Polyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with enlarged uterine size for gestational age, dyspnea, extremity swelling, or uterine contractions. Diagnosis is made based on ultrasound findings showing excessive amniotic fluid index ≥24 cm or single deepest pocket ≥8 cm. It is associated with significant neonatal and maternal morbidity and mortality. Mild cases can resolve spontaneously. Management of moderate-to-severe cases can include fetal monitoring, amnioreduction, administration of medications such as NSAIDs (e.g., indomethacin), and labor induction.
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is an abnormally high level of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity in the amniotic sac.
Epidemiology[1,2,6]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency range: 0.2%–1.6%
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is idiopathicIdiopathicDermatomyositis in 60%–70% of cases.
Intestinal obstructionIntestinal obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis
CNS:
AnencephalyAnencephalyA malformation of the nervous system caused by failure of the anterior neuropore to close. Infants are born with intact spinal cords, cerebellums, and brainstems, but lack formation of neural structures above this level. The skull is only partially formed but the eyes are usually normal. This condition may be associated with folate deficiency. Affected infants are only capable of primitive (brain stem) reflexes and usually do not survive for more than two weeks.Neural Tube Defects
Dandy-Walker malformation
Pulmonary:
Diaphragmatic herniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias
TrisomyTrisomyThe possession of a third chromosome of any one type in an otherwise diploid cell.Types of Mutations 18
Trisomy 21Trisomy 21Down syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21)
Fetal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types:
Twin-to-twin transfusion syndromeTwin-to-twin transfusion syndromeOccurs in 10%–15% of monochorionic twins due to arteriovenous anastomosis with imbalanced blood flow. Blood flows in a fixed direction from 1 fetus (donor) to another (recipient)Multiple Pregnancy
Gestational diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Maternal uremiaUremiaA clinical syndrome associated with the retention of renal waste products or uremic toxins in the blood. It is usually the result of renal insufficiency. Most uremic toxins are end products of protein or nitrogen catabolism, such as urea or creatinine. Severe uremia can lead to multiple organ dysfunctions with a constellation of symptoms.Acute Kidney Injury
Maternal hypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia
Fetal and placental tumors
Intrapartum infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., TORCH infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease)
Maternal intake of lithiumLithiumAn element in the alkali metals family. It has the atomic symbol li, atomic number 3, and atomic weight [6. 938; 6. 997]. Salts of lithium are used in treating bipolar disorder.Ebstein’s Anomaly
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity is derived from fetal urination
Fluid absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption happens through fetal swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility
EquilibriumEquilibriumOccurs when tumor cells survive the initial elimination attempt These cells are not able to progress, being maintained in a state of dormancy by the adaptive immune system. In this phase, tumor immunogenicity is edited, where T cells keep selectively attacking highly immunogenic tumor cells.This attack leaves other cells with less immunogenicity to potentially develop resistance to the immune response.Cancer Immunotherapy (i.e., a stable amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume) develops between the production and excretion of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity
2 major causes of polyhydramnios:
Increased fetal urination:
High cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics (fetal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types)
Volume overload (twin-to-twin transfusion syndromeTwin-to-twin transfusion syndromeOccurs in 10%–15% of monochorionic twins due to arteriovenous anastomosis with imbalanced blood flow. Blood flows in a fixed direction from 1 fetus (donor) to another (recipient)Multiple Pregnancy)
Osmotic diuresisOsmotic diuresisVolume Depletion and Dehydration (maternal diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, maternal uremiaUremiaA clinical syndrome associated with the retention of renal waste products or uremic toxins in the blood. It is usually the result of renal insufficiency. Most uremic toxins are end products of protein or nitrogen catabolism, such as urea or creatinine. Severe uremia can lead to multiple organ dysfunctions with a constellation of symptoms.Acute Kidney Injury)
Decreased fetal swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility/absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is associated with a 5-fold increased risk of fetal mortalityMortalityAll deaths reported in a given population.Measures of Health Status[4]
Two major causes of polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios:
Increased fetal urination:
High cardiac outputCardiac outputThe volume of blood passing through the heart per unit of time. It is usually expressed as liters (volume) per minute so as not to be confused with stroke volume (volume per beat).Cardiac Mechanics (fetal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types)
Volume overload (twin-to-twin transfusion syndromeTwin-to-twin transfusion syndromeOccurs in 10%–15% of monochorionic twins due to arteriovenous anastomosis with imbalanced blood flow. Blood flows in a fixed direction from 1 fetus (donor) to another (recipient)Multiple Pregnancy)
Osmotic diuresisOsmotic diuresisVolume Depletion and Dehydration (maternal diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, maternal uremiaUremiaA clinical syndrome associated with the retention of renal waste products or uremic toxins in the blood. It is usually the result of renal insufficiency. Most uremic toxins are end products of protein or nitrogen catabolism, such as urea or creatinine. Severe uremia can lead to multiple organ dysfunctions with a constellation of symptoms.Acute Kidney Injury)
Decreased fetal swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility/absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are asymptomatic and it is an incidental ultrasound finding.[1,2]
Most common finding: uterine size measures larger than expected for gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care
Symptomatic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may have:
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea (from increased intra-abdominal pressure opposing movement of the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy)[4]
Extremity edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Tightness of abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Rapidly enlarging abdomen
Decreased fetal movement
Many times baby is in breech presentationBreech presentationA malpresentation of the fetus at near term or during obstetric labor with the fetal cephalic pole in the fundus of the uterus. There are three types of breech: the complete breech with flexed hips and knees; the incomplete breech with one or both hips partially or fully extended; the frank breech with flexed hips and extended knees.Fetal Malpresentation and Malposition
Diagnosis
Diagnostic criteria can vary based on location. The following information is based on US medical society recommendations.
History[1,2]
Often unhelpful
Focus on the presence of risk factors (e.g., diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, genetic diseases).
Ask about the maternal perceptionPerceptionThe process by which the nature and meaning of sensory stimuli are recognized and interpreted.Psychiatric Assessment of fetal movement (often decreased).
Physical exam[1,2,6,9]
Assessments:
Abdominal size and tightness
Lower extremity edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
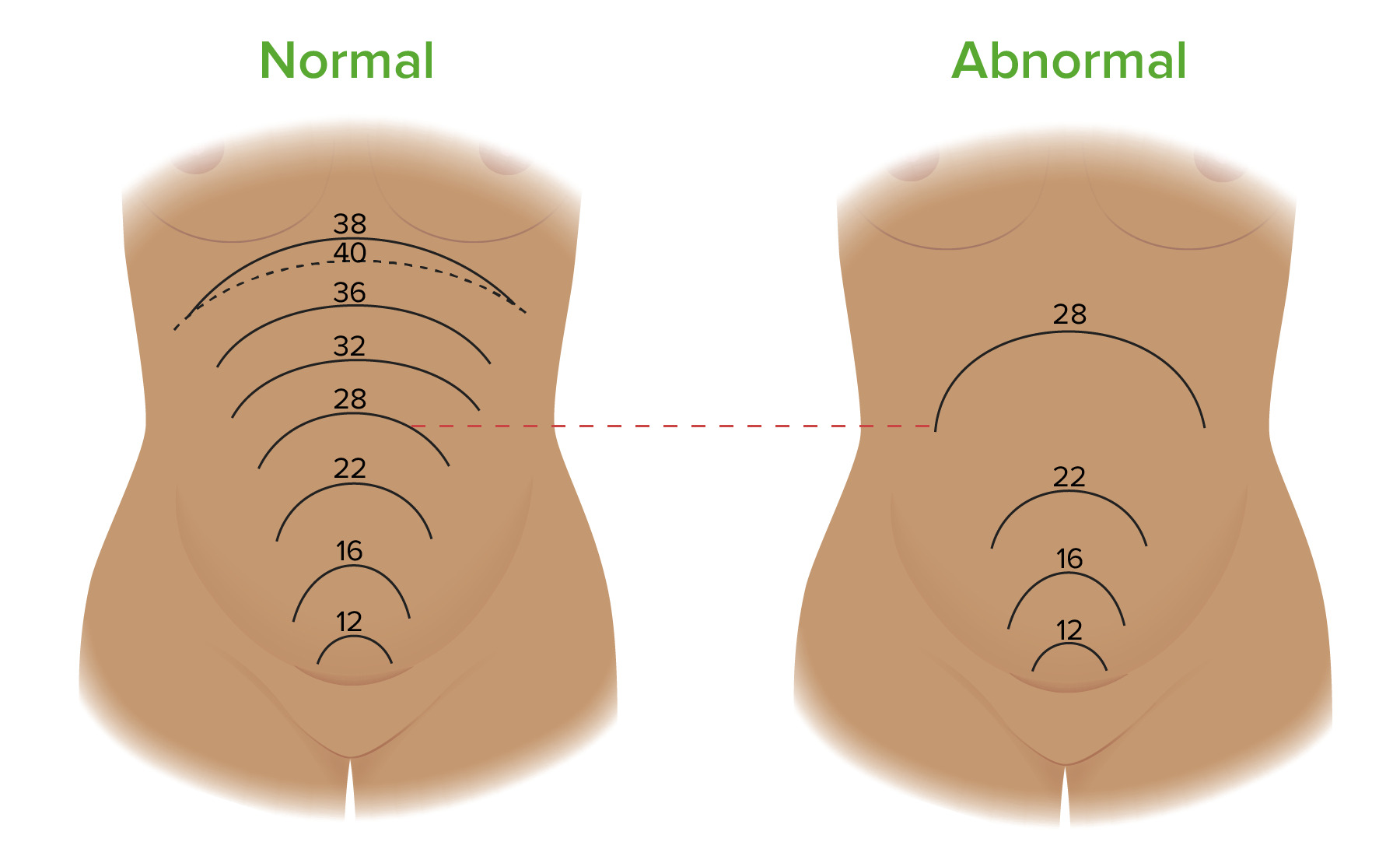
The gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care in weeks should be approximately equal to the fundal height (e.g., a fetus at 25 weeks gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care should have a FH of ~ 25 cm).
FH > 3 cm above the gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care in weeks is suspicious for polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios
Fundal heights throughout pregnancy in normal cases (left) and pregnancies complicated by polyhydramnios (right). The fundal height (FH) is the length between the pubic symphysis and the top of the fundus. The FH measured in centimeters should be approximately equal to the fetus’ gestational age in weeks. For example, at 28 weeks, the FH should be ~ 28 cm. A discrepancy of > 3 cm is suspicious for polyhydramnios. The image on the left shows where the fundus is located at different gestational ages throughout a normal pregnancy. The image on the right shows a potential progression of fundal growth in a pregnancy complicated by polyhydramnios. Notice how the FH at 28 weeks is significantly higher in the pregnancy complicated by polyhydramnios compared to a normal pregnancy.
The uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy is divided into 4 imaginary quadrants
Measure the deepest vertical pocket of fluid in each quadrant at least 1 cm wide and free of umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity or fetal parts.
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity index (AFI):
A sum of the deepest amniotic pocket in all four quadrants
Values between 8–18 cm are normal
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios = AFI ≥ 24 cm[3,8,9]
A single deepest pocket (SDP):
Depth of the single deepest pocket of fluid
Values between 2 and 8 cm are normal
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios = SDP ≥ 8 cm[3,8,9]
Consider amniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios:
Approximately 20 minutes later, a small volume of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity is removed and the concentration of dye is measured, allowing for calculation of the total amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume.
The gold standard test of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity measurement
Rarely done (not recommended by the US Society for Maternal-Fetal Medicine (SMFM) in cases of isolated polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, unless the individual desires chromosomal microarray genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies (which can be offered to all pregnant individuals))[9]
Can also be used for:
Fetal karyotypingKaryotypingMapping of the karyotype of a cell.Chromosome Testing for trisomy 21Trisomy 21Down syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21), 13, and 18
PCRPCRPolymerase chain reaction (PCR) is a technique that amplifies DNA fragments exponentially for analysis. The process is highly specific, allowing for the targeting of specific genomic sequences, even with minuscule sample amounts. The PCR cycles multiple times through 3 phases: denaturation of the template DNA, annealing of a specific primer to the individual DNA strands, and synthesis/elongation of new DNA molecules.Polymerase Chain Reaction (PCR) for detection of congenital infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Table: Classification of mild, moderate, and severe polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios
Classification of polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity index (AFI)
Single deep pocket (SDP)
Mild
24–29.9 cm
8–11.9 cm
Moderate
30–34.9 cm
12–15.9 cm
Severe
≥ 35 cm
≥ 16 cm
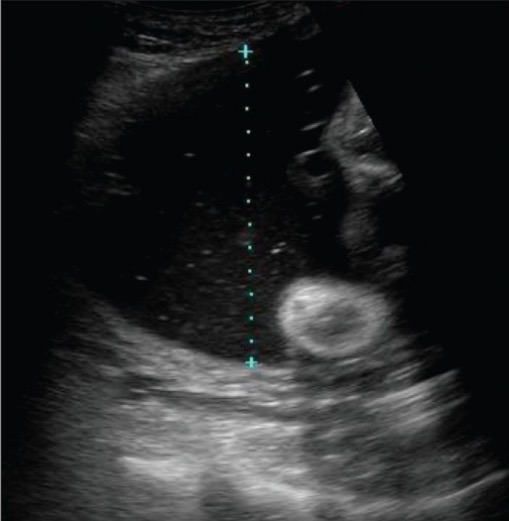
The photo demonstrates the measurement of a vertical pocket of amniotic fluid, which is used in the assessment of amniotic fluid volume. If this was the deepest fluid pocket present, it would be known as the single deepest pocket (SDP); values ≥ 8 cm are classified as polyhydramnios.
Image: “Demonstration of the technique to measure a single vertical pocket of liquor” by Kinare A. License: CC BY 2.0
Other diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests[3,4,9]
Although idiopathicIdiopathicDermatomyositis is the most common type of polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, it is a diagnosis of exclusion. Workup to identify potential causative etiologies can include the following (those indicated with an asterisk (*) are typically already part of routine antenatal care):
Middle cerebral arteryMiddle cerebral arteryThe largest of the cerebral arteries. It trifurcates into temporal, frontal, and parietal branches supplying blood to most of the parenchyma of these lobes in the cerebral cortex. These are the areas involved in motor, sensory, and speech activities.Cerebrovascular System: Anatomy peak systolic velocity measurement:
Measured by ultrasound
↑ Value indicates fetal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types (the fetus is preferentially directing more blood to the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification)
ScreeningScreeningPreoperative Care for diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus: glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose IntolerancetoleranceTolerancePharmacokinetics and Pharmacodynamics test*
TORCH infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
ScreeningScreeningPreoperative Care for alloimmunization (i.e., formation of maternal antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions to fetal blood):
ScreeningScreeningPreoperative Care for Kell, Duffy, D, and C antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions
LithiumLithiumAn element in the alkali metals family. It has the atomic symbol li, atomic number 3, and atomic weight [6. 938; 6. 997]. Salts of lithium are used in treating bipolar disorder.Ebstein’s Anomaly levels
Hemoglobin Bart (significant in individuals of Asian descent): may be heterozygous for alpha-thalassemiaalpha-ThalassemiaA disorder characterized by reduced synthesis of the alpha chains of hemoglobin. The severity of this condition can vary from mild anemia to death, depending on the number of genes deleted.Thalassemia
Note: Symptomatic polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios (e.g., dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth) often has an underlying etiology.[9]
Diagnostic checklist[1]
Fundal height (FH) measurement (“screeningScreeningPreoperative Care” test that should be done at every antenatal appointment): > 3 cm discrepancy between FH and weeks of gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care → ultrasonography
Ultrasound assessment of fluid (AFI or SDP) → classify as mild, moderate, or severe
Management may vary depending on location. The following information is based on US medical society recommendations.
Goals of management[1,9]
Antenatal:
Identify and treat any underlying etiology (e.g., gestational diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus (GDM))
Prevent stillbirth
Relieve maternal symptoms
Intrapartum/postpartum: Be prepared for obstetric complications for which polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is a risk factor. Some of the most clinically relevant include:
Umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity prolapse
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage with rupture of membranes
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Prenatal carePrenatal carePrenatal care is a systematic and periodic assessment of pregnant women during gestation to assure the best health outcome for the mother and her fetus. Prenatal care prevents and identifies maternal and fetal problems that adversely affect the pregnancy outcome. Prenatal Care[1,3,4,9]
Treatment depends on the severity of polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios
Duration: start at 32–34 weeks’ gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care (or when diagnosed) and continue through delivery
Frequency: once or twice weekly
Counseling is recommended to discuss[1]:
Increased risk of stillbirth and importance of maternal attentionAttentionFocusing on certain aspects of current experience to the exclusion of others. It is the act of heeding or taking notice or concentrating.Psychiatric Assessment to fetal movement (e.g., daily fetal kick counts)
Association with fetal anomalies and aneuploidy
Potential changes to routine care (e.g., additional monitoring, timing of delivery, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).)
Serial ultrasonography is performed to assess fetal growth and AFI
Severe/symptomatic polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is treated with:
A type of therapeutic amniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios (removal of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity through a thin needle under ultrasound guidance)
High incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of fluid reaccumulation
Indication: severe maternal discomfort and/or dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea in the setting of severe polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios[9]
Prostaglandin synthetase inhibitors (almost always indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs)):
Inhibits preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth contractions
Stimulation of fetal ADH secretionSecretionCoagulation Studies → ↓ of renal blood flowRenal blood flowThe amount of the renal blood flow that is going to the functional renal tissue, i.e., parts of the kidney that are involved in production of urine.Glomerular Filtration → ↓ diuresis
SMFM recommends against giving indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs) solely to decrease amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume.[9]
Some experts will use indomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs) when uterine distention from polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios is causing preterm contractions at < 32 weeks’ gestation for its combined tocolytic and AFI-reducing effects.[1]
Because of the risk of renal impairment and prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis closure of the ductus arteriosusDuctus arteriosusA fetal blood vessel connecting the pulmonary artery with the descending aorta.Patent Ductus Arteriosus (PDA), the course should be limited to 48 hours.[1]
Genetic counselingGenetic CounselingAn educational process that provides information and advice to individuals or families about a genetic condition that may affect them. The purpose is to help individuals make informed decisions about marriage, reproduction, and other health management issues based on information about the genetic disease, the available diagnostic tests, and management programs. Psychosocial support is usually offered.Myotonic Dystrophies
Intrauterine blood transfusion (fetal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types)
Laser photocoagulation (twin-to-twin transfusion syndromeTwin-to-twin transfusion syndromeOccurs in 10%–15% of monochorionic twins due to arteriovenous anastomosis with imbalanced blood flow. Blood flows in a fixed direction from 1 fetus (donor) to another (recipient)Multiple Pregnancy)
Delivery[9,10]
Timing of delivery is based on:
Underlying etiology
Complications
For idiopathicIdiopathicDermatomyositis/uncomplicated cases, induction of labor is usually recommended between 39 and 40 weeks’ gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care.
For mild idiopathicIdiopathicDermatomyositispolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios specifically, awaiting spontaneous labor is recommended by SMFM. [9]
For severe/symptomatic cases, induction of labor is recommended:
On an individual/case-by-case basis
Usually at 37 weeks
Possibly as early as 34 weeks, depending on the clinical scenario
Delivery at a tertiary care center is recommended owing to the significant possibility of fetal anomalies.[9]
Continuous fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring is recommended
SteroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors to enhance fetal lung maturity if preterm delivery is anticipated.
Complications[1,2,9,10]
Preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth
PrematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis rupture of membranes
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage with rupture of membranes (due to rapid decompression of the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy)
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Fetal malpositionFetal malpositionCommonly refers to any position other than right occiput anterior, left occiput anterior, or direct occiput anterior. All nonvertex presentations are also malpositionedFetal Malpresentation and Malposition
Umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity prolapse
Fetal death
Differential Diagnosis
PreeclampsiaPreeclampsiaA complication of pregnancy, characterized by a complex of symptoms including maternal hypertension and proteinuria with or without pathological edema. Symptoms may range between mild and severe. Pre-eclampsia usually occurs after the 20th week of gestation, but may develop before this time in the presence of trophoblastic disease.Hypertensive Pregnancy Disorders: a condition characterized by new-onset hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension after 20 weeks of gestation, and proteinuriaProteinuriaThe presence of proteins in the urine, an indicator of kidney diseases.Nephrotic Syndrome in Children or signs of end-organ damage. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with visual abnormalities, headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea, and/or epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear). Management includes the administration of antihypertensivesAntihypertensivesThe 1st-line medication classes for hypertension include thiazide-like diuretics, angiotensin-converting enzyme inhibitors (ACEis), angiotensin II receptor blockers (ARBs), and calcium channel blockers (CCBS). Contraindications, adverse effects, and drug-to-drug interactions are agent specific.Hypertension Drugs and possibly labor induction.
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage: the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity prematurely separates from the inner lining of the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy. Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage is a dangerous complication of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship often present with painful vaginal bleeding, uterine contractions, abdominal or back painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis birth. Management depends on the size/stability of the abruption, hemodynamic status of the mother and fetus, and gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care. It includes inpatient admission of the patient and possible delivery.
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR): a condition in which the heart is unable to pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols enough blood to meet the metabolic requirements of the body. Although uncommon in pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care, HF is possible and presents similarly to polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios: exertional dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, paroxysmal nocturnal dyspneaParoxysmal nocturnal dyspneaA disorder characterized by sudden attacks of respiratory distress in at rest patients with heart failure and pulmonary edema. It usually occurs at night after several hours of sleep in a reclining position. Patients awaken with a feeling of suffocation, coughing, a cold sweat, and tachycardia. When there is significant wheezing, it is called cardiac asthma.Pulmonary Edema, abdominal distentionAbdominal distentionMegacolon due to ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites and/or hepatomegaly. Diagnosis is by echocardiographyEchocardiographyUltrasonic recording of the size, motion, and composition of the heart and surrounding tissues. The standard approach is transthoracic.Tricuspid Valve Atresia (TVA). In HF, the FH will be normal with abdominal distension due to ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites. Management includes sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia restriction, administration of diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, inotropic agents, vasodilatorsVasodilatorsDrugs used to cause dilation of the blood vessels.Thromboangiitis Obliterans (Buerger Disease).
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, a condition of excessive amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume. The codes are specified by trimester and are crucial for prompting a workup for underlying causes like maternal diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus or fetal anomalies.
Domain
Code
Description
ICD-10-CM
O40.9XX0
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, unspecified, not applicable or unspecified
ICD-10-CM
O40.3XX0
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, severe, not applicable or unspecified
SNOMED CT
89362005
PolyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios (disorder)
Evaluation & Workup:
These codes are used to investigate the cause of polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios. An ultrasound is used to diagnose and assess for fetal anomalies, while a glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose IntolerancetoleranceTolerancePharmacokinetics and Pharmacodynamics test is ordered to screen the mother for gestational diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, a common cause.
Domain
Code
Description
CPT
76811
Ultrasound, pregnant uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy, real time with image documentationDocumentationSystematic organization, storage, retrieval, and dissemination of specialized information, especially of a scientific or technical nature. It often involves authenticating or validating information.Advance Directives, fetal and maternal evaluation plus detailed fetal anatomic examination
CPT
82951
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance; toleranceTolerancePharmacokinetics and Pharmacodynamics test (GTT), 3 specimens (includes fasting)
Procedures/Interventions:
This CPT code is for an amnioreductionAmnioreductionPolyhydramnios, a therapeutic procedure to remove excess amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity. This is performed to relieve maternal respiratory distress and to reduce the risk of preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth associated with uterine overdistension.
Domain
Code
Description
CPT
59001
AmniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios; therapeutic amniotic fluid reductionAmniotic Fluid ReductionCongenital Diaphragmatic Hernias (includes ultrasound guidance)
Complications & Supportive Procedures:
These codes are used to document the significant risks associated with polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios, including preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth, umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity prolapse when the membranes rupture, and postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage due to an overdistended uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy.
Domain
Code
Description
ICD-10-CM
O60.14X0
Preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth, third trimester, not applicable or unspecified
ICD-10-CM
O69.0XX0
Labor and delivery complicated by prolapse of cord, not applicable or unspecified
ICD-10-CM
O72.1
Other immediate postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Committee on Practice Bulletins. (2016). Practice bulletin no. 175: ultrasound in pregnancy. American College of Obstetricians and Gynecologists. https://pubmed.ncbi.nlm.nih.gov/27875472/
Gica, N., Iliescu, D.G. Mat C, Panaitescu A.M., Peltecu, G., Veduta, A. (2019). Differential diagnosis of polyhydramnios in a patient with gestational diabetes and structurally abnormal fetus. Maedica (Bucur) 14(3):301–304. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6861726/
Reddy, U.M., Abuhamad, A.Z., Levine, D., Saade, G.R. (2014). Fetal imaging: executive summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Institute of Ultrasound in Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of Radiologists in Ultrasound Fetal Imaging workshop. Obstet Gynecol 123(5):1070–1082. doi: 10.1097/AOG.0000000000000245. PMID: 24785860. https://pubmed.ncbi.nlm.nih.gov/24764329/
Dashe, J.S., Pressman, E.K., Hibbard, J.U. (2018). SMFM consult series #46: evaluation and management of polyhydramnios. Am J Obstet Gynecol 219(4):B2–B8. doi: 10.1016/j.ajog.2018.07.016. Epub 2018 Jul 23. PMID: 30048635. https://pubmed.ncbi.nlm.nih.gov/30048635/