Renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (RTA) is an imbalance in physiologic pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance caused by the kidney’s inability to acidify urine to maintain blood pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance at physiologic levels. Renal tubular acidoses exist in multiple types, including distal RTA (type 1Type 1Spinal Muscular Atrophy), proximal RTA (type 2), mixed RTA (type 3Type 3Spinal Muscular Atrophy), and hyperkalemic RTA (type 4Type 4Spinal Muscular Atrophy). Depending on the type of RTA, various mechanisms cause dysfunction of renal acid–base handling, resulting in a non–anion-gap metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis. All RTAs present clinically with some degree of metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis; however, distal RTA and proximal RTA also have hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, while hyperkalemic RTA does not. Diagnosis is primarily through the history and laboratory analysis, including measurement of serum and urine anion gaps. Treatment involves the correction of chronic metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis with alkali to prevent its long-term catabolic effects on boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and muscles, as well as addressing any underlying causes leading to the condition.
Renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (RTA) is an imbalance in physiologic pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance caused by the kidney’s inability to acidify urine to maintain blood pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance at physiologic levels.
Classification
RTA can be classified based on the clinical characteristics and physiologic defect:
Urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance > 5.3
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products HCO3–variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Table: Type 2 RTA (proximal)—impaired bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.ElectrolytessecretionSecretionCoagulation Studies
Characteristics
Impaired proximal HCO3 reabsorption
Urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base BalancevariableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products HCO3– 12–20 mM/L
Renal defect
Nonspecific tubule dysfunction or mutations in genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure involved in HCO3– reabsorption
Etiology
Familial
Fanconi syndrome
Drugs, toxins
Carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors inhibitors
Inherited mutations in carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors II
Very rare
Presents in infants and children
Renal defect
Inherited mutations in carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors II
Most cases reported in North Africa, in areas with high prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of consanguinityConsanguinityThe magnitude of inbreeding in humans.Basic Terms of Genetics
Table: Type 4Type 4Spinal Muscular Atrophy RTA (hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism)—impaired acid secretionSecretionCoagulation Studies
Characteristics
Impaired aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia release or response
Urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance < 5.3
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products HCO3– > 17 mM/L
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Renal defect
Impaired Na+ reabsorption via epithelial Na+ channel
Etiology
Congenital hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism (Addison disease)
Aldosterone resistanceAldosterone resistanceA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism
Diabetic nephropathyDiabetic nephropathyKidney injuries associated with diabetes mellitus and affecting kidney glomerulus; arterioles; kidney tubules; and the interstitium. Clinical signs include persistent proteinuria, from microalbuminuria progressing to albuminuria of greater than 300 mg/24 h, leading to reduced glomerular filtration rate and end-stage renal disease.Chronic Diabetic Complications
Most commonly caused by diabetic nephropathyDiabetic nephropathyKidney injuries associated with diabetes mellitus and affecting kidney glomerulus; arterioles; kidney tubules; and the interstitium. Clinical signs include persistent proteinuria, from microalbuminuria progressing to albuminuria of greater than 300 mg/24 h, leading to reduced glomerular filtration rate and end-stage renal disease.Chronic Diabetic Complications
Leading to hyporeninemic hypoaldosteronismHyporeninemic hypoaldosteronismReduced aldosterone synthesis due to decreased stimulation of Renin-angiotensin-aldosterone system.Hypoaldosteronism and urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy obstruction
RTA associated with medication usage is increasing in incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
Transplant medications (20% incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of hyperkalemic RTA in renal transplants)
Etiology
Distal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 1Type 1Spinal Muscular Atrophy)
Systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus
HypercalciuriaHypercalciuriaExcretion of abnormally high level of calcium in the urine, greater than 4 mg/kg/day.Nephrolithiasis:
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies intoxication
HyperparathyroidismHyperparathyroidismHyperparathyroidism is a condition associated with elevated blood levels of parathyroid hormone (PTH). Depending on the pathogenesis of this condition, hyperparathyroidism can be defined as primary, secondary or tertiary. Hyperparathyroidism
SarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance or autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance:
Marfan syndromeMarfan syndromeMarfan syndrome is a genetic condition with autosomal dominant inheritance. Marfan syndrome affects the elasticity of connective tissues throughout the body, most notably in the cardiovascular, ocular, and musculoskeletal systems. Marfan Syndrome
Ehlers-Danlos syndromeEhlers-Danlos syndromeEhlers-Danlos syndrome (EDS) is a heterogeneous group of inherited connective tissue disorders that are characterized by hyperextensible skin, hypermobile joints, and fragility of the skin and connective tissue. Ehlers-Danlos Syndrome
Sickle cell diseaseSickle cell diseaseSickle cell disease (SCD) is a group of genetic disorders in which an abnormal Hb molecule (HbS) transforms RBCs into sickle-shaped cells, resulting in chronic anemia, vasoocclusive episodes, pain, and organ damage.Sickle Cell Disease
Congenital obstruction of the urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy
Other causes:
Drugs:
LithiumLithiumAn element in the alkali metals family. It has the atomic symbol li, atomic number 3, and atomic weight [6. 938; 6. 997]. Salts of lithium are used in treating bipolar disorder.Ebstein’s Anomaly
Amphotericin BAmphotericin BMacrolide antifungal antibiotic produced by streptomyces nodosus obtained from soil of the orinoco river region of venezuela.Polyenes
Wilson diseaseWilson diseaseWilson disease (hepatolenticular degeneration) is an autosomal recessive disorder caused by various mutations in the ATP7B gene, which regulates copper transport within hepatocytes. Dysfunction of this transport mechanism leads to abnormal copper accumulations in the liver, brain, eyes, and other organs, with consequent major and variably expressed hepatic, neurologic, and psychiatric disturbances. Wilson Disease
Nephrocalcinosis:
Calcium deposits are visible in the kidneys in cases of hypercalciuria. This condition can arise from multiple causes, including hyperparathyroidism, vitamin D intoxication, and sarcoidosis and can result in type 1 renal tubular acidosis.
Proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 2)
In adults, the most common cause is monoclonal gammopathyMonoclonal gammopathyConditions characterized by the presence of m protein (monoclonal protein) in serum or urine without clinical manifestations of plasma cell dyscrasia.MALT Lymphoma:
Multiple myeloma
AmyloidosisAmyloidosisAmyloidosis is a disease caused by abnormal extracellular tissue deposition of fibrils composed of various misfolded low-molecular-weight protein subunits. These proteins are frequently byproducts of other pathological processes (e.g., multiple myeloma). Amyloidosis
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance or autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance
Apical Na+/H+antiporterAntiporterMembrane transporters that co-transport two or more dissimilar molecules in the opposite direction across a membrane. Usually the transport of one ion or molecule is against its electrochemical gradient and is ‘powered’ by the movement of another ion or molecule with its electrochemical gradient.The Cell: Cell Membrane of the proximal tubular cells
Basolateral Na+/HCO3– cotransporter of proximal tubular cells
Drugs:
Heavy metals (lead, mercury)
Carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors inhibitors (such as acetazolamideAcetazolamideOne of the carbonic anhydrase inhibitors that is sometimes effective against absence seizures. It is sometimes useful also as an adjunct in the treatment of tonic-clonic, myoclonic, and atonic seizures, particularly in women whose seizures occur or are exacerbated at specific times in the menstrual cycle. However, its usefulness is transient often because of rapid development of tolerance. Its antiepileptic effect may be due to its inhibitory effect on brain carbonic anhydrase, which leads to an increased transneuronal chloride gradient, increased chloride current, and increased inhibition.Carbonic Anhydrase Inhibitors, topiramateTopiramateA sulfamate-substituted fructose analog that was originally identified as a hypoglycemic agent. It is used for the treatment of epilepsy and migraine disorders, and may also promote weight loss.Second-Generation Anticonvulsant Drugs)
AminoglycosidesAminoglycosidesAminoglycosides are a class of antibiotics including gentamicin, tobramycin, amikacin, neomycin, plazomicin, and streptomycin. The class binds the 30S ribosomal subunit to inhibit bacterial protein synthesis. Unlike other medications with a similar mechanism of action, aminoglycosides are bactericidal. Aminoglycosides
Antiretrovirals (specifically, tenofovirTenofovirAn adenine analog reverse transcriptase inhibitor with antiviral activity against HIV-1 and hepatitis b. It is used to treat HIV infections and chronic hepatitis b, in combination with other antiviral agents, due to the emergence of antiviral drug resistance when it is used alone.Anti-HIV Drugs)
CisplatinCisplatinAn inorganic and water-soluble platinum complex. After undergoing hydrolysis, it reacts with DNA to produce both intra and interstrand crosslinks. These cross links appear to impair replication and transcription of DNA. The cytotoxicity of cisplatin correlates with cellular arrest in the g2 phase of the cell cycle.Alkylating Agents and Platinum, oxaliplatinOxaliplatinAn organoplatinum complex in which the platinum atom is complexed with 1, 2-diaminocyclohexane, and with an oxalate ligand which is displaced to yield active oxaliplatin derivatives. These derivatives form inter- and intra-strand DNA crosslinks that inhibit DNA replication and transcription. Oxaliplatin is an antineoplastic agent that is often administered with fluorouracil and folinic acid in the treatment of metastatic colorectal neoplasms.Alkylating Agents and Platinum
Valproic acidValproic acidA fatty acid with anticonvulsant and anti-manic properties that is used in the treatment of epilepsy and bipolar disorder. The mechanisms of its therapeutic actions are not well understood. It may act by increasing gamma-aminobutyric acid levels in the brain or by altering the properties of voltage-gated sodium channels.First-Generation Anticonvulsant Drugs
Miscellaneous:
Interstitial nephritis
Vitamin D deficiencyVitamin D DeficiencyA nutritional condition produced by a deficiency of vitamin D in the diet, insufficient production of vitamin D in the skin, inadequate absorption of vitamin D from the diet, or abnormal conversion of vitamin D to its bioactive metabolites. It is manifested clinically as rickets in children and osteomalacia in adults.Fat-soluble Vitamins and their Deficiencies
Secondary hyperparathyroidismSecondary hyperparathyroidismAbnormally elevated parathyroid hormone secretion as a response to hypocalcemia. It is caused by chronic kidney failure or other abnormalities in the controls of bone and mineral metabolism, leading to various bone diseases, such as renal osteodystrophy.Hyperparathyroidism
Kidney transplant
Other diseases associated with Fanconi syndrome:
Tyrosinemia
Cystinosis
GalactosemiaGalactosemiaGalactosemia is a disorder caused by defects in galactose metabolism. Galactosemia is an inherited, autosomal-recessive condition, which results in inadequate galactose processing and high blood levels of monosaccharide. The rare disorder often presents in infants with symptoms of lethargy, nausea, vomiting, diarrhea, and jaundice. Galactosemia
Hereditary fructose intoleranceHereditary fructose intoleranceAn autosomal recessive fructose metabolism disorder due to deficient fructose-1-phosphate aldolase activity, resulting in accumulation of fructose-1-phosphate. The accumulated fructose-1-phosphate inhibits glycogenolysis and gluconeogenesis, causing severe hypoglycemia following ingestion of fructose. Prolonged fructose ingestion in infants leads ultimately to hepatic failure and death. Patients develop a strong distaste for sweet food, and avoid a chronic course of the disease by remaining on a fructose- and sucrose-free diet.Disorders of Fructose Metabolism
von Gierke disease (glycogen storage diseaseGlycogen storage diseaseA group of inherited metabolic disorders involving the enzymes responsible for the synthesis and degradation of glycogen. In some patients, prominent liver involvement is presented. In others, more generalized storage of glycogen occurs, sometimes with prominent cardiac involvement.Benign Liver Tumors type I)
Wilson diseaseWilson diseaseWilson disease (hepatolenticular degeneration) is an autosomal recessive disorder caused by various mutations in the ATP7B gene, which regulates copper transport within hepatocytes. Dysfunction of this transport mechanism leads to abnormal copper accumulations in the liver, brain, eyes, and other organs, with consequent major and variably expressed hepatic, neurologic, and psychiatric disturbances. Wilson Disease
Lowe disease
Paroxysmal nocturnal hemoglobinuriaHemoglobinuriaThe presence of free hemoglobin in the urine, indicating hemolysis of erythrocytes within the vascular system. After saturating the hemoglobin-binding proteins (haptoglobins), free hemoglobin begins to appear in the urine.Transfusion Reactions
Mixed renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 3Type 3Spinal Muscular Atrophy)
No cases reported in adults.
In children, the most common cause is carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors II deficiency.
Hyperkalemic renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 4Type 4Spinal Muscular Atrophy)
In adults, the most common causes are:
Diabetic nephropathyDiabetic nephropathyKidney injuries associated with diabetes mellitus and affecting kidney glomerulus; arterioles; kidney tubules; and the interstitium. Clinical signs include persistent proteinuria, from microalbuminuria progressing to albuminuria of greater than 300 mg/24 h, leading to reduced glomerular filtration rate and end-stage renal disease.Chronic Diabetic Complications
Interstitial nephritis
Mild-to-moderate CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
Other causes:
Genetic:
Sickle cell diseaseSickle cell diseaseSickle cell disease (SCD) is a group of genetic disorders in which an abnormal Hb molecule (HbS) transforms RBCs into sickle-shaped cells, resulting in chronic anemia, vasoocclusive episodes, pain, and organ damage.Sickle Cell Disease
PseudohypoaldosteronismPseudohypoaldosteronismA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism
Calcineurin inhibitorsCalcineurin InhibitorsCompounds that inhibit or block the phosphatase activity of calcineurin.Immunosuppressants (cyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants, tacrolimusTacrolimusA macrolide isolated from the culture broth of a strain of streptomyces tsukubaensis that has strong immunosuppressive activity in vivo and prevents the activation of T-lymphocytes in response to antigenic or mitogenic stimulation in vitro.Immunosuppressants)
Angiotensin-converting–enzyme inhibitors (ACEisACEIsA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Heart Failure and Chronic Coronary Syndrome Medication)
ReninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation inhibitors
Heparin
TrimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim
Pentamidine
Miscellaneous:
Chronic obstruction of the urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy
Primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Critical illness
Pathophysiology
Distal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 1Type 1Spinal Muscular Atrophy)
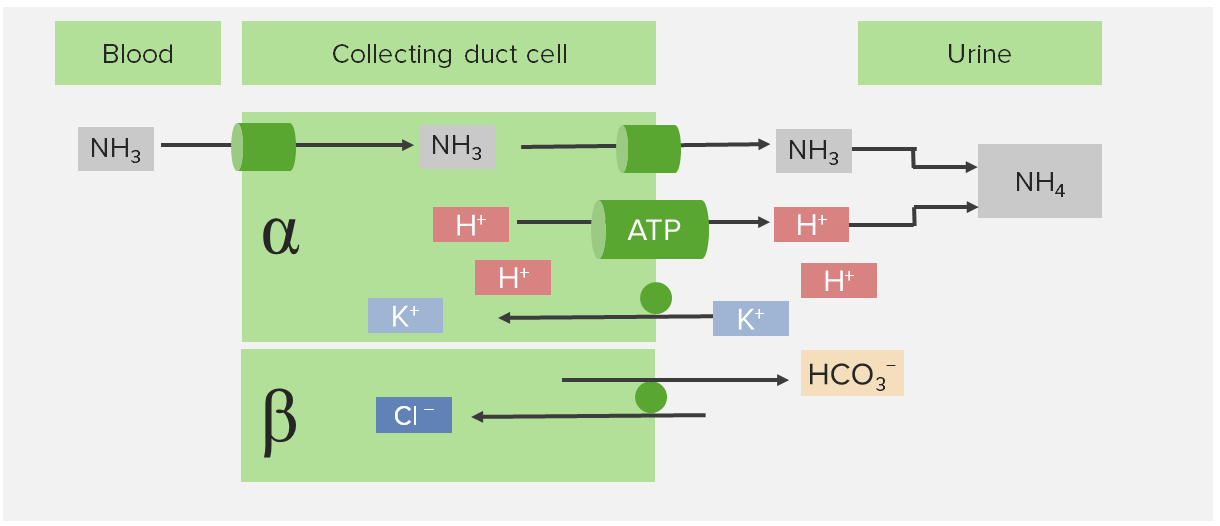
The pathophysiology of distal RTA (type 1Type 1Spinal Muscular Atrophy) is impaired acid secretionSecretionCoagulation Studies at the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma of the distal tubule.
Located at the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma of the distal tubule
α-intercalated cell:
Apical H+/K+-ATPase (1 H+ out of cell, 1 K+ into cell)
Apical H+-ATPase (1 H+ out of cell)
Basolateral Na+/K+-ATPase
Basolateral Cl–/HCO3– exchanger
β-intercalated cell:
Apical Cl–/HCO3– exchanger (1 HCO3– out of cell, 1 Cl– into cell)
Apical H+/K+-ATPase (1 H+ out of cell, 1 K+ into cell)
H+ combine with NH3+ (ammoniaAmmoniaA colorless alkaline gas. It is formed in the body during decomposition of organic materials during a large number of metabolically important reactions. Note that the aqueous form of ammonia is referred to as ammonium hydroxide.Acid-Base Balance) and other compounds (titratable acidsTitratable acidsAcid-Base Balance)
Acid–base homeostasisHomeostasisThe processes whereby the internal environment of an organism tends to remain balanced and stable.Cell Injury and Death is maintained
↑ Permeability of the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma to H+:
Collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma is normally impermeable to H+:
Prevents backflow of recently secreted H+
Allows for excretion of urine that is more acidic than plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products
↑ HCO3–secretionSecretionCoagulation Studies → net HCO3– loss → metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Severe metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis may occur in distal RTA (type 1Type 1Spinal Muscular Atrophy):
Serum HCO3– < 10 mEq/L if untreated
Occurs in the distal nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy → no downstream processes to compensate
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Hypocitraturia (predisposes to nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis)
Intercalated cells in distal RTA (type I)
Image by Lecturio.
Proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 2)
The pathophysiology of proximal RTA (type II) is impaired bicarbonate reabsorptionBicarbonate reabsorptionAcid-Base Balance at the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System.
Normal process of proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System HCO3– reabsorption:
Under normal circumstances, 80% of filtered HCO3– is reabsorbed in the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System.
Requires a complex mechanism because HCO3– is not freely permeable (due to charge):
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia–hydrogen ion exchanger 3 (NHE3NHE3A sodium-hydrogen antiporter expressed primarily by epithelial cells in the kidneys, it localizes to the apical membrane of the proximal kidney tubule, where it functions in sodium and water reabsorption and possibly calcium homeostasis. It also is expressed in heart, brain, and lung tissues and is resistant to amiloride inhibition.Carbonic Anhydrase Inhibitors) absorbs Na+ and secretes H+.
Secreted H+ combines with the filtered HCO3– to form H2CO3in the tubular lumen.
H2CO3 is converted into H2O and CO2 by apical carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors IV.
CO2 diffuses freely across the apical membrane back into the cell.
Intracellular carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors II converts CO2 + H2O back into H2CO3.
H2CO3 then can dissociate into H+ and HCO3–:
H+ is recycled through the process through NHE3NHE3A sodium-hydrogen antiporter expressed primarily by epithelial cells in the kidneys, it localizes to the apical membrane of the proximal kidney tubule, where it functions in sodium and water reabsorption and possibly calcium homeostasis. It also is expressed in heart, brain, and lung tissues and is resistant to amiloride inhibition.Carbonic Anhydrase Inhibitors
HCO3– is absorbed through the basolateral membrane via Na+–HCO3– cotransporter and HCO3––Cl– exchanger.
Net effects of the entire process:
Excretion of H+
AbsorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of HCO3–
Abnormal processes leading to proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 2):
Multiple myeloma: light chainsLight chainsPolypeptide chains, consisting of 211 to 217 amino acid residues and having a molecular weight of approximately 22 kda. There are two major types of light chains, kappa and lambda. Two ig light chains and two ig heavy chains (immunoglobulin heavy chains) make one immunoglobulin molecule.Immunoglobulins: Types and Functions are directly toxic to the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System cells
Drugs causing toxicityToxicityDosage Calculation to the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System cells via multiple mechanisms
Mutations in:
Apical NHE3NHE3A sodium-hydrogen antiporter expressed primarily by epithelial cells in the kidneys, it localizes to the apical membrane of the proximal kidney tubule, where it functions in sodium and water reabsorption and possibly calcium homeostasis. It also is expressed in heart, brain, and lung tissues and is resistant to amiloride inhibition.Carbonic Anhydrase Inhibitors
Basolateral Na+/HCO3– cotransporter
Complications:
Moderate metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Serum HCO3– 14–20 mEq/L, even if untreated
Majority of proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System HCO3– reabsorption capacity is maintained:
ThresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction for proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System HCO3– reabsorption lowered
Distal acidification is maintained → daily acid load is managed without worsening acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Fanconi syndrome
Bicarbonate reabsorption in the proximal tubule
CA-IV: carbonic anhydrase IV
CA-II: carbonic anhydrase II
Mixed renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 3Type 3Spinal Muscular Atrophy)
ARARAortic regurgitation (AR) is a cardiac condition characterized by the backflow of blood from the aorta to the left ventricle during diastole. Aortic regurgitation is associated with an abnormal aortic valve and/or aortic root stemming from multiple causes, commonly rheumatic heart disease as well as congenital and degenerative valvular disorders. Aortic RegurgitationmutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in the CA2geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics on chromosomeChromosomeIn a prokaryotic cell or in the nucleus of a eukaryotic cell, a structure consisting of or containing DNA which carries the genetic information essential to the cell.Basic Terms of Genetics 8q22:
Deficiency of carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors II (CAII):
Inability to acidify the urine distally at the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma
Severe bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes wasting:
Dangerously low serum bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
Concomitant renal potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia wasting
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia:
Due to failure of carbonic anhydraseCarbonic anhydraseA family of zinc-containing enzymes that catalyze the reversible hydration of carbon dioxide. They play an important role in the transport of carbon dioxide from the tissues to the lung.Carbonic Anhydrase Inhibitors–dependent potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia reabsorption
Occurs in the distal nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy → no downstream processes to compensate
Hyperkalemic renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 4Type 4Spinal Muscular Atrophy)
The classic mechanism for most individuals with hyperkalemic RTA (i.e., diabetic nephropathyDiabetic nephropathyKidney injuries associated with diabetes mellitus and affecting kidney glomerulus; arterioles; kidney tubules; and the interstitium. Clinical signs include persistent proteinuria, from microalbuminuria progressing to albuminuria of greater than 300 mg/24 h, leading to reduced glomerular filtration rate and end-stage renal disease.Chronic Diabetic Complications and mild-to-moderate CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease) ishyporeninemic hypoaldosteronismHyporeninemic hypoaldosteronismReduced aldosterone synthesis due to decreased stimulation of Renin-angiotensin-aldosterone system.Hypoaldosteronism.
Normal actions of aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:
Net effect is to:
Reabsorb Na+
Secrete K+
Secrete H+
Stimulates epithelial Na channel (ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome) at the principal cell
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia contributes to metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis:
↑ K+ inhibits ammoniagenesis in the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System
↓ Urinary ammonium → ↓ acid excretion
All other etiologies also involve some disturbance in the RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones → ↓ aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia state, which could be absolute or relative (i.e., aldosterone resistanceAldosterone resistanceA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism).
Renal tubular acidoses often do not have a specific clinical presentation and are only considered once metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis is discovered. Although some individuals are asymptomatic, many have significant symptoms caused by the underlying etiology of the RTA, rather than symptoms from the acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis itself.
Distal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 1Type 1Spinal Muscular Atrophy)
Adults:
Unexplained nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis
Sjögren syndromeSjögren SyndromeRheumatoid Arthritis with unexplained metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
OsteomalaciaOsteomalaciaDisorder caused by an interruption of the mineralization of organic bone matrix leading to bone softening, bone pain, and weakness. It is the adult form of rickets resulting from disruption of vitamin d; phosphorus; or calcium homeostasis.Osteomalacia and Rickets
RicketsRicketsDisorders caused by interruption of bone mineralization manifesting as osteomalacia in adults and characteristic deformities in infancy and childhood due to disturbances in normal bone formation. The mineralization process may be interrupted by disruption of vitamin d; phosphorus; or calcium homeostasis, resulting from dietary deficiencies, or acquired, or inherited metabolic, or hormonal disturbances.Osteomalacia and Rickets
Dental presentation of rickets seen in distal renal tubular acidosis:
Rickets can be seen in individuals with distal renal tubular acidosis, as it involves calcium wasting in the urine.
Image: “Showing open bite” by Department of Pedodontics and Preventive Dentistry, Sharad Pawar Dental College, Sawangi (M), Mahartashtra State, Wardha 442102, India. License: CC BY 3.0
Proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 2)
Usually occurs as a part of Fanconi syndrome, rather than isolated RTA:
Fanconi syndrome refers to broad proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System dysfunction
Abnormal reabsorption of phosphorus, uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis, amino acidsAmino acidsOrganic compounds that generally contain an amino (-NH2) and a carboxyl (-COOH) group. Twenty alpha-amino acids are the subunits which are polymerized to form proteins.Basics of Amino Acids, and glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance
Urinary wasting of all these substances occurs
Adults:
Individuals with multiple myeloma and Fanconi syndrome
Mixed renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 3Type 3Spinal Muscular Atrophy)
Metabolic defects often incompatible with survival to reproductive age
Those who do survive are unlikely to reproduce.
Affected children are observed to have:
Short stature
Marble brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification disease → mental retardation
Cerebral calcifications → deafness and blindnessBlindnessThe inability to see or the loss or absence of perception of visual stimuli. This condition may be the result of eye diseases; optic nerve diseases; optic chiasm diseases; or brain diseases affecting the visual pathways or occipital lobe.Retinopathy of Prematurity due to nerve compressionNerve CompressionBrachial Plexus Injuries
Facial dysmorphism
OsteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis → bone fracturesBone fracturesBreaks in bones.Bones: Remodeling and Healing
NephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis
Acute hypokalemic paralysis (associated with diaphragmatic respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure)
ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
ShockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock
Hyperkalemic renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 4Type 4Spinal Muscular Atrophy)
In adults, this is usually an incidental lab finding related to:
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Mild-to-moderate CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
Medications (NSAIDsNSAIDSPrimary vs Secondary Headaches, K-sparing diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, ACEisACEIsA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Heart Failure and Chronic Coronary Syndrome Medication, ARBsARBsAgents that antagonize angiotensin receptors. Many drugs in this class specifically target the angiotensin type 1 receptor.Heart Failure and Chronic Coronary Syndrome Medication, heparin, trimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim)
In children, this is usually due to a rare genetic disease:
PseudohypoaldosteronismPseudohypoaldosteronismA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronism type 2 (Gordon syndrome)
Congenital isolated hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism
Diagnosis
Renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis should be considered in the differential diagnosis of non–anion-gap metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (NAGMA).
Step 1
Once NAGMA is identified, consider the differential diagnosis:
RTA
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Dilutional acidosisDilutional acidosisMetabolic Acidosis (i.e., excessive IV normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids)
CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease (early-to-moderate severity)
Urinary diversion to the GI tract (i.e., ureterosigmoid fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula)
Unmeasured urinary anionsAnionsNegatively charged atoms, radicals or groups of atoms which travel to the anode or positive pole during electrolysis.Electrolytes (i.e., ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis)
UreaseUreaseAn enzyme that catalyzes the conversion of urea and water to carbon dioxide and ammonia.Nocardia/Nocardiosis positive urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection is present
Toxic alcohol poisoning (e.g., methanolMethanolA colorless, flammable liquid used in the manufacture of formaldehyde and acetic acid, in chemical synthesis, antifreeze, and as a solvent. Ingestion of methanol is toxic and may cause blindness.Metabolic Acidosis, ethylene glycolEthylene glycolA colorless, odorless, viscous dihydroxy alcohol. It has a sweet taste, but is poisonous if ingested. Ethylene glycol is the most important glycol commercially available and is manufactured on a large scale in the United States. It is used as an antifreeze and coolant, in hydraulic fluids, and in the manufacture of low-freezing dynamites and resins.Nephrolithiasis)
Urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation = 2(Na+ + K+) + (BUN/2.8) + (glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance/18)
–20 to –50: NAGMA not due to RTA (i.e., diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea)
Step 3
To differentiate between the types of RTA, evaluate:
Serum bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes level:
Proximal (type 2): variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
≥ 5.5 if serum HCO3– is > proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System reabsorption thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction
During treatment with bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
< 5.5 if serum HCO3– is ≤ proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System reabsorption thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction
Mixed (type 3Type 3Spinal Muscular Atrophy): variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Serum potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia:
If the diagnosis is still unclear, a bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes infusion test can be done:
IV bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes is given until the serum HCO3– = 18–20 mEq/L.
Urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance does not change, despite ↑ serum HCO3–
Fractional excretion of HCO3– is < 3% (normal level)
Proximal RTA (type 2)
Urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance increases as the serum HCO3– increases.
Fractional excretion of HCO3– is > 15% (↑ due to HCO3– wasting).
Management
General principles for distal and proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Goal of therapy is to normalize the serum bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes.
Mainstay of therapy is alkali (i.e., bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes) replacement.
Oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes or citrate can be used:
Citrate is converted into bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes in the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy.
1:1 ratio: 1 mEq of citrate becomes 1 mEq of bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes.
Citrate is beneficial for the treatment of nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis.
Serum potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia must be considered:
Potassium-containing preparations may be preferred if hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia is present.
Sodium-containing preparations are used otherwise.
Separate oral potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia replacement is often needed.
Pill burden is a large problem:
Most bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes and citrate tablets have relatively low doses of bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
Dosing is often multiple tablets per dose given multiple times per day.
Predisposes to noncomplianceNoncomplianceClinician–Patient Relationship and poor qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
Medication options:
Over-the-counter baking soda
1 teaspoon = 54 mEq sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
Most cost-effective option
Useful when high doses are needed to help reduce pill burden
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes tablets
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.HyperkalemiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes tablets
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia citrate liquid
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia citrate tablets or liquid
Distal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 1Type 1Spinal Muscular Atrophy)
Oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes (or equivalent): 1–2 mEq/kg/day in divided doses
Relatively easy to correct, because proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System HCO3– reabsorption is normal
May also require potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia supplementation
Proximal renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 2)
Treatment for proximal RTA is more complicated than simply replacing bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes:
Rationale:
Some supplemental bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes will always be wasted in the urine:
Much higher doses of bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes are needed.
Often unable to normalize the serum bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes regardless of treatment
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes wasting results in worsening hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia:
HCO3– travels through the nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy bound to Na+(NaHCO3).
↑ NaHCO3→ ↑ distal delivery of Na+ to principal cellsPrincipal cellsTubular System of collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma
↑ Na+ reabsorption by ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel→ ↑ K+secretionSecretionCoagulation Studies via ROMK channelROMK channelRenal Potassium Regulation
Treatment involves a combination approach:
Stop any offending drug/medication, if possible.
Treat underlying condition, if possible.
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes supplementation:
Oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
HydrochlorothiazideHydrochlorothiazideA thiazide diuretic often considered the prototypical member of this class. It reduces the reabsorption of electrolytes from the renal tubules. This results in increased excretion of water and electrolytes, including sodium, potassium, chloride, and magnesium. It is used in the treatment of several disorders including edema, hypertension, diabetes insipidus, and hypoparathyroidism.Thiazide Diuretics can be used to improve the pill burden:
Diuretic → mild volume contraction → stimulates proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System reabsorption of Na+ and HCO3–
Side effect is worsening hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia supplementation:
Exacerbated by thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.Hyponatremia use
Usually requires more K+ than is included in bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes supplements
Additional supplementation may be needed for Fanconi syndrome:
Phosphorus
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies
Frequent labs to monitor serum HCO3–, K+, and phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes
Mixed renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 3Type 3Spinal Muscular Atrophy)
NaHCO₃ for acute acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia supplementation
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies supplementation
Lithotripsy for renal stones
Surgical fixation of bony fractures
Frequent labs to monitor serum HCO3– and K+
Hyperkalemic renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 4Type 4Spinal Muscular Atrophy)
Treatment for hyperkalemic RTA differs significantly from that for the other forms of RTA, primarily in that oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes therapy is not the 1st-line treatment.
Oral aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia analog
Side effect of Na+ retention can limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation utility
Worsens hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
Can lead to volume overload (peripheral and pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema)
Low-K+ diet
Loop or thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication (particularly if unable to use fludrocortisoneFludrocortisoneA synthetic mineralocorticoid with anti-inflammatory activity.Mineralocorticoids)
Oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes therapy is not usually used.
Differential Diagnosis
Multiple myeloma: malignant plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products cell dyscrasia that leads to toxic levels of serum paraprotein. Presentation is with the CRAB syndrome, which includes hyperCalcemia, Renal failure, Anemia, and Bone lesions/painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. Proximal RTA (type 2) may also be present. Diagnosis is made with serum protein electrophoresisElectrophoresisAn electrochemical process in which macromolecules or colloidal particles with a net electric charge migrate in a solution under the influence of an electric current.Blotting Techniques (SPEP) with immunofixation (IFE), which identifies the abnormal paraprotein (known as the M-spike on the SPEP). Additional testing includes urine protein electrophoresisElectrophoresisAn electrochemical process in which macromolecules or colloidal particles with a net electric charge migrate in a solution under the influence of an electric current.Blotting Techniques (UPEP) and the serum free light chain ratio. Treatment involves chemotherapyChemotherapyOsteosarcoma and hematopoietic stem cell transplantationHematopoietic stem cell transplantationTransfer of hematopoietic stem cells from bone marrow or blood between individuals within the same species (homologous transplantation) or transfer within the same individual (autologous transplantation). Hematopoietic stem cell transplantation has been used as an alternative to bone marrow transplantation in the treatment of a variety of neoplasms.Organ Transplantation.
PseudohypoaldosteronismPseudohypoaldosteronismA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronismtype 1Type 1Spinal Muscular Atrophy: rare disorder that presents in the neonatal period as hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, and metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (type 4Type 4Spinal Muscular Atrophy hyperkalemic RTA). PseudohypoaldosteronismPseudohypoaldosteronismA heterogeneous group of disorders characterized by renal electrolyte transport dysfunctions. Congenital forms are rare autosomal disorders characterized by neonatal hypertension, hyperkalemia, increased renin activity and aldosterone concentration. The type I features hyperkalemia with sodium wasting; type II, hyperkalemia without sodium wasting. Pseudohypoaldosteronism can be the result of a defective renal electrolyte transport protein or acquired after kidney transplantation.Hypoaldosteronismtype 1Type 1Spinal Muscular Atrophy can be diagnosed by an elevated plasma renin activityPlasma renin activityRenal Artery Stenosis and an elevated aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia level. Management includes sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia supplementation and aggressive fluid and electrolyte management.
Cystinosis:Autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritancelysosomal storage diseaseLysosomal storage diseaseLysosomal storage diseases are a group of metabolic disorders caused by genetic mutations in the enzymes responsible for normal lysosomal function. The dysfunction of enzymatic processes causes an accumulation of undigested metabolites, resulting in cellular death. The main groups include sphingolipidoses, oligosaccharidoses, and mucolipidoses. Overview of Lysosomal Storage Diseases is the most common hereditary cause of Fanconi syndrome in children and is caused by a mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in a geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics encoding for the carrierCarrierVaccination protein cystinosin. Intralysosomal cystineCystineA covalently linked dimeric nonessential amino acid formed by the oxidation of cysteine. Two molecules of cysteine are joined together by a disulfide bridge to form cystine.Nephrolithiasis accumulates throughout the body, including in the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System cells, during the 1st year of life (resulting in type 2 proximal RTA and Fanconi syndrome). Progressive kidney damage (including to the glomerulus) occurs, and end-stage renal disease occurs during childhood. Treatment includes the cystine-depleting agent cysteamine and renal replacement therapy (including renal transplantation).
Sjögren syndromeSjögren SyndromeRheumatoid Arthritis: autoimmune disease in which glandular tissues, such as the salivary and lacrimal glandsLacrimal GlandsDacryocystitis, are infiltrated by lymphocytesLymphocytesLymphocytes are heterogeneous WBCs involved in immune response. Lymphocytes develop from the bone marrow, starting from hematopoietic stem cells (HSCs) and progressing to common lymphoid progenitors (CLPs). B and T lymphocytes and natural killer (NK) cells arise from the lineage.Lymphocytes: Histology, causing symptoms such as dry eyes and dry mouth. There are a wide range of extraglandular manifestations of Sjögren syndromeSjögren SyndromeRheumatoid Arthritis, including distal RTA (type 1Type 1Spinal Muscular Atrophy), Raynaud phenomenon, neuropathyNeuropathyLeprosy, and cutaneous vasculitisVasculitisInflammation of any one of the blood vessels, including the arteries; veins; and rest of the vasculature system in the body.Systemic Lupus Erythematosus. Diagnosis is validated by the clinical examination, serologic studies, and salivary glandSalivary glandGlands that secrete saliva in the mouth. There are three pairs of salivary glands (parotid gland; sublingual gland; submandibular gland).Diseases of the Salivary GlandsbiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma. A multidisciplinary approach is needed to treat affected individuals and to target symptom relief.
Systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus (SLESLESystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus): chronic autoimmune disease that causes immune complex deposition in organs, resulting in a wide range of possible systemic manifestations. Notable possible clinical features include malar rashMalar RashSystemic Lupus Erythematosus, nondestructive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis, lupus nephritisLupus nephritisGlomerulonephritis associated with autoimmune disease systemic lupus erythematosus. Lupus nephritis is histologically classified into 6 classes: class I – normal glomeruli, class II – pure mesangial alterations, class III – focal segmental glomerulonephritis, class IV – diffuse glomerulonephritis, class V – diffuse membranous glomerulonephritis, and class VI – advanced sclerosing glomerulonephritis (the world health organization classification 1982).Diffuse Proliferative Glomerulonephritis, serositisSerositisInflammation of a serous membrane.Systemic Lupus Erythematosus, cytopeniasCytopeniasIPEX Syndrome, thromboembolic disease, seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures, and/or psychosis. Hyperkalemic RTA (type 4Type 4Spinal Muscular Atrophy), may also be present. The diagnosis is made by meeting clinical criteria, which includes antinuclear antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions, SLE-specific antibodiesSLE-specific antibodiesSystemic Lupus Erythematosus, and specific clinical findings. Treatment options include hydroxychloroquineHydroxychloroquineA chemotherapeutic agent that acts against erythrocytic forms of malarial parasites. Hydroxychloroquine appears to concentrate in food vacuoles of affected protozoa. It inhibits plasmodial heme polymerase.Immunosuppressants and immunosuppressive medications (e.g., prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants, methotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy, mycophenolateMycophenolateImmunosuppressants mofetil).
Tyrosinemia:autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance genetic disorder caused by a defect in the breakdown of the amino acidAmino acidAmino acids (AAs) are composed of a central carbon atom attached to a carboxyl group, an amino group, a hydrogen atom, and a side chain (R group). Basics of Amino AcidstyrosineTyrosineA non-essential amino acid. In animals it is synthesized from phenylalanine. It is also the precursor of epinephrine; thyroid hormones; and melanin.Synthesis of Nonessential Amino Acids, resulting in failure to thriveFailure to ThriveFailure to thrive (FTT), or faltering growth, describes suboptimal weight gain and growth in children. The majority of cases are due to inadequate caloric intake; however, genetic, infectious, and oncological etiologies are also common. Failure to Thrive during the 1st month of life. Other clinical manifestations include proximal RTA (type 2), Fanconi syndrome, bloody stools, a cabbage-like odor, jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice, hepatomegaly, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Without treatment, cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis and hepatocellular carcinomaHepatocellular carcinomaHepatocellular carcinoma (HCC) typically arises in a chronically diseased or cirrhotic liver and is the most common primary liver cancer. Diagnosis may include ultrasound, CT, MRI, biopsy (if inconclusive imaging), and/or biomarkers. Hepatocellular Carcinoma (HCC) and Liver Metastases will develop. Treatment includes nitisinone and a low-tyrosine (i.e., low-protein) diet.
Wilson diseaseWilson diseaseWilson disease (hepatolenticular degeneration) is an autosomal recessive disorder caused by various mutations in the ATP7B gene, which regulates copper transport within hepatocytes. Dysfunction of this transport mechanism leads to abnormal copper accumulations in the liver, brain, eyes, and other organs, with consequent major and variably expressed hepatic, neurologic, and psychiatric disturbances. Wilson Disease: also known as hepatolenticular degenerationHepatolenticular degenerationWilson disease (hepatolenticular degeneration) is an autosomal recessive disorder caused by various mutations in the ATP7b gene, which regulates copper transport within hepatocytes. Dysfunction of this transport mechanism leads to abnormal copper accumulations in the liver, brain, eyes, and other organs, with consequent major and variably expressed hepatic, neurologic, and psychiatric disturbances.Wilson Disease. Wilson diseaseWilson diseaseWilson disease (hepatolenticular degeneration) is an autosomal recessive disorder caused by various mutations in the ATP7B gene, which regulates copper transport within hepatocytes. Dysfunction of this transport mechanism leads to abnormal copper accumulations in the liver, brain, eyes, and other organs, with consequent major and variably expressed hepatic, neurologic, and psychiatric disturbances. Wilson Disease is an autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance disorder associated with mutations in the ATP7BgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics, which result in copperCopperA heavy metal trace element with the atomic symbol cu, atomic number 29, and atomic weight 63. 55.Trace Elements accumulation in the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification, and corneaCorneaThe transparent anterior portion of the fibrous coat of the eye consisting of five layers: stratified squamous corneal epithelium; bowman membrane; corneal stroma; descemet membrane; and mesenchymal corneal endothelium. It serves as the first refracting medium of the eye.Eye: Anatomy. Presentation is with hepatic, neurologic, and psychiatric symptoms. Distal RTA (type 1Type 1Spinal Muscular Atrophy), may also be present. Diagnosis is established by detection of corneal deposits of copperCopperA heavy metal trace element with the atomic symbol cu, atomic number 29, and atomic weight 63. 55.Trace Elements (Kayser-Fleischer ringsKayser-Fleischer ringsCopper deposits in Descemet’s membrane of the cornea, manifested as green-brown rings that encircle the iris.Wilson Disease), low plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsceruloplasminCeruloplasminA multi-copper blood ferroxidase involved in iron and copper homeostasis and inflammation.Wilson Disease, and/or elevated levels of copperCopperA heavy metal trace element with the atomic symbol cu, atomic number 29, and atomic weight 63. 55.Trace Elements in the urine. Management is with the use of copper-chelating agents such as penicillaminePenicillamine3-mercapto-d-valine. The most characteristic degradation product of the penicillin antibiotics. It is used as an antirheumatic and as a chelating agent in wilson’s disease.Wilson Disease.
References
Bello, C., Duarte, J. S., & Vasconcelos, C. (2017). Diabetes mellitus and hyperkalemic renal tubular acidosis: case reports and literature review. J Bras Nefrol 39, pp. 481–485. https://doi.org/10.5935/0101-2800.20170086
Berend, K. (2017). Review of the diagnostic evaluation of normal anion gap metabolic acidosis. Kidney Dis (Basel) 3, pp. 149–159.
Dobbin, S., Petrie, J. R., Lean, M., & McKay, G. A. (2017). Fludrocortisone therapy for persistent hyperkalaemia. Diabetic medicine : a journal of the British Diabetic Association, 34(7), pp. 1005–1008. https://doi.org/10.1111/dme.13359
Karet, F. E. (2009). Mechanisms in hyperkalemic renal tubular acidosis. Journal of the American Society of Nephrology (JASN), 20(2), pp. 251–254. https://doi.org/10.1681/ASN.2008020166
Koratala, A., & Ruchi, R. (2017). Hypokalemia: A potentially life-threatening complication of tenofovir therapy. SAGE open medical case reports, 5. https://doi.org/10.1177/2050313X17741010
Marangella, M. (2017). Impiego del citrato nel paziente con Nefrolitiasi [Use of citrate in patients with nephrolithiasis]. Giornale italiano di nefrologia: organo ufficiale della Societa italiana di nefrologia, 34(4), pp. 51–60.
Goswami, R. P., Mondal, S., Karmakar, P. S., Ghosh, A. (2012). Type 3 renal tubular acidosis. Indian Journal of Nephrology, 22(6), 466–468. doi: 10.4103/0971-4065.106058. PMID: 23439805; PMCID: PMC3573491. Retrieved October 8, 2022, from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3573491/
Alsharidi, A., Al-Hamed, M., Alsuwaida, A. (2016). Carbonic anhydrase II deficiency: report of a novel mutation. CEN Case Reports 5(1), 108, 112. doi: 10.1007/s13730-015-0205-y. PMID: 28509178; PMCID: PMC5411668. Retrieved October 8, 2022, from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5411668/
Create your free account or log in to continue reading!