Acute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Diffuse alveolar damage involves damage to the endothelial and alveolar epithelial cells and is associated with inflammation and the development of hyaline membranes lining the inner alveolar walls. The reparative stage follows after weeks, with fibrosis possibly occurring later. Clinically, the following triad of findings favors a diagnosis of ARDS: acute or rapidly progressive dyspnea, hypoxic respiratory failure (partial pressure of O2/fraction of inspired O2 ratio < 300 mm Hg), and bilateral alveolar opacities on chest imaging. Management involves the determination and treatment of the cause while providing adequate oxygen, reducing further lung damage, and avoiding fluid overload. Most patients require mechanical ventilation. Acute respiratory distress syndrome is associated with high mortality or long-term complications potentially developing even after treatment.
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) is a clinical syndrome (not a pathologic diagnosis) characterized by a sudden onset of hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome and bilateral pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema without cardiac failureCardiac failureCongestive heart failure refers to the inability of the heart to supply the body with normal cardiac output to meet metabolic needs. Echocardiography can confirm the diagnosis and give information about the ejection fraction.Heart Failure.
The underlying mechanism of ARDS is diffuse alveolar damage (DAD):
Associated with inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and the development of hyaline membranes lining the inner alveolar walls
Epidemiology[1–3,5]
ARDS is the most common cause of non-cardiogenic pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema.
Approximately 140,000 to 160,000 cases of ARDS are reported in the United States each year.
Decline in numbers from earlier estimates (~190,000), likely due to improvements in sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock management, mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing strategies, and broader preventive care
COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). temporarily increased cases, but post-pandemic data stabilized the rates again.
≥ 20% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are mechanically ventilated meet the criteria for ARDS.
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) results from clinical disorders that affect the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy either directly or indirectly.
Direct lung injury:
Bacterial pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia (e.g., StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus pneumoniae)
Viral pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia (e.g., influenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza, SARS-CoV-2 [COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems).])
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock (most common cause)
Flail chestFlail chestFlail chest is a life-threatening traumatic injury that occurs when 3 or more contiguous ribs are fractured in 2 or more different locations. Patients present with chest pain, tachypnea, hypoxia, and paradoxical chest wall movement. Flail Chest
Head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma
BurnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Multiple transfusions (transfusion-related acute lung injuryTransfusion-related acute lung injuryA rare but serious transfusion-related reaction in which fluid builds up in the lungs unrelated to excessively high infusion rate and/or volume (transfusion-associated circulatory overload). Signs of transfusion-related acute lung injury include pulmonary secretions; hypotension; fever; dyspnea; tachypnea; tachycardia; and cyanosis.Transfusion Reactions (TRALI))
Drug overdose
Postcardiopulmonary bypass
Hematopoietic stem cell transplant
Fat embolismFat embolismBlocking of a blood vessel by fat deposits in the circulation. It is often seen after fractures of large bones or after administration of corticosteroids.Nonthrombotic Embolism and amniotic fluid embolismAmniotic Fluid EmbolismBlocking of maternal circulation by amniotic fluid that is forced into uterine veins by strong uterine contraction near the end of pregnancy. It is characterized by the sudden onset of severe respiratory distress and hypotension that can lead to maternal death.Complications during Childbirth
Risk of ARDS:
Increases in a patient with multiple predisposing clinical conditions
25% in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with severe trauma, which increases to 56% if there is associated sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Other risk factors:
Alcohol-abuse disorder
Cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity
Pathophysiology
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) begins with an initial injury to the pneumocytes and pulmonary endotheliumEndotheliumA layer of epithelium that lines the heart, blood vessels (vascular endothelium), lymph vessels (lymphatic endothelium), and the serous cavities of the body.Arteries: Histology, which starts a chain reaction of increasing inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and pulmonary damage that can have an uneven/patchy distribution.
Damage to the alveolar capillary membrane → endothelial cell membranes become leaky → protein-rich fluid exits into the interstitial and alveolar spaces
Release of pro-inflammatory cytokinesCytokinesNon-antibody proteins secreted by inflammatory leukocytes and some non-leukocytic cells, that act as intercellular mediators. They differ from classical hormones in that they are produced by a number of tissue or cell types rather than by specialized glands. They generally act locally in a paracrine or autocrine rather than endocrine manner.Adaptive Immune Response → leukocytesLeukocytesWhite blood cells. These include granular leukocytes (basophils; eosinophils; and neutrophils) as well as non-granular leukocytes (lymphocytes and monocytes).White Myeloid Cells: Histology are recruited to the interstitia and alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS)
Inactivation of the surfactantSurfactantSubstances and drugs that lower the surface tension of the mucoid layer lining the pulmonary alveoli.Acute Respiratory Distress Syndrome (ARDS) (which helps keep alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS) open)
FibrinFibrinA protein derived from fibrinogen in the presence of thrombin, which forms part of the blood clot.Rapidly Progressive Glomerulonephritis precipitates, plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsproteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis, necrotic debris, and dysfunctional surfactantSurfactantSubstances and drugs that lower the surface tension of the mucoid layer lining the pulmonary alveoli.Acute Respiratory Distress Syndrome (ARDS) form the “hyaline membranes” that line the inner alveolar walls (glassy/waxy appearance).
Loss of surfactantSurfactantSubstances and drugs that lower the surface tension of the mucoid layer lining the pulmonary alveoli.Acute Respiratory Distress Syndrome (ARDS) also results in a large increase in the surface tensionSurface tensionThe force acting on the surface of a liquid, tending to minimize the area of the surface.Acute Respiratory Distress Syndrome (ARDS) of alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS), leading to:
Alveolar instability
AtelectasisAtelectasisAtelectasis is the partial or complete collapse of a part of the lung. Atelectasis is almost always a secondary phenomenon from conditions causing bronchial obstruction, external compression, surfactant deficiency, or scarring. Atelectasis
Effects on lung function:
“Stiff lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy” → reduced lung complianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology
Reduced diffusing capacity, shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea, and hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome
Intrapulmonary shunting results from alveolar microvascular occlusion.
Reduction of pulmonary arterial blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure to the ventilated portions of the lung
Many patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship recover within 3–4 weeks after the initial lung injury.
Beginning stage of lung repair and resolution of pathophysiologic changes (reparative process)
Inflammatory exudates are converted into variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables quantities of alveolar duct and interstitial fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans.
Intimal fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans of pulmonary vessels leads to progressive vascular occlusion and pulmonary hypertensionPulmonary HypertensionPulmonary hypertension (PH) or pulmonary arterial hypertension (PAH) is characterized by elevated pulmonary arterial pressure, which can lead to chronic progressive right heart failure. Pulmonary hypertension is grouped into 5 categories based on etiology, which include primary PAH, and PH due to cardiac disease, lung or hypoxic disease, chronic thromboembolic disease, and multifactorial or unclear etiologies. Pulmonary Hypertension.
About 20–30% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship progress into a true fibrotic phase.
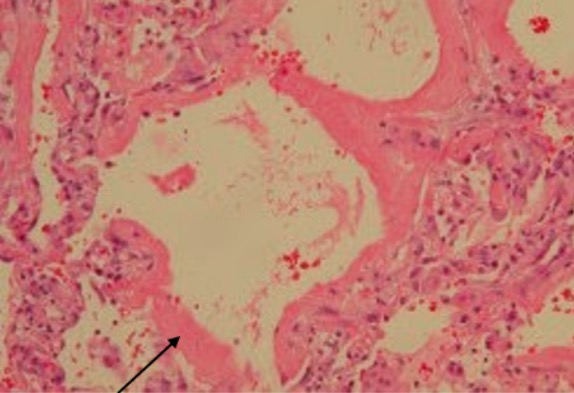
Acute respiratory distress syndrome: A 68-year-old man had mantle cell lymphoma and received chemotherapy. He was admitted to the hospital for fever and respiratory failure. Lung involvement by mantle cell lymphoma was excluded. Video-assisted thoracoscopic lung biopsy revealed diffuse alveolar damage with hyaline membranes lining the alveolar surfaces (arrow) consistent with ARDS.
Image: “Diffuse alveolar damage” by Chih-Hao Chang et al. License: CC BY 2.0, edited by Lecturio.
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever may/may not be present
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
CyanosisCyanosisA bluish or purplish discoloration of the skin and mucous membranes due to an increase in the amount of deoxygenated hemoglobin in the blood or a structural defect in the hemoglobin molecule.Pulmonary Examination
Lower extremity pitting edemaPitting edemaEdema caused by excess fluid without excess colloid. Leaves “pits” due to fluid displacement when pressure is applied to the areaEdema
Diagnosis
Berlin diagnostic criteria of ARDS[1,3,6,12,13]
Acute onset of respiratory symptoms (within 1 week after inciting event)
Diffuse bilateral infiltrates on chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
No evidence of left heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) or fluid overload
Partial pressurePartial pressureThe pressure that would be exerted by one component of a mixture of gases if it were present alone in a container.Gas Exchange of O2/fraction of inspired O2 (PaO2/FiO2) < 300 mm Hg:
Mild ARDS: 201–300 mm Hg with PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation or CPAPCPAPA technique of respiratory therapy, in either spontaneously breathing or mechanically ventilated patients, in which airway pressure is maintained above atmospheric pressure throughout the respiratory cycle by pressurization of the ventilatory circuit.Noninvasive Ventilation ≥ 5 cm H2O
Moderate ARDS: 101–200 mm Hg with PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation ≥ 5 cm H2O
Severe ARDS: ≤ 100 mm Hg with PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation ≥ 5 cm H2O
Diagnosis requires the presence of a known clinical risk factor (e.g., pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia, trauma, sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock), OR hydrostatic edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema is ruled out via imaging (e.g. echocardiographyEchocardiographyUltrasonic recording of the size, motion, and composition of the heart and surrounding tissues. The standard approach is transthoracic.Tricuspid Valve Atresia (TVA)) when a risk factor is absent.
2024 clinical definition of ARDS update: [24]
Includes both intubated and nonintubated patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship (such as those requiring high-flow nasal oxygen)
Includes ultrasound as an imaging modality especially in resource-limited settings
Significance of 2024 update:
Previous Berlin Definition limited ARDS diagnosis to intubated patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation ≥ 5 cm H₂O.
Additions made broaden the criteria and enhance early detection.
BNPBNPA peptide that is secreted by the brain and the heart atria, stored mainly in cardiac ventricular myocardium. It can cause natriuresis; diuresis; vasodilation; and inhibits secretion of renin and aldosterone. It improves heart function. It contains 32 amino acids.Renal Sodium and Water Regulation level:
< 100 pg/mL favors ARDS
Higher levels neither confirm heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) nor exclude ARDS.
Respiratory alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis may be present initially.
Respiratory acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis can occur with severe ARDS.
A-a gradient measures the difference between alveolar oxygen concentration and arterial oxygen.
Calculated using the following factors: age, atmospheric pressureAtmospheric pressureThe pressure at any point in an atmosphere due solely to the weight of the atmospheric gases above the point concerned.Ventilation: Mechanics of Breathing, FiO₂, arterial O₂, and CO₂ in blood gas
Imaging[4,16,19]
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests:
CardiomegalyCardiomegalyEnlargement of the heart, usually indicated by a cardiothoracic ratio above 0. 50. Heart enlargement may involve the right, the left, or both heart ventricles or heart atria. Cardiomegaly is a nonspecific symptom seen in patients with chronic systolic heart failure (heart failure) or several forms of cardiomyopathies.Ebstein’s Anomaly
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
Finding more consistent with pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia: consolidationConsolidationPulmonary Function Tests
CT scan:
Not necessary, but gives more pulmonary details
ARDS: widespread patchy airspace opacities that are more apparent in the dependent lung zones
ARDS excluded by the following findings:
Pericardial effusionPericardial effusionFluid accumulation within the pericardium. Serous effusions are associated with pericardial diseases. Hemopericardium is associated with trauma. Lipid-containing effusion (chylopericardium) results from leakage of thoracic duct. Severe cases can lead to cardiac tamponade.Pericardial Effusion and Cardiac Tamponade
CardiomegalyCardiomegalyEnlargement of the heart, usually indicated by a cardiothoracic ratio above 0. 50. Heart enlargement may involve the right, the left, or both heart ventricles or heart atria. Cardiomegaly is a nonspecific symptom seen in patients with chronic systolic heart failure (heart failure) or several forms of cardiomyopathies.Ebstein’s Anomaly
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
Inexpensive and no ionizing radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma exposure, but operator-dependent
Role in diagnosis has grown; important bedside tool in ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus settings due to its safety, portability, and diagnostic accuracy.
B lines with uneven pleural lines may indicate ARDS.
EchocardiographyEchocardiographyUltrasonic recording of the size, motion, and composition of the heart and surrounding tissues. The standard approach is transthoracic.Tricuspid Valve Atresia (TVA):
Helps distinguish cardiac dysfunction if the clinical presentation is unclear
Findings more consistent with a cardiogenic cause:
Severe aortic or mitral valveMitral valveThe valve between the left atrium and left ventricle of the heart.Heart: Anatomy dysfunction
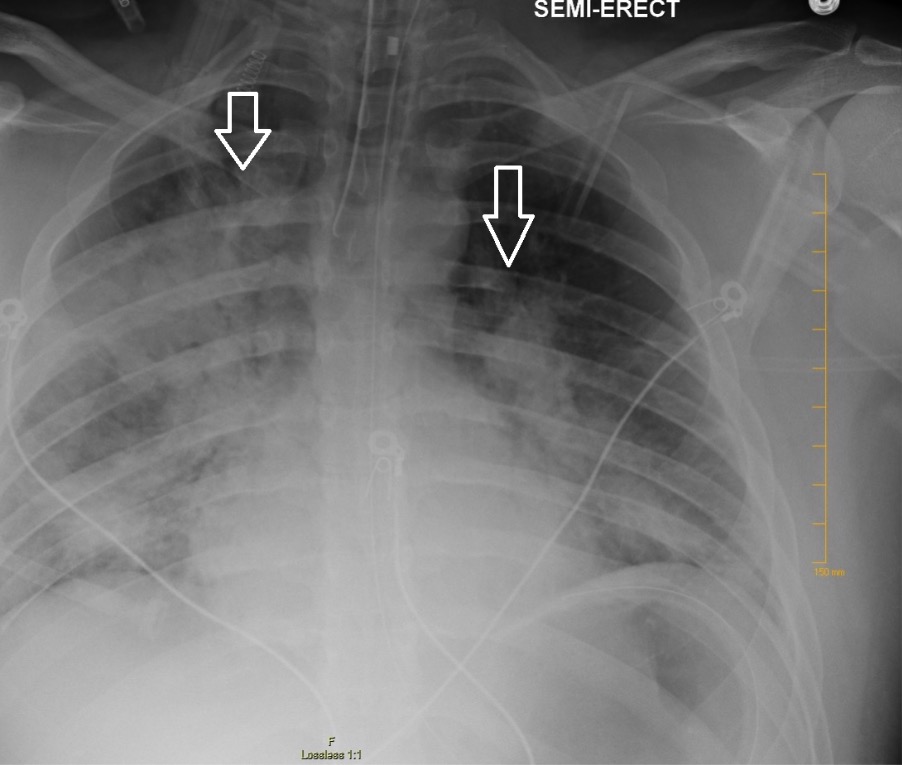
Chest X-ray showing bilateral patchy infiltrates suggestive of ARDS
Image: “Chest radiography demonstrating bilateral hilar opacities” by Ologun G O, Ridley D, Chea N D, et al. (September 08, 2017). Severe ARDS after laparoscopic appendectomy in a young adult. Cureus 9(9): e1664. doi:10.7759/cureus.1664. License: CC BY 4.0
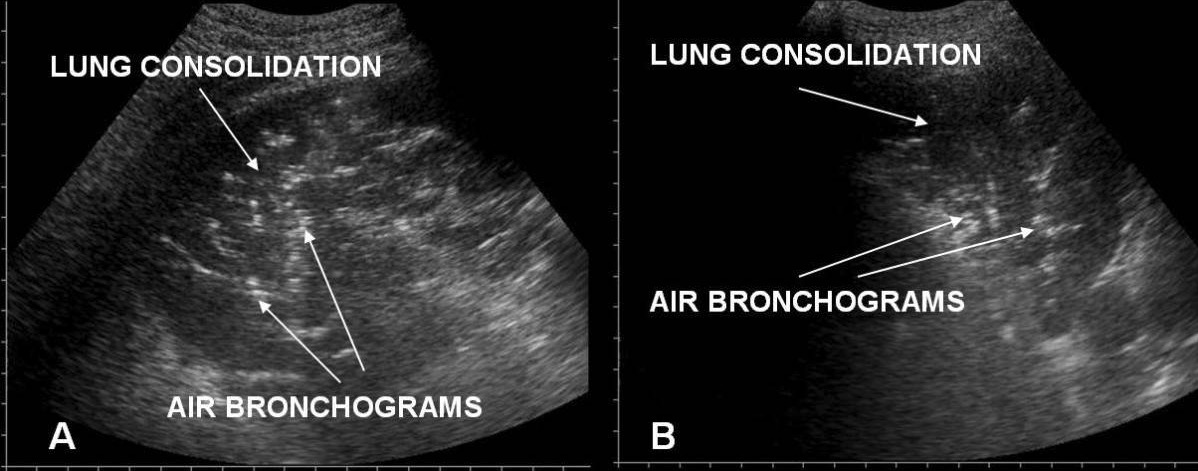
Acute respiratory distress syndrome versus acute cardiogenic pulmonary edema on chest/lung ultrasound: A: irregular pleural line in ARDS B: an even pleural line in acute cardiogenic pulmonary edema
Image: “Lung consolidations with air bronchograms” by Emergency Department S, Antonio Abate General Hospital, Tolmezzo, Italy. License: CC BY 2.0
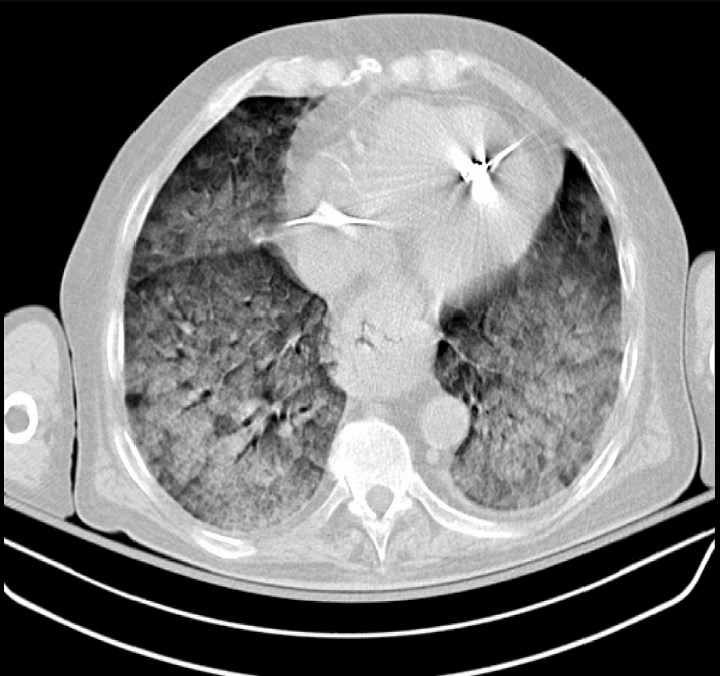
A CT scan showing severe ARDS: diffuse pulmonary opacifications present bilaterally
Image: “Chest CT scan indicative of severe ARDS” by Zagkotsis G, Markou M, Papanikolaou P, et al. (January 24, 2021). Acute Respiratory Distress Syndrome Induced by Parathyroid Storm. Cureus 13(1): e12881. doi:10.7759/cureus.12881. License: CC BY 4.0
Additional tests[6,16,19]
Certain tests are conducted to evaluate the suspected etiology and/or rule out other conditions:
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) and cardiac enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes in acute coronary syndrome
LipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion in pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Microbiologic studies (e.g., cultures) in sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock/infectious etiology
Non-pulmonary imaging in cases of trauma (brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification and spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy imaging) or abdominal etiology, such as peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury or pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (abdominal CT)
Management may vary based on practice location. The following information is based on US, European, UK, and international literature and guidelines for adult patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
General management[1]
Almost all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are managed in the ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus.
Correct the underlying causes, such as:
PneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Trauma
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Gastrointestinal bleedingGastrointestinal bleedingGastrointestinal bleeding (GIB) is a symptom of multiple diseases within the gastrointestinal (GI) tract. Gastrointestinal bleeding is designated as upper or lower based on the etiology’s location to the ligament of Treitz. Depending on the location of the bleeding, the patient may present with hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (fresh blood in stools). Gastrointestinal Bleeding/stress ulcers
Avoid excessive sedation, when possible.
Monitor closely for nosocomial infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease.
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require a high FiO2.
Most often delivered with invasive ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing, but noninvasive ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing (NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation) measures may be appropriate for:
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with lower FiO2 requirements (mild ARDS)
Potential NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation options include:
Mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing:[1,10,12,15–20]
Seek guidance from a pulmonologist or critical care consultant.
Goals for lung-protective ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing:
LimitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical VentilationbarotraumaBarotraumaInjury following pressure changes; includes injury to the eustachian tube, ear drum, lung and stomach.Invasive Mechanical Ventilation
So minimize FiO₂ as early as possible with PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation optimization is critical.
Typical measures:
Target low tidal volumes:
Goal: 4–8 mL/kg of predicted body weight (PBW); do not use actual weight.
5–20 cm H2O (start at minimum PEEPPEEPPressure remaining in the distal airways of the patient at the end of expirationInvasive Mechanical Ventilation for given FiO2)
Opens the collapsed alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS) and/or prevents collapse
Adjust respiratory rateRespiratory rateThe number of times an organism breathes with the lungs (respiration) per unit time, usually per minute.Pulmonary Examination (RRRRRelative risk (RR) is the risk of a disease or condition occurring in a group or population with a particular exposure relative to a control (unexposed) group.Measures of Risk) to maintain pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance (maximum: 35 breaths per minute)
If oxygenation is still an issue but peak pressures are high → consider “inverse ratio ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing”:
Inspiratory time lengthened → goal to be longer than expiratory time (I:E > 1:1)
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance goal: 7.3–7.45
Higher PaCO₂ (permissive hypercapniaHypercapniaA clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood.Neonatal Respiratory Distress Syndrome) is acceptable if necessary to maintain lung-protective ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing (as long as pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance > 7.2 is tolerated).
ECMO:[1,12,15–20,23]
Last resort or rescue therapy
An option if respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure is potentially reversible
Consider venovenous extracorporeal membrane oxygenation (ECMO) if PaO2/FiO2 < 80 mm Hg despite optimal ventilatory management[15,23]
Requires specialty services at designated centers
Most common complication: bleeding (particularly intracranial bleeding)
Fluid management[1,12,14,15,25]
Fluid management can be difficult in critically-ill patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
In general, use fluid restriction:
Goal: ↓ left atrial filling pressure → minimize pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema → improve oxygenation.
Maintain central venous pressureCentral venous pressureThe blood pressure in the central large veins of the body. It is distinguished from peripheral venous pressure which occurs in an extremity.Central Venous Catheter < 4 mm Hg in non–sepsis-related ARDS.
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (try to maintain mean arterial pressureMean Arterial PressureMean arterial pressure (MAP) is the average systemic arterial pressure and is directly related to cardiac output (CO) and systemic vascular resistance (SVR). The SVR and MAP are affected by the vascular anatomy as well as a number of local and neurohumoral factors.Vascular Resistance, Flow, and Mean Arterial Pressure (MAP) ≥ 65 mm Hg)
Hypoperfusion (e.g., renal function)
Exception: PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with certain conditions (e.g., sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis) may require a large fluid volume:
After early resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome, a net-neutral or slightly net-negative fluid status is recommended.
Pharmacologic therapies[1,3,10,12,15–20,25]
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids:
Given if the patient has another indication for use (otherwise, poor evidence for their use in ARDS)
Can be considered early (within 14 days) in the course of persistent and moderate-to-severe ARDS despite typical treatment.
Associated with lower mortalityMortalityAll deaths reported in a given population.Measures of Health Status for COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). ARDS
Common regimens:
DexamethasoneDexamethasoneAn anti-inflammatory 9-fluoro-glucocorticoid.Antiemetics 20 mg IV once a day for 5 days, then 10 mg once a day for 5 days
MethylprednisoloneMethylprednisoloneA prednisolone derivative with similar anti-inflammatory action.Immunosuppressants 1 mg/kg/day (divided doses) for 14 days, then taper (total of 28 days)
Neuromuscular blockadeNeuromuscular BlockadeThe intentional interruption of transmission at the neuromuscular junction by external agents, usually neuromuscular blocking agents. It is distinguished from nerve block in which nerve conduction (neural conduction) is interrupted rather than neuromuscular transmission. Neuromuscular blockade is commonly used to produce muscle relaxation as an adjunct to anesthesia during surgery and other medical procedures. It is also often used as an experimental manipulation in basic research. It is not strictly speaking anesthesia but is grouped here with anesthetic techniques. The failure of neuromuscular transmission as a result of pathological processes is not included here.Aminoglycosides:
Used to promote ventilator synchrony during paralysis
Consider using in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a PaO2/FiO2 ratio < 150 mm Hg.[15]
Preferred use early in the course of the disease ( first 48 hours) and ideally, should not be used for > 48 hours
Reevaluate use at least daily.
Adverse effects:
Allergic reaction
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Arrhythmias
Prolonged paralysis
Acquired muscle weakness
Pulmonary vasodilatorsVasodilatorsDrugs used to cause dilation of the blood vessels.Thromboangiitis Obliterans (Buerger Disease) (e.g., inhaled nitrous oxideNitrous oxideNitrogen oxide (N2O). A colorless, odorless gas that is used as an anesthetic and analgesic. High concentrations cause a narcotic effect and may replace oxygen, causing death by asphyxia.Inhaled Anesthetics):
Generally not recommended, as it may be harmful and worsen renal function even if oxygenation is temporarily improved
Can be considered as a rescue therapy in certain circumstances
COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). ARDS[12,17]
This brief word on the treatment of ARDS associated with COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). is based on the National Institutes of Health (NIH) COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). ARDS recommendations:
Mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing management follows typical ARDS protocol.
Additional therapies utilized in COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). ARDS:
DexamethasoneDexamethasoneAn anti-inflammatory 9-fluoro-glucocorticoid.Antiemetics is first-line.
Add baricitinibBaricitinibTargeted and Other Nontraditional Antineoplastic Therapy or tocilizumabTocilizumabImmunosuppressants if there is rapid respiratory deterioration or need for HFNC, NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation, or mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing, within 24–48 hours of hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium.
Remdesivir:
Recommended for hospitalized patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship requiring oxygen but not yet mechanically ventilated (e.g., on HFNC or NIVNIVNoninvasive ventilation (NIV) is an advanced respiratory support that does not require an artificial, invasive airway. This technique is commonly used during acute respiratory failure. The most common forms of NIV are noninvasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC).Noninvasive Ventilation).
Not routinely recommended once intubated or on ECMO.
Prone positioning: at least 12–16 hours/day in moderate-to-severe cases (PaO₂/FiO₂ <150 mmHg).
Unless contraindicated, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with COVID-19COVID-19Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that mainly affects the respiratory system but can also cause damage to other body systems (cardiovascular, gastrointestinal, renal, and central nervous systems). ARDS should be on prophylactic anticoagulationAnticoagulationPulmonary Hypertension Drugs.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[1,3]
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) is a serious condition that is usually associated with high mortalityMortalityAll deaths reported in a given population.Measures of Health Status and morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status (30%–50% mortalityMortalityAll deaths reported in a given population.Measures of Health Status).
Several risk factors have been identified that can estimate the prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas in a patient with ARDS:
Preexisting organ dysfunction from chronic diseases:
Chronic liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
Immunosuppression
Direct lung injuries result in twice the number of early phase mortalities compared to indirect causes of lung injury.
The majority of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship recover most of their lung function but will take months.[16,20]
Long-term complications[1]
Many patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will develop lung fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans, whereas some may require long-term mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing and oxygen supply.
Others: cognitive dysfunction (in 30%–55%), psychiatric illness (e.g., depression), reduced exercise endurance with muscle weakness
Differential Diagnosis
Cardiogenic pulmonary edemaCardiogenic Pulmonary EdemaPulmonary Edema: a condition caused by excess fluid in the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy, resulting from cardiac failureCardiac failureCongestive heart failure refers to the inability of the heart to supply the body with normal cardiac output to meet metabolic needs. Echocardiography can confirm the diagnosis and give information about the ejection fraction.Heart Failure. Cardiogenic etiology is suggested by an S3S3Heart Sounds or S4 gallopS4 gallopHeart Sounds, elevated jugular venous pressureJugular Venous PressurePortal Hypertension, and lower extremity edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema with typical chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests findings (pulmonary venous congestion, cardiomegalyCardiomegalyEnlargement of the heart, usually indicated by a cardiothoracic ratio above 0. 50. Heart enlargement may involve the right, the left, or both heart ventricles or heart atria. Cardiomegaly is a nonspecific symptom seen in patients with chronic systolic heart failure (heart failure) or several forms of cardiomyopathies.Ebstein’s Anomaly, pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion, response to diuresis). Management of cardiogenic pulmonary edemaCardiogenic Pulmonary EdemaPulmonary Edema involves diuresis.
Diffuse alveolar hemorrhage: a condition resulting from injury to the arteriolesArteriolesThe smallest divisions of the arteries located between the muscular arteries and the capillaries.Arteries: Histology, venulesVenulesThe minute vessels that collect blood from the capillary plexuses and join together to form veins.Veins: Histology, or capillariesCapillariesCapillaries are the primary structures in the circulatory system that allow the exchange of gas, nutrients, and other materials between the blood and the extracellular fluid (ECF). Capillaries are the smallest of the blood vessels. Because a capillary diameter is so small, only 1 RBC may pass through at a time.Capillaries: Histology. Diffuse alveolar hemorrhage is associated with multiple diseases (e.g., Goodpasture syndromeGoodpasture SyndromeGoodpasture syndrome, also known as anti-glomerular basement membrane (GBM) disease, is an autoimmune disease characterized by circulating antibodies directed against glomerular and alveolar basement membranes. Affected individuals present with symptoms of rapidly progressive glomerulonephritis and alveolar hemorrhage. Goodpasture Syndrome). HemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis is usually present. Diffuse alveolar hemorrhage may present with sudden-onset respiratory distress, like ARDS. Diagnosis is by chest CT and bronchoscopyBronchoscopyEndoscopic examination, therapy or surgery of the bronchi.Laryngomalacia and Tracheomalacia with bronchoalveolar lavageBronchoalveolar lavageWashing out of the lungs with saline or mucolytic agents for diagnostic or therapeutic purposes. It is very useful in the diagnosis of diffuse pulmonary infiltrates in immunosuppressed patients.Pulmonary Fibrosis (BAL), which shows fresh RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology and hemosiderin-laden macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation.
Acute interstitial pneumonitisPneumonitisHuman Herpesvirus 6 and 7 (Hamman-Rich syndrome): a fulminant form of diffuse lung injury that mimics ARDS. The onset of acute interstitial pneumonitisPneumonitisHuman Herpesvirus 6 and 7 is acute, and the symptoms include feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, cough, and dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea. Acute interstitial pneumonitisPneumonitisHuman Herpesvirus 6 and 7 may be a subset of idiopathicIdiopathicDermatomyositis ARDS but without a known risk factor. Diagnosis is by lung biopsyLung BiopsyAntineutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis, which shows diffuse damage to the alveoliAlveoliSmall polyhedral outpouchings along the walls of the alveolar sacs, alveolar ducts and terminal bronchioles through the walls of which gas exchange between alveolar air and pulmonary capillary blood takes place.Acute Respiratory Distress Syndrome (ARDS).
Acute exacerbation of idiopathicIdiopathicDermatomyositis pulmonary fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans: a condition similar to ARDS that presents with diffuse alveolar damage and acute interstitial pneumonitisPneumonitisHuman Herpesvirus 6 and 7, but with a worse prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas. Acute exacerbation of idiopathicIdiopathicDermatomyositis pulmonary fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans can occur in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with previously undiagnosed interstitial lung disease. Diagnosis is made by comparing previous radiographic and CT images, and by lung biopsyLung BiopsyAntineutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose Acute Respiratory Distress SyndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) (ARDS), a life-threatening form of acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure characterized by widespread inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation in the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy, non-cardiogenic pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema, and severe hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome.
Coding System
Code
Description
ICD-10-CM
J80
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS)
SNOMED CT
67782005
Adult respiratory distress syndrome (disorder)
Evaluation & Workup:
These codes are for the key diagnostic components of the Berlin definition of ARDS: a chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests showing bilateral opacities and an arterial blood gasArterial blood gasRespiratory Alkalosis (ABG) to calculate the PaO2/FiO2FiO2percentage of oxygen delivered directly to the patientInvasive Mechanical Ventilation ratio and determine the severity of hypoxemiaHypoxemiaNeonatal Respiratory Distress Syndrome.
This code is for invasive mechanical ventilationInvasive mechanical ventilationInvasive mechanical ventilation (IMV) is an advanced airway modality used for individuals with immediate or impending respiratory failure and/or in preparation for surgery. The IMV technique involves positive pressure ventilation delivered to the lungs through an endotracheal tube via a ventilator.Invasive Mechanical Ventilation, the primary supportive therapy for ARDS. A lung-protective ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing strategy with low tidal volumes is crucial to prevent further lung injury.
Coding System
Code
Description
ICD-10-PCS
5A1955Z
Respiratory VentilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing, Greater than 96 Consecutive Hours
References
Baron, R. M., Levy, B. D. (2018). Acute respiratory distress syndrome. In Jameson, J., Fauci A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., Loscalzo, J. (Eds.) Harrison’s Principles of Internal Medicine (20th ed.). McGraw-Hill.
Husain, A. N. (2020). Acute lung injury and acute respiratory distress syndrome (diffuse alveolar damage) In Kumar, V., Abbas, A. K., Aster, J. C., (Eds.). Robbins & Cotran Pathologic Basis of Disease. (10th ed., pp. 676–678).
Duggal, A., Panitchote, A., Siuba, M., Krishnan, S., Torbic, H., Hastings, A., Mehkri, O., Hanane, T., Hatipoglu, U., Hite, R. D., Mireles-Cabodevila, E. (2021). Implementation of protocolized care in ARDS improves outcomes. Respiratory Care, 66(4), 600–609. https://doi.org/10.4187/respcare.07999
Barrot, L., Asfar, P., Mauny, F., Winiszewski, H., Montini, F., Badie, J., Quenot, J.-P., Pili-Floury, S., Bouhemad, B., Louis, G., Souweine, B., Collange, O., Pottecher, J., Levy, B., Puyraveau, M., Vettoretti, L., Constantin, J.-M., Capellier, G. (2020). Liberal or conservative oxygen therapy for acute respiratory distress syndrome. New England Journal of Medicine, 382(11), 999–1008. https://doi.org/10.1056/NEJMoa1916431
Welker, C., Huang, J., Gil, I. J. N., Ramakrishna, H. (2021). 2021 Acute respiratory distress syndrome update, with coronavirus disease 2019 focus. Journal of Cardiothoracic and Vascular Anesthesia.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7912364/
Fan, E., Brodie, D., & Slutsky, A. S. (2018). Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. JAMA, 319(7), 698–710. https://doi.org/10.1001/jama.2017.21907
Vignon, P., Evrard, B., et al. (2020). Fluid Administration and monitoring in ARDS: which management? Intensive Care Medicine, 46(12), 2252–2264. https://doi.org/10.1007/s00134-020-06310-0
Papazian, L., Aubron, C., Brochard, L., et al. (2019). Formal guidelines: management of acute respiratory distress syndrome. Annals of Intensive Care, 9(1), 69. https://doi.org/10.1186/s13613-019-0540-9
Fan, E., et al. (2017). An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. American Journal of Respiratory & Critical Care Medicine, 195(9), 1253–1263. https://www.thoracic.org/statements/resources/cc/ards-guidelines.pdf
Hensley, M. K., & Prescott, H. C. (2022). Caring for the Critically Ill Patient with COVID-19. Clinics in chest medicine, 43(3), 441–456. https://doi.org/10.1016/j.ccm.2022.04.006
Griffiths, M. J. D., McAuley, D. F., et al. (2019). Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respiratory Research, 6(1), e000420. https://doi.org/10.1136/bmjresp-2019-000420
Qadir, N., Sahetya, S., Munshi, L., Summers, C., Abrams, D., Beitler, J., Bellani, G., Brower, R. G., Burry, L., Chen, J. T., Hodgson, C., Hough, C. L., Lamontagne, F., Law, A., Papazian, L., Pham, T., Rubin, E., Siuba, M., Telias, I., Patolia, S., … Fan, E. (2024). An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline. American journal of respiratory and critical care medicine, 209(1), 24–36. https://doi.org/10.1164/rccm.202311-2011ST
Matthay, M. A., Arabi, Y., Arroliga, A. C., Bernard, G., Bersten, A. D., Brochard, L. J., Calfee, C. S., Combes, A., Daniel, B. M., Ferguson, N. D., Gong, M. N., Gotts, J. E., Herridge, M. S., Laffey, J. G., Liu, K. D., Machado, F. R., Martin, T. R., McAuley, D. F., Mercat, A., Moss, M., … Wick, K. D. (2024). A New Global Definition of Acute Respiratory Distress Syndrome. American journal of respiratory and critical care medicine, 209(1), 37–47. https://doi.org/10.1164/rccm.202303-0558WS