Bullous Pemphigoid and Pemphigus Vulgaris (Clinical)
Bullous Pemphigoid and Pemphigus Vulgaris (Clinical)
Bullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Diagnosis is made with biopsy and immunofluorescence (IF) staining to identify and localize the antibodies. Management involves immunosuppression with corticosteroids and other steroid-sparing immunomodulatory agents.
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris:[1,2,5,6]
A non–life-threatening, chronic autoimmune disease
Caused by loss of adhesionAdhesionThe process whereby platelets adhere to something other than platelets, e.g., collagen; basement membrane; microfibrils; or other ‘foreign’ surfaces.Coagulation Studies between the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions and dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris:[1,7,9,10]
Caused by loss of adhesionAdhesionThe process whereby platelets adhere to something other than platelets, e.g., collagen; basement membrane; microfibrils; or other ‘foreign’ surfaces.Coagulation Studies between keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions (acantholysisAcantholysisSeparation of the prickle cells of the stratum spinosum of the epidermis, resulting in atrophy of the prickle cell layer. It is seen in diseases such as pemphigus vulgaris and darier disease.Varicella-Zoster Virus/Chickenpox)
Epidemiology and etiology[1,2,5,7,9,11]
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency per year
Racial/ethnic biasBiasEpidemiological studies are designed to evaluate a hypothesized relationship between an exposure and an outcome; however, the existence and/or magnitude of these relationships may be erroneously affected by the design and execution of the study itself or by conscious or unconscious errors perpetrated by the investigators or the subjects. These systematic errors are called biases. Types of Biases
None
More common in:
Ashkenazi Jewish
Southeast Europe
Middle East
India
Etiology
None have been proven, but several possible associations:
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy
UV lightUV lightThat portion of the electromagnetic spectrum immediately below the visible range and extending into the x-ray frequencies. The longer wavelengths (near-uv or biotic or vital rays) are necessary for the endogenous synthesis of vitamin D and are also called antirachitic rays; the shorter, ionizing wavelengths (far-uv or abiotic or extravital rays) are viricidal, bactericidal, mutagenic, and carcinogenic and are used as disinfectants.Bullous Pemphigoid and Pemphigus Vulgaris
Possible associations:
Drugs (most commonly penicillaminePenicillamine3-mercapto-d-valine. The most characteristic degradation product of the penicillin antibiotics. It is used as an antirheumatic and as a chelating agent in wilson’s disease.Wilson Disease, captoprilCaptoprilA potent and specific inhibitor of peptidyl-dipeptidase a. It blocks the conversion of angiotensin I to angiotensin II, a vasoconstrictor and important regulator of arterial blood pressure. Captopril acts to suppress the renin-angiotensin system and inhibits pressure responses to exogenous angiotensin.Hypertension Drugs)
UV lightUV lightThat portion of the electromagnetic spectrum immediately below the visible range and extending into the x-ray frequencies. The longer wavelengths (near-uv or biotic or vital rays) are necessary for the endogenous synthesis of vitamin D and are also called antirachitic rays; the shorter, ionizing wavelengths (far-uv or abiotic or extravital rays) are viricidal, bactericidal, mutagenic, and carcinogenic and are used as disinfectants.Bullous Pemphigoid and Pemphigus Vulgaris
Both bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris and pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris are autoimmune diseasesAutoimmune diseasesDisorders that are characterized by the production of antibodies that react with host tissues or immune effector cells that are autoreactive to endogenous peptides.Selective IgA Deficiency that attack anchoring connections of the epidermal keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions.
Anatomy and physiology review[1]
DesmosomesDesmosomesA type of junction that attaches one cell to its neighbor. One of a number of differentiated regions which occur, for example, where the cytoplasmic membranes of adjacent epithelial cells are closely apposed. It consists of a circular region of each membrane together with associated intracellular microfilaments and an intercellular material which may include, for example, mucopolysaccharides.Bullous Pemphigoid and Pemphigus Vulgaris:
Junctional complex
Connect epidermal keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions to each other
Hemidesmosomes:
Similar to desmosomesDesmosomesA type of junction that attaches one cell to its neighbor. One of a number of differentiated regions which occur, for example, where the cytoplasmic membranes of adjacent epithelial cells are closely apposed. It consists of a circular region of each membrane together with associated intracellular microfilaments and an intercellular material which may include, for example, mucopolysaccharides.Bullous Pemphigoid and Pemphigus Vulgaris
Anchor the basal epidermal keratinocyteKeratinocyteEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Erythema Multiforme layer to the underlying basement membraneBasement membraneA darkly stained mat-like extracellular matrix (ecm) that separates cell layers, such as epithelium from endothelium or a layer of connective tissue. The ecm layer that supports an overlying epithelium or endothelium is called basal lamina. Basement membrane (bm) can be formed by the fusion of either two adjacent basal laminae or a basal lamina with an adjacent reticular lamina of connective tissue. Bm, composed mainly of type IV collagen; glycoprotein laminin; and proteoglycan, provides barriers as well as channels between interacting cell layers.Thin Basement Membrane Nephropathy (TBMN)
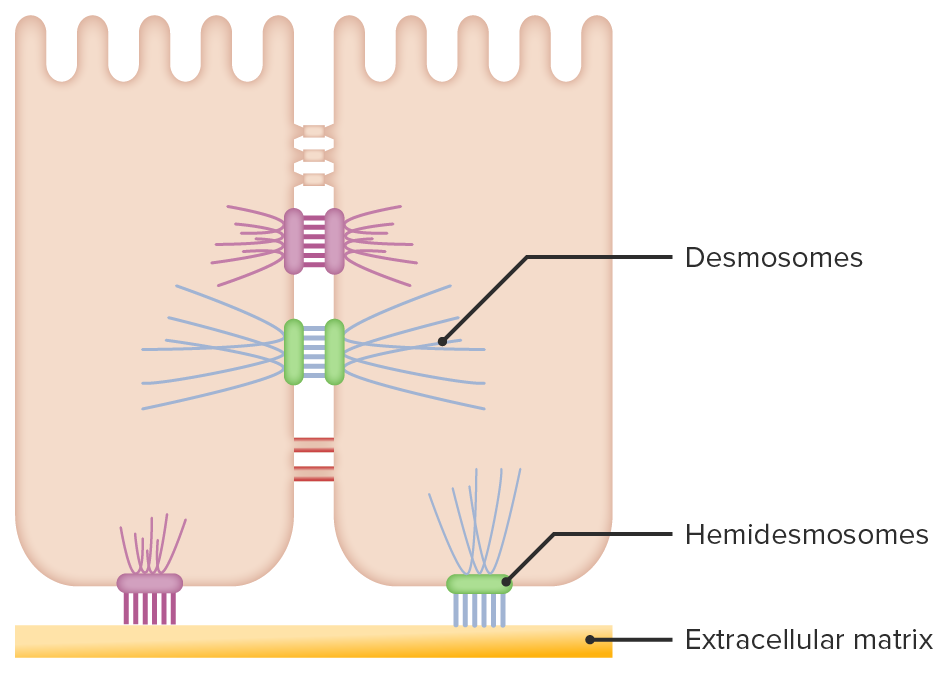
Epidermal keratinocyte connections:
Desmosomes connect keratinocytes to each other, while hemidesmosomes anchor the basal layer of keratinocytes to the basement membrane.
Image by Lecturio.
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris[1,2,11,12]
Type II hypersensitivity reactionType II hypersensitivity reactionType II hypersensitivity, also known as antibody-mediated cytotoxic hypersensitivity, is caused by immunoglobulin G (IgG) and IgM antibodies directed against antigens on cells or extracellular materials. The reaction leads to cytotoxic processes involving antibodies and the complement system. Type II Hypersensitivity Reaction
IgGIgGThe major immunoglobulin isotype class in normal human serum. There are several isotype subclasses of igg, for example, igg1, igg2a, and igg2b.Hypersensitivity PneumonitisautoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques attack hemidesmosomal proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis:
Targeted proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis: Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris antigens BP180 and BP230
Activation of complement and mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation → neutrophilsNeutrophilsGranular leukocytes having a nucleus with three to five lobes connected by slender threads of chromatin, and cytoplasm containing fine inconspicuous granules and stainable by neutral dyes.Innate Immunity: Phagocytes and Antigen Presentation and eosinophilsEosinophilsGranular leukocytes with a nucleus that usually has two lobes connected by a slender thread of chromatin, and cytoplasm containing coarse, round granules that are uniform in size and stainable by eosin.Innate Immunity: Phagocytes and Antigen Presentation release inflammatory mediators
ProteasesProteasesProteins and Peptides are produced → cause the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions to separate from the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions → result in large, tense bullaeBullaeErythema Multiforme
DesmosomesDesmosomesA type of junction that attaches one cell to its neighbor. One of a number of differentiated regions which occur, for example, where the cytoplasmic membranes of adjacent epithelial cells are closely apposed. It consists of a circular region of each membrane together with associated intracellular microfilaments and an intercellular material which may include, for example, mucopolysaccharides.Bullous Pemphigoid and Pemphigus Vulgaris connecting keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions to each other remain intact → overlying skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions is strong and taut
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris[1,7,9,10]
Type II hypersensitivity reactionType II hypersensitivity reactionType II hypersensitivity, also known as antibody-mediated cytotoxic hypersensitivity, is caused by immunoglobulin G (IgG) and IgM antibodies directed against antigens on cells or extracellular materials. The reaction leads to cytotoxic processes involving antibodies and the complement system. Type II Hypersensitivity Reaction
IgGIgGThe major immunoglobulin isotype class in normal human serum. There are several isotype subclasses of igg, for example, igg1, igg2a, and igg2b.Hypersensitivity PneumonitisautoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques attack desmosomal proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis:
Targeted proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis: desmogleinDesmogleinA group of desmosomal cadherins with cytoplasmic tails that resemble those of classical cadherins.The Cell: Cell Junctions (DSG) types 1 and 3
Disruption of desmosomesDesmosomesA type of junction that attaches one cell to its neighbor. One of a number of differentiated regions which occur, for example, where the cytoplasmic membranes of adjacent epithelial cells are closely apposed. It consists of a circular region of each membrane together with associated intracellular microfilaments and an intercellular material which may include, for example, mucopolysaccharides.Bullous Pemphigoid and Pemphigus Vulgaris → epidermal layers break apart → acantholysisAcantholysisSeparation of the prickle cells of the stratum spinosum of the epidermis, resulting in atrophy of the prickle cell layer. It is seen in diseases such as pemphigus vulgaris and darier disease.Varicella-Zoster Virus/Chickenpox
Dysfunctional skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions barrier
Susceptible to secondary infection
Hemidesmosomes remain intact:
Basal layer of keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions remain anchored to the basement membraneBasement membraneA darkly stained mat-like extracellular matrix (ecm) that separates cell layers, such as epithelium from endothelium or a layer of connective tissue. The ecm layer that supports an overlying epithelium or endothelium is called basal lamina. Basement membrane (bm) can be formed by the fusion of either two adjacent basal laminae or a basal lamina with an adjacent reticular lamina of connective tissue. Bm, composed mainly of type IV collagen; glycoprotein laminin; and proteoglycan, provides barriers as well as channels between interacting cell layers.Thin Basement Membrane Nephropathy (TBMN) → “row of tombstones” appearance on histology
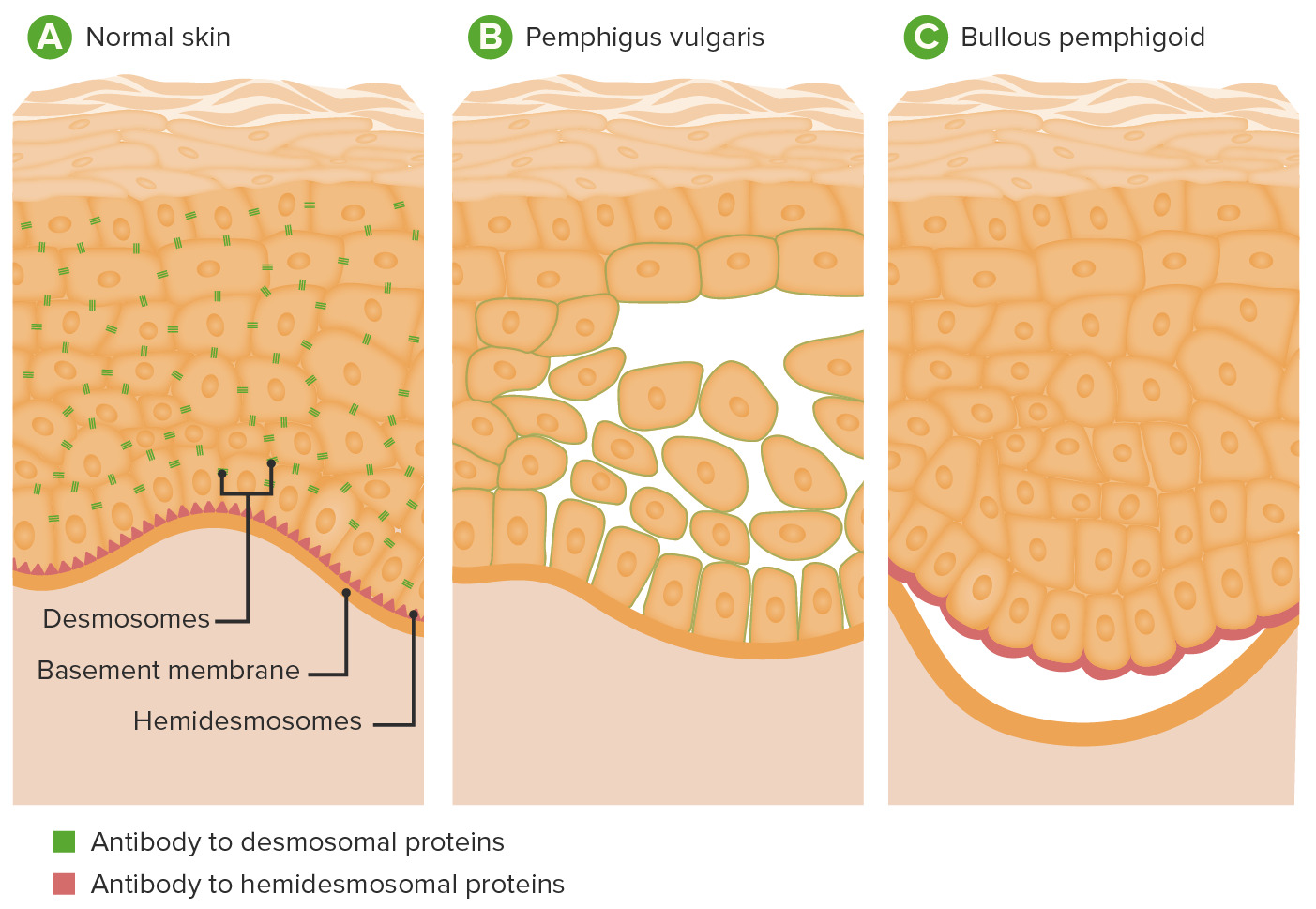
Pathophysiology of pemphigus vulgaris and bullous pemphigoid:
A: Location of desmosomes and hemidesmosomes in epidermis
B: In pemphigus vulgaris, antibodies to desmoglein result in disruption of desmosomes, causing acantholysis and blistering within the epidermis.
C: In bullous pemphigoid, antibodies against hemidesmosomal proteins result in separation of the epidermis from the dermis.
Image by Lecturio.
Clinical Presentation
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris[1,3,5,6]
Prodromal phase (lasting weeks to months):
PruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema) (moderate to severe)
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesions may appear:
Appear on normal or erythematous skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
Frequently affected locations:
Lower abdomen
Axillae
Extremity flexures
Inguinal folds
Mucosal involvement (10%‒30% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Cutaneous findings in bullous pemphigoid:
Multiple large, tense vesicles and bullae in the groin on normal to mildly erythematous skin
Image: “Localized flexural bullous pemphigoid” by Mehta V., Balachandran C. License: CC BY 2.0
Cutaneous findings in bullous pemphigoid: Multiple bullae, with some revealing moist erosions after rupture
Image: “A 74-year-old woman with a 1-month history of itching and skin rash” by Ghosh S., Ghosh A. K., Collier A. License: CC BY 2.0
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris[1,7,9,10,14]
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris is characterized by bullaeBullaeErythema Multiforme with the following properties:
Appear on normal or erythematous skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
Can occur anywhere on the body, most commonly:
Mucosa (almost always present):
Oral (often 1st site) → odynophagiaOdynophagiaEpiglottitis (painful swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility) → malnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Nasal mucosaNasal mucosaThe mucous lining of the nasal cavity, including lining of the nostril (vestibule) and the olfactory mucosa. Nasal mucosa consists of ciliated cells, goblet cells, brush cells, small granule cells, basal cells (stem cells) and glands containing both mucous and serous cells.Nose Anatomy (External & Internal) → epistaxisEpistaxisBleeding from the nose.Granulomatosis with Polyangiitis
ConjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy
VulvaVulvaThe vulva is the external genitalia of the female and includes the mons pubis, labia majora, labia minora, clitoris, vestibule, vestibular bulb, and greater vestibular glands. Vagina, Vulva, and Pelvic Floor: Anatomy, vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, and cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy
PenisPenisThe penis is the male organ of copulation and micturition. The organ is composed of a root, body, and glans. The root is attached to the pubic bone by the crura penis. The body consists of the 2 parallel corpora cavernosa and the corpus spongiosum. The glans is ensheathed by the prepuce or foreskin. Penis: Anatomy
Anus
Cutaneous:
Face and scalp
Trunk
GroinGroinThe external junctural region between the lower part of the abdomen and the thigh.Male Genitourinary Examination and axillaAxillaThe axilla is a pyramid-shaped space located between the upper thorax and the arm. The axilla has a base, an apex, and 4 walls (anterior, medial, lateral, posterior). The base of the pyramid is made up of the axillary skin. The apex is the axillary inlet, located between the 1st rib, superior border of the scapula, and clavicle. Axilla and Brachial Plexus: Anatomy
Secondary infection is common:
Purulent drainage
Surrounding erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion and indurationIndurationDermatologic Examination
Cutaneous findings in pemphigus vulgaris
Image: “Pemphigus Vulgaris Ulcer and Hemorrhagic Crust on the Trunk” by Mohsen Masjedi, Ali Asilian, Zabihollah Shahmoradi, Parvin Rajabi Dehnavi, and Bahareh Abtahi Naeini. License: CC BY 3.0, edited by Lecturio.
Mucosal erosion due to pemphigus vulgaris
Image: “Oral Lesions: The Clue to Diagnosis of Pemphigus Vulgaris” by Kuriachan D, Suresh R, Janardhanan M, Savithri V. License: CC BY 3.0
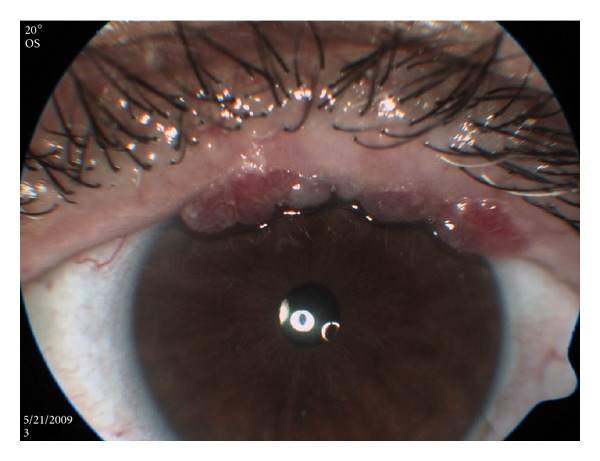
Conjunctival findings in pemphigus vulgaris
Image: “Multiple Conjunctival Papillomas of Eyelid Margins in Pemphigus vulgaris” by Avisar, I., Yassur, I., Kremer, I. License: CC BY 3.0
Diagnosis
Diagnosis involves checking for a Nikolsky signNikolsky SignDermatologic Examination, biopsies for routine histopathology and IF, and ELISAELISAAn immunoassay utilizing an antibody labeled with an enzyme marker such as horseradish peroxidase. While either the enzyme or the antibody is bound to an immunosorbent substrate, they both retain their biologic activity; the change in enzyme activity as a result of the enzyme-antibody-antigen reaction is proportional to the concentration of the antigen and can be measured spectrophotometrically or with the naked eye. Many variations of the method have been developed.St. Louis Encephalitis Virus testing.
Apply scraping pressure → look for skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions sloughing or blisterBlisterBullous Pemphigoid and Pemphigus Vulgaris rupture
Positive:skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions sloughing/rupture → disease within the epidermal layer
Negative:no skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions sloughing or rupture → disease at the dermal–epidermal junctionDermal–Epidermal JunctionBullous Pemphigoid and Pemphigus Vulgaris
Some experts recommend against in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who already have erosive skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesions[14]
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions biopsies → to assess the tissue itself:[1,11‒15]
Ideal biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma sites:
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris: lesional skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions[11]
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris: normal-appearing perilesional skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions (or mucosa)[14]
Routine histopathology (H&E staining)
Direct IF testing
Serum testing → to detect circulating antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions[1,12‒15]
Indirect IF
ELISAELISAAn immunoassay utilizing an antibody labeled with an enzyme marker such as horseradish peroxidase. While either the enzyme or the antibody is bound to an immunosorbent substrate, they both retain their biologic activity; the change in enzyme activity as a result of the enzyme-antibody-antigen reaction is proportional to the concentration of the antigen and can be measured spectrophotometrically or with the naked eye. Many variations of the method have been developed.St. Louis Encephalitis Virus
Table: Comparison of test findings
Test
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris[1,11,12]
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris[1,13-15]
Nikolsky’s sign
Negative
Positive
H&E staining
Subepidermal nonacantholytic blisters
Full-thickness epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions
Sparse inflammatory infiltrate in the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions
IF
Linear staining along the basement membraneBasement membraneA darkly stained mat-like extracellular matrix (ecm) that separates cell layers, such as epithelium from endothelium or a layer of connective tissue. The ecm layer that supports an overlying epithelium or endothelium is called basal lamina. Basement membrane (bm) can be formed by the fusion of either two adjacent basal laminae or a basal lamina with an adjacent reticular lamina of connective tissue. Bm, composed mainly of type IV collagen; glycoprotein laminin; and proteoglycan, provides barriers as well as channels between interacting cell layers.Thin Basement Membrane Nephropathy (TBMN)
Staining within the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions in a reticular (net-like) pattern
ELISAELISAAn immunoassay utilizing an antibody labeled with an enzyme marker such as horseradish peroxidase. While either the enzyme or the antibody is bound to an immunosorbent substrate, they both retain their biologic activity; the change in enzyme activity as a result of the enzyme-antibody-antigen reaction is proportional to the concentration of the antigen and can be measured spectrophotometrically or with the naked eye. Many variations of the method have been developed.St. Louis Encephalitis Virus
AutoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques against bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris antigens BP180 and BP230
AutoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques against DSG-1 and DSG-3
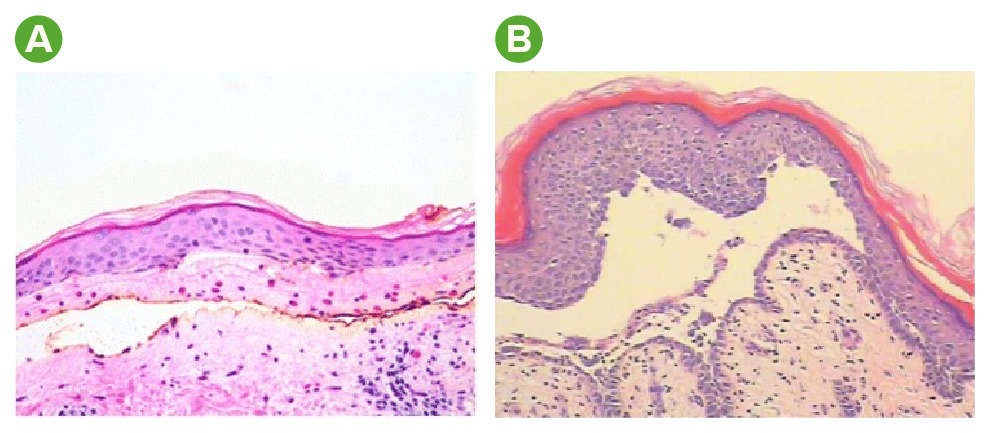
Histology findings in bullous pemphigoid and pemphigus vulgaris:
A: H&E staining in bullous pemphigoid reveals a subepidermal bulla and numerous eosinophils.
B: H&E staining in pemphigus vulgaris reveals a suprabasal acantholytic blister. Note the row-of-tombstone appearance (a layer of keratinocytes still attached to the basement membrane).
Image A: “Disease stabilization with pembrolizumab for metastatic acral melanoma in the setting of autoimmune bullous pemphigoid” by Beck, K. M., Dong, J., Geskin, L. J., Beltrani V. P., Phelps R. G., Carvajal, R. D., Schwartz, G., Saenger, Y. M., Gartrell, R. D. License: CC BY 4.0, edited by Lecturio.
Image B: “A rare presentation of pemphigus vulgaris as multiple pustules” by Yang, Y., Lin, M., Huang, S. J., Min, C., Liao, W. Q. License: CC BY 2.0, edited by Lecturio.
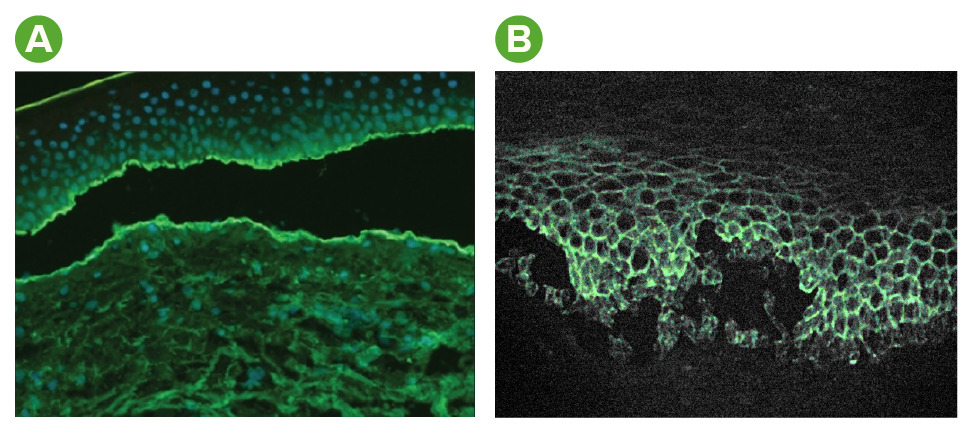
Immunofluorescence findings in bullous pemphigoid and pemphigus vulgaris:
A: In bullous pemphigoid, staining of complement and antibodies occurs at the dermal–epidermal junction.
B: In pemphigus vulgaris, staining of antibodies occurs within the epidermis in a reticular (net-like) pattern.
Image A: “A 74-year-old woman with a 1-month history of itching and skin rash” by Ghosh, S., Ghosh, A. K., Collier, A. License: CC BY 2.0, edited by Lecturio.
Image B: “Pemphigus immunofluorescence” by Emmanuelm. License: CC BY 3.0, edited by Lecturio.
Management
Individual protocols may vary based on location. The following information is based on international, European, and UK literature and guidelines for adult patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship. Management should be guided by specialist consultation (e.g., dermatology).
The goal of therapy for both bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris and pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris is to decrease autoantibody production while minimizing drug-induced side effects.
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions care:[11,12]
Example: clobetasolClobetasolA derivative of prednisolone with high glucocorticoid activity and low mineralocorticoid activity. Absorbed through the skin faster than fluocinonide, it is used topically in treatment of psoriasis but may cause marked adrenocortical suppression.Glucocorticoids propionate 0.05% cream
Taper from months 1‒4 to a dose of once/week; continue for a total of 12 months
Do not place on face or anogenital area.
Oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants (or prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants):
Doxycycline 200 mg daily (or other tetracyclineTetracyclineA naphthacene antibiotic that inhibits amino Acyl tRNA binding during protein synthesis.Drug-Induced Liver Injury) ± nicotinamide up to 2 g/day
MethotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy 10–12.5 mg/wk initially
DapsoneDapsoneA sulfone active against a wide range of bacteria but mainly employed for its actions against Mycobacterium leprae. Its mechanism of action is probably similar to that of the sulfonamides which involves inhibition of folic acid synthesis in susceptible organisms. It is also used with pyrimethamine in the treatment of malaria.Antimycobacterial Drugs 1–1.5 mg/kg daily
Severe disease (≥ 10 new lesions daily at different anatomical sites):[1,11,12]
≥ 10 new lesions daily at different anatomical sites
Options:
Superpotent topical corticosteroidsCorticosteroidsChorioretinitis (e.g., 30‒40 g/day of 0.5% clobetasolClobetasolA derivative of prednisolone with high glucocorticoid activity and low mineralocorticoid activity. Absorbed through the skin faster than fluocinonide, it is used topically in treatment of psoriasis but may cause marked adrenocortical suppression.Glucocorticoids propionate):
Follow the same taper as for mild-to-moderate disease.
Do not place on face or anogenital area.
Oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants
If not controlled (generally in 1‒3 weeks), can either:
Increase prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants dose to 0.75‒1 mg/kg/day
Add topical corticosteroid to the initial prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants regimen
Corticosteroid-dependent or relapsing disease:[1,11,12]
Add immunosuppressive drugsImmunosuppressive drugsAgents that suppress immune function by one of several mechanisms of action. Classical cytotoxic immunosuppressants act by inhibiting DNA synthesis. Others may act through activation of T-cells or by inhibiting the activation of helper cells. While immunosuppression has been brought about in the past primarily to prevent rejection of transplanted organs, new applications involving mediation of the effects of interleukins and other cytokines are emerging.Organ Transplantation, if not contraindicated:
MethotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy 5‒12.5 mg/wk
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants 1‒3 mg/kg/day, based on thiopurine methyltransferase activity
If contraindicated or patient is in generally poor health, consider:
Doxycycline ± nicotinamide
DapsoneDapsoneA sulfone active against a wide range of bacteria but mainly employed for its actions against Mycobacterium leprae. Its mechanism of action is probably similar to that of the sulfonamides which involves inhibition of folic acid synthesis in susceptible organisms. It is also used with pyrimethamine in the treatment of malaria.Antimycobacterial Drugs
OmalizumabOmalizumabAn anti-ige, recombinant, humanized monoclonal antibody which specifically binds to the c epsilon3 domain of immunoglobulin e, the site of high-affinity ige receptor binding. It inhibits the binding of ige to mast cells and basophils to reduce the severity of the allergic response and is used in the management of persistent allergic asthma.Asthma Drugs (consider in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with urticarial lesions and high serum IgEIgEAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Immunoglobulins: Types and Functions levels)
Resistant disease:[11,12]
Treat like relapsing disease with conventional immunosuppressive therapies
Other options:
RituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants
OmalizumabOmalizumabAn anti-ige, recombinant, humanized monoclonal antibody which specifically binds to the c epsilon3 domain of immunoglobulin e, the site of high-affinity ige receptor binding. It inhibits the binding of ige to mast cells and basophils to reduce the severity of the allergic response and is used in the management of persistent allergic asthma.Asthma Drugs
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas:[1,11,12]
Long-term remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches is possible (after months to years).
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris
Because of the severe nature of pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris, hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium is usually required until clinical control of the disease is achieved.[13]
Supportive care:[13,14]
Antiseptic baths
Ensure proper dental care.
Wound care:
Cover erosive lesions with low-adherence or nonadherent dressings.
Consider local emollientsEmollientsOleaginous substances used topically to soothe, soften or protect skin or mucous membranes. They are used also as vehicles for other dermatologic agents.Pityriasis Rosea and/or compresses.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control:
Local anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts
Analgesics
Ensure proper nutrition and hydration
Mild disease (< 5% of body surface area):[13‒15]
1st-line (choose 1 of the following):
Oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants (or prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants) 0.5‒1.5 mg/kg/day ± 1of the following:
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants
RituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants± oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 0.5 mg/kg/day
Contraindication to conventional immunosuppressive therapy
Options:
If only on oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants → add rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants
If taking rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants + prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants → increase prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants to 1 mg/kg/day
Rapid decrease after 3‒4 months if given in combination with rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants
Discontinuation of adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.VaccinationimmunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants can be considered at 6‒12 months to allow for slower tapering of oral corticosteroidsCorticosteroidsChorioretinitis
Table: Immunosuppressive therapy for pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris[13-15]
Medication
Typical dose
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants (or prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants)
0.5‒1.5 mg/kg/day
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants
RituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants
2 infusions of 1 g (2 weeks apart)
Note: These medications should be prescribed under the guidance of a specialist (e.g., dermatology)
Moderate-to-severe disease:[1,13‒15]
Criteria:
Multiple locations of mucosal involvement
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia and weight lossWeight lossDecrease in existing body weight.Bariatric Surgery secondary to oral lesions
Significant painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Lesions covering > 5% of body surface area
1st-line treatment (choose 1 of the following):
RituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants+ prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 1 mg/kg/day
Oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 1‒1.5 mg/kg/day ± 1of the following immunosuppressant agents:
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants
If initial therapy was rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants + prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 1 mg/kg/day → increase prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants to 1.5 mg/kg/day
If initial therapy was prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 1 mg/kg/day → increase to 1.5 mg/kg/day and add rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants or an immunosuppressant agent
If initial therapy was prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 1.5 mg/kg/day → add rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants or an immunosuppressant agent
Disease controlled: begin maintenance therapy
Maintenance therapy:
If initial therapy was oral prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants± immunosuppressant → slowly taper prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants and continue immunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants for up to 12 months
If initial therapy was rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants+ prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants → rapidly taper prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants at 4 weeks
Contraindicated in complete IgA deficiencyIgA deficiencyA dysgammaglobulinemia characterized by a deficiency of immunoglobulin a.Selective IgA Deficiency
Immunoadsorption:
≥ 2 cycles, each over 3‒4 days, separated by 4 weeks
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation:
Severe systemic infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Hypersensitivity to components of immunoadsorption column
MalnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries
Effects of long-term steroid use
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas:[1,13]
Often fatal without treatment
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock is the leading cause of death.
Slow clinical improvement is expected.
Evaluation before long-term corticosteroid or immunosuppressive therapy
General workup (all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship):[11,14]
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy panel
Hepatitis BHepatitis BHepatitis B virus (HBV) is a partially double-stranded DNA virus, which belongs to the Orthohepadnavirus genus and the Hepadnaviridae family. Most individuals with acute HBV infection are asymptomatic or have mild, self-limiting symptoms. Chronic infection can be asymptomatic or create hepatic inflammation, leading to liver cirrhosis and hepatocellular carcinoma (HCC). Hepatitis B Virus and C
Specific exams/management (based on proposed treatment risks):[11‒14]
DapsoneDapsoneA sulfone active against a wide range of bacteria but mainly employed for its actions against Mycobacterium leprae. Its mechanism of action is probably similar to that of the sulfonamides which involves inhibition of folic acid synthesis in susceptible organisms. It is also used with pyrimethamine in the treatment of malaria.Antimycobacterial Drugs treatment:
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants treatment: thiopurine methyltransferase (TPMT) activity
Ocular exam: exclude glaucomaGlaucomaGlaucoma is an optic neuropathy characterized by typical visual field defects and optic nerve atrophy seen as optic disc cupping on examination. The acute form of glaucoma is a medical emergency. Glaucoma is often, but not always, caused by increased intraocular pressure (IOP). Glaucoma and cataracts
High risk for tuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis:
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
Quantiferon/purified protein derivative (PPD)
Females of childbearing age: pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test
Corticosteroid treatment:
OsteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. OsteoporosisscreeningScreeningPreoperative Care and prophylaxisProphylaxisCephalosporins
InfluenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza (including H1N1)
Pneumococcal pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
SARS-CoV2
TetanusTetanusTetanus is a bacterial infection caused by Clostridium tetani, a gram-positive obligate anaerobic bacterium commonly found in soil that enters the body through a contaminated wound. C. tetani produces a neurotoxin that blocks the release of inhibitory neurotransmitters and causes prolonged tonic muscle contractions. Tetanus
Dermatitis herpetiformisDermatitis herpetiformisRare, chronic, papulo-vesicular disease characterized by an intensely pruritic eruption consisting of various combinations of symmetrical, erythematous, papular, vesicular, or bullous lesions. The disease is strongly associated with the presence of hla-b8 and hla-dr3 antigens. A variety of different autoantibodies has been detected in small numbers in patients with dermatitis herpetiformis.Celiac Disease: an uncommon autoimmune cutaneous eruption associated with celiac diseaseCeliac diseaseCeliac disease (also known as celiac sprue or gluten enteropathy) is an autoimmune reaction to gliadin, which is a component of gluten. Celiac disease is closely associated with HLA-DQ2 and HLA-DQ8. The immune response is localized to the proximal small intestine and causes the characteristic histologic findings of villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis. Celiac Disease: Dermatitis herpetiformisDermatitis herpetiformisRare, chronic, papulo-vesicular disease characterized by an intensely pruritic eruption consisting of various combinations of symmetrical, erythematous, papular, vesicular, or bullous lesions. The disease is strongly associated with the presence of hla-b8 and hla-dr3 antigens. A variety of different autoantibodies has been detected in small numbers in patients with dermatitis herpetiformis.Celiac Disease presents with intensely pruritic, inflammatory blisters on extensor surfaces. Nikolsky’s sign is negative. Diagnosis is confirmed on biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma and IF, which may show neutrophilic microabscessesNeutrophilic MicroabscessesPsoriasis and IgAIgARepresents 15-20% of the human serum immunoglobulins, mostly as the 4-chain polymer in humans or dimer in other mammals. Secretory iga is the main immunoglobulin in secretions.Immunoglobulins: Types and Functions deposits in the dermal papillary tips. Management includes dapsoneDapsoneA sulfone active against a wide range of bacteria but mainly employed for its actions against Mycobacterium leprae. Its mechanism of action is probably similar to that of the sulfonamides which involves inhibition of folic acid synthesis in susceptible organisms. It is also used with pyrimethamine in the treatment of malaria.Antimycobacterial Drugs and a gluten-free diet.
Stevens–Johnson syndrome: an immune-complex–mediated hypersensitivity reaction involving the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and mucous membranes, commonly triggered by medications: After a flu-like prodromal phase, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship develop erythematous macules with purpuric centers, bullaeBullaeErythema Multiforme, and skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions sloughing. Mucosal involvement is very common. Nikolsky’s sign is positive. Diagnosis is clinical, and management is supportive. Withdrawal of the causative agent is required.
Staphylococcal scalded skin syndromeStaphylococcal Scalded Skin SyndromeStaphylococcal scalded skin syndrome (SSSS), also known as Ritter disease and staphylococcal epidermal necrolysis, is a toxin-mediated condition caused by Staphylococcus aureus. The exfoliative toxin produced disseminates and cleaves desmoglein 1 in the epidermis, causing separation and detachment of the skin. Staphylococcal Scalded Skin Syndrome (SSSS) (SSSSSSSSStaphylococcal scalded skin syndrome (SSSS), also known as Ritter disease and staphylococcal epidermal necrolysis, is a toxin-mediated condition caused by Staphylococcus aureus. The exfoliative toxin produced disseminates and cleaves desmoglein 1 in the epidermis, causing separation and detachment of the skin. Staphylococcal Scalded Skin Syndrome (SSSS)): a life-threatening toxin-mediated disease, primarily of young children, caused by Staphylococcus aureusStaphylococcus aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Brain Abscess: DSG-1 is cleaved, resulting in diffuse cutaneous erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, tenderness, formation of bullaeBullaeErythema Multiforme, and superficial desquamationDesquamationStaphylococcal Scalded Skin Syndrome (SSSS) without mucosal involvement. Nikolsky’s sign is positive. Diagnosis is clinical and confirmed with culture data. Management is with antibiotics and supportive care.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose two distinct autoimmune blistering diseases: Bullous PemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris, which causes large, tense bullaeBullaeErythema Multiforme, and Pemphigus VulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris, which causes more fragile, easily ruptured blisters and erosionsErosionsCorneal Abrasions, Erosion, and Ulcers.
Coding System
Code
Description
ICD-10-CM
L12.0
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris
ICD-10-CM
L10.0
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris
Evaluation & Workup:
These codes are for a skin biopsySkin BiopsySecondary Skin Lesions, which is essential for diagnosis. One specimen is for standard histology, and a second from perilesional skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions is for direct immunofluorescence (DIF) to detect the autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques in the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.
Coding System
Code
Description
CPT
11102
Tangential biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions; single lesion
CPT
88346
Immunofluorescent study, each antibody; direct method
Medications:
These codes are for the primary immunosuppressive treatments. High-dose systemic corticosteroidsCorticosteroidsChorioretinitis like prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants are the first-line therapy, while rituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants, a monoclonal antibody, is used for severe or refractory cases.
Coding System
Code
Description
RxNorm
8640
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants (ingredient)
RxNorm
153281
RituximabRituximabA murine-derived monoclonal antibody and antineoplastic agent that binds specifically to the cd20 antigen and is used in the treatment of leukemia; lymphoma and rheumatoid arthritis.Immunosuppressants (ingredient)
References
Yancey, K. B., Lawley, T. J. (2008). Immunologically mediated skin diseases. In Fauci, A. S., Braunwald, E., Kasper, D.L., et al. (Eds.) Harrison’s Internal Medicine 1(7th ed., pp. 336–338).
Borradori, L., Van Beek, N., Feliciani, C., et al. (2022). Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). Journal of the European Academy of Dermatology and Venereology, 36(10), 1689–1704. https://doi.org/10.1111/jdv.18220
Venning, V. A., Taghipour, K., Mohd Mustapa, M. F., et al. (2012). British Association of Dermatologists’ guidelines for the management of bullous pemphigoid 2012. British Journal of Dermatology, 167(6), 1200–1214. https://doi.org/10.1111/bjd.12072
Murrell, D. F., Peña, S., Joly, P., et al. (2020). Diagnosis and management of pemphigus: recommendations of an international panel of experts. Journal of the American Academy of Dermatology, 82(3), 575.e.1–585.e1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7313440/
Joly, P., Horvath, B., Patsatsi, Α., et al. (2020). Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the European Academy of Dermatology and Venereology (EADV). Journal of the European Academy of Dermatology and Venereology, 34(9), 1900–1913. https://doi.org/10.1111/jdv.16752
Harman, K. E., Brown, D., Exton, L. S., et al. (2017). British Association of Dermatologists’ guidelines for the management of pemphigus vulgaris 2017. British Journal of Dermatology, 177(5), 1170–1201. https://doi.org/10.1111/bjd.15930
Murrell, D. F., et al. (2008). Consensus statement on definitions of disease, end points, and therapeutic response for pemphigus. Journal of the American Academy of Dermatology, 58(6), 1043–1046. https://www.jaad.org/article/S0190-9622(08)00118-7/fulltext
Hertl, M., et al. (2015). Pemphigus. S2 guideline for diagnosis and treatment—guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV). Journal of the European Academy of Dermatology and Venereology, 29, 405–414. https://onlinelibrary.wiley.com/doi/pdf/10.1111/jdv.12772
Murrell, D. F., et al. (2011). Definitions and outcome measures for bullous pemphigoid: Recommendations by an international panel of experts. Journal of the American Academy of Dermatology, 66(3), 479–485. https://www.jaad.org/article/S0190-9622(11)00840-1/pdf
Create your free account or log in to continue reading!