PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia is the main intracellular cation in all cells and is distributed unevenly between the intracellular fluidIntracellular fluidThe fluid inside cells.Body Fluid Compartments (98%) and extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (2%). This large disparity is necessary for maintaining the resting membrane potentialResting membrane potentialMembrane Potential of cells, and explains why K+ balance is tightly regulated. The GI tract secretes 5%–10% of the absorbed K+ daily; however, the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy are responsible for 90%–95% of the overall K+ regulation. While most of the K+ is reabsorbed in the proximal tubules, the majority of regulation occurs in the principal and α-intercalated cells of the collecting ducts. The most important regulatory mechanisms include aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia, plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ concentration, distal urinary flow rateFlow ratemaximum flow the ventilator will deliver a set tidal volume in liters per minuteInvasive Mechanical Ventilation, and the distal delivery of Na+ and water. HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia and hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia can result when K+ regulation is abnormal.
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia distribution:
Critical for nerve conduction and muscle contraction
Extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (ECF) space: 2%
Serum K+ levels represent the K+ in the ECF only.
Normal range: 3.5–5.2 mEq/L
Mechanisms of K+ balance:
Intake through the diet
GI losses (5%–10%)
Renal losses (90%–95%)
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System K+ shift:
K+ shifts primarily from the ECF into muscle and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy cells.
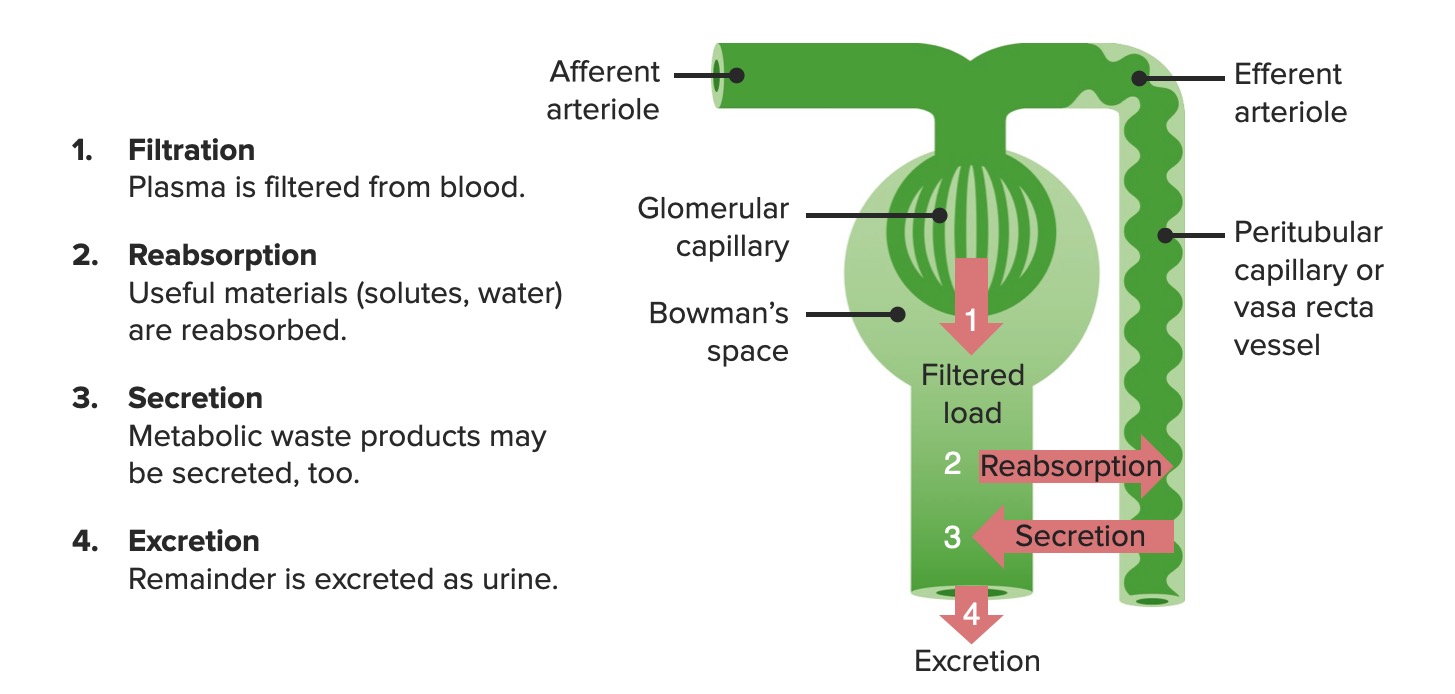
Renal processes to regulate water, electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, and waste
Filtration:PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products is filtered in the glomerular capillariesGlomerular capillariesKidneys: Anatomy, creating a filtrate that passes through the renal tubules.
Reabsorption: Required solutes and water are reabsorbed from the tubule lumen back into the blood.
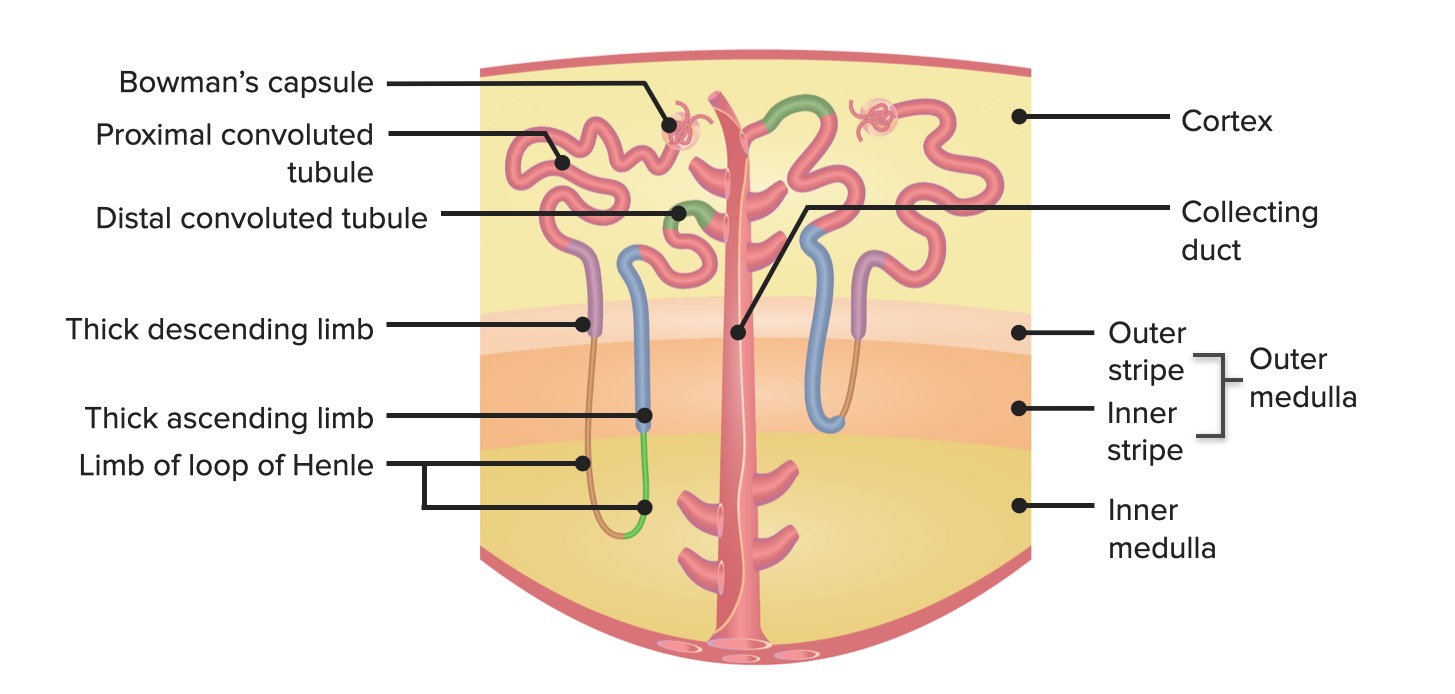
NephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy anatomy review
Nephrons are the functional units of the kidney.
NephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy segments (in order through which the filtrate flows):
Bowman’s capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides
Proximal convoluted tubuleProximal convoluted tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Osmotic Diuretics
Loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System:
Distal convoluted tubuleDistal convoluted tubuleThe portion of renal tubule that begins from the enlarged segment of the ascending limb of the loop of henle. It reenters the kidney cortex and forms the convoluted segments of the distal tubule.Gitelman Syndrome
Collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma
Types of nephrons:
Cortical (or superficial): Loops of Henle only penetrate as deep as the outer medulla.
Juxtamedullary:
Nephrons whose loops penetrate all the way into the inner medulla
Allow for ↑ concentration of the urine (due to ↑ osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation in the inner medulla)
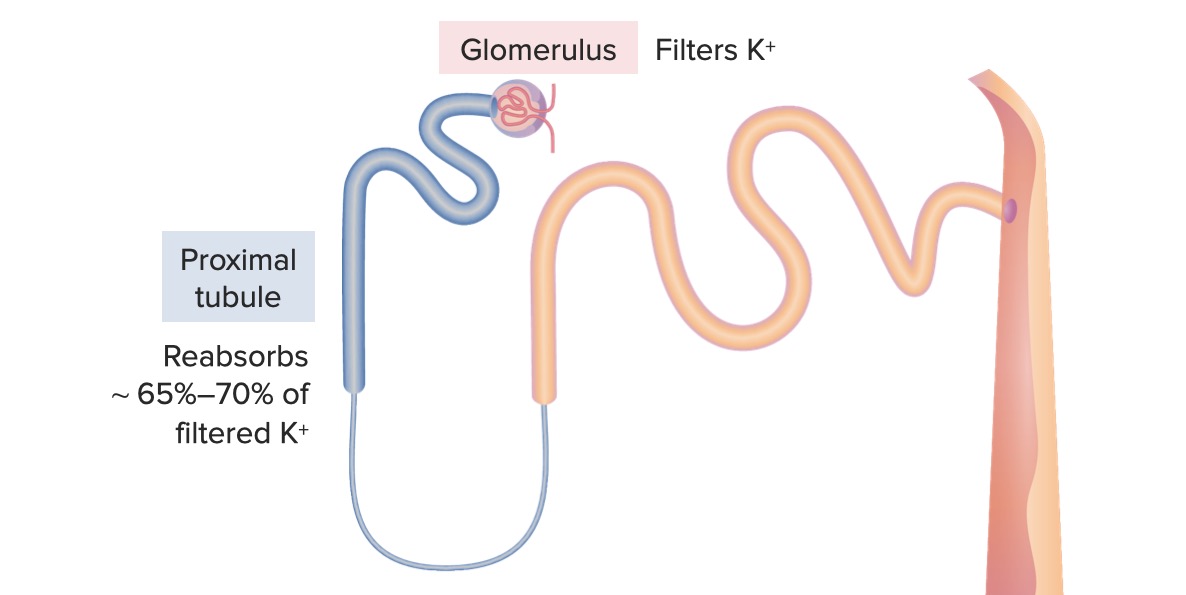
Proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System
Cells of the proximal convoluted tubuleProximal convoluted tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Osmotic Diuretics have the most absorptive capabilities in the entire nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy. All of the glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance, amino acidsAmino acidsOrganic compounds that generally contain an amino (-NH2) and a carboxyl (-COOH) group. Twenty alpha-amino acids are the subunits which are polymerized to form proteins.Basics of Amino Acids, and about 65% of Na+ and water are reabsorbed in the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System, in addition to a majority of the K+.
About 65%–70% of the filtered K+ is reabsorbed.
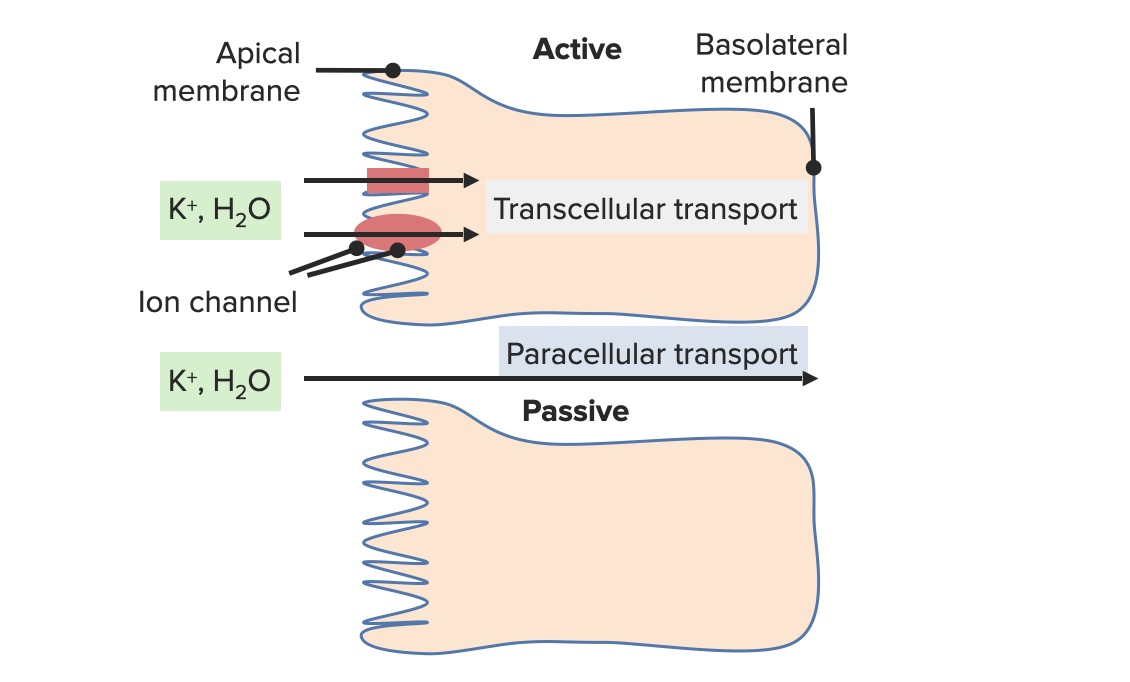
Reabsorption is paracellular (between cells) rather than transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System (which is an active process that requires energy).
Passive paracellular transport occurs via:
DiffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis
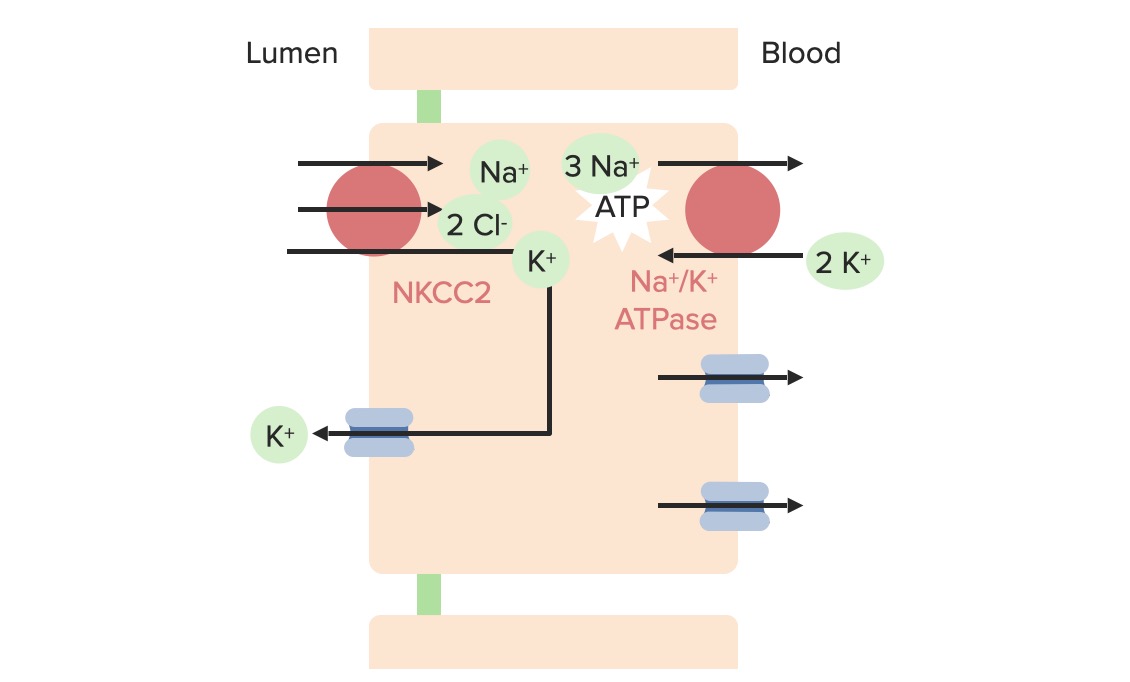
About 10%–25% of the filtered K+ is reabsorbed in the loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System. Reabsorption involves the following 2 transport proteinsTransport proteinsProteins and Peptides on the luminal side:
NKCC2 multiporter:
Active transportActive transportThe movement of materials across cell membranes and epithelial layers against an electrochemical gradient, requiring the expenditure of metabolic energy.The Cell: Cell Membrane (requires energy from basolateral Na+/K+ ATPase)
Transports the following into the cell from the tubule lumen:
1 Na+
1 K+
2 Cl–
Maintains electrical neutrality by moving 2 positively charged and 2 negatively charged ions together, all in the same direction
Loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication (furosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics, torsemideTorsemideA pyridine and sulfonamide derivative that acts as a sodium-potassium chloride symporter inhibitor. It is used for the treatment of edema associated with congestive heart failure; chronic renal insufficiency; and liver diseases. It is also used for the management of hypertension.Loop Diuretics, bumetanideBumetanideA sulfamyl diuretic.Loop Diuretics) inhibit NKCC2 → retains Na+, K+, and Cl– in the lumen.
ROMK (renal outer medullary potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia) channel:
Allows K+ to exit the cell into the tubular lumen
A regulated channel for passive transportPassive transportThe passive movement of molecules exceeding the rate expected by simple diffusion. No energy is expended in the process. It is achieved by the introduction of passively diffusing molecules to an environment or path that is more favorable to the movement of those molecules. Examples of facilitated diffusion are passive transport of hydrophilic substances across a lipid membrane through hydrophilic pores that traverse the membrane, and the sliding of a DNA binding protein along a strand of DNA.The Cell: Cell Membrane
Stimulated by low intracellular ATP: Na+/K+ ATPase has utilized ATP to bring K+ into the cell, which needs to be excreted.
Important for the recycling of K+ to allow NKCC2 to continue its function:
There is a much higher concentration of Na+ than K+ in the tubule lumen.
Recycling K+ into the tubule lumen allows NKCC2 to keep bringing more Na+ into the cells.
K+ movement at the thick ascending limb of the loop of Henle
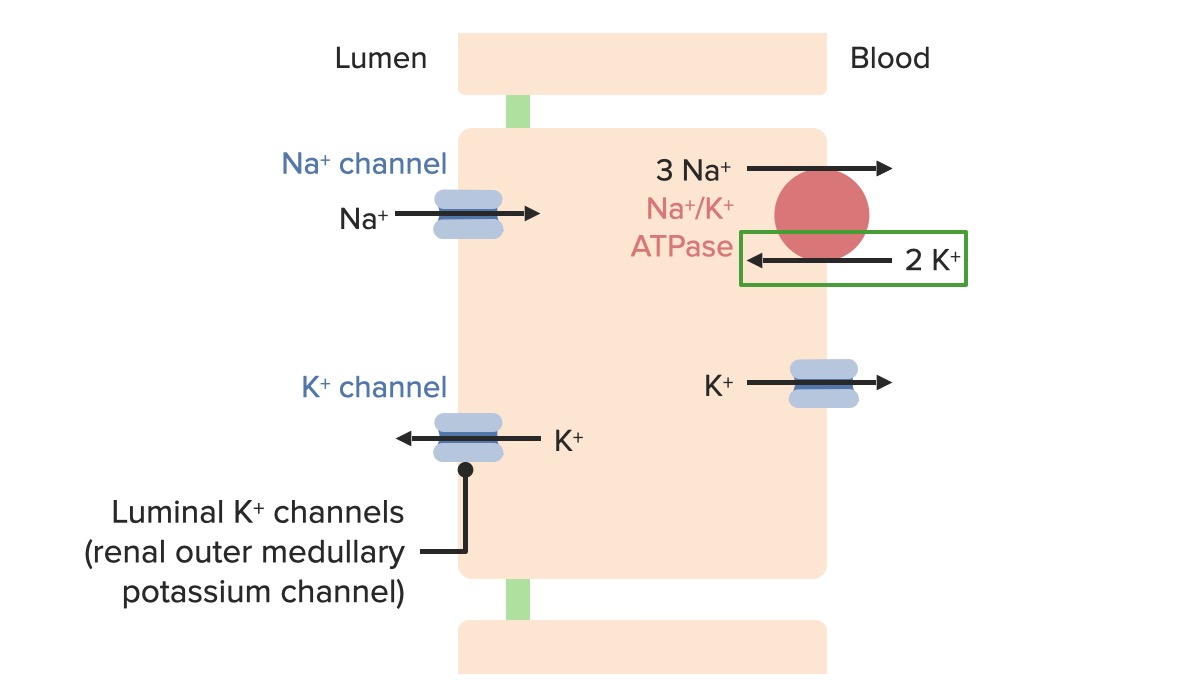
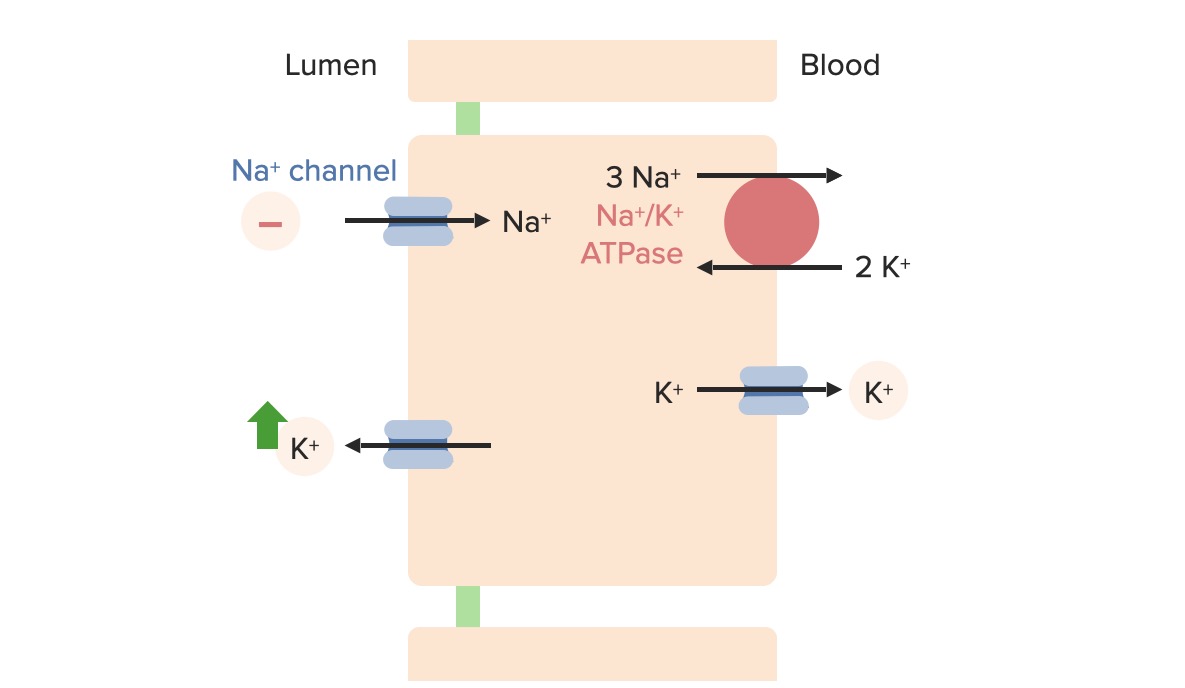
Although the largest amounts of K+ are reabsorbed in the proximal convoluted tubules, the primary sites of significant K+ regulation occur in the collecting ducts, within the principal and α-intercalated cells.
Na+/K+ATPase: 3 Na+ move out of the cell, 2 K+ move into the cell
Luminal side:
Epithelial sodium channelEpithelial sodium channelSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome (ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome): 1 Na+ moves into cell.
For each Na+ that moves into the cell, a Cl– is left behind in the tubular lumen.
Creates an electrical gradient where the luminal side is more negative
ROMK channel: A K+ moves out of the cell.
K+ moves into the principal cellsPrincipal cellsTubular System from the capillariesCapillariesCapillaries are the primary structures in the circulatory system that allow the exchange of gas, nutrients, and other materials between the blood and the extracellular fluid (ECF). Capillaries are the smallest of the blood vessels. Because a capillary diameter is so small, only 1 RBC may pass through at a time.Capillaries: Histology through the Na+/K+ATPase (active transportActive transportThe movement of materials across cell membranes and epithelial layers against an electrochemical gradient, requiring the expenditure of metabolic energy.The Cell: Cell Membrane) and out into the lumen through the ROMK channelsChannelsThe Cell: Cell Membrane (passive regulated transport).
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia exits into the lumen through the ROMK channelsChannelsThe Cell: Cell Membrane, which are controlled by factors that affect passive transportPassive transportThe passive movement of molecules exceeding the rate expected by simple diffusion. No energy is expended in the process. It is achieved by the introduction of passively diffusing molecules to an environment or path that is more favorable to the movement of those molecules. Examples of facilitated diffusion are passive transport of hydrophilic substances across a lipid membrane through hydrophilic pores that traverse the membrane, and the sliding of a DNA binding protein along a strand of DNA.The Cell: Cell Membrane:
DiffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis gradient:
↑ Intracellular K+ (K+ is primarily located in the ICFICFThe fluid inside cells.Body Fluid Compartments due to the Na+/K+ATPase)
↓ Luminal K+
Favors efflux of K+ into the lumen
Electrical gradient:
In the tubular lumen, every Na+ is accompanied by a Cl–.
When a Na ion moves through the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel, the accompanying chlorideChlorideInorganic compounds derived from hydrochloric acid that contain the Cl- ion.Electrolytes ion remains in the tubular lumen and generates the electrical gradient.
Increasingly negative luminal charge attracts K+.
↑ ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel activity→ ↑ electronegativity of tubular lumen→ ↑ affinity for K+ to move into tubular lumen through the ROMK channel
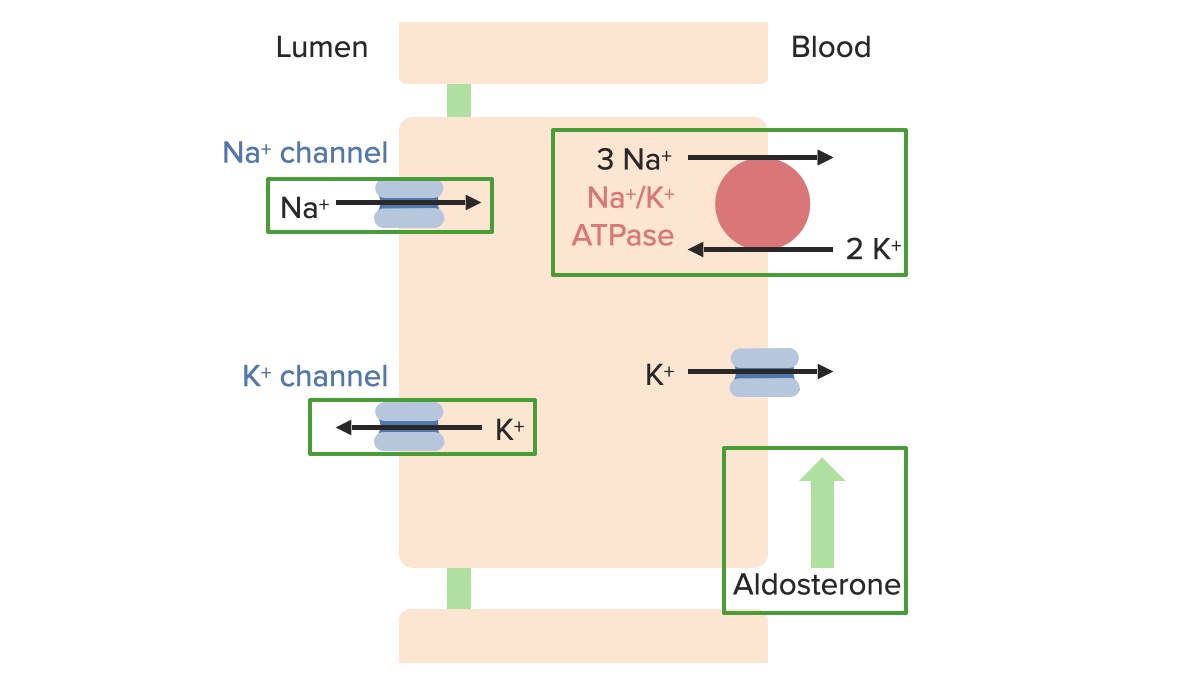
There are 4 primary factors that regulate K+ excretion at the level of the principal cellsPrincipal cellsTubular System:
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:
Stimulates basolateral Na+/K+ATPase to bring more K+ into the cells
ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle SyndromechannelsChannelsThe Cell: Cell Membrane AND
Increasing plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ concentration (same as aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia):
ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle SyndromechannelsChannelsThe Cell: Cell Membrane AND
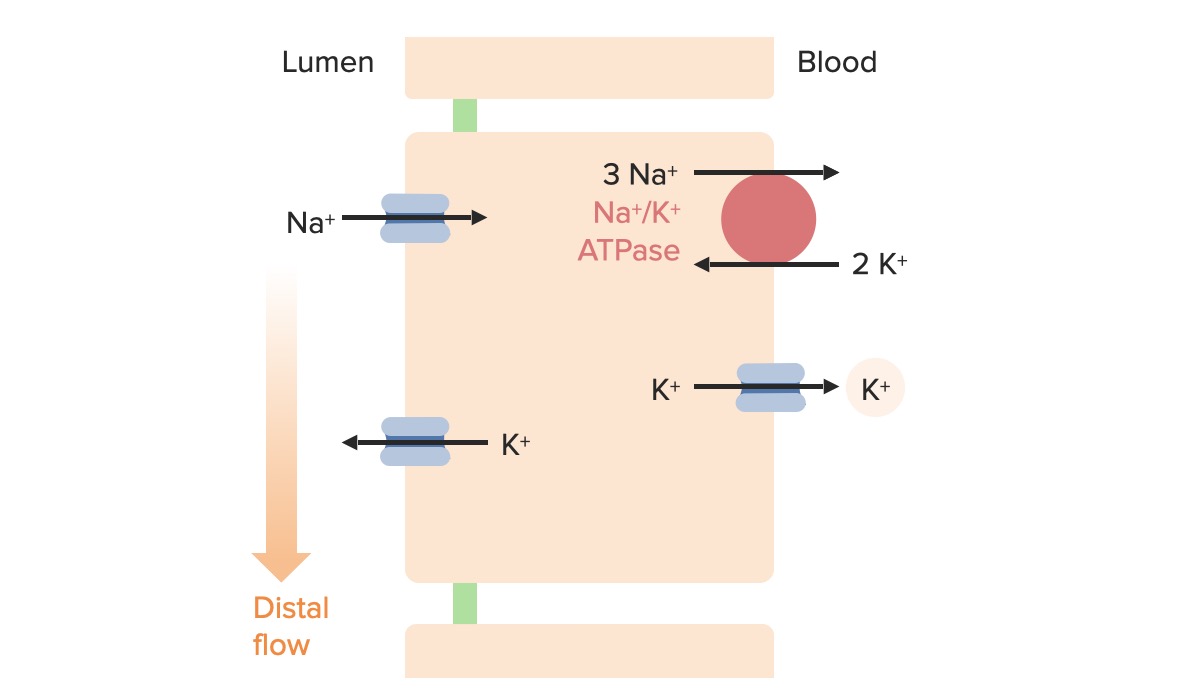
High flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure (e.g., polyuria):
K+ secreted by the ROMK channel is quickly moved to the next part of the nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy.
The concentration gradient favors diffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis of K+ into the tubular fluid.
End effect: ↑ urine flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure = ↑ K+ excretion (and ↓ serum K+)
Low flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure (e.g., oliguria):
There is less of a concentration gradient for the diffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis of K+ through the ROMK channel.
End effect: ↓ urine flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure = ↓ K+ excretion (and ↑ serum K+)
Distal Na+ delivery:
High distal Na+ delivery:
More Na+ is moving into the cell via the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel.
Less Na+ enters the cell via the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel.
Loop and thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication block the NKCC2 channelsChannelsThe Cell: Cell Membrane in the loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System:
Allow for ↑ Na+ delivery to the more distal collecting ducts
Represents the mechanism for hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia due to these diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication.
Effects of aldosterone and increasing plasma K+ concentration on regulatory transport proteins in the principal cells
Effects of tubular flow rate on K+ excretion: A faster flow rate moves the K+ away from the renal outer medullary potassium (ROMK) channels faster, maintaining a higher diffusion gradient. A slower flow rate keeps the K+ closer to the ROMK channels, decreasing the diffusion gradient, and decreasing K+ excretion.
Effects of distal sodium delivery on K+ excretion: As more Na+ is delivered to the principal cells in the collecting ducts, more Na is brought across the ENaC channels. This phenomenon increases the electronegative charge in the lumen, increasing the electrical gradient for K+ to flow into the lumen.
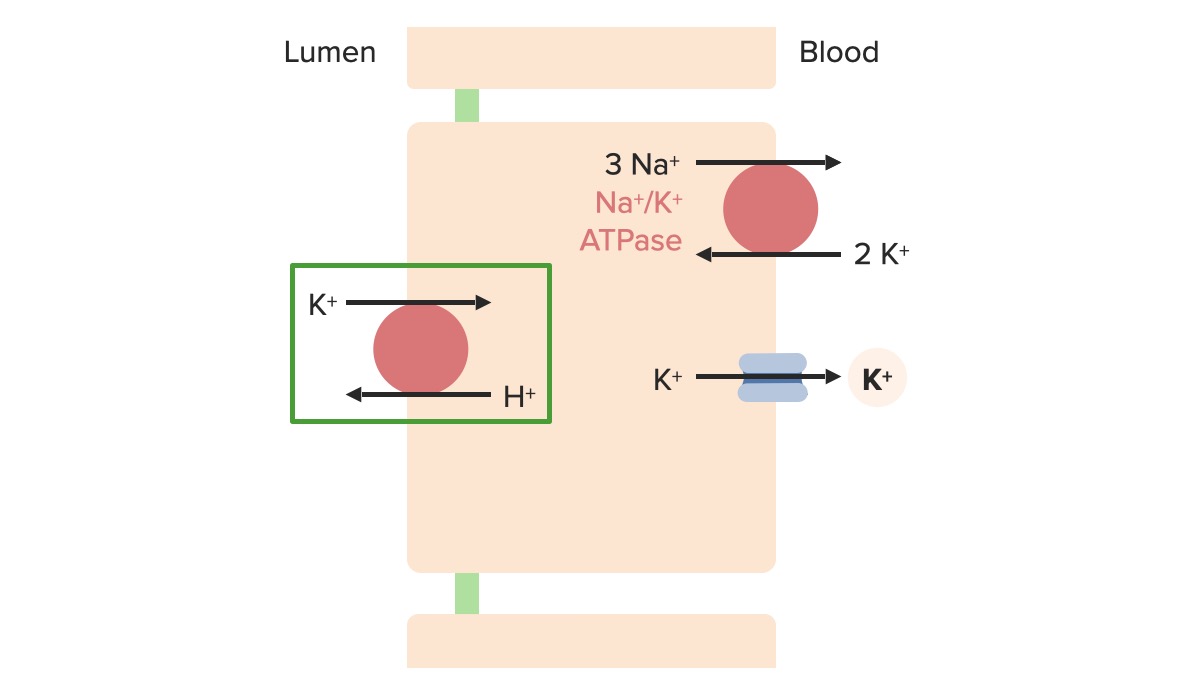
α-Intercalated cells allow for the fine-tuning of urinary K+ excretion.
Located in the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma
H+/K+ ATPase on the luminal side:
1 H+ out of the cell, 1 K+ into the cell
Active transportActive transportThe movement of materials across cell membranes and epithelial layers against an electrochemical gradient, requiring the expenditure of metabolic energy.The Cell: Cell Membrane protein (requires ATP for energy)
K+ conservation mechanism: enables urinary K+ excretion of < 15 mmol/day in hypokalemic states due to nonrenal losses
A normal Western diet contains approximately 40–120 mmol K+ per day. The normal response to ingested K+ occurs as follows:
Gut absorbs dietary K+ into the bloodstream.
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifts:
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia ions shift primarily into the muscle and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy cells.
Prevents excessive increases in ECF K+ concentration
Promoted by insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin and β2-adrenergic activity, which both ↑ the activity of Na+/K+ ATPase
Increased ECF K+ concentration triggers mechanisms for renal K+ excretion
↑ Number of open luminal ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome and ROMK channelsChannelsThe Cell: Cell Membrane
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia production is stimulated:
Further stimulates Na+/K+ ATPase
Further ↑ in luminal ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome and ROMK channelsChannelsThe Cell: Cell Membrane in principal cellsPrincipal cellsTubular System
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting into the muscle/liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy cells gradually reverses.
The remainder of the ingested K+ load is renally excreted.
Table: PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia content of selected foods
Food
Portion size
mmol K+
Avocado
1, medium
38
Sirloin steak
8 oz
23
Orange juice
8 oz
12
Potato, baked
7 oz
22
Raisins
⅔ cup
19
Tomato paste
½ cup
31
Banana
1, medium
12
Abnormalities
KidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy effectively regulate K+ excretion (especially at the α-intercalated cells).
Both hypo- and hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia due to decreased or increased intake is unlikely.
Exception: states of chronic malnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries (e.g., alcoholismAlcoholismA primary, chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be continuous or periodic.Wernicke Encephalopathy and Korsakoff Syndrome)
Clinical Relevance
Renal causes of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Several common causes of increased urinary losses of K+ leading to hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia include:
Diuretic use: DiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication can affect K+ levels in several ways. DiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication acting proximally to the collecting ducts, including loop and thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, increase distal Na+ delivery, which stimulates K+ excretion. Volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration as a result of the diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication can also activate the RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones, increasing aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies, which in turn increases K+ excretion.
A primary increase in mineralocorticoid activity: most often due to an aldosterone-producing adrenal adenomaAdrenal AdenomaCushing Syndrome or bilateral adrenal hyperplasiaBilateral Adrenal HyperplasiaHyperaldosteronism. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with increased mineralocorticoid activity usually have accompanying hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension.
Non-reabsorbable anionsAnionsNegatively charged atoms, radicals or groups of atoms which travel to the anode or positive pole during electrolysis.Electrolytes: The presence of non-reabsorbable anionsAnionsNegatively charged atoms, radicals or groups of atoms which travel to the anode or positive pole during electrolysis.Electrolytes in the lumen makes it more negative, increasing the amount of Na+ retained all the way into the collecting ducts. The increased distal delivery of Na+ and water then leads to an increased exchange of Na+ for K+ at the principal cellsPrincipal cellsTubular System, leading to hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia. Non-reabsorbable anionsAnionsNegatively charged atoms, radicals or groups of atoms which travel to the anode or positive pole during electrolysis.Electrolytes include bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes (increased with vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis), β-hydroxybutyrate (increased in ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis), and hippurate (increased with toluene use/glue sniffing).
Diabetic ketoacidosis: There are 3 different mechanisms that contribute to hypokalemia in diabetic ketoacidosis.
HypovolemiaHypovolemiaSepsis in Children induces hyperaldosteronismHyperaldosteronismHyperaldosteronism is defined as the increased secretion of aldosterone from the zona glomerulosa of the adrenal cortex. Hyperaldosteronism may be primary (resulting from autonomous secretion), or secondary (resulting from physiological secretion due to stimulation of the RAAS). Classically, hyperaldosteronism presents with hypertension, hypokalemia, and metabolic alkalosis.Hyperaldosteronism.
Production of the non-reabsorbable β-hydroxybutyrate anion is increased.
Less common causes: polyuria (due to psychogenic polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus)), renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis, hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes, use of amphotericin BAmphotericin BMacrolide antifungal antibiotic produced by streptomyces nodosus obtained from soil of the orinoco river region of venezuela.Polyenes, and low-calorie diets. Mutations in tubular-transport proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis, including Liddle’s syndrome, Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome, and Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome, can cause or contribute to hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
Renal causes of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Several common causes of reduced urinary losses of K+ leading to hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia include:
Reduced aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies: Any condition that reduces aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies will reduce K+ excretion. Causes of reduced aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies may include both hyporeninemic hypoaldosteronismHyporeninemic hypoaldosteronismReduced aldosterone synthesis due to decreased stimulation of Renin-angiotensin-aldosterone system.Hypoaldosteronism (situations of volume overload, diabetic nephropathyDiabetic nephropathyKidney injuries associated with diabetes mellitus and affecting kidney glomerulus; arterioles; kidney tubules; and the interstitium. Clinical signs include persistent proteinuria, from microalbuminuria progressing to albuminuria of greater than 300 mg/24 h, leading to reduced glomerular filtration rate and end-stage renal disease.Chronic Diabetic Complications, autonomic neuropathyNeuropathyLeprosy, and some systemic diseases) and hyperreninemic hypoaldosteronismHyperreninemic hypoaldosteronismReduced aldosterone synthesis due to direct adrenal issues.Hypoaldosteronism (including primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease, chronic heparin use, and several congenitalCongenitalChorioretinitis anomalies). Several drugs can also be causative, including ACE inhibitorsACE inhibitorsTruncus Arteriosus, NSAIDsNSAIDSPrimary vs Secondary Headaches, calcineurin inhibitorsCalcineurin InhibitorsCompounds that inhibit or block the phosphatase activity of calcineurin.Immunosuppressants, and heparin.
Reduced response to aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia: caused by potassium-sparing diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication like aldosterone antagonistsAldosterone antagonistsDrugs that bind to and block the activation of mineralocorticoid receptors by mineralocorticoids such as aldosterone.Heart Failure and Chronic Coronary Syndrome Medication (e.g., spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics, eplerenoneEplerenoneA spironolactone derivative and selective aldosterone receptor antagonist that is used in the management of hypertension and congestive heart failure, post-myocardial infarction.Potassium-sparing Diuretics) and ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome antagonists (e.g., amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome and triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics); voltage-dependent renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (due to impaired sodium reabsorptionSodium reabsorptionTubular System in the principal cellsPrincipal cellsTubular System); and pseudohypoaldosteronismPseudohypoaldosteronismA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism (a rare genetic disorder causing aldosterone resistanceAldosterone resistanceA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism).
Reduced distal Na+ and water delivery: results from effective arterial blood-volume depletion, including GI and renal losses, heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), and cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis. When distal delivery of Na and water decreases, less Na+ is reabsorbed in exchange for K+; therefore, less K+ is excreted.
Acute and CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease: As the number of functioning nephrons decreases, the ability of the kidney to excrete K+ decreases. PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia excretion is typically maintained as long as the patient is able to respond to aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia, and the delivery of Na+ and water is maintained. HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia tends to occur in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are oliguric or have additional problems that may contribute to hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.