Chorioamnionitis, also referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, and/or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Primary risk factors include prolonged rupture of membranes and prolonged labor. Chorioamnionitis is diagnosed by clinical findings, including maternal fever, plus one or more additional specific findings. Chorioamnionitis is managed with antibiotics, and by ensuring continued labor progress (or initiating progress) toward delivery. Chorioamnionitis typically resolves soon after delivery. Significant maternal and fetal complications are possible (including arrest of labor, postpartum hemorrhage, and maternal and/or fetal sepsis), warranting prompt diagnosis and treatment.
Also known as intraamniotic infection (IAI), chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis is an infection, and resulting inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation, of any combination of the fetal membranes (chorionChorionThe outermost extraembryonic membrane surrounding the developing embryo. In reptiles and birds, it adheres to the shell and allows exchange of gases between the egg and its environment. In mammals, the chorion evolves into the fetal contribution of the placenta.Placenta, Umbilical Cord, and Amniotic Cavity and amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity), amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity, placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity, umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity (funisitis), and/or the fetus.
Epidemiology[1,4–7]
ChorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis is the most common cause of peripartum infection, with the following incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency rates:
Overall incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 3.9%
All term deliveries: 1%–5%
Term pre-labor rupture of membranes (PROMPROMPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies.Prelabor Rupture of Membranes), any length: 7%
Term PROMPROMPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies.Prelabor Rupture of Membranes > 24 hours: 40%
Preterm deliveries: 40%–70%
Extreme preterm deliveries (< 24 weeks gestation): up to 94%
Etiology
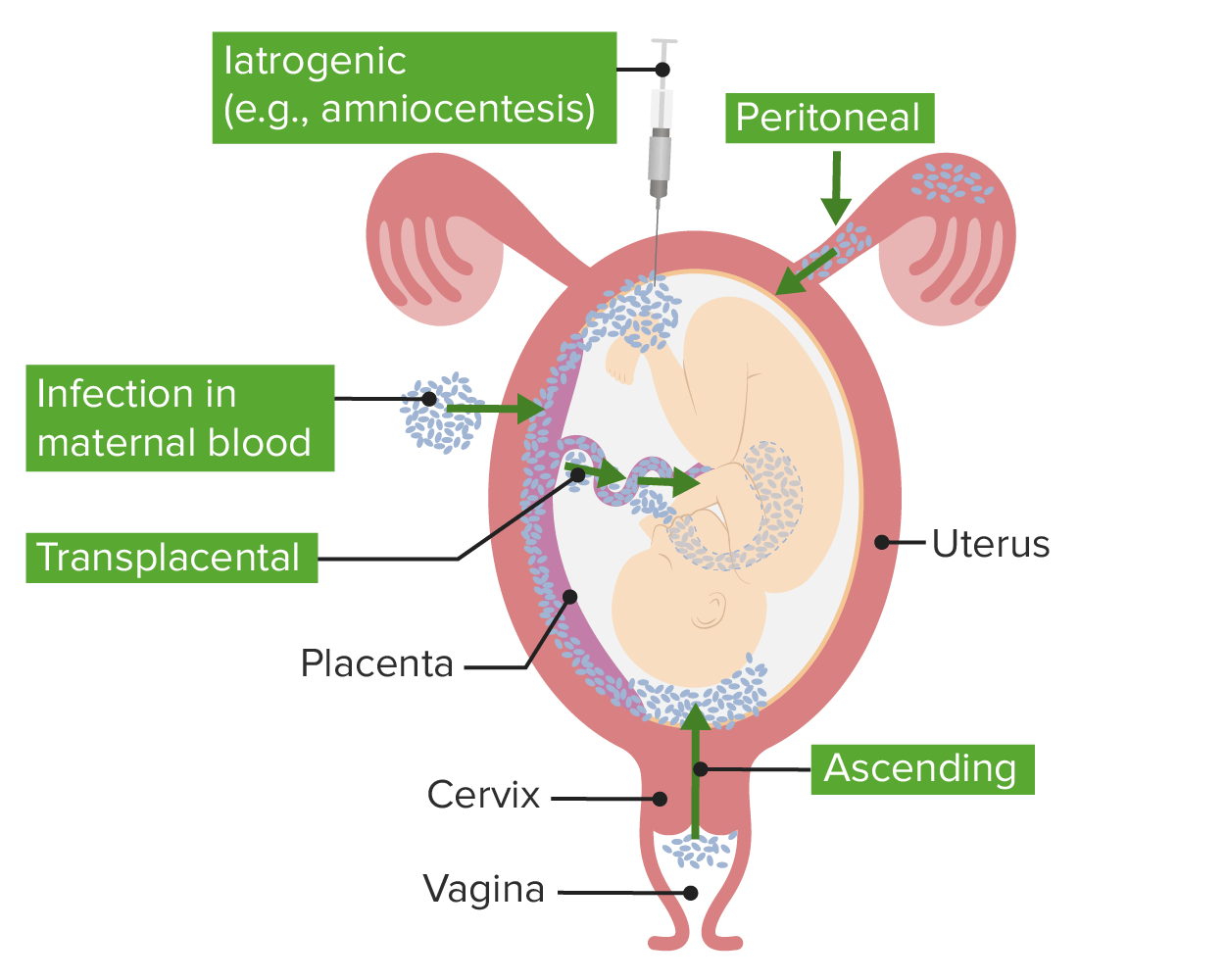
Intraamniotic infection and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation may be caused by the following mechanisms:[1,3,4,6,7]
Ascending migration of cervicovaginal flora (primary mechanism)
HematogenousHematogenousHepatocellular Carcinoma (HCC) and Liver Metastases spread to intervillous space, associated with maternal bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides
Direct infection after invasive procedures (e.g., amniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios)
Descending infection from the peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy via fallopian tubesFallopian tubesThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The fallopian tubes receive an ovum after ovulation and help move it and/or a fertilized embryo toward the uterus via ciliated cells lining the tubes and peristaltic movements of its smooth muscle. Uterus, Cervix, and Fallopian Tubes: Anatomy (very rare)
Routes of chorioamnionitis/funisitis:
There are multiple routes of infection that give rise to chorioamnionitis. Ascending infection from cervicovaginal flora is the most common etiology.
Image by Lecturio.
Risk factors:[1,3,4,6,7]
Prolonged rupture of membranes (ROM) > 18 hours
Most significant risk factor
In both term and preterm pregnancies
Prolonged labor
Preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth
Preterm PROMPROMPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies.Prelabor Rupture of Membranes (PPROM)
Multiple digital examinations (especially after ROM)
STIsSTIsSexually transmitted infections (STIs) or sexually transmitted diseases (STDs) are infections that spread either by vaginal intercourse, anal sex, or oral sex. Symptoms and signs may include vaginal discharge, penile discharge, dysuria, skin lesions (e.g., warts, ulcers) on or around the genitals, and pelvic pain. Some infections can lead to infertility and chronic debilitating disease.Sexually Transmitted Infections (STIs)
By far, the most common cause of chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis is the ascending migration of cervicovaginal flora.[1,3,4,6,7]
Cervicovaginal flora introduced into the amniotic cavityAmniotic cavityEmbryoblast and Trophoblast Development → infection → maternal and fetal inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Can lead to:
Labor
ROM
Uterine atony, which may lead to:
Arrest of labor → operative delivery
Postpartum atony → postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Maternal and/or fetal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Maternal immune response: neutrophilic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of membranes (chorionChorionThe outermost extraembryonic membrane surrounding the developing embryo. In reptiles and birds, it adheres to the shell and allows exchange of gases between the egg and its environment. In mammals, the chorion evolves into the fetal contribution of the placenta.Placenta, Umbilical Cord, and Amniotic Cavity/amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity)
Fetal immune response: neutrophilic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Microbiology:
Polymicrobial
Includes both aerobes and anaerobesAnaerobesLincosamides (especially in preterm gestation)
Most common organisms:
Genital mycoplasmas: Ureaplasma and MycoplasmaMycoplasmaMycoplasma is a species of pleomorphic bacteria that lack a cell wall, which makes them difficult to target with conventional antibiotics and causes them to not gram stain well. Mycoplasma bacteria commonly target the respiratory and urogenital epithelium. Mycoplasma pneumoniae (M. pneumoniae), the causative agent of atypical or “walking” pneumonia.Mycoplasma
Gardnerella vaginalisGardnerella vaginalisPolymicrobial, nonspecific vaginitis associated with positive cultures of gardnerella vaginalis and other anaerobic organisms and a decrease in lactobacilli. It remains unclear whether the initial pathogenic event is caused by the growth of anaerobes or a primary decrease in lactobacilli.Vulvovaginitis
BacteroidesBacteroidesBacteroides is a genus of opportunistic, anaerobic, gram-negative bacilli. Bacteroides fragilis is the most common species involved in human disease and is part of the normal flora of the large intestine.Bacteroides species
Enteric gram-negative rods (e.g., Escherichia coliEscherichia coliThe gram-negative bacterium Escherichia coli is a key component of the human gut microbiota. Most strains of E. coli are avirulent, but occasionally they escape the GI tract, infecting the urinary tract and other sites. Less common strains of E. coli are able to cause disease within the GI tract, most commonly presenting as abdominal pain and diarrhea. Escherichia coli)
Group B StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus
ListeriaListeriaListeria spp. are motile, flagellated, gram-positive, facultative intracellular bacilli. The major pathogenic species is Listeria monocytogenes. Listeria are part of the normal gastrointestinal flora of domestic mammals and poultry and are transmitted to humans through the ingestion of contaminated food, especially unpasteurized dairy products. Listeria Monocytogenes/Listeriosis monocytogenes (hematogenousHematogenousHepatocellular Carcinoma (HCC) and Liver Metastases spread)
Host defense mechanismsDefense mechanismsDefense mechanisms are normal subconscious means of resolving inner conflicts between an individual’s subjective moral sense and their thoughts, feelings, or actions. Defense mechanisms serve to protect the self from unpleasant feelings (anxiety, shame, and/or guilt) and are divided into pathologic, immature, mature, neurotic, and other types.Defense Mechanisms:
Cervical mucus plug
Intact fetal membranes:
Barrier function
Antimicrobial activity
Modulate immune response
Vaginal peroxide-producing lactobacilli → impair virulenceVirulenceThe degree of pathogenicity within a group or species of microorganisms or viruses as indicated by case fatality rates and/or the ability of the organism to invade the tissues of the host. The pathogenic capacity of an organism is determined by its virulence factors.Proteus of pathogens
Clinical Presentation
The vast majority of presenting women will either be in labor, have ruptured membranes, or both.[1,3–7]
Primary manifestations:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Uterine fundal tenderness
Purulent or foul-smelling fluid from the cervical os
Maternal tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children (> 100 bpm)
Fetal tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children (> 160 bpm)
Reduced fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology variability
Diagnosis
The following information is based on a joint workshop between the US National Institute of Child Health and Human Development (NICHD), the American College of Obstetricians and Gynecologists (ACOG), the US Society for Maternal-Fetal Medicine (SMFM), and the American Academy of Pediatrics (AAP). Other organizations may have slightly different specific diagnostic criteria or use different categorizationCategorizationTypes of Variables.[5]
There are 3 categories of IAI:
Isolated maternal feverIsolated maternal feverFever (oral temperature) of > 39 °C (102.2 °F) once, 38.0–38.9 °C (100.4–102.2 °F) on 2 occasions, 30 minutes apart with other potential causes of fever ruled outChorioamnionitis
Suspected IAI
Confirmed IAI
Isolated maternal feverIsolated maternal feverFever (oral temperature) of > 39 °C (102.2 °F) once, 38.0–38.9 °C (100.4–102.2 °F) on 2 occasions, 30 minutes apart with other potential causes of fever ruled outChorioamnionitis[3,5]
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever (oral temperature):
> 39 °C (102.2 °F) once
38.0–38.9 °C (100.4–102.02 °F) on 2 occasions, 30 minutes apart
Rule out other potential causes of feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever:
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children
Other testing based on associated signs and symptoms:
Blood cultures
Sputum testing
InfluenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza/COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). testing
If no other source is found, expert opinion recommends considering patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever > 39 °C (102.2 °F) as suspected IAI.
Suspected intraamniotic infectionSuspected intraamniotic infectionA condition encompassing fever and 1 of the following including fetal tachycardia > 160 bpm for ≥ 10 minutes, maternal leukocytosis with WBC > 15,000/mm3, and purulent cervical drainage on exam.Chorioamnionitis
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and at least 1 of the following:
Fetal tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children: > 160 beats per minute for ≥ 10 minutes
Must meet criteria for “suspected IAI” and have at least 1 of the following:
Positive amniotic-fluid test (obtained by amniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios):
↓ GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance (≤ 14 mg/dL)[7]
↑ WBC (in the absence of a bloody tap, > 30 cells/mm3)[7]
Histopathology (after delivery) showing inflammatory infiltrates in membranes
Management
The goal of management is to minimize the risks of maternal and fetal complications.
Antibiotics:[3,5,7]
Indicated in all 3 categories of IAI :
ACOG states that “antibiotics should be considered” in isolated maternal feverIsolated maternal feverFever (oral temperature) of > 39 °C (102.2 °F) once, 38.0–38.9 °C (100.4–102.2 °F) on 2 occasions, 30 minutes apart with other potential causes of fever ruled outChorioamnionitis owing to the significant potential benefits with low risk.
Given starting at diagnosis and continued through delivery
Standard regimen: ampicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.PenicillinsPLUS gentamicinGentamicinAminoglycosides
Dosing recommended by ACOG:
AmpicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins 2 g IV every 6 hours PLUS
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides 900 mg IV every 8 hours OR
VancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides 1 g IV every 12 hours
If patient undergoes cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery:
Add anaerobic coverage; options include:
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides 900 mg IV once
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess 500 mg IV once
AzithromycinAzithromycinA semi-synthetic macrolide antibiotic structurally related to erythromycin. It has been used in the treatment of Mycobacterium avium intracellulare infections, toxoplasmosis, and cryptosporidiosis.Macrolides and Ketolides (single preoperative dose)
Give a single postpartum dose of the chosen regimen (e.g., 1 additional dose of ampicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins and gentamicinGentamicinAminoglycosides).
Antipyretics:[3,5,7]
To prevent risk to the fetus associated with ↑ maternal temperature
AcetaminophenAcetaminophenAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen
Progress towards delivery:[3]
Think of “delivery” like draining an abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease:
Removes infection from the mother
Removes baby from the infection
Augment labor if it is dysfunctional (common):
Oxytocin
IAI does not necessitate immediate delivery, but continued progress should be made.
In preterm patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship:
IAI is an indication to initiate induction of labor (IOL).
Management is complex: based on gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care and clinical scenario
Continuous fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring[7]
Route of delivery:[3]
Based on routine obstetric indications
Vaginal delivery preferred (↓ morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status/mortalityMortalityAll deaths reported in a given population.Measures of Health Status compared to cesarean)
Postpartum care:[3,5,7]
Usually routine care
Monitor for wound infection
IAI typically resolves quickly after delivery.
Indications that antibiotics should be continued postpartum:
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery (single dose only)
Persistent feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
BacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides
Signs of sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Good communicationCommunicationThe exchange or transmission of ideas, attitudes, or beliefs between individuals or groups.Decision-making Capacity and Legal Competence is critical to ensuring appropriate care of the newbornNewbornAn infant during the first 28 days after birth.Physical Examination of the Newborn. These infants need to be monitored and/or worked up for sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock and potential complications. Critical items for the obstetric team to communicate with the neonatal team include:
Gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care
Maternal and/or fetal tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Group B streptococcal status
Duration of labor
Duration of ROM
Highest maternal temperature
Results of any amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity tests
Medications given to the mother:
ProstaglandinsProstaglandinsA group of compounds derived from unsaturated 20-carbon fatty acids, primarily arachidonic acid, via the cyclooxygenase pathway. They are extremely potent mediators of a diverse group of physiological processes.Eicosanoids
Antimicrobials
Antipyretics
AnesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts use
Complications
Maternal complications[3,5,7]
Dysfunctional labor (infected uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy does not contract well)
Operative delivery
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage (infected uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy does not clamp down well)
Maternal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Postpartum endometritisPostpartum EndometritisInflammation of the endometrium, usually caused by intrauterine infections. Endometritis is the most common cause of postpartum fever.Postpartum Endometritis
Adult respiratory distress syndrome
Neonatal complications[3,7]
The earlier the gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care at delivery, the higher the risk for neonatal complications.
MeningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis
Intraventricular hemorrhageIntraventricular hemorrhageBleeding within the cerebral ventricles. It is associated with intraventricular trauma, aneurysm, vascular malformations, hypertension and in very low birth weight infants.Intracerebral Hemorrhage (IVH)
PneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
Bronchopulmonary dysplasia
Cerebral palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
PrematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis birth (with many of its own associated complications):
Necrotizing enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis (NECNECNecrotizing enterocolitis (NEC) is an intestinal inflammatory process that can lead to mucosal injury and necrosis. The condition is multifactorial, with underlying risk factors that include prematurity and formula feeding. The clinical presentation varies in severity from feeding intolerance, acute findings on abdominal exam, and systemic symptoms. Necrotizing Enterocolitis)
Death
Differential Diagnosis
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection (UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs))/pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess: a common condition in pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care with an increased risk of pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess. Symptoms of pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess include feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, dysuriaDysuriaPainful urination. It is often associated with infections of the lower urinary tract.Urinary Tract Infections (UTIs), suprapubic or flank painFlank painPain emanating from below the ribs and above the ilium.Renal Cell Carcinoma, costovertebral angle tenderness, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Diagnosis is made based on bacteriuriaBacteriuriaThe presence of bacteria in the urine which is normally bacteria-free. These bacteria are from the urinary tract and are not contaminants of the surrounding tissues. Bacteriuria can be symptomatic or asymptomatic. Significant bacteriuria is an indicator of urinary tract infection.Urinary Tract Infections (UTIs) in Children in the setting of the aforementioned symptoms. Treatment is with antibiotics.
Upper respiratory tract infection (URI): a common condition, especially in winterWinterPityriasis Rosea. Symptoms include nasal congestion, rhinorrheaRhinorrheaExcess nasal drainage.Respiratory Syncytial Virus, sore throatSore throatPharyngitis is an inflammation of the back of the throat (pharynx). Pharyngitis is usually caused by an upper respiratory tract infection, which is viral in most cases. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, and hoarseness.Pharyngitis, cough, and feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be tested for influenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza and COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).. A chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is usually required to confirm the diagnosis of pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia, although the X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests can often be delayed until after delivery, except in more severe cases.
Acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis: presents with severe abdominal painAbdominal PainAcute Abdomen, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. The diagnosis may be confirmed with an ultrasound or CT scan (CT scan exposes the fetus to significant radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma and should be used extremely judiciously). AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis rarely presents intrapartum, whereas IAI is rare outside of labor or when membranes are still intact. Management is surgical.
Epidural-associated feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever: Evidence points to a frequent and significant association between a rise in maternal temperature and neuraxial anesthesiaNeuraxial anesthesiaNeuraxial anesthesia is commonly used for lower abdominal and lower extremity surgeries or for pain relief.Anesthesiology: History and Basic Concepts that typically occurs quickly. There are no reliable tests to identify neuraxial anesthesiaNeuraxial anesthesiaNeuraxial anesthesia is commonly used for lower abdominal and lower extremity surgeries or for pain relief.Anesthesiology: History and Basic Concepts as the cause of a feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever; therefore, close observation and/or presumptive treatment for IAI may be appropriate.
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage: occurs when the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity begins to separate prematurely, compromising fetal blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure and oxygenation. Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage typically presents with uterine cramping or painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and vaginal bleeding. FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever is usually not present. Lack of feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, the presence of bleeding, and characteristic findings on fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring make the diagnosis and help distinguish abruption from IAI. Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage is an obstetrical emergency that requires prompt management, including urgent delivery in most cases.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis, also known as intra-amniotic infection (IAI), which is an infection of the chorionChorionThe outermost extraembryonic membrane surrounding the developing embryo. In reptiles and birds, it adheres to the shell and allows exchange of gases between the egg and its environment. In mammals, the chorion evolves into the fetal contribution of the placenta.Placenta, Umbilical Cord, and Amniotic Cavity, amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity, and amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity, typically occurring during labor. Codes are specified by trimester.
Domain
Code
Description
ICD-10-CM
O41.1230
ChorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis, third trimester, not applicable or unspecified
SNOMED CT
237084003
ChorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis (disorder)
Evaluation & Workup:
This CPT code is for an amniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios, a procedure to sample amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity. While chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis is often diagnosed clinically, this procedure can be used to perform a Gram stainGram stainKlebsiella and culture of the fluid to confirm the infection.
Domain
Code
Description
CPT
59000
AmniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios; diagnostic
Medications:
These codes are used to prescribe the standard intrapartum antibiotic regimen for chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis, which is intravenous ampicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins and gentamicinGentamicinAminoglycosides, to treat the maternal infection and prevent neonatal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock.
Domain
Code
Description
RxNorm
859
AmpicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins (ingredient)
AmpicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins
Complications & Supportive Procedures:
These codes are used to document the serious potential maternal and fetal complications of chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis, including maternal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, neonatal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, and postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage.
Domain
Code
Description
ICD-10-CM
O85
Puerperal sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
ICD-10-CM
P36.9
Bacterial sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock of newbornNewbornAn infant during the first 28 days after birth.Physical Examination of the Newborn, unspecified
ICD-10-CM
O72.1
Other immediate postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Higgins RD, Saade G, Polin RA, et al. (2016). Evaluation and management of women and newborns with a maternal diagnosis of chorioamnionitis: summary of a workshop. Obstet Gynecol 127:426. doi: 10.1097/AOG.0000000000001246.