management includes smoking cessation, pulmonary rehabilitation, and pharmacotherapy.
Chronic obstructive pulmonary diseasePulmonary diseaseDiseases involving the respiratory system.Blastomyces/Blastomycosis (COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)) is a heterogeneous lung disease characterized by chronic respiratory symptoms due to airflow limitation resulting from airwayAirwayABCDE Assessment disease and/or parenchymal destruction.
Types[1,5,7]
The subtypes may have differing presentations and response to therapy. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may have any combination of both.
Chronic bronchitisChronic bronchitisA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus:
Clinically defined
Productive cough > 3 months per year for at least 2 consecutive years
This definition has been used for decades and is the gold standard.
Clinical trials often use the term “chronic mucus hypersecretion.”
Must be in the absence of other causes of chronic cough
EmphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD):
Pathologically or radiologically defined
Destruction and permanent dilation of alveolar sacs
Epidemiology[1,5,7]
Worldwide:
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency: 11.7% (expected to rise) in individuals over 40
Annual deaths: 3 million
4th leading cause of death (soon to be 3rd)
In the United States:
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency: 16 million people
Annual deaths: > 140,000
3rd leading cause of death
Age:
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency peaks around 50–60 years of age
Age of onset is lower for heavy smokers.
SexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria:
Cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases (90% of cases)
2nd-hand smoke
Air pollutionPollutionThe presence of contaminants or pollutant substances in the air (air pollutants) that interfere with human health or welfare, or produce other harmful environmental effects. The substances may include gases; particulate matter; or volatile organic chemicals.Asthma
Indoor air pollutionPollutionThe presence of contaminants or pollutant substances in the air (air pollutants) that interfere with human health or welfare, or produce other harmful environmental effects. The substances may include gases; particulate matter; or volatile organic chemicals.Asthma from fire pits and stoves
Risk factors[2]
PrematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis birth
The pattern of pathologic changes depends on an individual’s underlying disease. The disease process predominantly affects the airways, but the lung parenchyma and pulmonary vasculature are also involved.
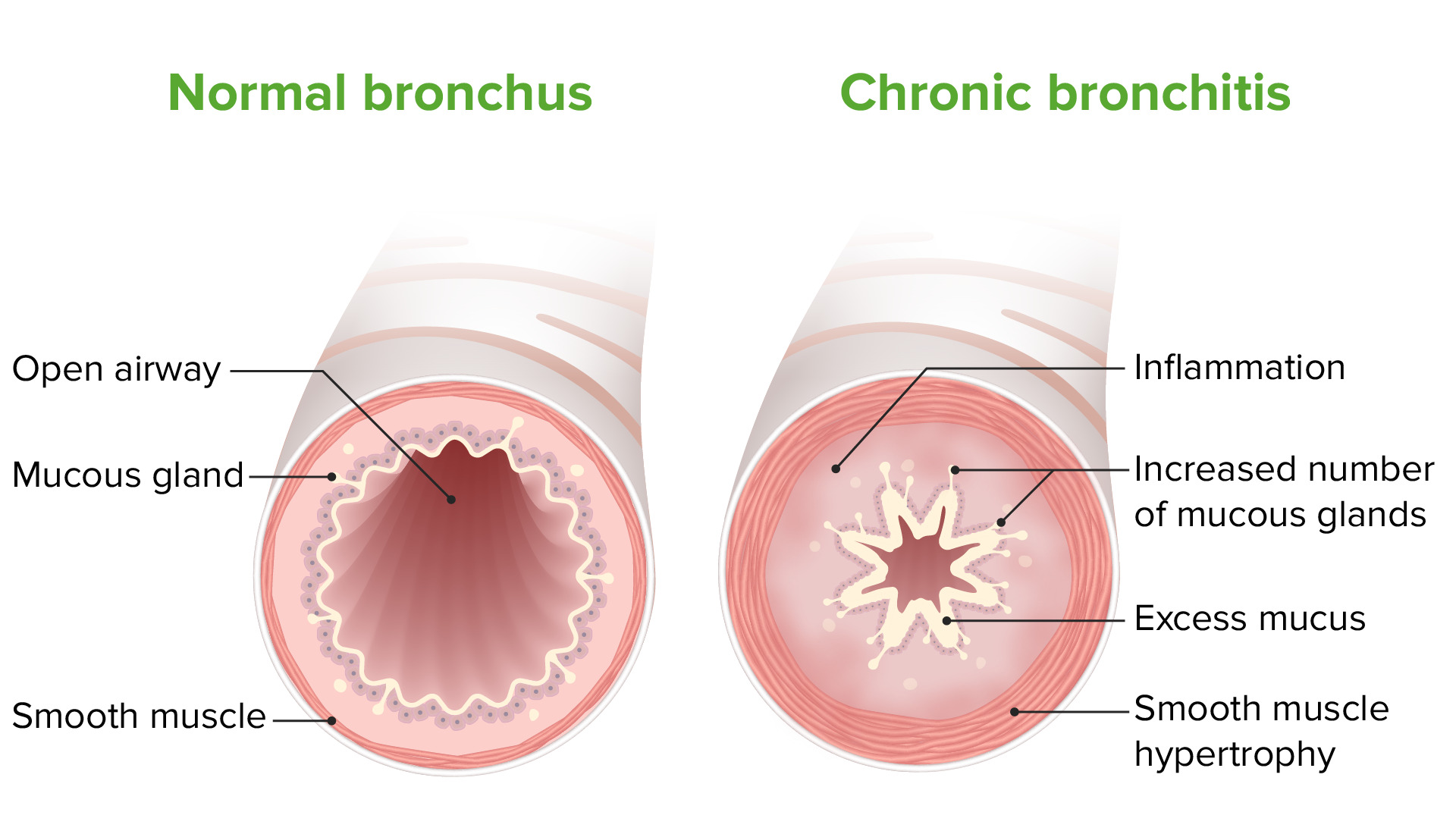
Chronic bronchitisChronic bronchitisA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus[5,7,21]
Damage to endothelial cells → ↓ mucociliary clearanceMucociliary clearanceA nonspecific host defense mechanism that removes mucus and other material from the lungs by ciliary and secretory activity of the tracheobronchial submucosal glands. It is measured in vivo as mucus transfer, ciliary beat frequency, and clearance of radioactive tracers.Acute Bronchitis
Mucous gland (goblet cellGoblet cellA glandular epithelial cell or a unicellular gland. Goblet cells secrete mucus. They are scattered in the epithelial linings of many organs, especially the small intestine and the respiratory tract.Barrett Esophagus) hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation → mucus hypersecretion and plugging
AirwayAirwayABCDE AssessmentedemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema and smooth muscle hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation and hypertrophyHypertrophyGeneral increase in bulk of a part or organ due to cell enlargement and accumulation of fluids and secretions, not due to tumor formation, nor to an increase in the number of cells (hyperplasia).Cellular Adaptation → luminal narrowing
Peribronchial fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans → bronchial distortionDistortionDefense Mechanisms
Chronic bronchitis pathophysiology: Inflammation, smooth muscle hypertrophy, and excess mucus production lead to progressive airway obstruction.
Image by Lecturio.
EmphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD)[5,7,21]
In normal lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy, there is a balance between:
ProteasesProteasesProteins and Peptides → break down elastin and connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology as part of normal tissue repairtissue repairThe process of generating a scar or less functional tissue with a different form and/or composition of the original tissue.Wound Healing:
Neutrophil elastaseElastaseA protease of broad specificity, obtained from dried pancreas. Molecular weight is approximately 25, 000. The enzyme breaks down elastin, the specific protein of elastic fibers, and digests other proteins such as fibrin, hemoglobin, and albumin.Proteins and Peptides
Matrix metalloproteinaseMatrix metalloproteinaseA family of zinc-dependent metalloendopeptidases that is involved in the degradation of extracellular matrix components.Pulmonary Fibrosis (MMP)
Cathepsins
Antiproteases → balance proteaseProteaseEnzyme of the human immunodeficiency virus that is required for post-translational cleavage of gag and gag-pol precursor polyproteins into functional products needed for viral assembly. HIV protease is an aspartic protease encoded by the amino terminus of the pol gene.HIV Infection and AIDS activity:
AAT
Secretory leukoprotease inhibitor derived from airwayAirwayABCDE AssessmentepitheliumEpitheliumThe epithelium is a complex of specialized cellular organizations arranged into sheets and lining cavities and covering the surfaces of the body. The cells exhibit polarity, having an apical and a basal pole. Structures important for the epithelial integrity and function involve the basement membrane, the semipermeable sheet on which the cells rest, and interdigitations, as well as cellular junctions. Surface Epithelium: Histology
Elafin
MMP tissue inhibitor
In emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD):
ProteaseProteaseEnzyme of the human immunodeficiency virus that is required for post-translational cleavage of gag and gag-pol precursor polyproteins into functional products needed for viral assembly. HIV protease is an aspartic protease encoded by the amino terminus of the pol gene.HIV Infection and AIDS activity exceeds antiprotease activity → tissue destruction
Alveolar destruction leads to:
Enlarged alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS)
↑ ComplianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology
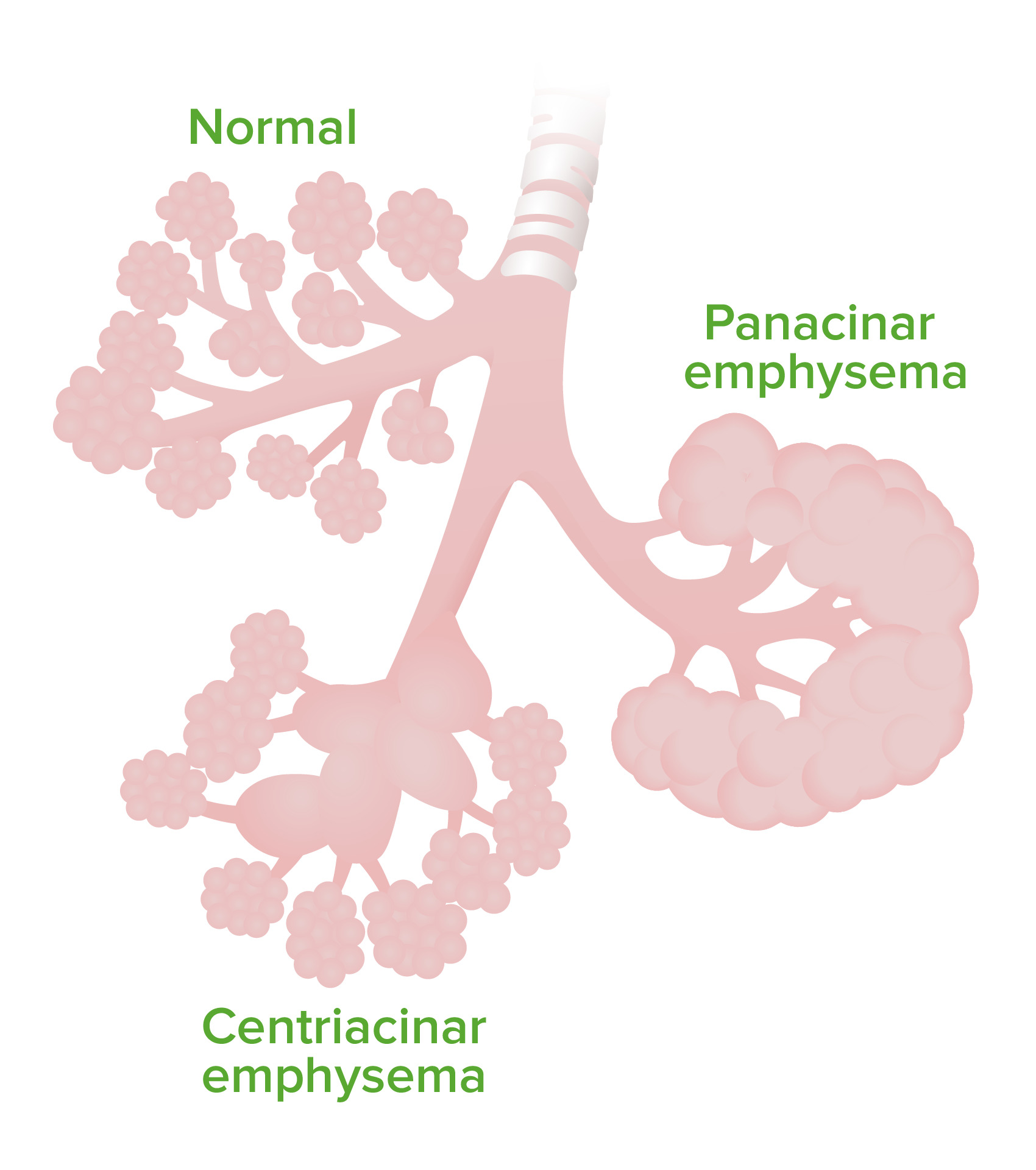
Centriacinar emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD) (associated with cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases):
Destruction of the respiratory bronchiolesBronchiolesThe small airways branching off the tertiary bronchi. Terminal bronchioles lead into several orders of respiratory bronchioles which in turn lead into alveolar ducts and then into pulmonary alveoli.Bronchial Tree: Anatomy and a central portion of the acini
More severe in the apical lung fields
Panacinar emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD) (associated with AAT deficiency):
Destruction of all parts of the acinus
More severe in the basal lung fields
Emphysema: The image demonstrates the difference in affected areas in centriacinar vs panacinar emphysema.
Image by Lecturio.
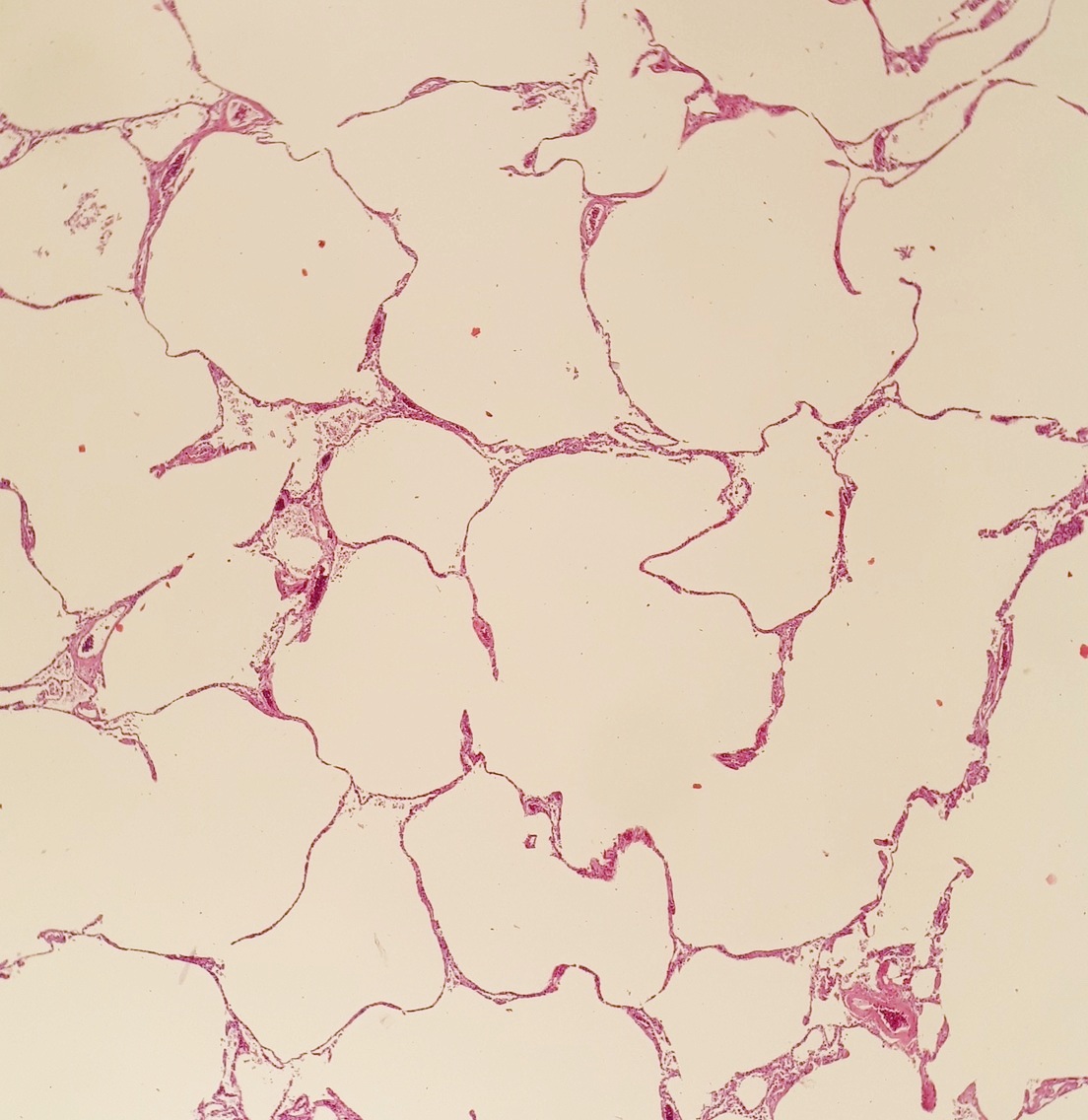
Histopathology of severe emphysema showing enlarged alveoli (white spaces)
Image: “Histopathology of emphysema” by Mikael Häggström, M.D. License: Public Domain
Effects of the pulmonary vasculature[5,21]
Tissue destruction → ↓ ability to oxygenate blood
HypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome → vasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure in small pulmonary arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology → ↑ vascular resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing
Chronic hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome → vascular remodelingVascular remodelingThe active alterations of vascular wall structures, often leading to elevated vascular resistance. It is associated with aging; atherosclerosis; diabetes mellitus; hypertension; pregnancy; pulmonary hypertension; and stroke, but is also a normal part of embryogenesis.Cor Pulmonale → irreversible pulmonary hypertensionPulmonary HypertensionPulmonary hypertension (PH) or pulmonary arterial hypertension (PAH) is characterized by elevated pulmonary arterial pressure, which can lead to chronic progressive right heart failure. Pulmonary hypertension is grouped into 5 categories based on etiology, which include primary PAH, and PH due to cardiac disease, lung or hypoxic disease, chronic thromboembolic disease, and multifactorial or unclear etiologies. Pulmonary Hypertension
Clinical Presentation
History[21]
When evaluating a patient with potential COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD), be sure to ask about:
Current or past smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Number of pack-years
Exposure to occupational dust or biomass smoke from indoor heating sources
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship suffer from chronic, progressive symptoms with acute exacerbations.
General:
Progressive dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea (particularly with exertion)
Chronic cough
Sputum production
Chest tightness
Weight gain or loss
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Acute exacerbation:
Worsening dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
Increased cough
Purulent sputum production
WheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever may or may not be present.
Physical examination[1,6,7,17,21]
COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) is usually at an advanced stage by the time exam findings are present. When examining a patient with possible COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD), look for the following findings:
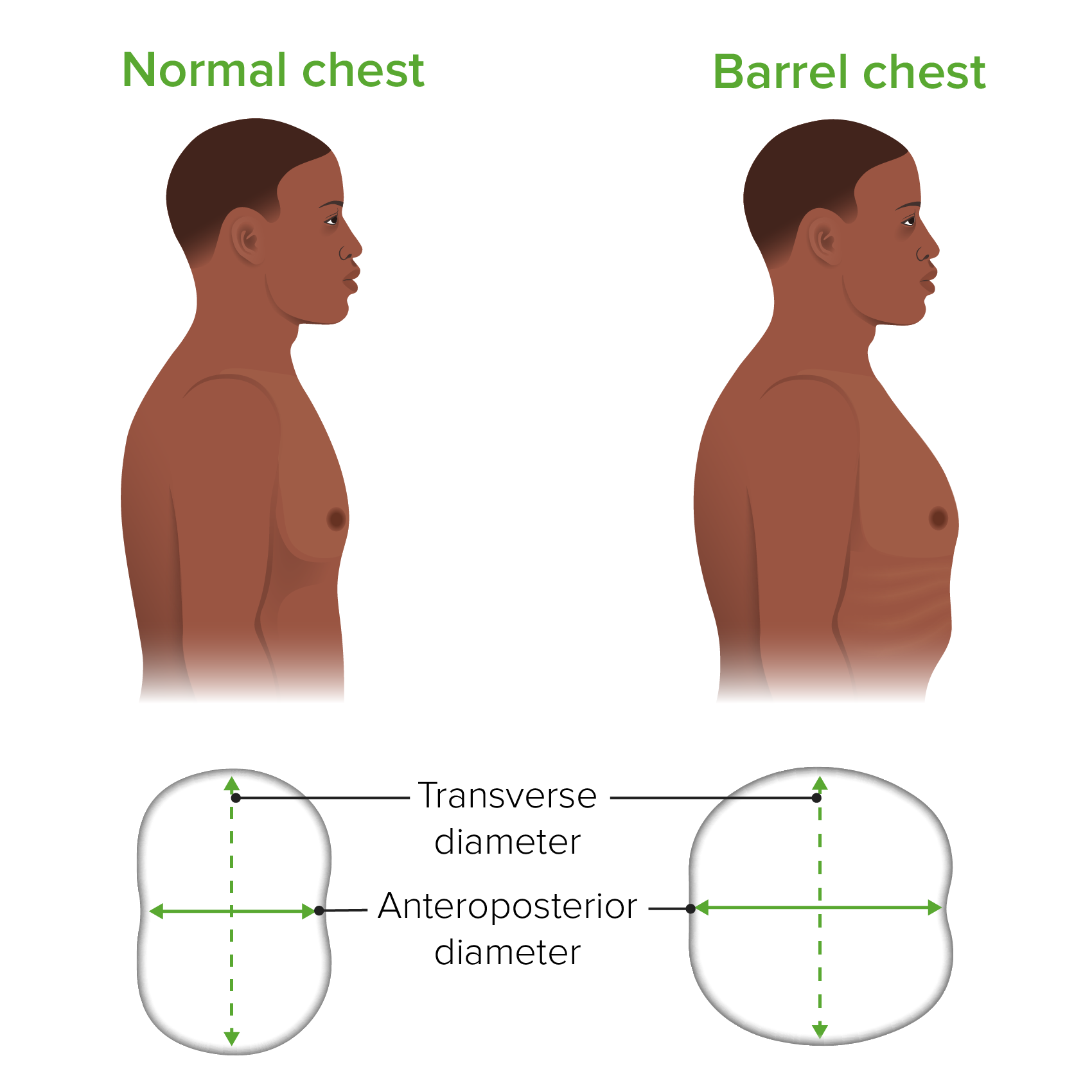
Barrel chest: increased anteroposterior (AP) chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy diameter from hyperinflationHyperinflationImaging of the Lungs and Pleura
WheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing
Diminished breath sounds
PalpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination and percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination:
Hyperresonance on percussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination
Reduced chest wallChest wallThe chest wall consists of skin, fat, muscles, bones, and cartilage. The bony structure of the chest wall is composed of the ribs, sternum, and thoracic vertebrae. The chest wall serves as armor for the vital intrathoracic organs and provides the stability necessary for the movement of the shoulders and arms. Chest Wall: Anatomy expansion
Extremities:
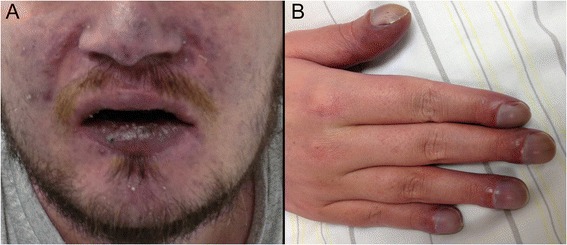
CyanosisCyanosisA bluish or purplish discoloration of the skin and mucous membranes due to an increase in the amount of deoxygenated hemoglobin in the blood or a structural defect in the hemoglobin molecule.Pulmonary Examination
Not typical for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) alone
Presence should raise suspicion for other comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus (e.g., lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung Cancer, bronchiectasisBronchiectasisBronchiectasis is a chronic disease of the airways that results from permanent bronchial distortion. This results from a continuous cycle of inflammation, bronchial damage and dilation, impaired clearance of secretions, and recurrent infections. Bronchiectasis, interstitial lung disease)
Findings suggestive of cor pulmonaleCor PulmonaleCor pulmonale is right ventricular (RV) dysfunction caused by lung disease that results in pulmonary artery hypertension. The most common cause of cor pulmonale is chronic obstructive pulmonary disease. Dyspnea is the usual presenting symptom. Cor Pulmonale:
Peripheral edemaPeripheral edemaPeripheral edema is the swelling of the lower extremities, namely, legs, feet, and ankles.Edema
Barrel chest as seen in emphysema: Note the increase in the anteroposterior diameter.
Image by Lecturio.
Clinical signs of hypoxemia: A: Cyanosis B: Digital clubbing
Image: “Clinical signs of chronic hypoxaemia” by Maximilian Patzig et al. License: CC BY 4.0
Clinical phenotypes[5]
Historically, textbooks used the terms “blue bloaterBlue bloaterA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus” and “pink puffer” to describe the phenotypes of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD), as these terms describe some of the clinical manifestations. However, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship often present with a mixture of features.
Chronic bronchitisChronic bronchitisA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus (“blue bloaterBlue bloaterA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus”):
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be overweight.
Frequent, productive cough
Peripheral edemaPeripheral edemaPeripheral edema is the swelling of the lower extremities, namely, legs, feet, and ankles.Edema
CyanosisCyanosisA bluish or purplish discoloration of the skin and mucous membranes due to an increase in the amount of deoxygenated hemoglobin in the blood or a structural defect in the hemoglobin molecule.Pulmonary Examination
EmphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD) (“pink puffer”):
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are generally thin and tachypneic.
Barrel chest
Infrequent cough
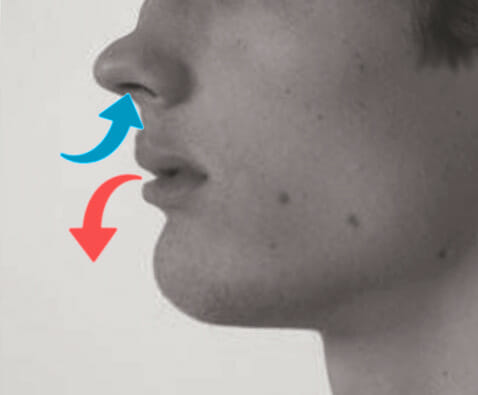
Pursed lip breathing
Accessory muscle use
Tripod positioning
Hyperresonant chest
Demonstrating pursed lip breathing, which is seen in emphysema
Image: “Pursed lip breathing” by O.Chaigasame. License: CC BY 4.0
There is substantial overlap between COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) symptoms and those of other disorders that cause airflow obstruction, such as asthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma and bronchiectasisBronchiectasisBronchiectasis is a chronic disease of the airways that results from permanent bronchial distortion. This results from a continuous cycle of inflammation, bronchial damage and dilation, impaired clearance of secretions, and recurrent infections. Bronchiectasis, so further testing helps confirm the diagnosis of COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD).
Pulmonary function tests
Pulmonary function tests (PFTs)are used to confirm COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) diagnosis. Testing results are indicative of obstruction, which is largely irreversible. Keep in mind, PFT findings alone are not diagnostic for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) and must be taken in context with the patient’s symptoms and biologic characteristics (e.g., age, sexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria, and height can affect baseline spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests values).
FRC: functional residual capacityFunctional residual capacityThe volume of air remaining in the lungs at the end of a normal, quiet expiration. It is the sum of the residual volume and the expiratory reserve volume. Common abbreviation is frc.Ventilation: Mechanics of Breathing
DLCODLCOPulmonary Function Tests: diffusing capacity of the lung for carbon monoxideCarbon monoxideCarbon monoxide (CO). A poisonous colorless, odorless, tasteless gas. It combines with hemoglobin to form carboxyhemoglobin, which has no oxygen carrying capacity. The resultant oxygen deprivation causes headache, dizziness, decreased pulse and respiratory rates, unconsciousness, and death.Carbon Monoxide Poisoning
↑ RV and total lung capacityTotal lung capacityThe volume of air contained in the lungs at the end of a maximal inspiration. It is the equivalent to each of the following sums: vital capacity plus residual volume; inspiratory capacity plus functional residual capacity; tidal volume plus inspiratory reserve volume plus functional residual capacity; or tidal volume plus inspiratory reserve volume plus expiratory reserve volume plus residual volume.Ventilation: Mechanics of Breathing (air trapping)
EmphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD):
Due to loss of surface area for gas exchangeGas exchangeHuman cells are primarily reliant on aerobic metabolism. The respiratory system is involved in pulmonary ventilation and external respiration, while the circulatory system is responsible for transport and internal respiration. Pulmonary ventilation (breathing) represents movement of air into and out of the lungs. External respiration, or gas exchange, is represented by the O2 and CO2 exchange between the lungs and the blood.Gas Exchange
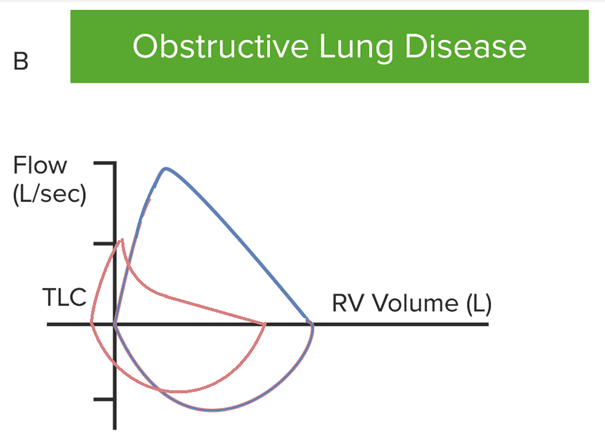
Rapid fall in expiratory flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure (dynamic airwayAirwayABCDE Assessment collapse) → produces a concave pattern
Post-bronchodilator test:[17,21]
Used to assess the reversibility of the obstructive condition
Inhaled albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs (400 µg) is administered.
FEV1/FVC ratio is measured:
70% is considered the lower limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal.
Postbronchodilator ratio < 70% indicates a non–fully reversible airflow obstruction.
Minimal reversibility is expected in COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD).
Flow-volume curve in a case of obstructive lung disease (red). Note that both flows are reduced due to obstruction. Dynamic airway collapse causes a rapid fall in expiratory flow, leading to a concave contour. Residual volume is increased due to air trapping, causing the curve to shift to the left.
TLC: total lung capacity
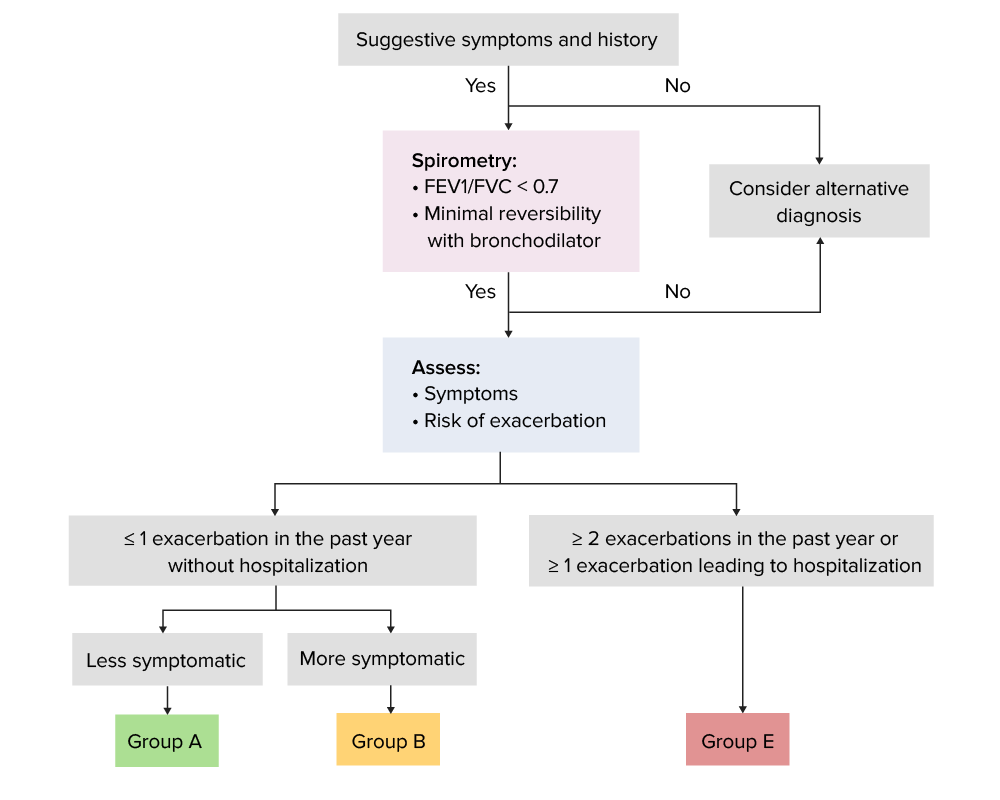
In addition to COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) diagnosis, spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests (postbronchodilator) results may be used in conjunction with symptoms to help stage severity. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) and equivalent National Institute for Health and Care Excellence (NICE) criteria are as follows:
Table: The Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria
GOLD class[21]
NICE 2010[17]
Severity of COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
Low risk: ≤ 1 exacerbation in the past year without hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
High risk: ≥ 2 exacerbations per year or ≥ 1 exacerbation leading to hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
Assessment:[8,21]
Group A:
Less symptomatic:
Mild or infrequent symptoms, such as dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea with strenuous exerciseStrenuous exercisePhysical activity which is usually regular and done with the intention of improving or maintaining physical fitness or health. Contrast with physical exertion which is concerned largely with the physiologic and metabolic response to energy expenditure.Cardiovascular Response to Exercise
CAT score < 10
Low risk of exacerbation
Group B:
More symptomatic:
Moderate to severe symptoms, such as the patient having to walk more slowly or to stop to catch their breath
CAT score ≥ 10 or persistent dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea at rest
Low risk of exacerbation
Group C:
Less symptomatic
High risk of exacerbation
Group D:
More symptomatic
High risk of exacerbation
Group E:
A new proposal in the 2023 GOLD guidelines
Groups C and D are grouped to include all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship at high risk of exacerbation (≥ 2 exacerbations per year or ≥ 1 exacerbation leading to hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium).[21]
Other systems (which are similar to the GOLD assessment) used to assess COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) severity and prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas include:
BODE (Body massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast index, airflow Obstruction, Dyspnea, and Exercise capacity) index
COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) Foundation system
↑ BNPBNPA peptide that is secreted by the brain and the heart atria, stored mainly in cardiac ventricular myocardium. It can cause natriuresis; diuresis; vasodilation; and inhibits secretion of renin and aldosterone. It improves heart function. It contains 32 amino acids.Renal Sodium and Water Regulation in cor pulmonaleCor PulmonaleCor pulmonale is right ventricular (RV) dysfunction caused by lung disease that results in pulmonary artery hypertension. The most common cause of cor pulmonale is chronic obstructive pulmonary disease. Dyspnea is the usual presenting symptom. Cor Pulmonale
AAT testing: Consider if COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) symptoms are present (not in typical demographic):
Younger
Nonsmoker
Concomitant, unexplained liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Blood eosinophil count:
May be used to help identify patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) exacerbations (despite appropriate bronchodilator therapy)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with eosinophil count > 300 cells/µL are most likely to benefit from inhaled corticosteroidsCorticosteroidsChorioretinitis.[12]
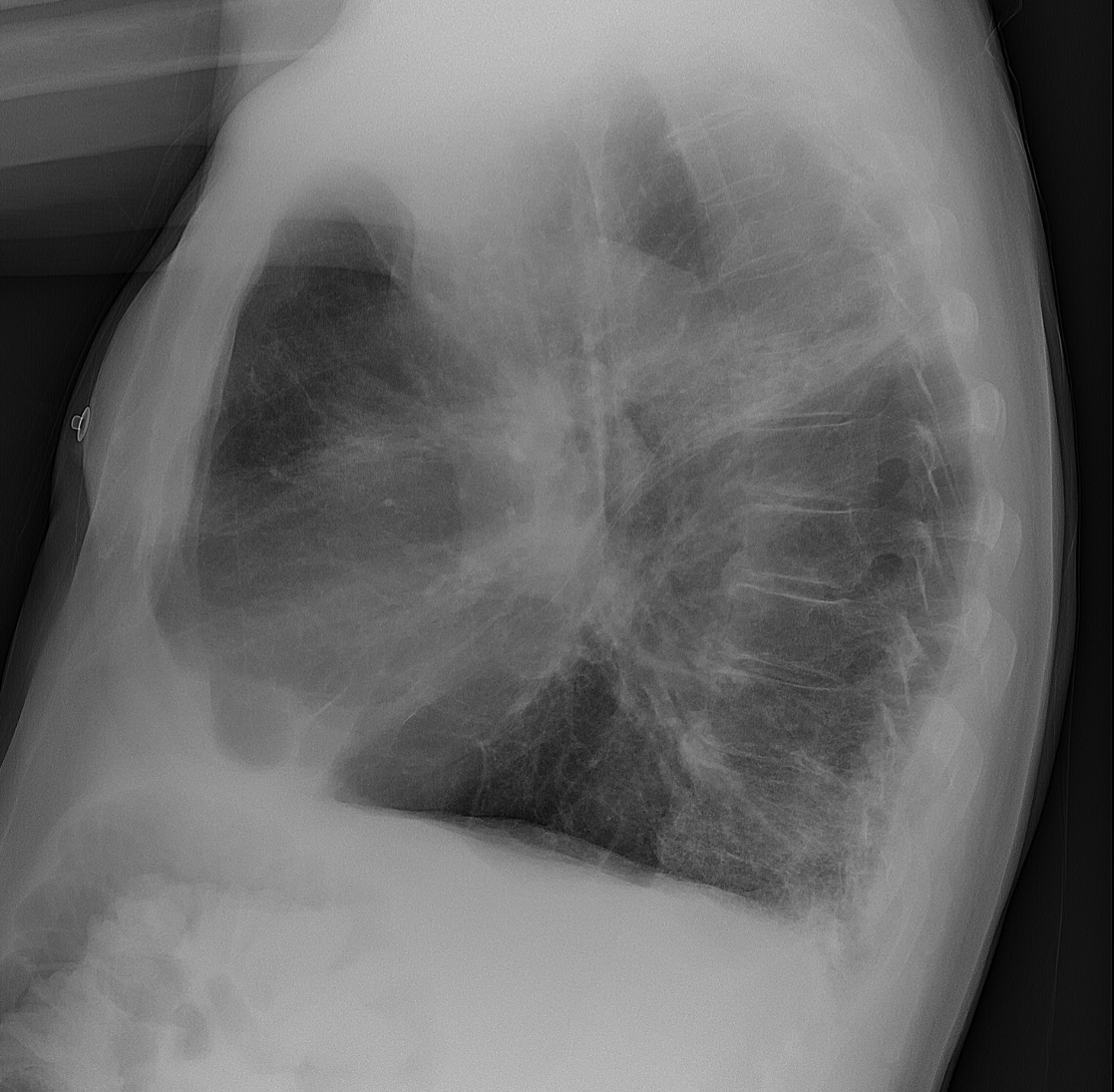
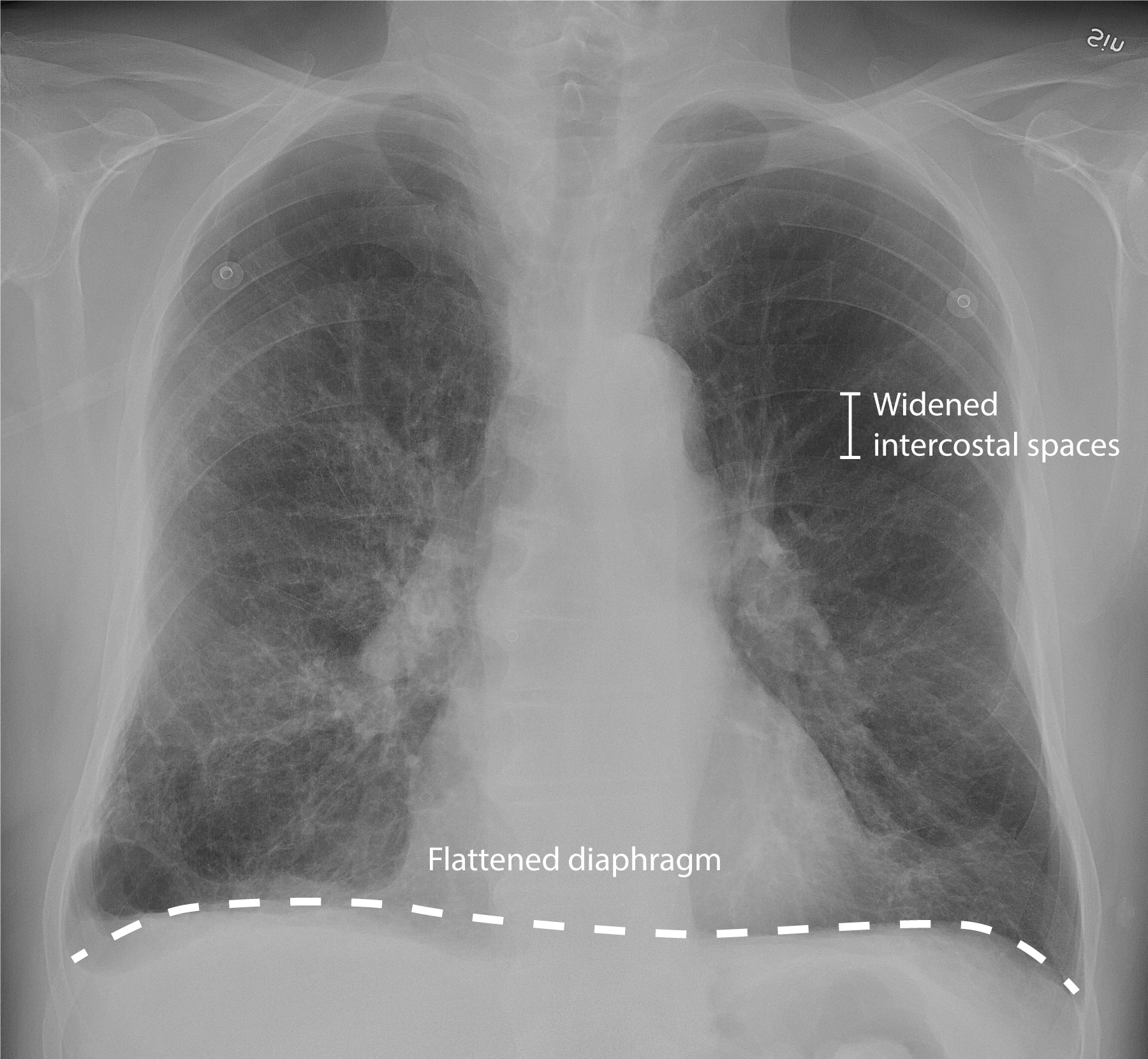
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests:[17,21]
Not used to diagnose COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD), but may be used to:
Exclude other diagnoses
Assess concurrent conditions (e.g., kyphoscoliosisKyphoscoliosisOsteomalacia and Rickets, bronchiectasisBronchiectasisBronchiectasis is a chronic disease of the airways that results from permanent bronchial distortion. This results from a continuous cycle of inflammation, bronchial damage and dilation, impaired clearance of secretions, and recurrent infections. Bronchiectasis))
Horizontal ribsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy
Flattened, low diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy
Hyperlucency
Attenuated peripheral vascular markings (due to parenchymal destruction)
Chest X-ray of an 81-year-old man with chronic obstructive pulmonary disease (COPD) and concomitant pneumonia
Image: “Chest X-ray of an 81-year-old man with chronic obstructive pulmonary disease (COPD), and concomitant pneumonia” by Mikael Häggström, M.D. License: CC0 1.0
Chest X-ray of an 81-year-old man with chronic obstructive pulmonary disease (COPD) presenting mainly with productive cough: Note the widened intercostal spaces, flattened diaphragm, and opacity in the inferior right upper lobe, which suggests concomitant pneumonia.
Image by Lecturio.
Chest CT:[17,21]
Able to assess emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD) extent and distribution
Criteria for lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung CancerscreeningScreeningPreoperative Care are metMETPreoperative Care
Management may vary depending on practice location. The following information is based on US and UK literature and guidelines.
Principles/treatment goals for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with stable COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)[21]
↓ Symptoms
↓ Exacerbations
↑ Patient function
↑ QualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
There is evidence that smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation and oxygen therapy prolong survival. No medications have been definitively proven to be disease-modifying, but trials are ongoing.
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation:
Critical in slowing lung function decline
NicotineNicotineNicotine is highly toxic alkaloid. It is the prototypical agonist at nicotinic cholinergic receptors where it dramatically stimulates neurons and ultimately blocks synaptic transmission. Nicotine is also important medically because of its presence in tobacco smoke.Stimulants replacement and pharmacotherapy may help improve long-term abstinence.
Vaccinations for:
Pneumococcal pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
InfluenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza
COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).
Tdap (if not previously vaccinated)
ShinglesShinglesVaricella-zoster virus (VZV) is a linear, double-stranded DNA virus in the Herpesviridae family. Shingles (also known as herpes zoster) is more common in adults and occurs due to the reactivation of VZV. Varicella-Zoster Virus/Chickenpox
Pulmonary rehabilitation:
Guided exercise and behavioral interventions
Goal is to improve functional capacity.
Helpful for all grades of COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
O2 therapy can improve survival if:
O2 saturation is < 88% in a stable patient (partial pressurePartial pressureThe pressure that would be exerted by one component of a mixture of gases if it were present alone in a container.Gas Exchange of oxygen (PaO₂) ≤ 55 mm Hg)
PaO₂ < 60 mm Hg and concurrent pulmonary hypertensionPulmonary HypertensionPulmonary hypertension (PH) or pulmonary arterial hypertension (PAH) is characterized by elevated pulmonary arterial pressure, which can lead to chronic progressive right heart failure. Pulmonary hypertension is grouped into 5 categories based on etiology, which include primary PAH, and PH due to cardiac disease, lung or hypoxic disease, chronic thromboembolic disease, and multifactorial or unclear etiologies. Pulmonary Hypertension, right-sided heart failureRight-Sided Heart FailureEbstein’s Anomaly, or polycythemiaPolycythemiaAn increase in the total red cell mass of the blood.Renal Cell Carcinoma
May be considered for chronic, severe hypercapniaHypercapniaA clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood.Neonatal Respiratory Distress Syndrome and hospitalizations for acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
During periods of high community prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). and influenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza, individuals with COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) should follow basic infection control measures:
Handwashing
Social distancing
Masking
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with AAT deficiency:
Refer to specialty centers for additional treatment.
Specialist referral[17]
Consultation with a specialist may be indicated if:
Diagnosis is uncertain
COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) is severe
Cor pulmonaleCor PulmonaleCor pulmonale is right ventricular (RV) dysfunction caused by lung disease that results in pulmonary artery hypertension. The most common cause of cor pulmonale is chronic obstructive pulmonary disease. Dyspnea is the usual presenting symptom. Cor Pulmonale is present
Frequent infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
HemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis
Symptoms disproportionate to objective findings
Additional medications may be needed (typical inhaled medications not providing adequate response)
Medications for long-term management
Medical therapy can:[21]
↓ Symptoms
↓ Exacerbation frequency and severity
Improve health status and qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
Short- and long-acting beta-agonists (SABAs and LABAs)
Short-and long-acting muscarinic antagonistsMuscarinic antagonistsDrugs that bind to but do not activate muscarinic receptors, thereby blocking the actions of endogenous acetylcholine or exogenous agonists. Muscarinic antagonists have widespread effects including actions on the iris and ciliary muscle of the eye, the heart and blood vessels, secretions of the respiratory tract, GI system, and salivary glands, GI motility, urinary bladder tone, and the central nervous system.Anticholinergic Drugs (SAMAs and LAMAs)
Medication recommendations vary slightly between different guidelines (e.g., GOLD recommends monotherapy for group B and ATA recommends dual therapy).
In general:
Long-acting agents are preferred for maintenance therapy.
Short-acting agents are used:
For immediate relief of symptoms (rescue)
In addition to long-acting therapy
ICS:
Not used as long-term monotherapy
Should be included (in combination therapy) if there are features of asthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma present
Combination therapy usually starts with LAMA/LABA.
Prescribing considerations:[17,21]
Ensure training in inhaler technique.
Be aware of:
Drug and device availability
Cost
Patient preference
Patient ability to use device
Minimize the number and types of devices, when possible.
Examples of device types:
Dry powder inhalers (DPIs)
Metered-dose inhalers (MDIs)
Soft mist inhalers (SMIs)
Nebulizers
For MDIs and SMIs, if there are concerns about the patient’s ability to perform coordinated triggering and deep, slow inhalation, consider spacer/valved holding chamber (VHC).
Note:[9]
About half of individuals who smoke have respiratory symptoms but no evidence of airwayAirwayABCDE Assessment obstruction on PFTs.
There is no evidence to support using bronchodilatorsBronchodilatorsAsthma Drugs or inhaled glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids in these patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Table: Inhaled medication options for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) (adult)[3,8,11,15,21]
Class
Medication options*
Typical initial dose
SABAs
AlbuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs
MDI or DPI (90 mcg): 2 inhalations every 4–6 hours, as needed
Nebulized solution (0.083%): 2.5 mg inhaled every 4–6 hours, as needed
DPI (18 µg/capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides): contents of 1 capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides inhaled daily
Umeclidinium
DPI (62.5 µg): 1 inhalation daily
GlycopyrrolateGlycopyrrolateA muscarinic antagonist used as an antispasmodic, in some disorders of the gastrointestinal tract, and to reduce salivation with some anesthetics.Anticholinergic Drugs
FluticasoneFluticasoneA steroid with glucocorticoid receptor activity that is used to manage the symptoms of asthma; allergic rhinitis, and atopic dermatitis.Glucocorticoids and salmeterolSalmeterolAsthma Drugs
DPI (250 µg/50 µg): 1 inhalation twice daily
BudesonideBudesonideA glucocorticoid used in the management of asthma, the treatment of various skin disorders, and allergic rhinitis.Asthma Drugs and formoterolFormoterolAsthma Drugs
FluticasoneFluticasoneA steroid with glucocorticoid receptor activity that is used to manage the symptoms of asthma; allergic rhinitis, and atopic dermatitis.Glucocorticoids and vilanterolVilanterolAsthma Drugs
DPI: 1 inhalation daily
ICS/LAMA/LABAs
BudesonideBudesonideA glucocorticoid used in the management of asthma, the treatment of various skin disorders, and allergic rhinitis.Asthma Drugs, glycopyrrolateGlycopyrrolateA muscarinic antagonist used as an antispasmodic, in some disorders of the gastrointestinal tract, and to reduce salivation with some anesthetics.Anticholinergic Drugs, and formoterolFormoterolAsthma Drugs
MDI: 2 inhalations twice daily
FluticasoneFluticasoneA steroid with glucocorticoid receptor activity that is used to manage the symptoms of asthma; allergic rhinitis, and atopic dermatitis.Glucocorticoids, umeclidinium, and vilanterolVilanterolAsthma Drugs
DPI: 1 inhalation daily
*List is not exhaustive.
GOLD 2023 treatment recommendations[8,12,16,21]
The GOLD criteria are used to recommend an evidence-based approach to COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD). The initial choice of pharmacologic therapy should be determined by an individualized approach based on a patient’s symptoms and exacerbation history, preferences, comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus, and spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests results.[12]
Recommended therapy escalates with each group based on the clinical presentation.
Suggested treatment for all groups:
General management (e.g., smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation, vaccinations)
SABA, SAMA, or combination as needed for episodic dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
If concomitant asthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma → ICS is mandatory
Keep in mind, this is a more effective algorithm for initial treatment than for individuals already on maintenance therapy.[8]
Subsequent adjustments are based on response → examples:
Continued symptoms on LABA or LAMA → escalate to LAMA/LABA combination
If symptoms on combination therapy, consider:
Switching type of device or medication
Investigating other potential causes
Augmenting/optimizing nonpharmacologic therapy
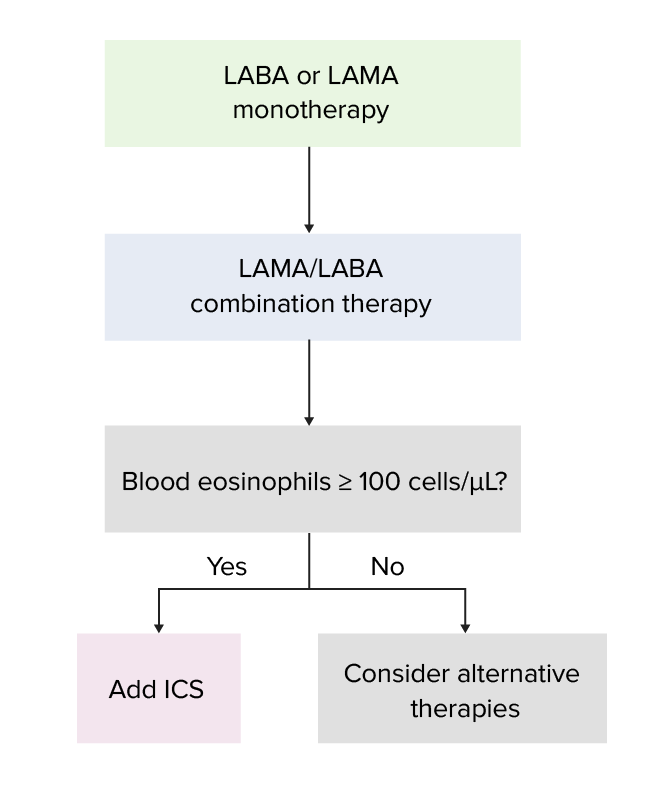
If persistent exacerbations, escalate as follows:
LABA or LAMA monotherapy → LAMA/LABA combination
LAMA/LABA combination → check blood eosinophilsEosinophilsGranular leukocytes with a nucleus that usually has two lobes connected by a slender thread of chromatin, and cytoplasm containing coarse, round granules that are uniform in size and stainable by eosin.Innate Immunity: Phagocytes and Antigen Presentation:
≥ 300 cells/µL → add ICS to combination therapy
100–300 cells/µL → may benefit from adding ICS to combination therapy
Table: GOLD treatment recommendations based on classification[8,16,21]
Classification
Symptom assessment
Risk of exacerbation
Recommended therapy
Group A
Less symptomatic
Low
Preferred: LABA or LAMA
Alternative: SABA or SAMA
Group B
More symptomatic
Preferred: LAMA/LABA combination
Alternative: LABA or LAMA
Group E
Group C*
Less symptomatic
High
LAMA/LABA combination
ICS/LAMA/LABA if blood eosinophilsEosinophilsGranular leukocytes with a nucleus that usually has two lobes connected by a slender thread of chromatin, and cytoplasm containing coarse, round granules that are uniform in size and stainable by eosin.Innate Immunity: Phagocytes and Antigen Presentation ≥ 300 cells/µL (consider if 100–300 cells/µL)
Group D*
More symptomatic
*Old classifications
Stepwise approach to augmenting therapy in patients with persistent exacerbations[21]
Image by Lecturio.
Official ATA recommendations[15,19]
For dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea or exercise intolerance:
Dual therapywith LAMA/LABA combination therapy is recommended over monotherapy.
If persistent symptoms → triple therapy with ICS/LAMA/LABA in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with ≥ 1 exacerbation in the past year requiring:
Antibiotics
Oral steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
For advanced dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea despite optimal therapy → opioidOpioidCompounds with activity like opiate alkaloids, acting at opioid receptors. Properties include induction of analgesia or narcosis.Constipation therapy can be considered with a shared decision-making approach
De-escalating triple therapy: ICS can be withdrawn if no exacerbations in the past year.
No recommendation for or against adding ICS in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) and eosinophiliaEosinophiliaAbnormal increase of eosinophils in the blood, tissues or organs.Autosomal Dominant Hyperimmunoglobulin E Syndrome
Long-term oral corticosteroid use is not recommended.
NICE recommendations[17]
LAMA/LABA combination should be offered if:
Continued symptoms despite nonpharmacologic therapy
On short-acting bronchodilator therapy
ICS/LABA therapy for:
Asthmatic features
Continued symptoms despite nonpharmacologic therapy
On short-acting bronchodilator therapy
If LAMA/LABA or ICS/LABA therapy is inadequate → ICS/LAMA/LABA therapy:
Consider if:
Nonpharmacologic therapy is optimized
No other cause for worsening symptoms
Symptoms are negatively impacting qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
≥ 1 severe exacerbations requiring hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium or ≥ 2 moderate exacerbations within a year
Trial for 3 months → if not improved, switch back
Additional medications[17,21]
Long-term antibiotics:
MacrolidesMacrolidesMacrolides and ketolides are antibiotics that inhibit bacterial protein synthesis by binding to the 50S ribosomal subunit and blocking transpeptidation. These antibiotics have a broad spectrum of antimicrobial activity but are best known for their coverage of atypical microorganisms. Macrolides and Ketolides (e.g., azithromycinAzithromycinA semi-synthetic macrolide antibiotic structurally related to erythromycin. It has been used in the treatment of Mycobacterium avium intracellulare infections, toxoplasmosis, and cryptosporidiosis.Macrolides and Ketolides, erythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides) associated with reduced exacerbations for 1 year (no data showing efficacy beyond 1 year)
May increase bacterial resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may keep antibiotics at home for use in an exacerbation as part of their self-management program.
Generally not used unless unable to use other long-term options
Examples:
Aminophylline
TheophyllineTheophyllineA methyl xanthine derivative from tea with diuretic, smooth muscle relaxant, bronchial dilation, cardiac and central nervous system stimulant activities. Theophylline inhibits the 3.Asthma Drugs
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with:
Chronic bronchitisChronic bronchitisA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus
Severe to very severe COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
History of exacerbations
May:
Improve lung function
Reduce moderate and severe exacerbations
Mucolytics:
May reduce risk of exacerbations in select patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
RegularRegularInsulin follow-up for management is essential because COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) is a chronic disease with a varying clinical course.
Review:
Symptoms and frequency of exacerbations
Risk factor exposure (e.g., smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases status)
Medication list and complianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology
Inhaler technique
Physical activity and exercise
VaccinationVaccinationVaccination is the administration of a substance to induce the immune system to develop protection against a disease. Unlike passive immunization, which involves the administration of pre-performed antibodies, active immunization constitutes the administration of a vaccine to stimulate the body to produce its own antibodies.Vaccination status
ComorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus
SpirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests monitoring should occur regularly (at least annually).
Adjust interventions, as necessary:
Augment or de-escalate therapy, when appropriate.
Reassess need for pulmonary rehabilitation.
Surgical intervention[17,20,21]
Surgery is reserved for severe cases not controlled with medical therapy to improve qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life.
Bronchoscopic LVR using a one-way endobronchial valve can improve FEV1 and functional outcomes.
Total thoracic lung volume is reduced, and healthier lung tissue is preferentially ventilated and perfused.
Lung transplant: indicated in end-stage lung disease
Palliative and end-of-life care[17,21]
Palliative treatments may be helpful to patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship at all stages of COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
Can include symptom relief of:
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
AnxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder and depression
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Since continued decline in lung function is expected, continual discussions should occur about the following:
Disease process
Treatment options and goals of care
ResuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome wishes and advance directivesAdvance DirectivesThe term advance directive (AD) refers to treatment preferences and/or the designation of a surrogate decision-maker in the event that a person becomes unable to make medical decisions on their own behalf. Advance directives represent the ethical principle of autonomy and may take the form of a living will, health care proxy, durable power of attorney for health care (DPAHC), and/or a physician’s order for life-sustaining treatment (POLST). Advance Directives
An exacerbation of COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) is an acute increase in symptoms beyond the normal day-to-day variation.[21]
Often triggered by:
Viral and bacterial respiratory infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Poor air qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement
Symptoms:
↑ Frequency and severity of cough
↑ Volume or change in character of sputum
↑ DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
Can be managed with outpatient or inpatient therapy, depending upon severity
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
Respiratory rateRespiratory rateThe number of times an organism breathes with the lungs (respiration) per unit time, usually per minute.Pulmonary Examination
Heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology
Oxygenation
C-reactive protein (CRP; if drawn)
Obtain:
Laboratory studies
ABG
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG)
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
Assess need for noninvasive ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing (NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation):
Severe dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea with increased work of breathingWork of breathingRespiratory muscle contraction during inhalation. The work is accomplished in three phases: lung compliance work, that required to expand the lungs against its elastic forces; tissue resistance work, that required to overcome the viscosity of the lung and chest wall structures; and airway resistance work, that required to overcome airway resistance during the movement of air into the lungs. Work of breathing does not refer to expiration, which is entirely a passive process caused by elastic recoil of the lung and chest cage.Pulmonary Examination or signs of respiratory fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Respiratory acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance ≤ 7.35 and partial pressurePartial pressureThe pressure that would be exerted by one component of a mixture of gases if it were present alone in a container.Gas Exchange of arterial carbon dioxide (PaCO2) ≥ 45 mm Hg)
Generally contraindicated if impaired consciousness or unable to clear secretions
Obtain ABG after 2 hours → compare with baseline
Intubate if worse or pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance < 7.25
Via nebulizer or MDIs with NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation (delivered with adaptor)
Initially dosed every hour for up to 2–3 doses
Then, continue every 2–4 hours based on patient symptoms and response.
Assess frequently for adverse cardiovascular effects.
Systemic corticosteroidsCorticosteroidsChorioretinitis: equivalent of 40 mg of prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants daily
Antibiotics:
Recommended if:
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
↑ Sputum volume
Sputum purulence
Should be initiated in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship requiring invasive or noninvasive ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing
Choice of therapy based on local resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing patterns
Options include:
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate
FluoroquinolonesFluoroquinolonesFluoroquinolones are a group of broad-spectrum, bactericidal antibiotics inhibiting bacterial DNA replication. Fluoroquinolones cover gram-negative, anaerobic, and atypical organisms, as well as some gram-positive and multidrug-resistant (MDR) organisms. Fluoroquinolones
Indications for hospital admission:
Severe underlying COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
Significant comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus
Failure to respond to initial medical management
Insufficient home support
Acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
New physical signs (e.g., cyanosisCyanosisA bluish or purplish discoloration of the skin and mucous membranes due to an increase in the amount of deoxygenated hemoglobin in the blood or a structural defect in the hemoglobin molecule.Pulmonary Examination)
Indications for ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus admission:
Invasive mechanical ventilationInvasive mechanical ventilationInvasive mechanical ventilation (IMV) is an advanced airway modality used for individuals with immediate or impending respiratory failure and/or in preparation for surgery. The IMV technique involves positive pressure ventilation delivered to the lungs through an endotracheal tube via a ventilator.Invasive Mechanical Ventilation needed
Hemodynamic instability
Mental status changes
Persistent or worsening hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome, hypercapniaHypercapniaA clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood.Neonatal Respiratory Distress Syndrome, or respiratory acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis despite oxygen administration or noninvasive ventilatory support.
Table: COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) exacerbation management by severity[21]
Severity
Criteria
Iverview of management
Mild
VAS < 5
RRRRRelative risk (RR) is the risk of a disease or condition occurring in a group or population with a particular exposure relative to a control (unexposed) group.Measures of Risk < 24 breaths/min
RRRRRelative risk (RR) is the risk of a disease or condition occurring in a group or population with a particular exposure relative to a control (unexposed) group.Measures of Risk ≥ 24 breaths/min
HR ≥ 95/min
O2 < 92% or change > 3% from baseline
CRP ≥ 10
ABG without acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Above plus ABG demonstrating worsening hypercapniaHypercapniaA clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood.Neonatal Respiratory Distress Syndrome and acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Above plus hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
ABG: arterial blood gas CRP: C-reactive protein HR: heart rate RR: respiratory rate VAS: visual analogue scale (measure of clinical dyspnea based on a scale of 0 to 10, with 10 being the worst dyspnea ever experienced)
1st choice: prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 40 mg daily (or equivalent) for total of 5 days
Alternatives:
Nebulized budesonideBudesonideA glucocorticoid used in the management of asthma, the treatment of various skin disorders, and allergic rhinitis.Asthma Drugs
Oral therapy preferred, but IV therapy may be required
Follow-up sputum cultures to ensure PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas or other resistant pathogens not present
Follow up ABG frequently (initially) to evaluate for CO2 retention and worsening acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Wean oxygen or NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation settings, as possible
Respiratory therapy consultation is often helpful.
Discharge:
Ensure clinical stability.
Double-check home maintenance therapy and optimize, if necessary.
Assess patient understanding of acute and chronic medications.
Reassess inhaler technique.
Determine if continued oxygen therapy is required.
Schedule follow-up within 1–4 weeks.
Acute COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) exacerbation with COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).[10,21]
COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). testing should be performed if patient presents with symptoms suggestive of infection.
Mild COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).: follow usual protocols for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD)
Moderate-to-severe COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).:
Additional pharmacotherapeutic approaches (in addition to usual management):
Remdesivir (start as soon as possible within 7 days after symptom onset)
Manage acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure with:
Complications associated with COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) include:[1]
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
Respiratory infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
Pulmonary hypertensionPulmonary HypertensionPulmonary hypertension (PH) or pulmonary arterial hypertension (PAH) is characterized by elevated pulmonary arterial pressure, which can lead to chronic progressive right heart failure. Pulmonary hypertension is grouped into 5 categories based on etiology, which include primary PAH, and PH due to cardiac disease, lung or hypoxic disease, chronic thromboembolic disease, and multifactorial or unclear etiologies. Pulmonary Hypertension → cor pulmonaleCor PulmonaleCor pulmonale is right ventricular (RV) dysfunction caused by lung disease that results in pulmonary artery hypertension. The most common cause of cor pulmonale is chronic obstructive pulmonary disease. Dyspnea is the usual presenting symptom. Cor Pulmonale
Long-term complications of steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors → osteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis
Antibiotic-related diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea (Clostridium difficileClostridium difficileA common inhabitant of the colon flora in human infants and sometimes in adults. The type species clostridioides difficile is formerly known as Clostridium difficile. It is a causative agent for clostridioides infections and is associated with pseudomembranous enterocolitis in patients receiving antibiotic therapy.ClostridiacolitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis)
X-ray showing a right-sided pneumothorax in a patient with chronic obstructive pulmonary disease (COPD): Pneumoperitoneum (arrow points to air under the diaphragm) is noted due to a diaphragmatic defect, which allows air from the pneumothorax to escape into the abdominal cavity.
Image:“Chest/abdomen X-ray showing right pneumothorax and also air under diaphragm suggesting perforated viscus.” by Fernanda Duarte et al. License: CC BY 4.0
Alpha-1 antitrypsinAlpha-1 antitrypsinPlasma glycoprotein member of the serpin superfamily which inhibits trypsin; neutrophil elastase; and other proteolytic enzymes.Alpha-1 Antitrypsin (AAT) Deficiency (AAT) deficiency: a genetic disorder causing the defective production of the proteaseProteaseEnzyme of the human immunodeficiency virus that is required for post-translational cleavage of gag and gag-pol precursor polyproteins into functional products needed for viral assembly. HIV protease is an aspartic protease encoded by the amino terminus of the pol gene.HIV Infection and AIDS inhibitor alpha-1 antitrypsinAlpha-1 antitrypsinPlasma glycoprotein member of the serpin superfamily which inhibits trypsin; neutrophil elastase; and other proteolytic enzymes.Alpha-1 Antitrypsin (AAT) Deficiency. Mutations leading to AAT deficiency can cause lung disease, production of an abnormal form of the enzyme leading to liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy dysfunction, or both. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may present with emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD), spontaneous pneumothoraxPneumothoraxA pneumothorax is a life-threatening condition in which air collects in the pleural space, causing partial or full collapse of the lung. A pneumothorax can be traumatic or spontaneous. Patients present with a sudden onset of sharp chest pain, dyspnea, and diminished breath sounds on exam.Pneumothorax, cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis, hepatitis, or hepatocellular carcinomaHepatocellular carcinomaHepatocellular carcinoma (HCC) typically arises in a chronically diseased or cirrhotic liver and is the most common primary liver cancer. Diagnosis may include ultrasound, CT, MRI, biopsy (if inconclusive imaging), and/or biomarkers. Hepatocellular Carcinoma (HCC) and Liver Metastases. Symptomatic adults with irreversible airflow obstruction on spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests should have a serum AAT level test. Management for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD) is supportive therapy that follows the guidelines for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD). For individuals who are not current smokers, IV infusions of AAT are recommended.
AsthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma: a chronic, inflammatory condition characterized by reversible airflow obstruction in the lower airways. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with intermittent or persistent wheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing, cough, and dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea. Diagnosis is usually confirmed with a pulmonary function testPulmonary function testPulmonary function tests are a group of diagnostic procedures yielding useful, quantifiable information about the rate of the flow of air through the individual’s airways, lung capacity, and the efficiency of gas exchange in relation to time. The most commonly utilized tests include spirometry (before and after bronchodilator use), lung volumes, and quantitation of diffusing capacity for carbon monoxide (CO). The tests can be influenced by the individual’s effort/fatigue, disease state, or anatomical malformation.Pulmonary Function Tests showing a reversible, obstructive pattern. Management varies based on severity and includes bronchodilatorsBronchodilatorsAsthma Drugs and inhaled corticosteroidsCorticosteroidsChorioretinitis for inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation control.
BronchiectasisBronchiectasisBronchiectasis is a chronic disease of the airways that results from permanent bronchial distortion. This results from a continuous cycle of inflammation, bronchial damage and dilation, impaired clearance of secretions, and recurrent infections. Bronchiectasis: a chronic condition with bronchial dilatation and destruction as a result of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and infection. Symptoms include dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, chronic cough, and purulent sputum. The diagnosis is made with imaging (X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests and CT). Management includes bronchodilatorsBronchodilatorsAsthma Drugs and antibiotics for acute exacerbations.
BronchiolitisBronchiolitisInflammation of the bronchioles.Pediatric Chest Abnormalities obliterans: a chronic, obstructive disease of the small airways usually caused by repeated cycles of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and scarringScarringInflammation. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with cough and persistent, progressive dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea. Pulmonary function tests are used for diagnosis. Management includes steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors and bronchodilatorsBronchodilatorsAsthma Drugs.
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR): an inability to produce normal cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics to meet metabolic needs. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage, and peripheral edemaPeripheral edemaPeripheral edema is the swelling of the lower extremities, namely, legs, feet, and ankles.Edema. BNPBNPA peptide that is secreted by the brain and the heart atria, stored mainly in cardiac ventricular myocardium. It can cause natriuresis; diuresis; vasodilation; and inhibits secretion of renin and aldosterone. It improves heart function. It contains 32 amino acids.Renal Sodium and Water Regulation will be elevated and pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema may be seen on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests. EchocardiographyEchocardiographyUltrasonic recording of the size, motion, and composition of the heart and surrounding tissues. The standard approach is transthoracic.Tricuspid Valve Atresia (TVA) confirms the diagnosis. Management relies on diuresis and medical optimization of cardiac function with beta blockers and ACE inhibitorsACE inhibitorsTruncus Arteriosus.
CysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans: an autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance disorder leading to dysfunction of chlorideChlorideInorganic compounds derived from hydrochloric acid that contain the Cl- ion.ElectrolyteschannelsChannelsThe Cell: Cell Membrane, which results in hyperviscous mucus and the accumulation of secretions. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship often have chronic respiratory infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, failure to thriveFailure to ThriveFailure to thrive (FTT), or faltering growth, describes suboptimal weight gain and growth in children. The majority of cases are due to inadequate caloric intake; however, genetic, infectious, and oncological etiologies are also common. Failure to Thrive, and pancreatic insufficiency. The gold standard for diagnosis is the sweat chlorideChlorideInorganic compounds derived from hydrochloric acid that contain the Cl- ion.Electrolytes test, which can be complemented by genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies. Management includes cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans transmembrane conductance regulator (CFTR) modulator therapy and system-specific strategies for supportive care.
Pulmonary embolismPulmonary EmbolismPulmonary embolism (PE) is a potentially fatal condition that occurs as a result of intraluminal obstruction of the main pulmonary artery or its branches. The causative factors include thrombi, air, amniotic fluid, and fat. In PE, gas exchange is impaired due to the decreased return of deoxygenated blood to the lungs. Pulmonary Embolism: obstruction of the pulmonary arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology most often due to thrombus migration from the deep venous system. Signs and symptoms include pleuritic chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, tachypneaTachypneaIncreased respiratory rate.Pulmonary Examination, and tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children. Severe cases can result in hemodynamic instability or cardiopulmonary arrestCardiopulmonary arrestCardiac arrest is the sudden, complete cessation of cardiac output with hemodynamic collapse. Patients present as pulseless, unresponsive, and apneic. Rhythms associated with cardiac arrest are ventricular fibrillation/tachycardia, asystole, or pulseless electrical activity.Cardiac Arrest. Chest CTACTAA non-invasive method that uses a ct scanner for capturing images of blood vessels and tissues. A contrast material is injected, which helps produce detailed images that aid in diagnosing vascular diseases.Pulmonary Function Tests is the primary method of diagnosis. Management includes oxygenation, anticoagulationAnticoagulationPulmonary Hypertension Drugs, and thrombolytic therapy for unstable patientsUnstable PatientsBlunt Chest Trauma.
Billing and Coding
Diagnosis Codes:
COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) is coded based on the specific type (e.g., emphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD), chronic bronchitisChronic bronchitisA subcategory of chronic obstructive pulmonary disease. The disease is characterized by hypersecretion of mucus accompanied by a chronic (more than 3 months in 2 consecutive years) productive cough. Infectious agents are a major cause of chronic bronchitis.Rhinovirus) and the presence of an acute exacerbation.
EmphysemaEmphysemaEnlargement of air spaces distal to the terminal bronchioles where gas-exchange normally takes place. This is usually due to destruction of the alveolar wall. Pulmonary emphysema can be classified by the location and distribution of the lesions.Chronic Obstructive Pulmonary Disease (COPD), unspecified
Evaluation & Workup:
This CPT code is for spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests, a type of pulmonary function testPulmonary function testPulmonary function tests are a group of diagnostic procedures yielding useful, quantifiable information about the rate of the flow of air through the individual’s airways, lung capacity, and the efficiency of gas exchange in relation to time. The most commonly utilized tests include spirometry (before and after bronchodilator use), lung volumes, and quantitation of diffusing capacity for carbon monoxide (CO). The tests can be influenced by the individual’s effort/fatigue, disease state, or anatomical malformation.Pulmonary Function Tests that is required to diagnose COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD) by demonstrating irreversible airflow obstruction (a low FEV1/FVC ratio).
Coding System
Code
Description
CPT
94060
Bronchodilation responsiveness, spirometrySpirometryMeasurement of volume of air inhaled or exhaled by the lung.Pulmonary Function Tests as in 94010, pre- and post-bronchodilator administration
Medications:
These codes are for the cornerstone inhaler therapies for COPDCOPDChronic obstructive pulmonary disease (COPD) is a lung disease characterized by progressive, largely irreversible airflow obstruction. The condition usually presents in middle-aged or elderly persons with a history of cigarette smoking. Signs and symptoms include prolonged expiration, wheezing, diminished breath sounds, progressive dyspnea, and chronic cough. Chronic Obstructive Pulmonary Disease (COPD). Short-acting beta-agonists (SABAs) like albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs are used for rescue, while long-acting muscarinic antagonistsMuscarinic antagonistsDrugs that bind to but do not activate muscarinic receptors, thereby blocking the actions of endogenous acetylcholine or exogenous agonists. Muscarinic antagonists have widespread effects including actions on the iris and ciliary muscle of the eye, the heart and blood vessels, secretions of the respiratory tract, GI system, and salivary glands, GI motility, urinary bladder tone, and the central nervous system.Anticholinergic Drugs (LAMAs) like tiotropium are used for maintenance.
Coding System
Code
Description
RxNorm
435
AlbuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs (ingredient)
RxNorm
225389
Tiotropium (ingredient)
ATC
R03BB04
Tiotropium bromideTiotropium BromideA scopolamine derivative and cholinergic antagonist that functions as a bronchodilator agent. It is used in the treatment of chronic obstructive pulmonary disease.Anticholinergic Drugs
Singh, D., Agusti, A., et al. (2019). Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. European Respiratory Journal, 53(5), 1900164. https://doi.org/10.1183/13993003.00164-2019
Han, M. K., Ye, W., et al. (2022). Bronchodilators in tobacco-exposed persons with symptoms and preserved lung function. New England Journal of Medicine, 387(13), 1173–1184. https://doi.org/10.1056/NEJMoa2204752
Halpin, D. M. G., Criner, G. J., et al. (2021). Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease: the 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine, 203(1), 24–36. https://doi.org/10.1164/rccm.202009-3533SO
Martinez, F. J., Rabe, K. F., et al. (2021). Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease: a randomized, double-blind, multicenter, parallel-group study. American Journal of Respiratory and Critical Care Medicine, 203(5), 553–564. https://doi.org/10.1164/rccm.202006-2618OC
Celli, B. R., Singh, D., Vogelmeier, C., Agusti, A. (2022). New perspectives on chronic obstructive pulmonary disease. International Journal of Chronic Obstructive Pulmonary Disease, 17, 2127–2136. https://doi.org/10.2147/COPD.S365771
Lipson, D. A., Criner, G., et al. (2019). The IMPACT trial: single inhaler triple therapy vs dual therapies: efficacy across multiple COPD endpoints over time. Airway Pharmacology and Treatment, PA2482. https://doi.org/10.1183/13993003.congress-2019.PA2482
Thompson, P. J., Criner, G. J., et al. (2022). Effect of chronic mucus hypersecretion on treatment responses to inhaled therapies in patients with chronic obstructive pulmonary disease: post hoc analysis of the IMPACT trial. Respirology, 27(12), 1034–1044. https://doi.org/10.1111/resp.14339
Nici, L., Mammen, M. J., et al. (2020). Pharmacologic management of chronic obstructive pulmonary disease: an official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 201(9), e56–e69. https://doi.org/10.1164/rccm.202003-0625ST
Patel, A. R., et al. (2019). Global initiative for chronic obstructive lung disease: the changes made. Cureus. https://doi.org/10.7759/cureus.4985
National Institute for Health and Care Excellence. (NICE). (2019). Chronic obstructive pulmonary disease in over 16s: diagnosis and management. Retrieved January 17, 2023, from https://www.nice.org.uk/guidance/ng115
National Institute for Health and Care Excellence (NICE). (2018). Chronic obstructive pulmonary disease (Acute exacerbation): Antimicrobial prescribing. Retrieved January 17, 2023, from https://www.nice.org.uk/guidance/ng114
Criner, G. J., Bourbeau, J., et al. (2015). Prevention of acute exacerbations of COPD. Chest, 147(4), 894–942. https://doi.org/10.1378/chest.14-1676
Garner, J. L., Shah, P. L. (2022). Bronchoscopic lung volume reduction: to the heart of the matter. American Journal of Respiratory and Critical Care Medicine, 206(6), 655–656. https://doi.org/10.1164/rccm.202206-1026ED
Global Initiative for Chronic Obstructive Lung Disease. (2023). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report). Retrieved June 24, 2023, from https://goldcopd.org/2023-gold-report-2/
Create your free account or log in to continue reading!