Laryngitis is an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body's defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy most commonly due to infection or trauma that can be either acute or chronic. In this condition, the 2 folds of mucous membranes that make up the vocal cordsVocal cordsA pair of cone-shaped elastic mucous membrane projecting from the laryngeal wall and forming a narrow slit between them. Each contains a thickened free edge (vocal ligament) extending from the thyroid cartilage to the arytenoid cartilage, and a vocal muscle that shortens or relaxes the vocal cord to control sound production.Larynx: Anatomy become inflamed and irritated. The inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body's defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation results in a distortionDistortionDefense Mechanisms of the voice produced, resulting in a hoarse sound that may lead to an inability to produce any sound (aphonia) in severe cases. In the presence of an infectious cause, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship often also present with rhinorrheaRhinorrheaExcess nasal drainage.Respiratory Syncytial Virus, cough, and mild sore throatSore throatPharyngitis is an inflammation of the back of the throat (pharynx). Pharyngitis is usually caused by an upper respiratory tract infection, which is viral in most cases. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, and hoarseness.Pharyngitis.
Laryngitis may be secondary to infection, allergiesAllergiesA medical specialty concerned with the hypersensitivity of the individual to foreign substances and protection from the resultant infection or disorder.Selective IgA Deficiency, trauma, benignBenignFibroadenoma or malignant lesions, neurologic dysfunction, functional issues, or systemic causes (see table).
Causes of acute laryngitis
Causes of chronic laryngitis
Viral (most common):
RhinovirusRhinovirusRhinovirus is an acid-labile, positive-sense RNA virus of the Picornavirus family. The virus, which causes the common cold, is most often acquired through the airway via the inhalation of aerosols containing rhinovirus and fomites. Rhinovirus
InfluenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/InfluenzavirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology
Parainfluenza virusParainfluenza virusHuman parainfluenza viruses (HPIVs) are single-stranded, linear, negative-sense RNA viruses of the family Paramyxoviridae and the genus Paramyxovirus. Human parainfluenza viruses are the 2nd most common cause of lower respiratory disease in children, after the respiratory syncytial virus.Parainfluenza Virus
AdenovirusAdenovirusAdenovirus (member of the family Adenoviridae) is a nonenveloped, double-stranded DNA virus. Adenovirus is transmitted in a variety of ways, and it can have various presentations based on the site of entry. Presentation can include febrile pharyngitis, conjunctivitis, acute respiratory disease, atypical pneumonia, and gastroenteritis. Adenovirus
CoronavirusCoronavirusCoronaviruses are a group of related viruses that contain positive-sense, single-stranded RNA. Coronavirus derives its name from “κορώνη korṓnē” in Greek, which translates as “crown,” after the small club-shaped proteins visible as a ring around the viral envelope in electron micrographs. Coronavirus
Respiratory syncytial virusRespiratory Syncytial VirusRespiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract.Respiratory Syncytial Virus
Compromised immune systems may suffer from herpes, HIVHIVAnti-HIV Drugs, or coxsackievirusCoxsackievirusCoxsackievirus is a member of a family of viruses called Picornaviridae and the genus Enterovirus. Coxsackieviruses are single-stranded, positive-sense RNA viruses, and are divided into coxsackie group A and B viruses. Both groups of viruses cause upper respiratory infections, rashes, aseptic meningitis, or encephalitis. CoxsackievirusinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Bacterial:
Group A streptococcusGroup A StreptococcusA species of gram-positive, coccoid bacteria isolated from skin lesions, blood, inflammatory exudates, and the upper respiratory tract of humans. It is a group a hemolytic Streptococcus that can cause scarlet fever and rheumatic fever.Postinfectious Glomerulonephritis
StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus pneumoniae
Corynebacterium diphtheriaeCorynebacterium diphtheriaeDiphtheria is an infectious disease caused by corynebacterium diphtheriae that most often results in respiratory disease with membranous inflammation of the pharynx, sore throat, fever, swollen glands, and weakness. The hallmark sign is a sheet of thick, gray material covering the back of the throat.Diphtheria
Moraxella catarrhalisMoraxella catarrhalisGram-negative aerobic cocci of low virulence that colonize the nasopharynx and occasionally cause meningitis; bacteremia; empyema; pericarditis; and pneumonia.Moraxella
Haemophilus influenzaeHaemophilus InfluenzaeA species of Haemophilus found on the mucous membranes of humans and a variety of animals. The species is further divided into biotypes I through viii.Haemophilus
Bordetella pertussisBordetella pertussisA species of gram-negative, aerobic bacteria that is the causative agent of whooping cough. Its cells are minute coccobacilli that are surrounded by a slime sheath.Bordetella
Bacillus anthracisBacillus anthracisA species of bacteria that causes anthrax in humans and animals.Anthrax
Mycobacterium tuberculosisMycobacterium tuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes.Tuberculosis
Fungal:
HistoplasmaHistoplasmaHistoplasmosis is an infection caused by Histoplasma capsulatum, a dimorphic fungus. The fungus exists as a mold at low temperatures and as yeast at high temperatures. H. capsulatum is the most common endemic fungal infection in the US and is most prevalent in the midwestern and central states along the Ohio and Mississippi River valleys.Histoplasma/Histoplasmosis
BlastomycesBlastomycesBlastomycosis is an infection caused by inhalation of the spores of the fungus, Blastomyces. Blastomyces species thrive in moist soil and decaying material and are common in the Ohio and Mississippi River valleys and the Great Lakes regions of the United States and Canada. Although most patients are asymptomatic, some can develop pneumonia.Blastomyces/Blastomycosis
CandidaCandidaCandida is a genus of dimorphic, opportunistic fungi. Candida albicans is part of the normal human flora and is the most common cause of candidiasis. The clinical presentation varies and can include localized mucocutaneous infections (e.g., oropharyngeal, esophageal, intertriginous, and vulvovaginal candidiasis) and invasive disease (e.g., candidemia, intraabdominal abscess, pericarditis, and meningitis). Candida/Candidiasis (immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
CryptococcusCryptococcusCryptococcosis is an opportunistic, fungal infection caused by the Cryptococcus species. The principal pathogens in humans are C. neoformans (primary) and C. gattii. Cryptococcus neoformans is typically found in pigeon droppings and acquired by inhaling dust from contaminated soil. The majority of affected patients are immunocompromised. Cryptococcus/Cryptococcosis
CoccidioidesCoccidioidesCoccidioidomycosis, commonly known as San Joaquin Valley fever, is a fungal disease caused by Coccidioides immitis or Coccidioides posadasii. When Coccidioides spores are inhaled, they transform into spherules that result in infection. Coccidioidomycosis is also a common cause of community-acquired pneumonia and can cause severe disease in the immunocompromised.Coccidioides/Coccidioidomycosis
AllergiesAllergiesA medical specialty concerned with the hypersensitivity of the individual to foreign substances and protection from the resultant infection or disorder.Selective IgA Deficiency
Nerve damage
Acid reflux
Autoimmune disorders
Anatomic defects (e.g., polyps, nodules, sores, cancer on the larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy)
Neurological disease (e.g., Parkinson’s, myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis)
Trauma
Stroke
Clinical Presentation
History
Triggering factors: concurrent upper respiratory infectionUpper respiratory infectionRhinitis, vocal overuse/abuse, exposure to allergens or toxins
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases, alcohol use, new medications
Recent or past surgery involving the head and/or neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Recent or past trauma involving the head and/or neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Signs and Symptoms (variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables)
Dry or sore throatSore throatPharyngitis is an inflammation of the back of the throat (pharynx). Pharyngitis is usually caused by an upper respiratory tract infection, which is viral in most cases. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, and hoarseness.Pharyngitis
Coughing
Frequent throatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy clearing
Increased salivaSalivaThe clear, viscous fluid secreted by the salivary glands and mucous glands of the mouth. It contains mucins, water, organic salts, and ptyalin.Salivary Glands: Anatomy production
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia
Globus pharyngeus (feeling of a lump in the throatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy)
Swollen lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy in the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess, chest, or face
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea
Vocal fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Aphonia (inability to voice a sound)
Diagnosis
Laryngitis due to trauma: a history of trauma to the head and/or neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Acute viral laryngitis: diagnosed by the low vocal pitch and hoarsenessHoarsenessAn unnaturally deep or rough quality of voice.Parapharyngeal Abscess
Fungal laryngitis: confirmation made by biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma and culturing of abnormal lesions
Laryngoscopy or stroboscopy for direct and complete visualization of true vocal folds, false vocal folds, epiglottisEpiglottisA thin leaf-shaped cartilage that is covered with laryngeal mucosa and situated posterior to the root of the tongue and hyoid bone. During swallowing, the epiglottis folds back over the larynx inlet thus prevents foods from entering the airway.Larynx: Anatomy, pyriform sinus; and vallecula for:
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion (reddening)
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema (swellingSwellingInflammation)
Dilated blood vessels (acute)
Thick, dry laryngeal tissue (chronic)
Stiff vocal folds
Viscous secretions in the vicinity of the vocal folds
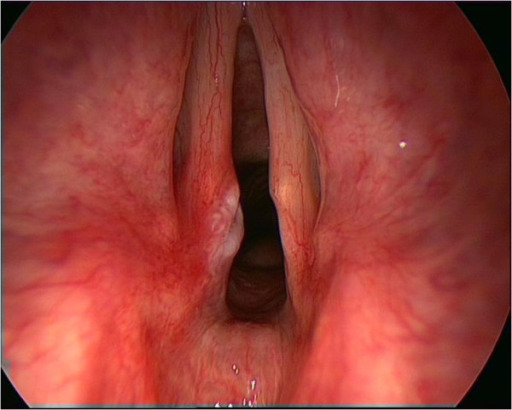
Inflamed, erythematous vocal cords demonstrate injury in a patient with a chronic cough. Notice a distinct area of injury on the left vocal cord posteriorly.
Image: “The larynx in cough” by Consultant Otolaryngologist, Imperial College London, London, UK. License: CC BY 2.0
Management
Acute laryngitis
Chronic laryngitis
Viral
Vocal rest, therapy, and oral hygiene
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways medication
Mucolytics
Home remedies (salt water, honey)
Hydration
Humidification
Reflux
Wearing loose clothing
Smaller but more frequent meals
Avoid caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants, alcohol, spicy foods
Over-the-counter medications for neutralizing acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance (antacids)
Topical nasal steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
Immunotherapy
AntihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines
Topical nystatinNystatinMacrolide antifungal antibiotic complex produced by streptomyces noursei, s. Aureus, and other streptomyces species. The biologically active components of the complex are nystatin a1, a2, and a3.Polyenes (as a suspension or pastille)
Autoimmune
CyclophosphamideCyclophosphamidePrecursor of an alkylating nitrogen mustard antineoplastic and immunosuppressive agent that must be activated in the liver to form the active aldophosphamide. It has been used in the treatment of lymphoma and leukemia. Its side effect, alopecia, has been used for defleecing sheep. Cyclophosphamide may also cause sterility, birth defects, mutations, and cancer.Immunosuppressants
PrednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants
Persistent but self-limited, typically resolving within 3 weeks
Recovery is enhanced when patient follows the treatment regimen.
In viral laryngitis, symptoms can persist for an extended period, even when upper respiratory tract inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation has been resolved.
Chronic
Laryngitis that persists for more than 3 weeks
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas is dependent on the etiology of laryngitis.
Associated head and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess cancer risk factors (e.g., tobacco and alcohol use)
Red flag symptomatologySymptomatologyScarlet Fever of a possible malignancyMalignancyHemothorax (e.g., hemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis, unilateral painUnilateral PainCluster Headaches, dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia, unexplained weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea)
Differential Diagnosis
The following conditions are in included in the differential diagnoses of laryngitis:
Any condition that presents with dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia:patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship experience difficulty swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility certain foods or liquids, while others can’t swallow at all. DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia may present due to allergiesAllergiesA medical specialty concerned with the hypersensitivity of the individual to foreign substances and protection from the resultant infection or disorder.Selective IgA Deficiency or “colds,” dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration, gastroesophageal reflux diseaseGastroesophageal Reflux DiseaseGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD), certain medications, or tumors in the mouth, throatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy, or esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy.
Gastroesophageal reflux diseaseGastroesophageal Reflux DiseaseGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD): the upward movement of gastric acidGastric acidHydrochloric acid present in gastric juice.Gastroesophageal Reflux Disease (GERD) into the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy, which results in heartburnHeartburnSubsternal pain or burning sensation, usually associated with regurgitation of gastric juice into the esophagus.Gastroesophageal Reflux Disease (GERD) or chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. Acid reflux may spill over into the larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy, and acidic irritation to larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy may result in voice hoarsenessHoarsenessAn unnaturally deep or rough quality of voice.Parapharyngeal Abscess.
TonsillitisTonsillitisTonsillitis is inflammation of the pharynx or pharyngeal tonsils, and therefore is also called pharyngitis. An infectious etiology in the setting of tonsillitis is referred to as infectious pharyngitis, which is caused by viruses (most common), bacteria, or fungi. Tonsillitis: an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pharyngeal tonsilsTonsilsTonsillitis that is most commonly present in combination with an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pharynxPharynxThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking. Pharynx: Anatomy. TonsillitisTonsillitisTonsillitis is inflammation of the pharynx or pharyngeal tonsils, and therefore is also called pharyngitis. An infectious etiology in the setting of tonsillitis is referred to as infectious pharyngitis, which is caused by viruses (most common), bacteria, or fungi. Tonsillitis is very common among children and young adults and is primarily caused by virusesVirusesMinute infectious agents whose genomes are composed of DNA or RNA, but not both. They are characterized by a lack of independent metabolism and the inability to replicate outside living host cells.Virology and group A streptococci.
Laryngeal carcinoma: a malignant tumorTumorInflammation of the larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy that affects older men most commonly. Risk factors include smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases and excessive alcohol consumption.
Allergic rhinitisAllergic rhinitisAn inflammation of the nasal mucosa triggered by allergens.Rhinitis: an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the nasal mucosaNasal mucosaThe mucous lining of the nasal cavity, including lining of the nostril (vestibule) and the olfactory mucosa. Nasal mucosa consists of ciliated cells, goblet cells, brush cells, small granule cells, basal cells (stem cells) and glands containing both mucous and serous cells.Nose Anatomy (External & Internal) classified into allergic, non-allergic, and infectious. Allergic rhinitisAllergic rhinitisAn inflammation of the nasal mucosa triggered by allergens.Rhinitis is due to a type 1Type 1Spinal Muscular Atrophy hypersensitivity reaction. All 3 types present with nasal congestion, rhinorrheaRhinorrheaExcess nasal drainage.Respiratory Syncytial Virus, and sneezingSneezingThe sudden, forceful, involuntary expulsion of air from the nose and mouth caused by irritation to the mucous membranes of the upper respiratory tract.Rhinovirus.
References
Aboul Hosn O, Sutton AE. Acute Laryngitis. [Updated 2026 Feb 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534871/