Substances can accumulate in the cytoplasm, nucleusNucleusWithin a eukaryotic cell, a membrane-limited body which contains chromosomes and one or more nucleoli (cell nucleolus). The nuclear membrane consists of a double unit-type membrane which is perforated by a number of pores; the outermost membrane is continuous with the endoplasmic reticulum. A cell may contain more than one nucleus.The Cell: Organelles, or organellesOrganellesA cell is a complex unit that performs several complex functions. An organelle is a specialized subunit within a cell that fulfills a specific role or function. Organelles are enclosed within their own lipid bilayers or are unbound by membranes. The Cell: Organelles as a result of an intrinsic cellular dysfunction or metabolic abnormalities. Commonly seen substances are pigments, calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes, ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements, fat, cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism, and glycogen. These substances are produced by the cell and can increase in amount when there is inadequate removal of the substance or failure of metabolite degradation. Defective protein foldingProtein foldingProcesses involved in the formation of tertiary protein structure.Proteins and Peptides, packaging, and transport, both genetic and acquired, also produce substance accumulation. In some instances, deposition is from an external source, such as coal dust. The cell does not have an inherent mechanism of eliminationEliminationThe initial damage and destruction of tumor cells by innate and adaptive immunity. Completion of the phase means no cancer growth. Cancer Immunotherapy, so material builds up in the exposed site.
Intrinsic abnormality in the cell function (genetic disease)
Exogenous source
Effect: Substances that accumulate may or may not be harmful.
Mechanisms
Abnormal metabolism:
Normal substance produced → defect in packaging and transport → substance build-up
Seen in fatty liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy (increase in lipid particles)
Abnormal substance (misfolded proteinsMisfolded ProteinsCell Injury and Death) produced → overwhelms repair → accumulate in the endoplasmic reticulumEndoplasmic reticulumA system of cisternae in the cytoplasm of many cells. In places the endoplasmic reticulum is continuous with the plasma membrane (cell membrane) or outer membrane of the nuclear envelope. If the outer surfaces of the endoplasmic reticulum membranes are coated with ribosomes, the endoplasmic reticulum is said to be rough-surfaced; otherwise it is said to be smooth-surfaced.The Cell: Organelles (ER)
Seen in ɑ-1 antitrypsin deficiency
Lack of enzyme:
SubstrateSubstrateA substance upon which the enzyme acts.Basics of Enzymes → failure to convert to the final product (no enzyme) → increased amount of substrateSubstrateA substance upon which the enzyme acts.Basics of Enzymes
Seen in lysosomal storage diseaseLysosomal storage diseaseLysosomal storage diseases are a group of metabolic disorders caused by genetic mutations in the enzymes responsible for normal lysosomal function. The dysfunction of enzymatic processes causes an accumulation of undigested metabolites, resulting in cellular death. The main groups include sphingolipidoses, oligosaccharidoses, and mucolipidoses. Overview of Lysosomal Storage Diseases
Deposition of an exogenous material or indigestible substance:
Exogenous substance → cell with no capacity to degrade or transport → accumulation
Seen in silicosisSilicosisA form of pneumoconiosis resulting from inhalation of dust containing crystalline form of silicon dioxide, usually in the form of quartz. Amorphous silica is relatively nontoxic.Pneumoconiosis (silica) and anthracosis (carbon)
Pigments
Exogenous pigments
Pigments coming from outside the body:
Tattoos: pigments phagocytosed by macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation, often without inflammatory response
Carbon or coal dust:
Anthracotic or carbon pigment: carbonaceous debris from urban living, coal mining, and cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
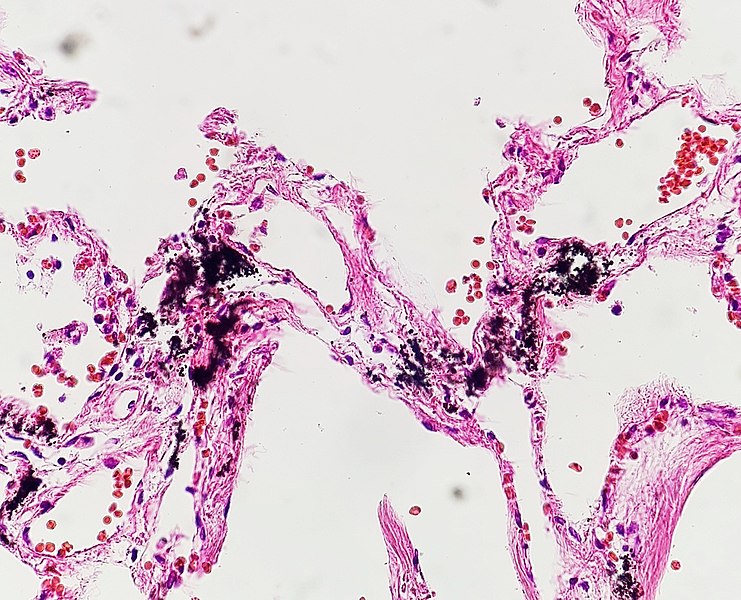
Associated with anthracosis, accumulation of black pigment in the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
Coal worker’s pneumoconiosisPneumoconiosisPneumoconiosis is an occupational disease that results from the inhalation and deposition of mineral dusts and other inorganic particles in the lung. It can be categorized according to the type of causative particle involved or by the type of response provoked.Pneumoconiosis: fibrotic lung disease that develops from the reaction to accumulated carbon dust in the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
Histopathology of pulmonary anthracosis, showing interstitial black material
Image: “Histopathology of pulmonary anthracosis” by Mikael Häggström, M.D. License: CC0 1.0
Section of a lung showing changes consistent with chronic exposure to coal dust (anthracosis): Areas appear black due to the build-up of coal-dust particles.
Image: “Black Lung in Appalachia” by US National Library of Medicine. License: Public Domain
Endogenous pigments
Endogenous pigments are synthesized within the body.
LipofuscinLipofuscinA naturally occurring lipid pigment with histochemical characteristics similar to ceroid. It accumulates in various normal tissues and apparently increases in quantity with age.Macular Degeneration or lipochrome:
Wear and tear or aging pigment
Derived from lipid peroxidationLipid peroxidationPeroxidase catalyzed oxidation of lipids using hydrogen peroxide as an electron acceptor.Drug-Induced Liver Injury and accumulates in lysosomesLysosomesA class of morphologically heterogeneous cytoplasmic particles in animal and plant tissues characterized by their content of hydrolytic enzymes and the structure-linked latency of these enzymes. The intracellular functions of lysosomes depend on their lytic potential. The single unit membrane of the lysosome acts as a barrier between the enzymes enclosed in the lysosome and the external substrate. The activity of the enzymes contained in lysosomes is limited or nil unless the vesicle in which they are enclosed is ruptured or undergoes membrane fusion.The Cell: Organelles
Found most commonly in the heart and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
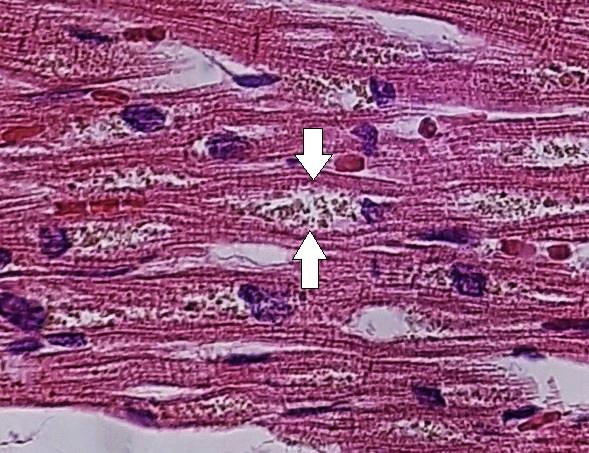
Brown atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation: Significant amounts of lipofuscinLipofuscinA naturally occurring lipid pigment with histochemical characteristics similar to ceroid. It accumulates in various normal tissues and apparently increases in quantity with age.Macular Degeneration impart a brown discoloration to the affected organ.
Microscopic morphology: yellow-brown pigment granules often surrounding the nucleusNucleusWithin a eukaryotic cell, a membrane-limited body which contains chromosomes and one or more nucleoli (cell nucleolus). The nuclear membrane consists of a double unit-type membrane which is perforated by a number of pores; the outermost membrane is continuous with the endoplasmic reticulum. A cell may contain more than one nucleus.The Cell: Organelles
Lipofuscin (arrows) in the cardiac muscle
Image: “Myocardial lipofuscin” by Mikael Häggström, M.D. License: CC0 1.0
Hemosiderosis (ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements):
Accumulation of hemosiderinHemosiderinHeme Metabolism, a storage form of ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements,in macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentationwithout side effects
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements physiology:
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements has 2 storage forms: ferritinFerritinIron-containing proteins that are widely distributed in animals, plants, and microorganisms. Their major function is to store iron in a nontoxic bioavailable form. Each ferritin molecule consists of ferric iron in a hollow protein shell (apoferritins) made of 24 subunits of various sequences depending on the species and tissue types.Hereditary Hemochromatosis and hemosiderinHemosiderinHeme Metabolism
↑ IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements → ferritinFerritinIron-containing proteins that are widely distributed in animals, plants, and microorganisms. Their major function is to store iron in a nontoxic bioavailable form. Each ferritin molecule consists of ferric iron in a hollow protein shell (apoferritins) made of 24 subunits of various sequences depending on the species and tissue types.Hereditary Hemochromatosis forms hemosiderinHemosiderinHeme Metabolism granules (hemosiderinHemosiderinHeme Metabolism pigment = aggregates of ferritinFerritinIron-containing proteins that are widely distributed in animals, plants, and microorganisms. Their major function is to store iron in a nontoxic bioavailable form. Each ferritin molecule consists of ferric iron in a hollow protein shell (apoferritins) made of 24 subunits of various sequences depending on the species and tissue types.Hereditary HemochromatosismicellesMicellesParticles consisting of aggregates of molecules held loosely together by secondary bonds. The surface of micelles are usually comprised of amphiphatic compounds that are oriented in a way that minimizes the energy of interaction between the micelle and its environment. Liquids that contain large numbers of suspended micelles are referred to as emulsions.Malabsorption and Maldigestion)
Local bruise or extravasated blood cells to the site of injury
Multiple transfusions (overload of exogenous ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements)
Hemolytic anemiaHemolytic AnemiaHemolytic anemia (HA) is the term given to a large group of anemias that are caused by the premature destruction/hemolysis of circulating red blood cells (RBCs). Hemolysis can occur within (intravascular hemolysis) or outside the blood vessels (extravascular hemolysis). Hemolytic Anemia (red cell lysis releases ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements)
Genetic defectGenetic DefectIon Channel Myopathy of ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements metabolism (hemochromatosisHemochromatosisA disorder of iron metabolism characterized by a triad of hemosiderosis; liver cirrhosis; and diabetes mellitus. It is caused by massive iron deposits in parenchymal cells that may develop after a prolonged increase of iron absorption.Hereditary Hemochromatosis)
HemochromatosisHemochromatosisA disorder of iron metabolism characterized by a triad of hemosiderosis; liver cirrhosis; and diabetes mellitus. It is caused by massive iron deposits in parenchymal cells that may develop after a prolonged increase of iron absorption.Hereditary Hemochromatosis (ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements):
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements accumulates in the parenchyma due to excessive iron absorptionIron absorptionDigestion and Absorption.
Associated with side effects
Types:
Hereditary: due to mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations of genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure
Secondary: due to parenteral administration of ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements (e.g., transfusions)
Found in:
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy: cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions: abnormal pigmentation (especially sun-exposed areas)
PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy: diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
Heart: cardiomyopathyCardiomyopathyCardiomyopathy refers to a group of myocardial diseases associated with structural changes of the heart muscles (myocardium) and impaired systolic and/or diastolic function in the absence of other heart disorders (coronary artery disease, hypertension, valvular disease, and congenital heart disease). Cardiomyopathy: Overview and Types, arrhythmias
LysosomesLysosomesA class of morphologically heterogeneous cytoplasmic particles in animal and plant tissues characterized by their content of hydrolytic enzymes and the structure-linked latency of these enzymes. The intracellular functions of lysosomes depend on their lytic potential. The single unit membrane of the lysosome acts as a barrier between the enzymes enclosed in the lysosome and the external substrate. The activity of the enzymes contained in lysosomes is limited or nil unless the vesicle in which they are enclosed is ruptured or undergoes membrane fusion.The Cell: Organelles and mitochondriaMitochondriaSemiautonomous, self-reproducing organelles that occur in the cytoplasm of all cells of most, but not all, eukaryotes. Each mitochondrion is surrounded by a double limiting membrane. The inner membrane is highly invaginated, and its projections are called cristae. Mitochondria are the sites of the reactions of oxidative phosphorylation, which result in the formation of ATP. They contain distinctive ribosomes, transfer RNAs; amino Acyl tRNA synthetases; and elongation and termination factors. Mitochondria depend upon genes within the nucleus of the cells in which they reside for many essential messenger RNAs. Mitochondria are believed to have arisen from aerobic bacteria that established a symbiotic relationship with primitive protoeukaryotes.The Cell: Organelles engage in bidirectional crosstalk essential for maintaining cellular homeostasisHomeostasisThe processes whereby the internal environment of an organism tends to remain balanced and stable.Cell Injury and Death. Dysfunction in either organelle can contribute to accumulation-related pathologies:
Impaired lysosomal acidification leads to ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements retention within lysosomesLysosomesA class of morphologically heterogeneous cytoplasmic particles in animal and plant tissues characterized by their content of hydrolytic enzymes and the structure-linked latency of these enzymes. The intracellular functions of lysosomes depend on their lytic potential. The single unit membrane of the lysosome acts as a barrier between the enzymes enclosed in the lysosome and the external substrate. The activity of the enzymes contained in lysosomes is limited or nil unless the vesicle in which they are enclosed is ruptured or undergoes membrane fusion.The Cell: Organelles, resulting in functional ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements deficiency.
Mitochondrial dysfunction promotes the buildup of damaged organellesOrganellesA cell is a complex unit that performs several complex functions. An organelle is a specialized subunit within a cell that fulfills a specific role or function. Organelles are enclosed within their own lipid bilayers or are unbound by membranes. The Cell: Organelles and oxidized proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis.
The PINK1/Parkin pathway regulates mitophagy; mutations in this pathway cause the accumulation of dysfunctional mitochondriaMitochondriaSemiautonomous, self-reproducing organelles that occur in the cytoplasm of all cells of most, but not all, eukaryotes. Each mitochondrion is surrounded by a double limiting membrane. The inner membrane is highly invaginated, and its projections are called cristae. Mitochondria are the sites of the reactions of oxidative phosphorylation, which result in the formation of ATP. They contain distinctive ribosomes, transfer RNAs; amino Acyl tRNA synthetases; and elongation and termination factors. Mitochondria depend upon genes within the nucleus of the cells in which they reside for many essential messenger RNAs. Mitochondria are believed to have arisen from aerobic bacteria that established a symbiotic relationship with primitive protoeukaryotes.The Cell: Organelles.
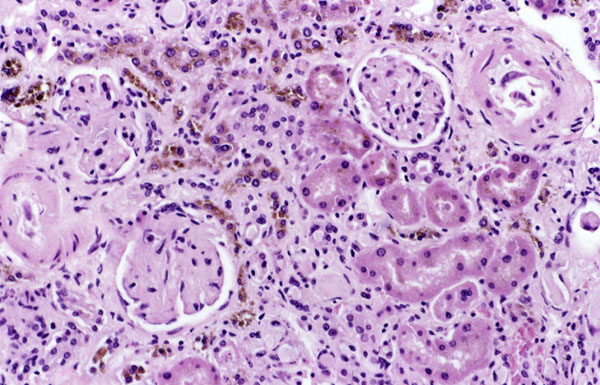
Brownish deposits from hemosiderin in the kidney
Image: “Hemosiderin” by National Institutes of Health. License: Public Domain
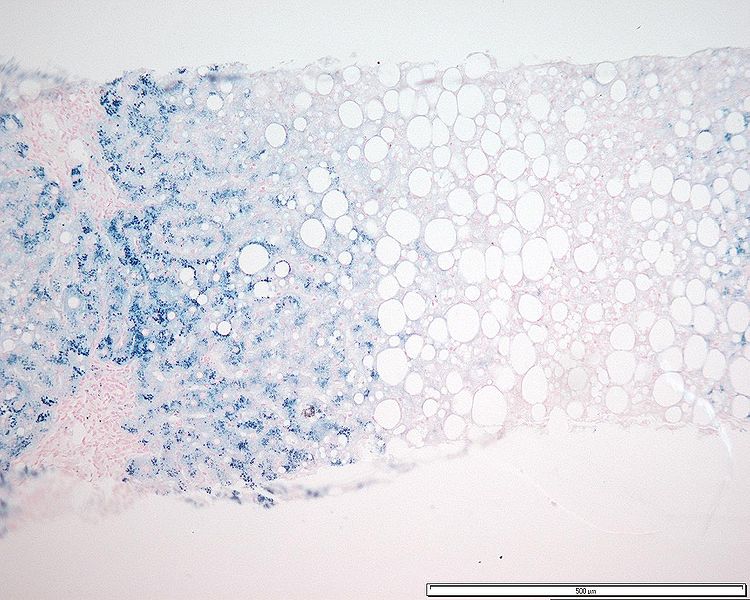
Histopathology of a liver with homozygous genetic hemochromatosis. The blue coloration of iron is seen after its histochemical reaction with Prussian blue dye.
Image: “Hemochromatosis acini” by BioMed Central Dermatology, Mathew, J. et al. License: CC BY 3.0
Orange-yellow compound produced from the breakdown of heme from RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology
Heme → biliverdinBiliverdin1, 3, 6, 7-tetramethyl-4, 5-dicarboxyethyl-2, 8-divinylbilenone. Biosynthesized from hemoglobin as a precursor of bilirubin.Heme Metabolism (“green bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy”) → bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism (“red bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy”)
Conjugated in the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy and excreted in bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy
JaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice: yellow discoloration of mucous membranes and skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions due to accumulation of bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism
Found in:
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy or biliary disease (conjugated bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism)
Hemolysis (unconjugated bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism)
Scleral icterus: the first clinical sign of bilirubin deposition in the body
Image: “Jaundice eye new” by CDC/Dr. Thomas F. Sellers/Emory University. License: Public Domain
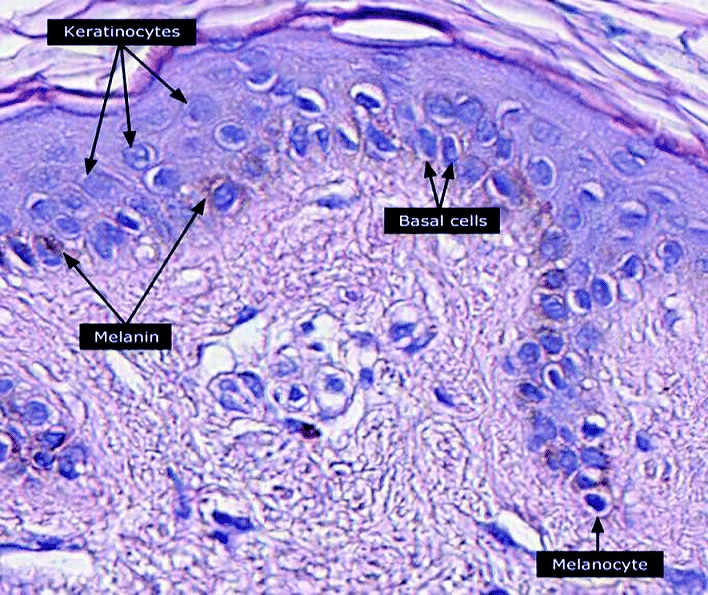
MelaninMelaninInsoluble polymers of tyrosine derivatives found in and causing darkness in skin (skin pigmentation), hair, and feathers providing protection against sunburn induced by sunlight. Carotenes contribute yellow and red coloration.Seborrheic Keratosis:
Brown-black pigment formed by melanocytesMelanocytesMammalian pigment cells that produce melanins, pigments found mainly in the epidermis, but also in the eyes and the hair, by a process called melanogenesis. Coloration can be altered by the number of melanocytes or the amount of pigment produced and stored in the organelles called melanosomes. The large non-mammalian melanin-containing cells are called melanophores.Skin: Structure and Functions and transferred to keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions
Main forms of melaninMelaninInsoluble polymers of tyrosine derivatives found in and causing darkness in skin (skin pigmentation), hair, and feathers providing protection against sunburn induced by sunlight. Carotenes contribute yellow and red coloration.Seborrheic Keratosis:
Eumelanin (brown/black): stronger shielding property against ultraviolet (UV) radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Pheomelanin (yellow/orange): less UV protection, produces free radicalsFree radicalsHighly reactive molecules with an unsatisfied electron valence pair. Free radicals are produced in both normal and pathological processes. They are proven or suspected agents of tissue damage in a wide variety of circumstances including radiation, damage from environment chemicals, and aging. Natural and pharmacological prevention of free radical damage is being actively investigated.Ischemic Cell Damage and contributes to oxidative stressOxidative stressA disturbance in the prooxidant-antioxidant balance in favor of the former, leading to potential damage. Indicators of oxidative stress include damaged DNA bases, protein oxidation products, and lipid peroxidation products.Cell Injury and Death
Neuromelanin: found in the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Clinical correlationCorrelationDetermination of whether or not two variables are correlated. This means to study whether an increase or decrease in one variable corresponds to an increase or decrease in the other variable.Causality, Validity, and Reliability:
BenignBenignFibroadenoma accumulations (frecklesFrecklesPrimary Skin Lesions, molesMolesPrimary Skin Lesions): nevusNevusNevi (singular nevus), also known as “moles,” are benign neoplasms of the skin. Nevus is a non-specific medical term because it encompasses both congenital and acquired lesions, hyper- and hypopigmented lesions, and raised or flat lesions. Nevus/Nevi
Light-skinned individuals or populations living further from the equator: richer pheomelanin, higher risk for carcinogenesisCarcinogenesisThe origin, production or development of cancer through genotypic and phenotypic changes which upset the normal balance between cell proliferation and cell death. Carcinogenesis generally requires a constellation of steps, which may occur quickly or over a period of many years.Carcinogenesis
Image shows a nevus, a benign, uniformly pigmented brown papule with dark color due to high concentration of melanin
Micrograph of epidermis showing the melanocytes, keratinocytes, and melanin
Image: “Micrograph of keratinocytes, basal cells and melanocytes in the epidermis” by Setijanti H.B. et al. License: CC BY 4.0
Calcium Accumulation
Metastatic calcification
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes deposition in normal or abnormal tissues due to hypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia
HypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia:
ParathyroidParathyroidThe parathyroid glands are 2 pairs of small endocrine glands found in close proximity to the thyroid gland. The superior parathyroid glands are lodged within the parenchyma of the upper poles of the right and left thyroid lobes; the inferior parathyroid glands are close to the inferior tips or poles of the lobes.Parathyroid Glands: Anatomy hormone (PTH) excess or hyperparathyroidismHyperparathyroidismHyperparathyroidism is a condition associated with elevated blood levels of parathyroid hormone (PTH). Depending on the pathogenesis of this condition, hyperparathyroidism can be defined as primary, secondary or tertiary. Hyperparathyroidism:
ParathyroidParathyroidThe parathyroid glands are 2 pairs of small endocrine glands found in close proximity to the thyroid gland. The superior parathyroid glands are lodged within the parenchyma of the upper poles of the right and left thyroid lobes; the inferior parathyroid glands are close to the inferior tips or poles of the lobes.Parathyroid Glands: Anatomy tumors
Secondary hyperparathyroidismSecondary hyperparathyroidismAbnormally elevated parathyroid hormone secretion as a response to hypocalcemia. It is caused by chronic kidney failure or other abnormalities in the controls of bone and mineral metabolism, leading to various bone diseases, such as renal osteodystrophy.Hyperparathyroidism from renal disease (due to phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes retention)
Resorption of boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types tissue:
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and TypesmetastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Increased boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types turnover (Paget’s disease)
Bone marrowBone marrowThe soft tissue filling the cavities of bones. Bone marrow exists in two types, yellow and red. Yellow marrow is found in the large cavities of large bones and consists mostly of fat cells and a few primitive blood cells. Red marrow is a hematopoietic tissue and is the site of production of erythrocytes and granular leukocytes. Bone marrow is made up of a framework of connective tissue containing branching fibers with the frame being filled with marrow cells.Bone Marrow: Composition and Hematopoiesis malignancies (multiple myeloma, leukemia)
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies disorders (vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies intoxication, sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis)
Affects acid-secreting cells (alkali environment predisposes to metastatic calcification):
Gastric mucosaGastric mucosaLining of the stomach, consisting of an inner epithelium, a middle lamina propria, and an outer muscularis mucosae. The surface cells produce mucus that protects the stomach from attack by digestive acid and enzymes. When the epithelium invaginates into the lamina propria at various region of the stomach (cardia; gastric fundus; and pylorus), different tubular gastric glands are formed. These glands consist of cells that secrete mucus, enzymes, hydrochloric acid, or hormones.Stomach: Anatomy
LungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
KidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy (nephrocalcinosisNephrocalcinosisA condition characterized by calcification of the renal tissue itself. It is usually seen in distal renal tubular acidosis with calcium deposition in the distal kidney tubules and the surrounding interstitium. Nephrocalcinosis causes renal insufficiency.X-linked Hypophosphatemic Rickets)
Systemic arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology
Pulmonary veinsPulmonary veinsThe veins that return the oxygenated blood from the lungs to the left atrium of the heart.Lungs: Anatomy
Dystrophic calcification
Deposition of calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes in abnormal (necrotic) tissues with normal calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes levels
Gross morphology: hard, yellowish granules or deposits
Microscopic morphology:
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes salts: basophilic, amorphous granular appearance
Psammoma bodies: concentric lamellated structures from calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes build-up (in papillary thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cancer, meningiomaMeningiomaMeningiomas are slow-growing tumors that arise from the meninges of the brain and spinal cord. The vast majority are benign. These tumors commonly occur in individuals with a history of high doses of skull radiation, head trauma, and neurofibromatosis 2. Meningioma, ovarian papillary serous cystadenocarcinoma)
Found in:
Blood vessels (atheromas of atherosclerosisAtherosclerosisAtherosclerosis is a common form of arterial disease in which lipid deposition forms a plaque in the blood vessel walls. Atherosclerosis is an incurable disease, for which there are clearly defined risk factors that often can be reduced through a change in lifestyle and behavior of the patient. Atherosclerosis)
Damaged heart valves
Aging
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., tuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis, toxoplasmosisToxoplasmosisToxoplasmosis is an infectious disease caused by Toxoplasma gondii, an obligate intracellular protozoan parasite. Felines are the definitive host, but transmission to humans can occur through contact with cat feces or the consumption of contaminated foods. The clinical presentation and complications depend on the host’s immune status. Toxoplasma/Toxoplasmosis)
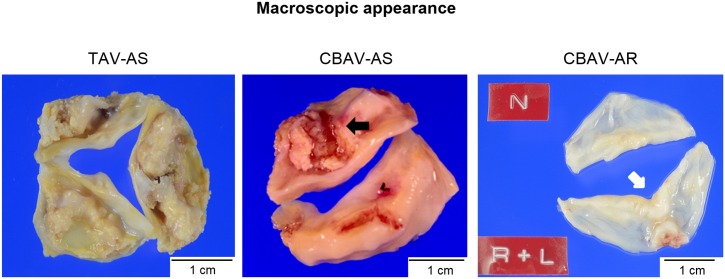
Images of excised aortic valves: First picture (left): tricuspid aortic valve stenosis (TAV-AS) illustrating calcifications (white-yellow deposits) with fused commissures. Second picture: congenital bicuspid aortic valve stenosis (CBAV-AS) with 2 calcified cusps with raphe (black arrow) and severe fibrous thickening. Third picture (right): congenital bicuspid aortic valve regurgitation (CBAV-AR); R (right coronary cusp) and L (left coronary cusp) are fused, with coaptation sites thicker than the other portions (white arrow).
Image: “Macroscopic appearance” by Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Osaka, Japan. License: CC BY 4.0
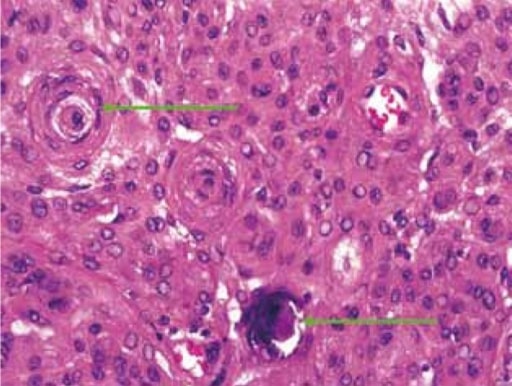
Histopathology illustrates psammoma bodies (green arrows) in meningioma
Image: “Histopathology Reveals Psammoma Bodies” by Department of Radiodiagnosis, Government Medical College, Nagpur Maharashtra, India. License: CC BY 2.5
Increased protein reabsorptionin the proximal renal tubule:
Affects kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy (proteinuriaProteinuriaThe presence of proteins in the urine, an indicator of kidney diseases.Nephrotic Syndrome in Children in nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome)
Abundant immunoglobulin synthesisSynthesisPolymerase Chain Reaction (PCR) in plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products cells → protein accumulation in the ER → Russell bodies
Increased cytoskeletal proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis:
CytoskeletonCytoskeletonThe network of filaments, tubules, and interconnecting filamentous bridges which give shape, structure, and organization to the cytoplasm.The Cell: Cytosol and CytoskeletonproteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis:
Support the plasma membranePlasma membraneA cell membrane (also known as the plasma membrane or plasmalemma) is a biological membrane that separates the cell contents from the outside environment. A cell membrane is composed of a phospholipid bilayer and proteins that function to protect cellular DNA and mediate the exchange of ions and molecules.The Cell: Cell Membrane and the organization of organellesOrganellesA cell is a complex unit that performs several complex functions. An organelle is a specialized subunit within a cell that fulfills a specific role or function. Organelles are enclosed within their own lipid bilayers or are unbound by membranes. The Cell: Organelles
MicrotubulesMicrotubulesSlender, cylindrical filaments found in the cytoskeleton of plant and animal cells. They are composed of the protein tubulin and are influenced by tubulin modulators.The Cell: Cytosol and Cytoskeleton, actinActinFilamentous proteins that are the main constituent of the thin filaments of muscle fibers. The filaments (known also as filamentous or f-actin) can be dissociated into their globular subunits; each subunit is composed of a single polypeptide 375 amino acids long. This is known as globular or g-actin. In conjunction with myosins, actin is responsible for the contraction and relaxation of muscle.Skeletal Muscle Contraction filaments, myosinMyosinA diverse superfamily of proteins that function as translocating proteins. They share the common characteristics of being able to bind actins and hydrolyze mgATP. Myosins generally consist of heavy chains which are involved in locomotion, and light chains which are involved in regulation. Within the structure of myosin heavy chain are three domains: the head, the neck and the tail. The head region of the heavy chain contains the actin binding domain and mgATPase domain which provides energy for locomotion. The neck region is involved in binding the light-chains. The tail region provides the anchoring point that maintains the position of the heavy chain. The superfamily of myosins is organized into structural classes based upon the type and arrangement of the subunits they contain.Skeletal Muscle Contraction filaments, or intermediate filamentsIntermediate filamentsCytoplasmic filaments intermediate in diameter (about 10 nanometers) between the microfilaments and the microtubules. They may be composed of any of a number of different proteins and form a ring around the cell nucleus.The Cell: Cytosol and Cytoskeleton
Found in:
Alzheimer’s disease: One of the hallmarks is neurofibrillary tangle (microtubule-associated tau proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis).
AlcoholicAlcoholicPersons who have a history of physical or psychological dependence on ethanol.Mallory-Weiss Syndrome (Mallory-Weiss Tear)liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease: has alcoholicAlcoholicPersons who have a history of physical or psychological dependence on ethanol.Mallory-Weiss Syndrome (Mallory-Weiss Tear) hyaline or Mallory hyaline, a cytoplasmic inclusion (made of keratinKeratinA class of fibrous proteins or scleroproteins that represents the principal constituent of epidermis; hair; nails; horny tissues, and the organic matrix of tooth enamel. Two major conformational groups have been characterized, alpha-keratin, whose peptide backbone forms a coiled-coil alpha helical structure consisting of type I keratin and a type II keratin, and beta-keratin, whose backbone forms a zigzag or pleated sheet structure. Alpha-keratins have been classified into at least 20 subtypes. In addition multiple isoforms of subtypes have been found which may be due to gene duplication.Seborrheic Keratosisintermediate filamentsIntermediate filamentsCytoplasmic filaments intermediate in diameter (about 10 nanometers) between the microfilaments and the microtubules. They may be composed of any of a number of different proteins and form a ring around the cell nucleus.The Cell: Cytosol and Cytoskeleton)
ɑ-1 antitrypsin deficiency: Genetic mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations leads to misfolding of ɑ-1antitrypsin.
Abnormal ɑ-1antitrypsin accumulates in the ER of the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy → cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
Lack of functional ɑ-1antitrypsin → alveolar damage in the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
Abnormal proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis (protein aggregationAggregationThe attachment of platelets to one another. This clumping together can be induced by a number of agents (e.g., thrombin; collagen) and is part of the mechanism leading to the formation of a thrombus.Coagulation Studies diseases):
Form complex interactions with other proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis in neurodegenerative disorders
Often involve impaired qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement control systems, such as the ubiquitin-proteasome system and autophagyAutophagyThe segregation and degradation of various cytoplasmic constituents via engulfment by multivesicular bodies; vacuoles; or autophagosomes and their digestion by lysosomes. It plays an important role in biological metamorphosis and in the removal of bone by osteoclasts. Defective autophagy is associated with various diseases, including neurodegenerative diseases and cancer.Cellular Adaptation
AmyloidosisAmyloidosisAmyloidosis is a disease caused by abnormal extracellular tissue deposition of fibrils composed of various misfolded low-molecular-weight protein subunits. These proteins are frequently byproducts of other pathological processes (e.g., multiple myeloma). Amyloidosis:
Extracellular deposition of amyloid, an insoluble fibrillar protein
Amyloid stains pink or red in Congo red stain and apple-green birefringence under polarized light.
Multiple Proteinopathy Interactions
Recent evidence suggests that pathological proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis can interact and influence each other’s aggregationAggregationThe attachment of platelets to one another. This clumping together can be induced by a number of agents (e.g., thrombin; collagen) and is part of the mechanism leading to the formation of a thrombus.Coagulation Studies:
Tau and amyloid-β co-aggregate at synapses in Alzheimer’s disease, enhancing neurotoxicity.
α-synuclein and tau show cross-seeding capabilities in Parkinson’s disease and related disorders.
Co-occurring proteinopathies are more common with aging and are associated with the APOE4 genotypeGenotypeThe genetic constitution of the individual, comprising the alleles present at each genetic locus.Basic Terms of Genetics.
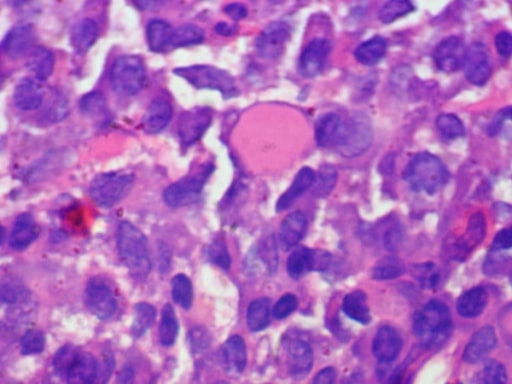
Photomicrograph of bone biopsy (multiple myeloma): sheet of plasma cells with a prominent large Russell body (homogeneous eosinophilic inclusion)
Image: “Russell body” by Department of Pathology, Dr, Ram Manohar Lohia Hospital, New Delhi, India. License: CC BY 2.0
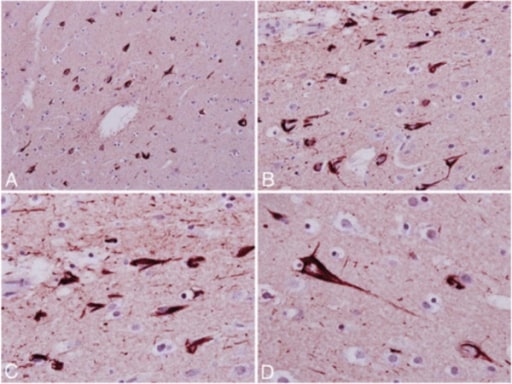
Photomicrographs of chronic traumatic encephalopathy that show tau-immunostained section of the frontal cortex with neurofibrillary tangles and neuritic threads (A and B). Higher magnification (C and D) shows band- and flame-shaped neurofibrillary tangles.
Image: “Index case of military CTE” by Departments of Neurology, Icahn School of Medicine at Mount Sinai, One Gustave L Levy Place, New York, NY 10029, USA. License: CC BY 2.0
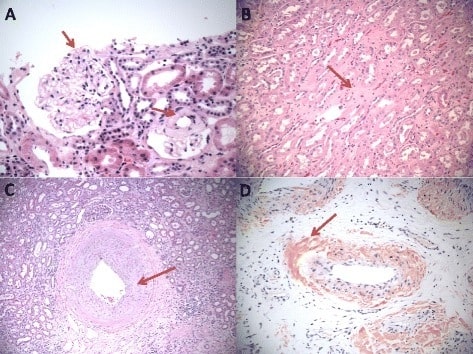
Amyloid deposits in the kidney under hematoxylin and eosin stain: A. Glomerular amyloid deposits in mesangial spaces (red arrow). B. Interstitial amyloidosis (red arrow). C. Vascular amyloidosis (red arrow). D. Congo red stain of vascular amyloid deposits (red arrow).
Image: “Amyloid deposits in the three major compartments of the kidney” by Department of Pathology, Yale University School of Medicine, New Haven, CT, USA. License: CC BY 4.0
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy (major organ for fat metabolism)
Kidney
Heart
Skeletal muscle
Found in:
Fatty liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy: associated with alcohol use disorderAlcohol use disorderAlcohol is one of the most commonly used addictive substances in the world. Alcohol use disorder (AUD) is defined as pathologic consumption of alcohol leading to impaired daily functioning. Acute alcohol intoxication presents with impairment in speech and motor functions and can be managed in most cases with supportive care. Alcohol Use Disorder and non-alcoholic steatotic liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Others: toxin injury, diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus, anoxia, obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity, metabolic syndromeMetabolic syndromeMetabolic syndrome is a cluster of conditions that significantly increases the risk for several secondary diseases, notably cardiovascular disease, type 2 diabetes, and nonalcoholic fatty liver. In general, it is agreed that hypertension, insulin resistance/hyperglycemia, and hyperlipidemia, along with central obesity, are components of the metabolic syndrome. Metabolic Syndrome, metabolic dysfunction-associated steatotic liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease (MASLD, formerly Non-alcoholic fatty liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease, NAFLD)
Gross morphology: yellow discoloration of the organ
Microscopic morphology:
Vacuoles of lipidic content within the cells
Vacuoles have well-defined edges.
CholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism
Accumulates in phagocytic cells due to lipid overload
Microscopic morphology: intracellular vacuoles
Found in:
AtherosclerosisAtherosclerosisAtherosclerosis is a common form of arterial disease in which lipid deposition forms a plaque in the blood vessel walls. Atherosclerosis is an incurable disease, for which there are clearly defined risk factors that often can be reduced through a change in lifestyle and behavior of the patient. Atherosclerosis
Atherosclerotic plaquePlaquePrimary Skin Lesions: accumulation of cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism, seen as vacuoles, in the intimal smooth muscle cells and macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation
Plaques or nodules from intracellular cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism in the subepithelialSubepithelialMembranoproliferative Glomerulonephritisconnective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and tendons
Found in altered lipid metabolismLipid MetabolismLipid metabolism is the processing of lipids for energy use, energy storage, and structural component production. Lipid metabolism uses fats from dietary sources or from fat stores in the body. A complex series of processes involving digestion, absorption, and transport are required for the proper metabolism of lipids. Lipid Metabolism
Cholesterolosis
Cholesterol-laden macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation or foam cellsFoam cellsLipid-laden macrophages originating from monocytes or from smooth muscle cells.Atherosclerosis in the lamina propriaLamina propriaWhipple’s Disease of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
Frequently coexists with cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol MetabolismgallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
Niemann-Pick diseaseNiemann-Pick diseaseNiemann-Pick disease (NPD) is a rare, inherited, lysosomal storage disorder. The disease is classified on the basis of the genetic mutation. Type A and type B result from mutations in the SMPD-1 gene, resulting in acid sphingomyelinase enzyme deficiency. Type C results from NPC1 or NPC2 gene mutations, which are needed for intracellular transport of lipids.Niemann-Pick Disease, type C
Autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritancelysosomal storage diseaseLysosomal storage diseaseLysosomal storage diseases are a group of metabolic disorders caused by genetic mutations in the enzymes responsible for normal lysosomal function. The dysfunction of enzymatic processes causes an accumulation of undigested metabolites, resulting in cellular death. The main groups include sphingolipidoses, oligosaccharidoses, and mucolipidoses. Overview of Lysosomal Storage Diseases due to mutations in either NPC1 or NPC2
Impaired cholesterolCholesterolThe principal sterol of all higher animals, distributed in body tissues, especially the brain and spinal cord, and in animal fats and oils.Cholesterol Metabolism transport out of the lysosome
Xanthelasma palpebrarum, a type of xanthoma, affecting the upper and lower eyelids
Image: “ File:Xanthelasma” by Klaus D. Peter. License: CC BY 3.0
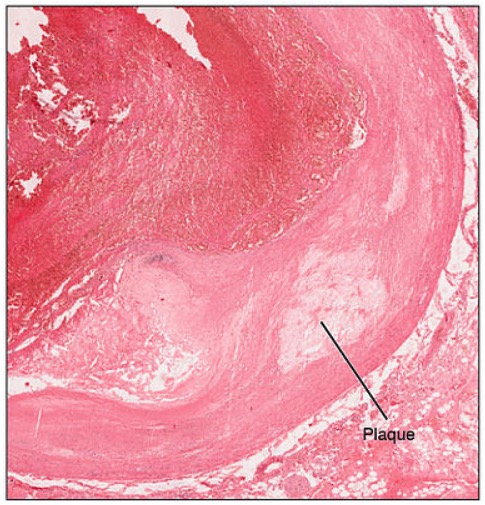
Cross-section of a blood vessel showing an atherosclerotic plaque in its wall
Image: “Atherosclerosis” by OpenStax College. License: CC BY 3.0
PhospholipidsPhospholipidsLipids containing one or more phosphate groups, particularly those derived from either glycerol (phosphoglycerides) or sphingosine (sphingolipids). They are polar lipids that are of great importance for the structure and function of cell membranes and are the most abundant of membrane lipids, although not stored in large amounts in the system.Lipid Metabolism
Released from damaged cell membranes in cell injuryCell injuryThe cell undergoes a variety of changes in response to injury, which may or may not lead to cell death. Injurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Cell Injury and Death
Myelin figuresMyelin figuresLarge whorled phospholipid precipitates (from the damaged membrane), which are phagocytosed or degraded to fatty acidsCell Injury and Death (whorled phospholipidsPhospholipidsLipids containing one or more phosphate groups, particularly those derived from either glycerol (phosphoglycerides) or sphingosine (sphingolipids). They are polar lipids that are of great importance for the structure and function of cell membranes and are the most abundant of membrane lipids, although not stored in large amounts in the system.Lipid Metabolism):
Accumulate in the cytosolCytosolA cell’s cytoskeleton is a network of intracellular protein fibers that provides structural support, anchors organelles, and aids intra- and extracellular movement.The Cell: Cytosol and Cytoskeleton
Degraded into fatty acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance or phagocytosed when the cell dies
Glycogen Accumulation
Glycogen: normally stored in the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy and skeletal musclesSkeletal musclesA subtype of striated muscle, attached by tendons to the skeleton. Skeletal muscles are innervated and their movement can be consciously controlled. They are also called voluntary muscles.Muscle Tissue: Histology
Excessive glycogen deposits within cells found in:
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance metabolism abnormalities (diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus, insulin resistanceInsulin resistanceDiminished effectiveness of insulin in lowering blood sugar levels: requiring the use of 200 units or more of insulin per day to prevent hyperglycemia or ketosis.Diabetes Mellitus)
Glycogen storage diseasesGlycogen Storage DiseasesA group of inherited metabolic disorders involving the enzymes responsible for the synthesis and degradation of glycogen. In some patients, prominent liver involvement is presented. In others, more generalized storage of glycogen occurs, sometimes with prominent cardiac involvement.Benign Liver Tumors (GSDs):
Over 15 distinct types with specific enzyme deficiencies
Most GSDs result from pathogenic variants in genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure that encode enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes involved in glycogen synthesisSynthesisPolymerase Chain Reaction (PCR), degradation, or regulation
Clinical presentations vary by type, ranging from hepatomegaly and hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia to myopathyMyopathyDermatomyositis, cardiomyopathyCardiomyopathyCardiomyopathy refers to a group of myocardial diseases associated with structural changes of the heart muscles (myocardium) and impaired systolic and/or diastolic function in the absence of other heart disorders (coronary artery disease, hypertension, valvular disease, and congenital heart disease). Cardiomyopathy: Overview and Types, and neurodevelopmental abnormalities
Microscopic morphology:
Glycogen: clear vacuoles in the cytoplasm
Rose-to-violet color when stained with Best’s carmine or PAS (periodic acid-Schiff) reaction
Diastase removes glycogen from the histologic section.
Affected organs: liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, heart, skeletal muscle, kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy, and pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
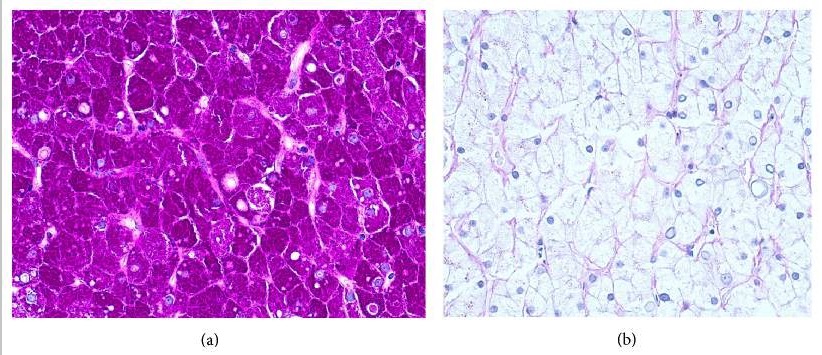
Liver biopsy: (a) Periodic Acid-Schiff stain-positive for glycogen accumulation (rose-violet color) (b) Glycogen abolishes after pretreatment with diastase.
Image: “Liver Biopsy” by US National Library of Medicine. License: CC BY 4.0
Hyaline Change
Description
Not a pattern of accumulation but a histologic finding also seen in various retained substances
Can be intra- or extracellular
Microscopic morphology: glassy, homogeneousHomogeneousImaging of the Spleen pink appearance in the cell (hematoxylin and eosin stain)
Due to leakage of plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsproteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis and deposition of concentric extracellular material
Seen in hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension and diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
From hepatocyte apoptosisApoptosisA regulated cell death mechanism characterized by distinctive morphologic changes in the nucleus and cytoplasm, including the endonucleolytic cleavage of genomic DNA, at regularly spaced, internucleosomal sites, I.e., DNA fragmentation. It is genetically-programmed and serves as a balance to mitosis in regulating the size of animal tissues and in mediating pathologic processes associated with tumor growth.Ischemic Cell Damage (cell shrinkage, pyknosisPyknosisIschemic Cell Damage, karyorrhexisKaryorrhexisIschemic Cell Damage, and cellular fragmentationFragmentationChronic Apophyseal Injury)
Seen in yellow feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, hepatitis
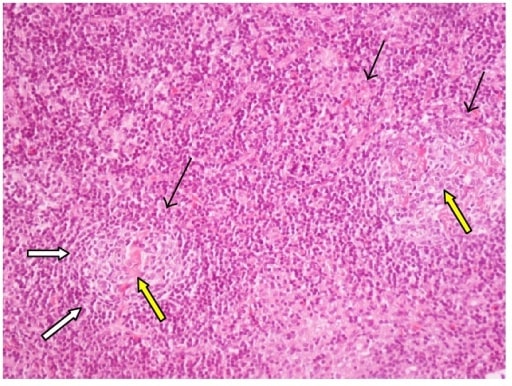
Lymph node biopsy (hematoxylin and eosin stain): 2 follicles with hyaline-vascular changes (yellow arrow), regressed germinal centers (black arrows) surrounded by concentric layers of small lymphocytes (white arrows)
Image: “Castleman’s Disease” by 1st Department of Internal Medicine and Diabetes Center, Tzaneio General Hospital of Piraeus, 18536 Piraeus, Greece. License: CC BY 4.0
References
Albores-Saavedra, J., & Angeles-Angeles, A. (2011). Diseases of the gallbladder. In A. Burt, B. Portmann, & L. Ferrell (Eds.), MacSween’s Pathology of the Liver (6th ed.). Elsevier, Inc.
Nasti, T., & Timares, L. (2015). MC1R, Eumelanin and Pheomelanin: Their role in determining the susceptibility to skin cancer. Photochemistry and Photobiology, 91(1), 188–200. https://doi.org/10.1111/php.12335
Oakes, S. (2020). Cell injury, cell death and adaptation. In V. Kumar, A. Abbas, J. Aster, & S. Robbins, Robbins and Cotran Pathologic Basis of Disease (10th ed., pp. 33–65, 83). Elsevier, Inc.
Seo, A. Y., Xu, J., Servais, S., Hofer, T., Marzetti, E., Wohlgemuth, S. E., Knutson, M. D., Chung, H. Y., & Leeuwenburgh, C. (2008). Mitochondrial iron accumulation with age and functional consequences. Aging cell, 7(5), 706–716. https://doi.org/10.1111/j.1474-9726.2008.00418.x
Kaushik, S., Tasset, I., Arias, E., Pampliega, O., Wong, E., Martinez-Vicente, M., & Cuervo, A. M. (2021). Autophagy and the hallmarks of aging. Ageing Research Reviews, 72, Article 101468. https://doi.org/10.1016/j.arr.2021.101468
Goldman, L., & Schafer, A. I. (2024). Goldman-Cecil medicine (27th ed.). Elsevier.
Kobayashi, T., Iwaki, M., Nakajima, A., Nogami, A., & Yoneda, M. (2022). Current research on the pathogenesis of MASLD/MASH and the gut-liver axis: Gut microbiota, dysbiosis, and leaky-gut syndrome. International Journal of Molecular Sciences, 23(19), Article 11689. https://doi.org/10.3390/ijms231911689
Zhang, L., Yang, J., Deng, Y., Deng, W., & Li, L. (2023). Computational profiling and prognostic modeling based on lysosome-related genes in colorectal cancer. Frontiers in Genetics, 14, Article 1203035. https://doi.org/10.3389/fgene.2023.1203035
Create your free account or log in to continue reading!