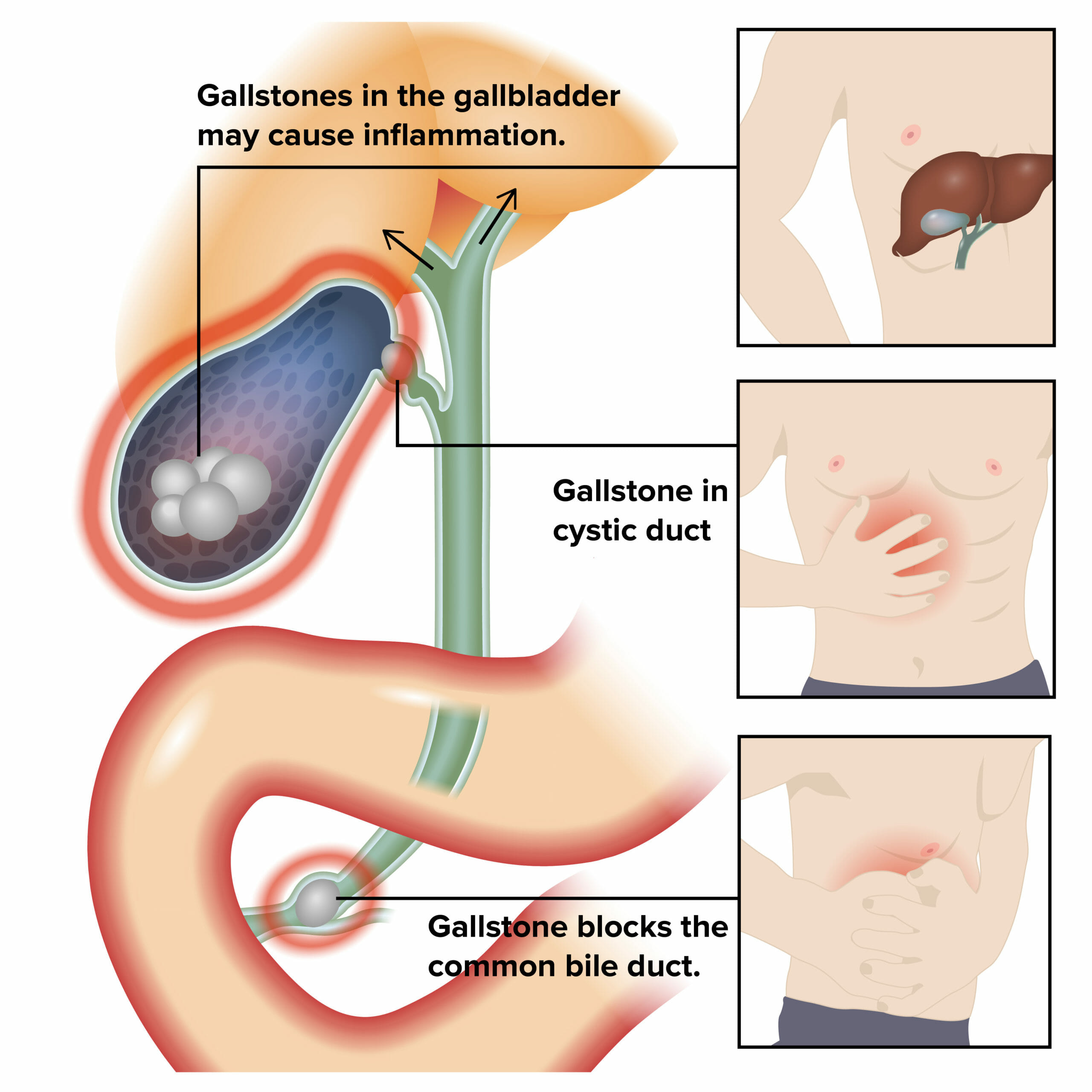
Cholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis (calculous cholecystitis) but inflammation without gallstones (acalculous cholecystitis) can occur in a minority of patients. The acute type usually presents with right upper quadrant (RUQ) pain, fever, and leukocytosis. The diagnosis is made clinically and confirmed via ultrasound (US). The definitive management is cholecystectomy, preferably performed within 72 hours. This condition can present as a mild condition or as a severe disease (with complications such as gallbladder gangrene, perforation, empyema) which require emergent intervention.
CholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis is the inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy (GB). Types:
Calculous cholecystitisCalculous CholecystitisCholecystitis: GB inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation as a complication of gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis or cholelithiasisCholelithiasisCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant). Cholelithiasis
Acute:cysticCysticFibrocystic Change duct obstruction/GB inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of sudden onset, associated with intense painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Chronic: chronic inflammationChronic InflammationInflammation and fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans of the GB, associated with:
Less painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways intensity
Mechanical irritation from gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
Recurrent attacks of acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis
Acalculous cholecystitisAcalculous cholecystitisInflammation of the gallbladder wall in the absence of gallstones.Cholecystitis: GB inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation due to GB stasis and ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
GallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis are absent.
Usually in critically ill and/or immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Epidemiology[1,3]
Women > men
Peak incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 40–50 years
Develops in 6%–11% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with symptomatic gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
Risk factors:
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care or hormone therapy
Older age
Native American or Hispanic
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity; rapid weight gain/loss
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Etiology and Pathophysiology
Etiology: most commonly due to obstructing gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis in the GB, causing symptoms[8]
Obstruction leads to distention and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy.
Other contributing factors to GB inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation:
ProstaglandinsProstaglandinsA group of compounds derived from unsaturated 20-carbon fatty acids, primarily arachidonic acid, via the cyclooxygenase pathway. They are extremely potent mediators of a diverse group of physiological processes.Eicosanoids (↑ GB contraction)
LysolecithinLysolecithinDerivatives of phosphatidylcholines obtained by their partial hydrolysis which removes one of the fatty acid moieties.Cholecystitis, an inflammatory mediator which is normally absent in bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy, but is produced in cases of GB wall trauma
May or may not be associated with bacterial infection (Escherichia coliEscherichia coliThe gram-negative bacterium Escherichia coli is a key component of the human gut microbiota. Most strains of E. coli are avirulent, but occasionally they escape the GI tract, infecting the urinary tract and other sites. Less common strains of E. coli are able to cause disease within the GI tract, most commonly presenting as abdominal pain and diarrhea. Escherichia coli,EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus, KlebsiellaKlebsiellaKlebsiella are encapsulated gram-negative, lactose-fermenting bacilli. They form pink colonies on MacConkey agar due to lactose fermentation. The main virulence factor is a polysaccharide capsule. Klebsiella pneumoniae is the most important pathogenic species.Klebsiella, EnterobacterEnterobacterMultidrug-resistant Organisms and Nosocomial Infections)
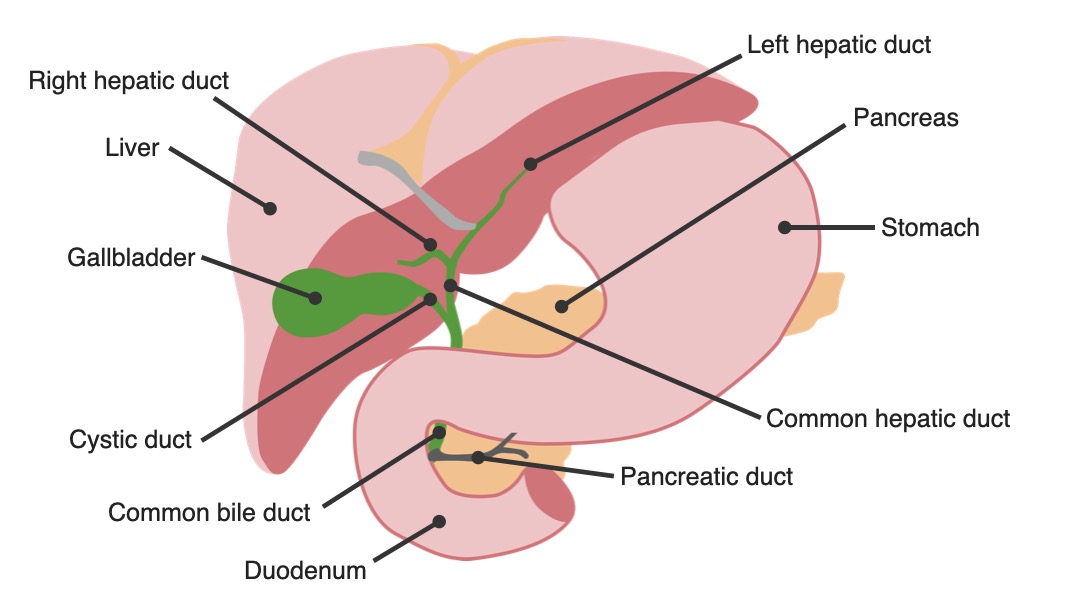
Anatomy of the biliary tree: gallbladder in relation to other organs
Image by Lecturio.
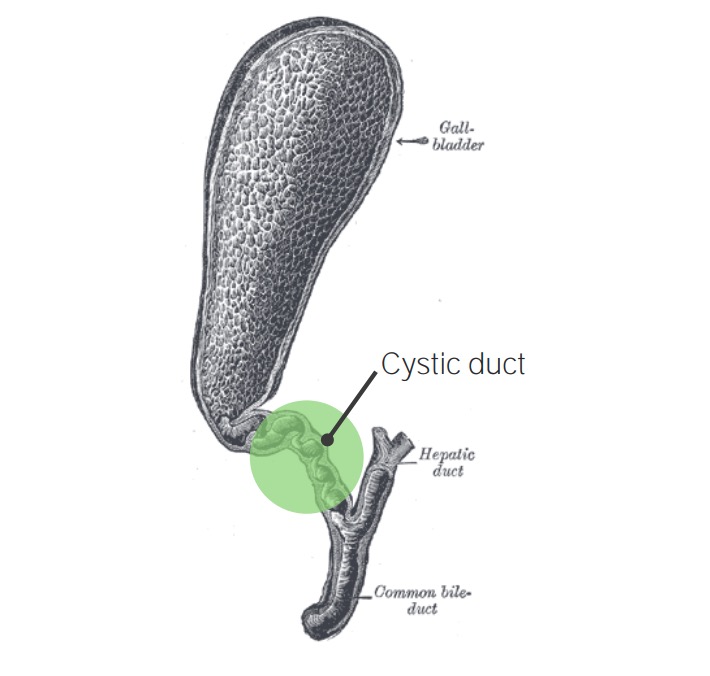
Gallbladder with cholecystitis: cystic duct obstruction
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma to the right scapula
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
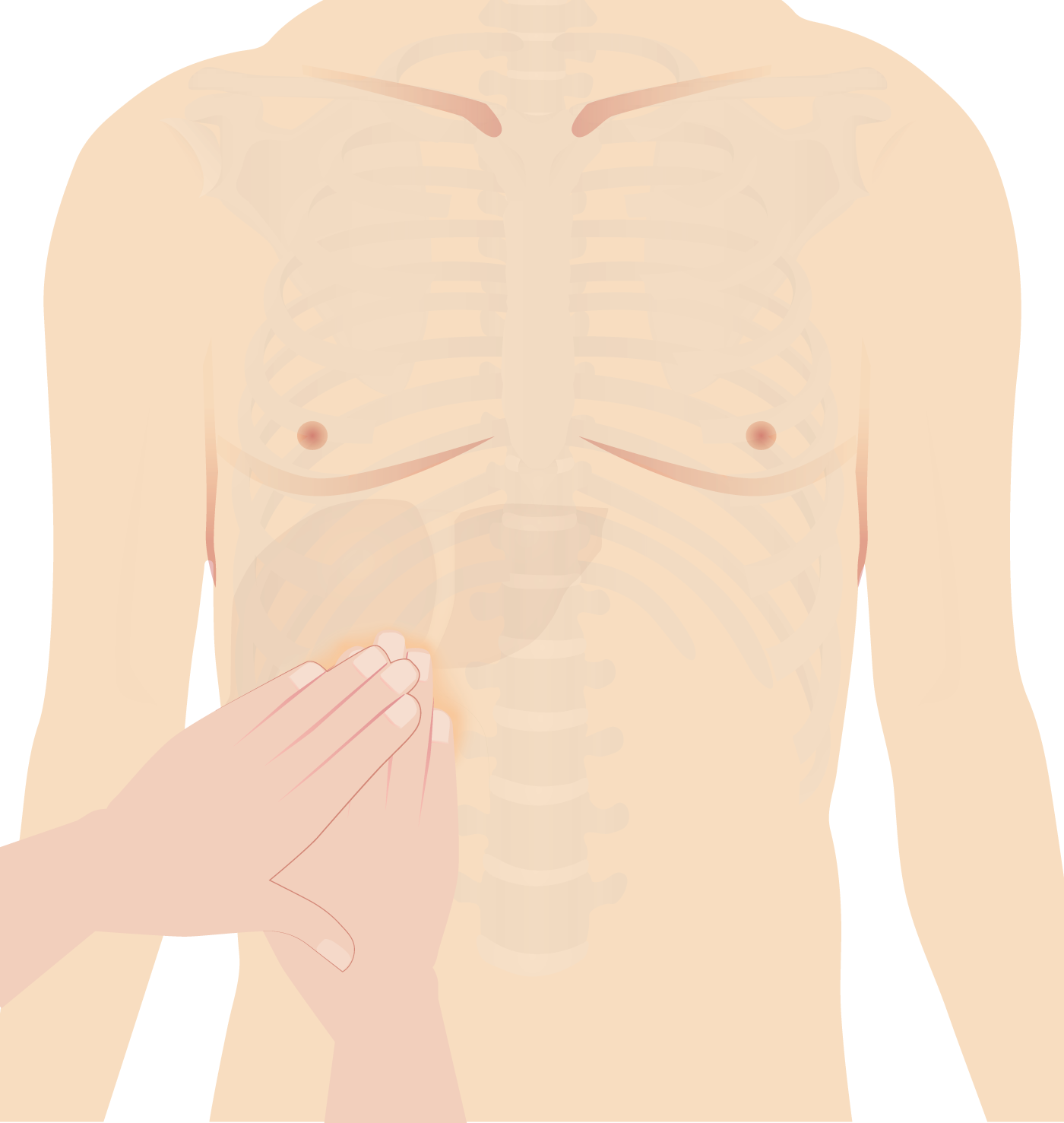
Boas’s sign is hyperesthesia below the right scapula (noted in acute cholecystitis).
Inflamed GB descends and comes in contact with the examiner’s handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy, causing painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways/discomfort.
Abdominal guardingAbdominal GuardingAcute Abdomen, rebound: local peritoneal inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Murphy’s sign: Examiner places hand on the gallbladder area (right subcostal area). Patient is instructed to take a deep breath. On inspiration, the inflamed gallbladder descends, coming in contact with the examiner’s hand and causing pain.
Image by Lecturio.
Diagnosis
Diagnosing acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis requires a combination of clinical, laboratory, and imaging studies.
Physical examination[5,7,8]
Tenderness to palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination in RUQ/epigastric area
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Laboratory tests[5,7,8]
Liver function testsLiver function testsLiver function tests, also known as hepatic function panels, are one of the most commonly performed screening blood tests. Such tests are also used to detect, evaluate, and monitor acute and chronic liver diseases.Liver Function Tests (LFTs):
BilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism and alkaline phosphataseAlkaline PhosphataseAn enzyme that catalyzes the conversion of an orthophosphoric monoester and water to an alcohol and orthophosphate.Osteosarcoma: normal in uncomplicated cases
Elevation of bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism and alkaline phosphataseAlkaline PhosphataseAn enzyme that catalyzes the conversion of an orthophosphoric monoester and water to an alcohol and orthophosphate.Osteosarcoma should raise suspicion for complications (e.g., cholangitis, choledocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis)
Mild elevation of alanineAlanineA non-essential amino acid that occurs in high levels in its free state in plasma. It is produced from pyruvate by transamination. It is involved in sugar and acid metabolism, increases immunity, and provides energy for muscle tissue, brain, and the central nervous system.Synthesis of Nonessential Amino Acids aminotransferase (ALTALTAn enzyme that catalyzes the conversion of l-alanine and 2-oxoglutarate to pyruvate and l-glutamate.Liver Function Tests) and aspartateAspartateOne of the non-essential amino acids commonly occurring in the l-form. It is found in animals and plants, especially in sugar cane and sugar beets. It may be a neurotransmitter.Synthesis of Nonessential Amino Acids aminotransferase (ASTASTEnzymes of the transferase class that catalyze the conversion of l-aspartate and 2-ketoglutarate to oxaloacetate and l-glutamate.Liver Function Tests)
Renal function and electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption, lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion (may be elevated)
C-reactive protein (CRP)
Coagulation studiesCoagulation studiesCoagulation studies are a group of hematologic laboratory studies that reflect the function of blood vessels, platelets, and coagulation factors, which all interact with one another to achieve hemostasis. Coagulation studies are usually ordered to evaluate patients with bleeding or hypercoagulation disorders.Coagulation Studies (INR)
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test in women
Imaging[5,7,8]
Ultrasound (US): test of choice (84% sensitivity, 99% specificity for the diagnosis of gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis)[8]
GB wall thickening > 4 mm
GB wall edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema (double-wall sign)
Presence of gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
GB enlargement > 8 cm in the long axis and > 4 cm in the short axis
Air in the GB wall (indicative of gangreneGangreneDeath and putrefaction of tissue usually due to a loss of blood supply.Small Bowel Obstruction)
Intravenous injection of radioactive tracer that gets excreted in the bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy by hepatocytesHepatocytesThe main structural component of the liver. They are specialized epithelial cells that are organized into interconnected plates called lobules.Liver: Anatomy
If the cysticCysticFibrocystic Change duct is not obstructed, the tracer will be seen in the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy.
Abnormal if gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy not visualized within 30–60 minutes[5]
Delayed imaging (taken after 3–4 hours) and/or morphineMorphineThe principal alkaloid in opium and the prototype opiate analgesic and narcotic. Morphine has widespread effects in the central nervous system and on smooth muscle.Opioid Analgesics augmentation can be performed.
Nonvisualization of the GB on delayed imaging or 30 minutes after morphineMorphineThe principal alkaloid in opium and the prototype opiate analgesic and narcotic. Morphine has widespread effects in the central nervous system and on smooth muscle.Opioid Analgesics augmentation indicates cysticCysticFibrocystic Change duct obstruction.[3]
False positiveFalse positiveAn FP test result indicates that a person has the disease when they do not.Epidemiological Values of Diagnostic Tests (cysticCysticFibrocystic Change duct obstruction without cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis) seen in:[1,3]
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Fasting states (no stimulus for GB contraction)
↑ BilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism (4.4 mg/dL)
Not a 1st-choice test for suspected cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, as most gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis will not be visualized on CT (20% missed)[1]
Will show GB inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Provides information about surrounding structures and additional complications
Used if patient presents with peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury, bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis, or sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Magnetic resonance cholangiopancreatographyMagnetic resonance cholangiopancreatographyNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis (MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis):[7,9]
Indication: choledocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis is suspected
US did not show common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct stones, but the bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct is dilated on US and/or LFTs are abnormal[9]
MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis is sensitive in detecting stones in the cysticCysticFibrocystic Change duct, but has lower sensitivity (than US) in detecting GB wall edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema.
Abdominal MRI:[5]
An alternative if CT is contraindicated
Findings: enlarged GB, thickened GB wall, pericholecystic high signal
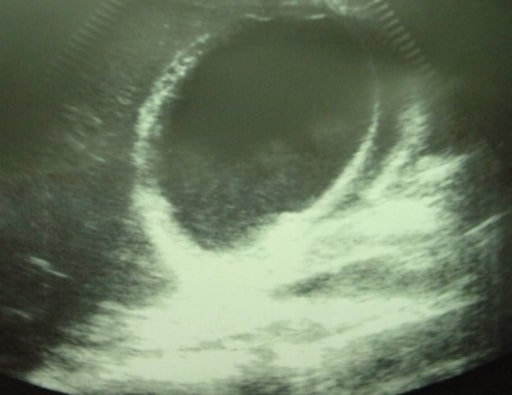
Ultrasound of a patient with acute cholecystitis: A very large gallstone with significant surrounding edema can be seen.
Image: “Ultrasound of a patient with acute cholecystitis” by Department of Emergency Medicine, University of Maryland School of Medicine, 110 South Paca Street, 6th Floor, Suite 200, Baltimore 21201, MD, USA. License: CC BY 4.0
Acute cholecystitis showing pericholecystic fluid
Image: “Ultrasonographic image of the gallbladder” by Department of Surgery, University Hospital Hassan II, Morocco. License: CC BY 2.0
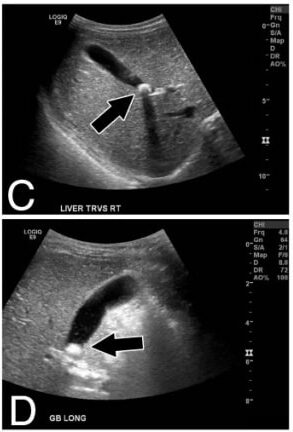
Panels C, D: Transverse and longitudinal ultrasound views of liver and gallbladder (arrows indicate the gallstone)
Image: “Calcified gallstone” by Division of Pediatric Surgery, Children’s Hospital Los Angeles, 4650 Sunset Blvd Mailstop 100, Los Angeles, CA 90027, USA. License: CC BY 2.0
Diagnostic criteria for acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis[5]
The Tokyo Guidelines proposed the following criteria to diagnose acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis. Diagnosis requires 1 item from A and 1 item from B, while positive imaging findings (C) confirm the diagnosis when it is suspected clinically.
Local signs of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation:
RUQ tenderness/massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Systemic signs of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Imaging findings characteristic of acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis
Assess severity[4,5,8]
Assess severity at the time of diagnosis and repeat evaluation by 24 and 48 hours after diagnosis.[4]
Several stratification systems are available; for Tokyo guidelines 2018 (calculator), see table below.[5]
Because not all patient variables are included in scoring systems, clinical judgmentJudgmentThe process of discovering or asserting an objective or intrinsic relation between two objects or concepts; a faculty or power that enables a person to make judgments; the process of bringing to light and asserting the implicit meaning of a concept; a critical evaluation of a person or situation.Psychiatric Assessment is important and the use of scoring is for guidance.[8]
Table: Severity assessment of acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis (Tokyo guidelines)[5]
Category
Description
Findings
Clinical impact
Grade I
Mild
Limited disease in the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
No organ dysfunction
Does not meet criteria for grade II or III
Performing cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy is low risk.
Grade II
Moderate
Any 1 of the following in the setting of no organ dysfunction:
Extensive disease in the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy (pericholecystic abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, gangrenous cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, emphysematous cholecystitisEmphysematous cholecystitisA variant of acute cholecystitis with inflammation of the gallbladder that is characterized by the pockets of gas in the gallbladder wall. It is due to secondary infection caused by gas-forming organisms, and has a high risk of perforation.Cholecystectomy, biliary peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury, hepatic abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease)
Illness is > 72 hours.
Tender RUQ palpable massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
WBC > 18,000/mm3
Performing cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy is expected to be more difficult.
Surgery may not be favorable in the acute phaseAcute phaseShort Bowel Syndrome.
Grade III
Severe
With organ dysfunction (includes any 1 of the following):
Cardiovascular dysfunction (hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension: requires dopamineDopamineOne of the catecholamine neurotransmitters in the brain. It is derived from tyrosine and is the precursor to norepinephrine and epinephrine. Dopamine is a major transmitter in the extrapyramidal system of the brain, and important in regulating movement.Receptors and Neurotransmitters of the CNS ≥ 5 µg/kg/min, or norepinephrineNorepinephrinePrecursor of epinephrine that is secreted by the adrenal medulla and is a widespread central and autonomic neurotransmitter. Norepinephrine is the principal transmitter of most postganglionic sympathetic fibers, and of the diffuse projection system in the brain that arises from the locus ceruleus.Receptors and Neurotransmitters of the CNS (any dose))
Renal dysfunction (oliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation, creatinine >2.0 mg/dL)
Respiratory dysfunction (partial pressurePartial pressureThe pressure that would be exerted by one component of a mixture of gases if it were present alone in a container.Gas Exchange of oxygen (PaO2)/fraction of inspired oxygen (FiO2FiO2percentage of oxygen delivered directly to the patientInvasive Mechanical Ventilation) ratio < 300)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require intensive care and urgent treatment (either surgery or biliary drainage)
Management
Management guidelines may vary depending on practice location. The following information is based on literature and guidelines from the US, UK, and Japan.
CholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy is the treatment of choice, but other nonsurgical therapy can be used initially for poor surgical candidates.
Supportive therapy[4,6,8]
AnalgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts: nonsteroidal anti-inflammatory drugs (NSAIDsNSAIDSPrimary vs Secondary Headaches) (preferable), opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics
Ketorolac (NSAIDNSAIDNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs)): IV 15–30 mg every 6 hours as needed
MorphineMorphineThe principal alkaloid in opium and the prototype opiate analgesic and narcotic. Morphine has widespread effects in the central nervous system and on smooth muscle.Opioid Analgesics, hydromorphoneHydromorphoneAn opioid analgesic made from morphine and used mainly as an analgesic. It has a shorter duration of action than morphine.Opioid Analgesics, or meperidine (opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics used if NSAIDNSAIDNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs) is inadequate or contraindicated)
AntiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics
Nothing by mouth
Start antibiotics[4]
Antimicrobial management[4,6,11]
General insights:
Intravenous antibiotics:[4]
Adjunctive therapy
Can be used as primary treatment if surgery is contraindicated (in high-risk patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Cultures:[4,6]
Blood cultures:
Benefit not fully studied in trials; recommendation is to not routinely order them for community-acquired infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (especially in grade I acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis).[6]
Help in microorganism identificationIdentificationDefense Mechanisms and susceptibility when there is antimicrobial resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing
BileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy culture:
Obtain specimen for severity grades II and III[4]
BileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy and tissue cultures are sent if there is perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, or emphysematous changes.
Administer antibiotics:
Preferably within 1 hour if patient has a septic presentation
Within 6 hours after diagnosis is made
Goals:
LimitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical VentilationinflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Reduce systemic septic response
Prevent abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease formation
Antibiotic coverage:[4–6,11]
Should cover EnterobacteriaceaeEnterobacteriaceaeA family of gram-negative, facultatively anaerobic, rod-shaped bacteria that do not form endospores. Its organisms are distributed worldwide with some being saprophytes and others being plant and animal parasites. Many species are of considerable economic importance due to their pathogenic effects on agriculture and livestock.Cephalosporins and common gram-positiveGram-PositivePenicillins organisms; most common isolates include:[4]
E. coli
KlebsiellaKlebsiellaKlebsiella are encapsulated gram-negative, lactose-fermenting bacilli. They form pink colonies on MacConkey agar due to lactose fermentation. The main virulence factor is a polysaccharide capsule. Klebsiella pneumoniae is the most important pathogenic species.Klebsiella spp.
PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas spp.
EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus spp.
StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus spp.
Additional considerations:
Antibiotics with anti-PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas coverage is needed in those with grade III community-acquired acute cholangitisAcute CholangitisAcute cholangitis is a life-threatening condition characterized by fever, jaundice, and abdominal pain which develops as a result of stasis and infection of the biliary tract. Septic shock, liver abscess, and multi-organ dysfunction are potential serious complications. Acute Cholangitis and cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis until identificationIdentificationDefense Mechanisms of causative organism/s.
Anaerobic coverage needed if there is an associated distal small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy or colon-related infection (e.g., biliary-enteric anastomosis)
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides is not recommended due to increased resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing.
VancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides should be added to cover EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with grade III disease.[11]
The Infectious Diseases Society of America recommends against routine use of anti–methicillin-resistant Staphylococcus aureusStaphylococcus aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Brain Abscess(MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus) coverage unless there is evidence of MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus.
Broad-spectrumBroad-SpectrumFluoroquinolones antibiotics should be adjusted when susceptibility results become available.
Antibiotic regimens:
Single-agent regimen:[6,11]
AmpicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins–sulbactamSulbactamA beta-lactamase inhibitor with very weak antibacterial action. The compound prevents antibiotic destruction of beta-lactam antibiotics by inhibiting beta-lactamases, thus extending their spectrum activity. Combinations of sulbactam with beta-lactam antibiotics have been used successfully for the therapy of infections caused by organisms resistant to the antibiotic alone.Cephalosporins (only if resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing is < 20%): 1.5–3 g IV every 6 hours
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins: 3.375 or 4.5 g IV every 6 hours
Cefoxitin 2 g IV every 6 hours
MoxifloxacinMoxifloxacinA fluoroquinolone that acts as an inhibitor of DNA topoisomerase II and is used as a broad-spectrum antibacterial agent.Fluoroquinolones: 400 mg IV every 24 hours
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam: 1 g IV every 24 hours
ImipenemImipenemSemisynthetic thienamycin that has a wide spectrum of antibacterial activity against gram-negative and gram-positive aerobic and anaerobic bacteria, including many multiresistant strains. It is stable to beta-lactamases. Clinical studies have demonstrated high efficacy in the treatment of infections of various body systems. Its effectiveness is enhanced when it is administered in combination with cilastatin, a renal dipeptidase inhibitor.Carbapenems and Aztreonam–cilastatinCilastatinA renal dehydropeptidase-i and leukotriene d4 dipeptidase inhibitor. Since the antibiotic, imipenem, is hydrolyzed by dehydropeptidase-i, which resides in the brush border of the renal tubule, cilastatin is administered with imipenem to increase its effectiveness. The drug also inhibits the metabolism of leukotriene d4 to leukotriene e4.Carbapenems and Aztreonam: 500 mg IV every 6 hours or 1 g IV every 8 hours
MeropenemMeropenemA thienamycin derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of bacterial infections, including infections in immunocompromised patients.Carbapenems and Aztreonam: 1 g IV every 8 hours
DoripenemDoripenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of infections such as hospital-acquired pneumonia, and complicated intra-abdominal or urinary-tract infections, including pyelonephritis.Carbapenems and Aztreonam 500 mg IV every 8 hours
Double-agent regimen (combined with metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess 500 mg every 8 hours, which is warranted in biliary-enteric anastomosis):[6,11]
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins 1–2 g IV every 8 hours
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins 1–2 g IV every 12–24 hours
Cefuroxime 1.5 g IV every 8 hours
CefotaximeCefotaximeSemisynthetic broad-spectrum cephalosporin.Cephalosporins 1–2 g IV every 6–8 hours
CefepimeCefepimeA fourth-generation cephalosporin antibacterial agent that is used in the treatment of infections, including those of the abdomen, urinary tract, respiratory tract, and skin. It is effective against pseudomonas aeruginosa and may also be used in the empiric treatment of febrile neutropenia.Cephalosporins 2 g every 8–12 hours
CeftazidimeCeftazidimeSemisynthetic, broad-spectrum antibacterial derived from cephaloridine and used especially for pseudomonas and other gram-negative infections in debilitated patients.Cephalosporins 2 g every 8 hours
CiprofloxacinCiprofloxacinA broad-spectrum antimicrobial carboxyfluoroquinoline.Fluoroquinolones 400 mg every 12 hours
AztreonamAztreonamThe carbapenems and aztreonam are both members of the bactericidal beta-lactam family of antibiotics (similar to penicillins). They work by preventing bacteria from producing their cell wall, ultimately leading to bacterial cell death. Carbapenems and Aztreonam 1–2 g every 6–8 hours
Table: Antibiotic regimens in cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis[11]
Grade
Grade I
Grade II
Grade III or health care–associated infection
Single agents
AmpicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins–sulbactamSulbactamA beta-lactamase inhibitor with very weak antibacterial action. The compound prevents antibiotic destruction of beta-lactam antibiotics by inhibiting beta-lactamases, thus extending their spectrum activity. Combinations of sulbactam with beta-lactam antibiotics have been used successfully for the therapy of infections caused by organisms resistant to the antibiotic alone.Cephalosporinsa
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam
Cefoxitin
MoxifloxacinMoxifloxacinA fluoroquinolone that acts as an inhibitor of DNA topoisomerase II and is used as a broad-spectrum antibacterial agent.Fluoroquinolones
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam
MoxifloxacinMoxifloxacinA fluoroquinolone that acts as an inhibitor of DNA topoisomerase II and is used as a broad-spectrum antibacterial agent.Fluoroquinolones
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam
ImipenemImipenemSemisynthetic thienamycin that has a wide spectrum of antibacterial activity against gram-negative and gram-positive aerobic and anaerobic bacteria, including many multiresistant strains. It is stable to beta-lactamases. Clinical studies have demonstrated high efficacy in the treatment of infections of various body systems. Its effectiveness is enhanced when it is administered in combination with cilastatin, a renal dipeptidase inhibitor.Carbapenems and Aztreonam–cilastatinCilastatinA renal dehydropeptidase-i and leukotriene d4 dipeptidase inhibitor. Since the antibiotic, imipenem, is hydrolyzed by dehydropeptidase-i, which resides in the brush border of the renal tubule, cilastatin is administered with imipenem to increase its effectiveness. The drug also inhibits the metabolism of leukotriene d4 to leukotriene e4.Carbapenems and Aztreonam
MeropenemMeropenemA thienamycin derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of bacterial infections, including infections in immunocompromised patients.Carbapenems and Aztreonam
Agents that may be used alone OR in combination with metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscessb
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins
Cefuroxime
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins
CefepimeCefepimeA fourth-generation cephalosporin antibacterial agent that is used in the treatment of infections, including those of the abdomen, urinary tract, respiratory tract, and skin. It is effective against pseudomonas aeruginosa and may also be used in the empiric treatment of febrile neutropenia.Cephalosporins
CeftazidimeCeftazidimeSemisynthetic, broad-spectrum antibacterial derived from cephaloridine and used especially for pseudomonas and other gram-negative infections in debilitated patients.Cephalosporins
CefepimeCefepimeA fourth-generation cephalosporin antibacterial agent that is used in the treatment of infections, including those of the abdomen, urinary tract, respiratory tract, and skin. It is effective against pseudomonas aeruginosa and may also be used in the empiric treatment of febrile neutropenia.Cephalosporins
CeftazidimeCeftazidimeSemisynthetic, broad-spectrum antibacterial derived from cephaloridine and used especially for pseudomonas and other gram-negative infections in debilitated patients.Cephalosporins
Cefozopran
AztreonamAztreonamThe carbapenems and aztreonam are both members of the bactericidal beta-lactam family of antibiotics (similar to penicillins). They work by preventing bacteria from producing their cell wall, ultimately leading to bacterial cell death. Carbapenems and Aztreonam
a Only if resistance is < 20% b Most mild-to-moderate uncomplicated biliary infections do not require metronidazole. Both the Tokyo guidelines[11] and the Infectious Diseases Society of America[6] recommend anaerobic coverage in biliary-enteric anastomosis. Another anti-anaerobic therapy option is clindamycin (though resistance in Bacteroides spp. is significant).
Duration of antibiotics:[11]
Switch to oral antibiotics when patient is able to tolerate oral diet.
Grades I and II cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis:
May discontinue 24 hours after cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
Treat for 4–7 days when necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, or emphysematous changes are noted at cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
Grade III cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis:
Treat for 4–7 days after cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
Treat for at least 2 weeks if gram-positiveGram-PositivePenicillinscocciCocciBacteriology (e.g., EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus) bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides is present.
Health care–associated infection: Gram-positiveGram-PositivePenicillinscocciCocciBacteriology (e.g., EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus) bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides requires 2 weeks of treatment.
Surgical treatment[4,7,8,10]
CholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy:
Definitive treatment
Approach:
Laparoscopic is the standard of careStandard of careThe minimum acceptable patient care, based on statutes, court decisions, policies, or professional guidelines.Malpractice (lower risk of infection, shorter hospital stay).[4,7]
Open surgery: reserved for complicated cases
Timing:
Surgery performed early (within 72 hours of presentation): better outcomes[4]
Surgery performed > 72 hours is relatively safe, but ↑ inflammatory changes after 72 hours → ↑ complications, ↑ hospital stay, ↑ risk of conversion to open surgery[10]
According to the World Society of Emergency Surgery (WSES) guidelines, if cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy is not performed within the 1st 10 days of symptoms, surgery should be delayed by 45 days (unless disease progresses) to allow inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation to subside.[8]
Emergent surgery: may be required for emphysematous gallbladderEmphysematous GallbladderCholecystectomy, gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: AnatomyperforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis/gangreneGangreneDeath and putrefaction of tissue usually due to a loss of blood supply.Small Bowel Obstruction, generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
Surgical considerations by grade:[4,5]
Grade I cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis:
Surgery at the early stage or within 72 hours after onset is recommended.
If initially managed conservatively and no response is noted in 24 hours, proceed with surgery.
Grade II cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis:
The degree of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation is likely associated with increased operative difficulty.
Surgery depends on the patient performance status.
If status is good → proceed with early surgery.
If status is poor → initial supportive therapy and biliary drainage/cholecystotomy
Grade III cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis:
Urgent treatment (surgery and/or drainage)
Intensive care
Those presenting with > 10 days of symptoms → delay surgery unless disease becomes progressive.
Complications of surgery:
BileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct injury
Biliary leaks
Injury to nearby structures
Post-cholecystectomy syndrome
Percutaneous cholecystostomy:
GB is drained/decompressed with a tube placed endoscopically or percutaneously under radiologic guidance.
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with:
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to surgery
CholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis not resolving with antibiotics/supportive management
Acalculous cholecystitisAcalculous cholecystitisInflammation of the gallbladder wall in the absence of gallstones.Cholecystitis (especially the severely ill)
Late presentation (> 72 hours after symptom onset)
Outcomes:[7]
Improvement is usually noted in 72 hours.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who stabilize and become surgical candidates (e.g., those with calculus cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis) should undergo cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy.
No improvement with drainage indicates gangreneGangreneDeath and putrefaction of tissue usually due to a loss of blood supply.Small Bowel Obstruction → emergency cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy is indicated.
In those who continue to be poor surgical candidates, percutaneous gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy stone extraction can be performed.
Endoscopic retrograde cholangiopancreatographyEndoscopic Retrograde CholangiopancreatographyFiberoptic endoscopy designed for duodenal observation and cannulation of Vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (Vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis (ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis):
Prior to surgery, if US shows that common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct (CBDCBDAtypical Parkinsonian Syndromes) stones are present
RUQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways/tenderness/massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Comprehensive metabolic panelComprehensive metabolic panelPrimary vs Secondary Headaches (includes renal and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy function)
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption, lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion
PT/INR
CRP
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test in women
Imaging studies:
Ultrasonography
HIDA, if needed
Additional imaging (e.g., CT needed if other sources of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and/or infection are considered; MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis if common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct stone is suspected)
IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
AntiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics
Antibiotic therapy (if clinically indicated)
Additional test: blood cultures (if indicated)
Determine appropriateness and timing of definitive treatment (laparoscopic cholecystectomyLaparoscopic cholecystectomyExcision of the gallbladder through an abdominal incision using a laparoscope.Cholecystectomy)
If early surgery is performed, send bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy culture in grades II and III.
If early laparoscopic cholecystectomyLaparoscopic cholecystectomyExcision of the gallbladder through an abdominal incision using a laparoscope.Cholecystectomy will not be performed, determine alternative management.
Reassess patient.
Complications
Several clinically relevant complications of cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis include:[3]
Gangrenous cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis
Most common complication
Severe inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation leads to necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of the GB wall
Usually affects patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, elderly patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship, or those with delayed diagnosis
Emphysematous cholecystitisEmphysematous cholecystitisA variant of acute cholecystitis with inflammation of the gallbladder that is characterized by the pockets of gas in the gallbladder wall. It is due to secondary infection caused by gas-forming organisms, and has a high risk of perforation.Cholecystectomy
Infection with gas-forming bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology (Clostridium)
Gas in the GB wall (may manifest as abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the AbdomencrepitusCrepitusOsteoarthritis on exam)
Usually in diabetic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Very distended GB filled with colorless mucoid fluid (white bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy)
Prolonged impaction of a gallstone in the cysticCysticFibrocystic Change duct → bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme MetabolismabsorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption within the GB
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula forms between the inflamed GB and duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (cholecystoenteric fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula).
Gallstone travels into the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy → small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis
GallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: AnatomyperforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
10% of acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis
Leads to a pericholecystic abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease or generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
Mirizzi syndromeMirizzi syndromeComplication of cholelithiasis characterized by obstructive jaundice; abdominal pain, and fever.Cholecystitis
Presents with jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and abdominal painAbdominal PainAcute Abdomen
Other biliary/liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy conditions
Biliary colic: post-prandial painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways/nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics caused by brief intermittent cysticCysticFibrocystic Change duct obstruction. Associated with normal blood tests, gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis (no signs of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation) on US.
Biliary dyskinesiaBiliary dyskinesiaA motility disorder characterized by biliary colic, absence of gallstones, and an abnormal gallbladder ejection fraction. It is caused by gallbladder dyskinesia and/or sphincter of oddi dysfunction.Cholecystectomy: dysfunctional motilityMotilityThe motor activity of the gastrointestinal tract.Gastrointestinal Motility of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy (with no stones). The clinical picture is similar to biliary colic/cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis. Diagnosed by HIDA scanHIDA scanNuclear Imaging with cholecystokininCholecystokininA peptide, of about 33 amino acids, secreted by the upper intestinal mucosa and also found in the central nervous system. It causes gallbladder contraction, release of pancreatic exocrine (or digestive) enzymes, and affects other gastrointestinal functions. Cholecystokinin may be the mediator of satiety.Gastrointestinal Secretions (CCK) injection where results show low GB ejection fractionEjection fractionCardiac Cycle.
CholedocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis/cholangitis:gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis in the common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct cause obstruction (choledocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis), which may lead to infection (cholangitis). This condition presents with high bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism (> 2.0) and alkaline phosphataseAlkaline PhosphataseAn enzyme that catalyzes the conversion of an orthophosphoric monoester and water to an alcohol and orthophosphate.Osteosarcoma, with early elevation of transaminasesTransaminasesA subclass of enzymes of the transferase class that catalyze the transfer of an amino group from a donor (generally an amino acid) to an acceptor (generally a 2-keto acid). Most of these enzymes are pyridoxyl phosphate proteins.Autoimmune Hepatitis.
Gallstone pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis: intermittent obstruction of junction of CBDCBDAtypical Parkinsonian Syndromes and pancreatic duct from a migrating gallstone leads to pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. Work-up shows elevated amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption/lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion with pancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation on US/CT scan.
Hepatitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy parenchyma due to infectious etiology or other causes. Usually associated with very high transaminasesTransaminasesA subclass of enzymes of the transferase class that catalyze the transfer of an amino group from a donor (generally an amino acid) to an acceptor (generally a 2-keto acid). Most of these enzymes are pyridoxyl phosphate proteins.Autoimmune Hepatitisand elevated bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism. Ultrasound would not show any gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis.
Non-biliary conditions
Peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease: ulcerationUlcerationCorneal Abrasions, Erosion, and Ulcers of gastric or duodenal mucosa. Presents with epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear), nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Unlike in cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is often relieved by eating. Diagnosis is by upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD).
Acute gastroenteritisGastroenteritisGastroenteritis is inflammation of the stomach and intestines, commonly caused by infections from bacteria, viruses, or parasites. Transmission may be foodborne, fecal-oral, or through animal contact. Common clinical features include abdominal pain, diarrhea, vomiting, fever, and dehydration.Gastroenteritis: usually self-limited viral infection of the gastrointestinal tract. Manifestations include abdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, and diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea. Symptoms resolve with supportive management.
Acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis: an infection/inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy. Usual presentation includes nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, anorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the right lower quadrantRight lower quadrantAnterior Abdominal Wall: Anatomy (RLQ). In certain cases (pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care, retrocecal position of the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy), may also present with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in RUQ.
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy. Epigastric/RUQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is sudden in onset and typically sharp, radiating to the back, and is relieved on bending forward. Etiologies consist of gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis and increased alcohol consumption.
NephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis: also known as kidney stonesKidney stonesNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis. Presents with sudden onset of severe right or left flankLeft FlankSurgical Anatomy of the AbdomenpainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is colicky in nature and associated with urinary symptoms (dysuriaDysuriaPainful urination. It is often associated with infections of the lower urinary tract.Urinary Tract Infections (UTIs), hematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma). Diagnosis is by non-contrast CT scan (sometimes plain X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests), which shows stones in the urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy.
Fitz-Hugh Curtis syndrome: perihepatitis occurring due to acute pelvic inflammatory diseaseAcute Pelvic Inflammatory DiseasePelvic Inflammatory Disease. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship manifest with RUQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, but there is also notable lower quadrant painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. Uterine, adnexal, and/or cervical motion tenderness with vaginal discharge is also found. Aminotransferases are often normal or are mildly elevated. LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: AnatomycapsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.BacteroidesinflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation is seen as pericholecystic fluidPericholecystic FluidImaging of the Liver and Biliary Tract on US. HIDA scanHIDA scanNuclear Imaging would be negative.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, or inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy, most commonly caused by gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis. The codes distinguish between acute and chronic cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis.
Coding System
Code
Description
ICD-10-CM
K81.0
Acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis
ICD-10-CM
K81.1
Chronic cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis
ICD-10-CM
K81.9
CholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, unspecified
Ultrasound, abdominal, real time with image documentationDocumentationSystematic organization, storage, retrieval, and dissemination of specialized information, especially of a scientific or technical nature. It often involves authenticating or validating information.Advance Directives; limited
CPT
78227
Hepatobiliary scintigraphyScintigraphySjögren Syndrome, including gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy when present, with or without pharmacologic intervention
Procedures/Interventions:
This CPT code is for a laparoscopic cholecystectomyLaparoscopic cholecystectomyExcision of the gallbladder through an abdominal incision using a laparoscope.Cholecystectomy, the definitive surgical treatment for cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis, which involves removing the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy.
Coding System
Code
Description
CPT
47562
LaparoscopyLaparoscopyLaparoscopy is surgical exploration and interventions performed through small incisions with a camera and long instruments. Laparotomy and Laparoscopy, surgical; cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
Mayumi, T., Okamoto, K., Takada, T., Strasberg, S. M., Solomkin, J. S., Schlossberg, D., Pitt, H. A., Yoshida, M., Gomi, H., Miura, F., Garden, O. J., Kiriyama, S., Yokoe, M., Endo, I., Asbun, H. J., Iwashita, Y., Hibi, T., Umezawa, A., Suzuki, K., Itoi, T., … Yamamoto, M. (2018). Tokyo Guidelines 2018: management bundles for acute cholangitis and cholecystitis. Journal of Hepato-biliary-pancreatic Sciences, 25(1), 96–100. https://doi.org/10.1002/jhbp.519
Hirota, M., Takada, T., Kawarada, Y., Nimura, Y., Miura, F., Hirata, K., Mayumi, T., Yoshida, M., Strasberg, S., Pitt, H., Gadacz, T. R., de Santibanes, E., Gouma, D. J., Solomkin, J. S., Belghiti, J., Neuhaus, H., Büchler, M. W., Fan, S. T., Ker, C. G., Padbury, R. T., … Dervenis, C. (2007). Diagnostic criteria and severity assessment of acute cholecystitis: Tokyo Guidelines. Journal of Hepato-Biliary-Pancreatic Surgery, 14(1), 78–82. https://doi.org/10.1007/s00534-006-1159-4
Solomkin, J. S., Mazuski, J. E., Bradley, J. S., Rodvold, K. A., Goldstein, E. J., Baron, E. J., O’Neill, P. J., Chow, A. W., Dellinger, E. P., Eachempati, S. R., Gorbach, S., Hilfiker, M., May, A. K., Nathens, A. B., Sawyer, R. G., Bartlett, J. G. (2010). Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clinical Infectious Diseases, 50(2), 133–164. https://doi.org/10.1086/649554
National Institute for Health Care and Excellence. (2014). Gallstone disease: diagnosis and management. Retrieved August 9, 2022, from https://www.nice.org.uk/guidance/cg188
Ansaloni, L., Pisano, M., Coccolini, F., et al. (2016). 2016 WSES guidelines on acute calculous cholecystitis. World Journal of Emergency Surgery, 11, 25. https://doi.org/10.1186/s13017-016-0082-5
Park, M. S., Yu, J. S., Kim, Y. H., Kim, M. J., Kim, J. H., Lee, S., Cho, N., Kim, D. G., Kim, K. W. (1998). Acute cholecystitis: comparison of MR cholangiography and US. Radiology, 209(3), 781–785. https://doi.org/10.1148/radiology.209.3.9844674
Wu, X. D., Tian, X., Liu, M. M., Wu, L., Zhao, S., Zhao, L. (2015). Meta-analysis comparing early versus delayed laparoscopic cholecystectomy for acute cholecystitis. British Journal of Surgery, 102(11), 1302–1313. https://doi.org/10.1002/bjs.9886
Gomi, H., Solomkin, J. S., Schlossberg, D., Okamoto, K., Takada, T., Strasberg, S. M., Ukai, T., Endo, I., Iwashita, Y., Hibi, T., Pitt, H. A., Matsunaga, N., Takamori, Y., Umezawa, A., Asai, K., Suzuki, K., Han, H. S., Hwang, T. L., Mori, Y., Yoon, Y. S., … Yamamoto, M. (2018). Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis. Journal of Hepato-Biliary-Pancreatic Sciences, 25(1), 3–16. https://doi.org/10.1002/jhbp.518
Create your free account or log in to continue reading!