Subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral "bridging" veins.Subdural Hemorrhage (SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral "bridging" veins.Subdural Hemorrhage) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injuryClosed Head InjurySubdural Hemorrhage) causing a tearing injury to the extracerebral “bridging” veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology, but rupture of small arteriesSmall arteriesArteries: Histology within this space or intracranial hypotensionIntracranial hypotensionReduction of cerebrospinal fluid pressure characterized clinically by orthostatic headache and occasionally by an abducens nerve palsy; hearing loss; nausea; neck stiffness, and other symptoms. This condition may be spontaneous or secondary to cerebrospinal fluid leak; spinal puncture; neurosurgical procedures; dehydration; uremia; trauma; and other processes. Chronic hypotension may be associated with subdural hematomas or hygromas.Subdural Hemorrhage may also be causative. Acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral "bridging" veins.Subdural Hemorrhage presents, immediately following head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma, with an altered level of consciousnessAltered Level of ConsciousnessIntracerebral Hemorrhage that may span from a momentary loss of consciousness to comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma, which makes it a potentially life-threatening condition. Chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral "bridging" veins.Subdural Hemorrhage may also occur, presenting with a more gradual neurologic deterioration. Diagnosis is based on clinical suspicion following head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma and confirmed with neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant (e.g., noncontrast head CT). Management includes stabilization, stopping (possibly reversing) all anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants, monitoring in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus, and neurosurgical intervention.
Subdural hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception (SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage) is bleeding, usually caused by head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma, producing a collection of blood between the dural and arachnoid meningeal layers surrounding the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification, within the potential subdural spaceSubdural spacePotential cavity which separates the arachnoid mater from the dura mater.Subdural Hemorrhage.[1]
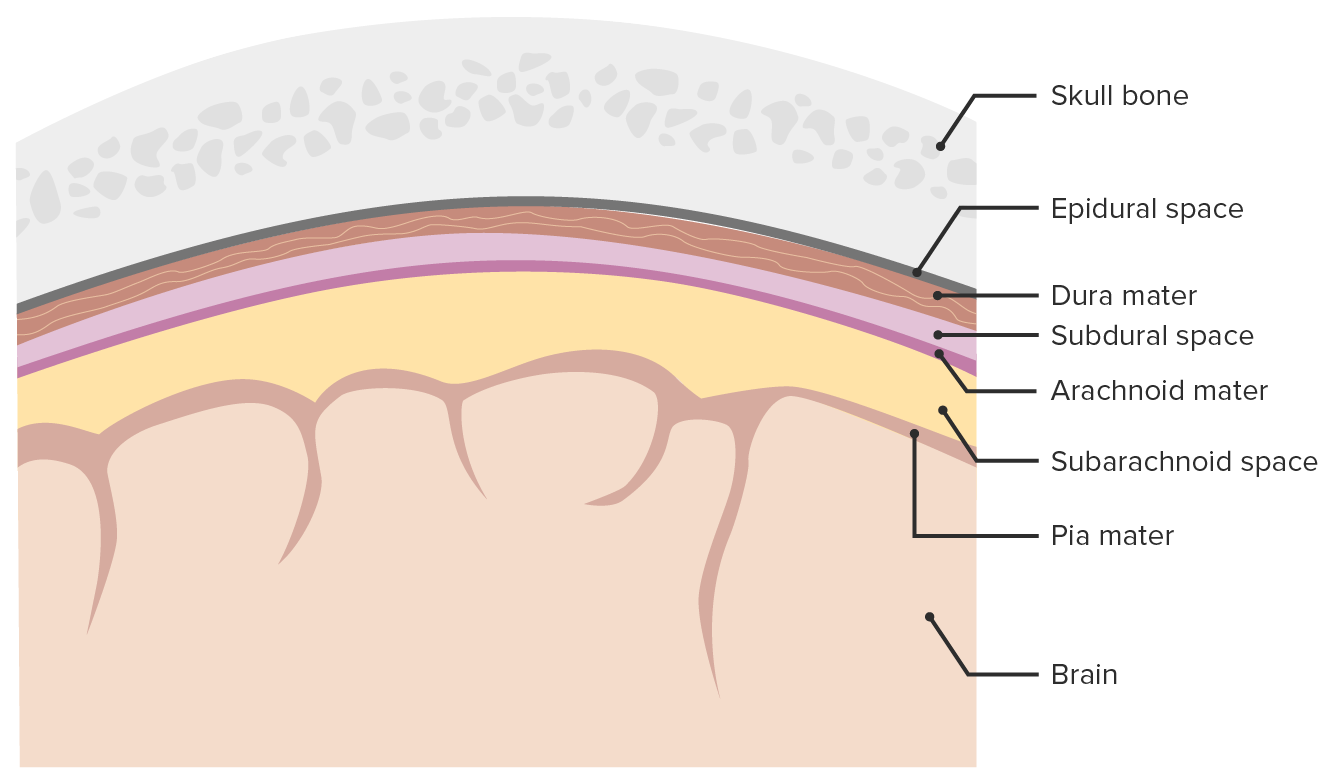
Meninges and meningeal spaces: The image depicts the 3 layers (dura mater, arachnoid mater, and pia mater) surrounding the brain and spinal cord. The meninges serve as mechanical protection of the CNS. The meninges also support the cerebral and spinal blood vessels and allow for passage of the CSF. The subarachnoid space is filled with CSF. Only the subarachnoid space is a true space present in physiologic conditions, whereas the epidural and subdural spaces form only because of pathologic processes. The subdural space opens if the arachnoid mater separates from the dura mater, most commonly because of trauma and pathologic processes.
Image by Lecturio.
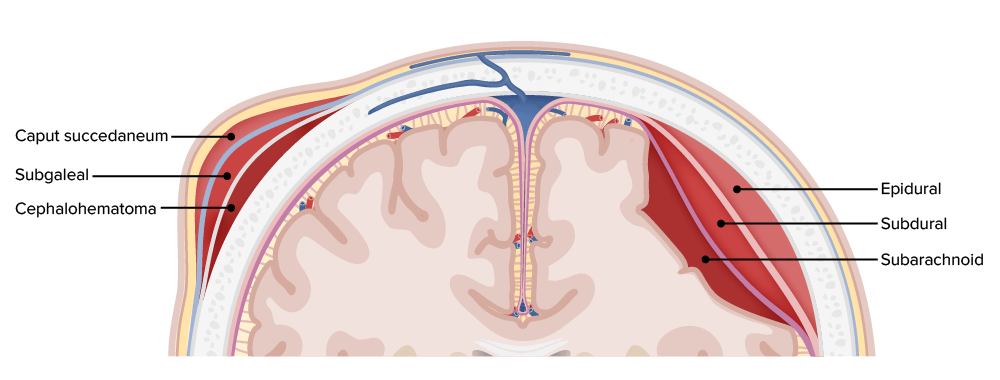
Hemorrhages by location within the different layers of the meninges and scalp
Image by Lecturio.
Epidemiology[1,11]
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency:
10% of cases of head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma necessitating hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
20% of cases of severe traumatic brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification injuries (TBIs)
More common in persons on antiplatelet/anticoagulant therapies
Etiology[1,11]
SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage is caused by rupture of vasculature (typically bridging veinsBridging VeinsSubdural Hemorrhage) between the arachnoid and dural meningeal layers. The primary etiology is trauma.
Acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage:
Blunt head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma (e.g., impact during road traffic accident)
Nonaccidental trauma (e.g., shaken baby syndromeShaken baby syndromeBrain injuries resulted from vigorous shaking of an infant or young child held by the chest, shoulders, or extremities causing extreme cranial acceleration. It is characterized by the intracranial and intraocular hemorrhages with no evident external trauma. Serious cases may result in death.Child Abuse)
Chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage:
Traumatic:
In adults, falls:
Especially in older adults and those with alcohol use disorderAlcohol use disorderAlcohol is one of the most commonly used addictive substances in the world. Alcohol use disorder (AUD) is defined as pathologic consumption of alcohol leading to impaired daily functioning. Acute alcohol intoxication presents with impairment in speech and motor functions and can be managed in most cases with supportive care. Alcohol Use Disorder
Often from standing height
In infants:
Shaken baby syndromeShaken baby syndromeBrain injuries resulted from vigorous shaking of an infant or young child held by the chest, shoulders, or extremities causing extreme cranial acceleration. It is characterized by the intracranial and intraocular hemorrhages with no evident external trauma. Serious cases may result in death.Child Abuse
Birth trauma
Nontraumatic:
Intracranial hypotensionIntracranial hypotensionReduction of cerebrospinal fluid pressure characterized clinically by orthostatic headache and occasionally by an abducens nerve palsy; hearing loss; nausea; neck stiffness, and other symptoms. This condition may be spontaneous or secondary to cerebrospinal fluid leak; spinal puncture; neurosurgical procedures; dehydration; uremia; trauma; and other processes. Chronic hypotension may be associated with subdural hematomas or hygromas.Subdural Hemorrhage (low CSF volume, usually due to a leak)
Spontaneous: connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology disorders, cerebral amyloid angiopathyAmyloid angiopathyA heterogeneous group of sporadic or familial disorders characterized by amyloid deposits in the walls of small and medium sized blood vessels of cerebral cortex and meninges. Clinical features include multiple, small lobar cerebral hemorrhage; cerebral ischemia; and cerebral infarction. Cerebral amyloid angiopathy is unrelated to generalized amyloidosis. Amyloidogenic peptides in this condition are nearly always the same ones found in alzheimer disease.Alzheimer Disease
IatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome: epidural, lumbar punctureLumbar PunctureFebrile Infant
The larger space between the dural membrane and the cortical surface of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification stretches the bridging veinsBridging VeinsSubdural Hemorrhage, increasing the risk of tearing.
Due to:
Advanced age
Chronic alcoholismAlcoholismA primary, chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be continuous or periodic.Wernicke Encephalopathy and Korsakoff Syndrome
Neurodegenerative diseases
Chronic diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
Previous traumatic brain injuryTraumatic brain injuryA form of acquired brain injury which occurs when a sudden trauma causes damage to the brain.Le Fort Fractures
Increased risk of hemorrhage due to:
Antithrombotic therapy (e.g., aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs), clopidogrelClopidogrelA ticlopidine analog and platelet purinergic p2y receptor antagonist that inhibits adenosine diphosphate-mediated platelet aggregation. It is used to prevent thromboembolism in patients with arterial occlusive diseases; myocardial infarction; stroke; or atrial fibrillation.Antiplatelet Drugs, direct oral anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants)
Coagulopathy (e.g., thrombocytopeniaThrombocytopeniaThrombocytopenia occurs when the platelet count is < 150,000 per microliter. The normal range for platelets is usually 150,000-450,000/µL of whole blood. Thrombocytopenia can be a result of decreased production, increased destruction, or splenic sequestration of platelets. Patients are often asymptomatic until platelet counts are < 50,000/µL. Thrombocytopenia, liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease, hemophiliaHemophiliaThe hemophilias are a group of inherited, or sometimes acquired, disorders of secondary hemostasis due to deficiency of specific clotting factors. Hemophilia A is a deficiency of factor VIII, hemophilia B a deficiency of factor IX, and hemophilia C a deficiency of factor XI. Patients present with bleeding events that may be spontaneous or associated with minor or major trauma.Hemophilia)
Vascular malformation
Intracranial aneurysmIntracranial aneurysmAbnormal outpouching in the wall of intracranial blood vessels. Most common are the saccular (berry) aneurysms located at branch points in circle of willis at the base of the brain. Vessel rupture results in subarachnoid hemorrhage or intracranial hemorrhages. Giant aneurysms (>2. 5 cm in diameter) may compress adjacent structures, including the oculomotor nerve.Brain Aneurysms
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
AtherosclerosisAtherosclerosisAtherosclerosis is a common form of arterial disease in which lipid deposition forms a plaque in the blood vessel walls. Atherosclerosis is an incurable disease, for which there are clearly defined risk factors that often can be reduced through a change in lifestyle and behavior of the patient. Atherosclerosis
BrainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and ClassificationtumorTumorInflammation/neoplasm (primary or metastatic)
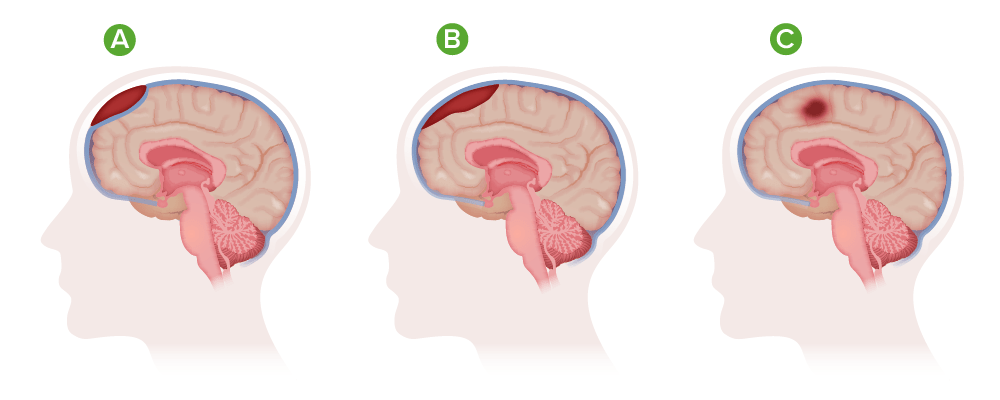
Types of hematoma: A) Epidural; B) Subdural; C) Intracranial
SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage occurs because of bleeding within the subdural spaceSubdural spacePotential cavity which separates the arachnoid mater from the dura mater.Subdural Hemorrhage. This may resolve by resorption or may become chronic by membranous encapsulation.[1,6]
Acute subdural hematomaAcute Subdural HematomaAccumulation of blood in the subdural space with acute onset of neurological symptoms. Symptoms may include loss of consciousness, severe headache, and deteriorating mental status.Subdural Hemorrhage:[1]
Rupture of small arteriesSmall arteriesArteries: Histology (< 1 mm diameter), which are often in the temporoparietal area, can also contribute to SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage formation (seen in 30%).
Blood then collects between layers. HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception is crescent-shaped (following the contours of the dura).
Bleeding is blocked by rising ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) or direct compressionCompressionBlunt Chest Trauma by the forming thrombus.
Intracranial hypotensionIntracranial hypotensionReduction of cerebrospinal fluid pressure characterized clinically by orthostatic headache and occasionally by an abducens nerve palsy; hearing loss; nausea; neck stiffness, and other symptoms. This condition may be spontaneous or secondary to cerebrospinal fluid leak; spinal puncture; neurosurgical procedures; dehydration; uremia; trauma; and other processes. Chronic hypotension may be associated with subdural hematomas or hygromas.Subdural Hemorrhage:
Low CSF pressure decreases brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification buoyancy → traction on meningeal support → vascular rupture
Even minor trauma or whiplash injury can result in SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage.
Chronic subdural hematomaChronic Subdural HematomaAccumulation of blood in the subdural space with delayed onset of neurological symptoms. Symptoms may include loss of consciousness, severe headache, and deteriorating mental status.Subdural Hemorrhage:[1]
Forms from an acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage that has thrombosed:
FibroblastsFibroblastsConnective tissue cells which secrete an extracellular matrix rich in collagen and other macromolecules.Sarcoidosis elaborate collagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology over the dural layer, stabilizing the outer surface of the thrombus.
Thinner membrane develops over the inner surface of the clot → complete encapsulation
Process takes approximately 2 weeks.
Formation of subdural hygroma:
Occurs with accumulation of cerebrospinal fluidCerebrospinal FluidA watery fluid that is continuously produced in the choroid plexus and circulates around the surface of the brain; spinal cord; and in the cerebral ventricles.Ventricular System: Anatomy (CSF) within the subdural spaceSubdural spacePotential cavity which separates the arachnoid mater from the dura mater.Subdural Hemorrhage
A tear in the arachnoid and the dural border cell layer allows passage of CSF → formation of hygroma
Hygroma is protein-rich, thus, is a potential osmotic draw of fluid into the cavity, leading to the expansion of the hygroma.
Acute-on-chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage:[1,8]
Recurrent trauma may cause bleeding into an otherwise stable (i.e., thrombosed) SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage or hygroma causing enlargement.
Older patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship and alcoholicAlcoholicPersons who have a history of physical or psychological dependence on ethanol.Mallory-Weiss Syndrome (Mallory-Weiss Tear)patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are at an increased risk (↑ risk of falls, causing recurrent traumatic injuries).
Clinical Presentation
Neurologic presentation depends on the size, location, and rate of growth of the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception, as well as the length of time since the initiating event.[1,6]
Onset of symptoms:[3,6]
Acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage: presents immediately (up to 72 hours after the event)
Subacute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage presents 3–21 days after the event.
Chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage presents > 21 days after the event.
In the absence of trauma, SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage may be difficult to categorize.
Neurologic symptoms and signs:[5]
Nature of neurologic symptoms/signs depend largely on the following characteristics of the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception:
Location
Size
Rate of growth
Acuity
Acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage:
½ present as comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Delayed acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage may present with Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma) 15 and negative CT in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship on antiplatelet/anticoagulant therapy; deterioration occurs within 24 hours.
Subacute or chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage may present with gradual deterioration in level of consciousness/somnolence/depression.
Features of raised ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP):
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Focal neurologic deficitsNeurologic DeficitsHigh-Risk Headaches (dependent on brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification region affected):
Cranial nerve palsiesCranial Nerve PalsiesCranial nerve palsy is a congenital or acquired dysfunction of 1 or more cranial nerves that will, in turn, lead to focal neurologic abnormalities in movement or autonomic dysfunction of its territory. Head/neck trauma, mass effect, infectious processes, and ischemia/infarction are among the many etiologies for these dysfunctions. Diagnosis is initially clinical and supported by diagnostic aids. Management includes both symptomatic measures and interventions aimed at correcting the underlying cause.Cranial Nerve Palsies
Nuchal rigidityNuchal RigidityMeningitis (presence with SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage usually indicates concomitant subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage).
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
Abnormal posturing:
Decorticate (flexor)
Decerebrate (extensor)
Chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage:
Altered mental state:
DeliriumDeliriumDelirium is a medical condition characterized by acute disturbances in attention and awareness. Symptoms may fluctuate during the course of a day and involve memory deficits and disorientation. Delirium
Somnolence
Progression to comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Cognitive decline:
Impaired memoryMemoryComplex mental function having four distinct phases: (1) memorizing or learning, (2) retention, (3) recall, and (4) recognition. Clinically, it is usually subdivided into immediate, recent, and remote memory.Psychiatric Assessment/dementiaDementiaMajor neurocognitive disorders (NCD), also known as dementia, are a group of diseases characterized by decline in a person’s memory and executive function. These disorders are progressive and persistent diseases that are the leading cause of disability among elderly people worldwide.Major Neurocognitive Disorders
Confusion
Personality changes
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
Diagnosis
Suspect SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage in any elderly person presenting with head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma, altered mental statusAltered Mental StatusSepsis in Children, decreased level of consciousness, or neurologic symptoms/signs. Head CT should be performed emergently.[3,6]
History and examination[6]
Features:
Recent history of trauma
Neurologic signs and symptoms (e.g., loss of consciousness or period of decreased alertness, potential seizure activity)
Inquire about:
Use of aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs), antithrombotics, or anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants
History of liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease, renal disease, or bleeding disordersBleeding disordersHypocoagulable conditions, also known as bleeding disorders or bleeding diathesis, are a diverse group of diseases that result in abnormal hemostasis. Physiologic hemostasis is dependent on the integrity of endothelial cells, subendothelial matrix, platelets, and coagulation factors. The hypocoagulable states result from abnormalities in one or more of these contributors, resulting in ineffective thrombosis and bleeding.Hypocoagulable Conditions
PeriorbitalPeriorbitalOrbital and Preseptal Cellulitis or retroauricular ecchymosisEcchymosisExtravasation of blood into the skin, resulting in a nonelevated, rounded or irregular, blue or purplish patch, larger than a petechia.Orbital Fractures, otorrheaOtorrheaOtitis Externa, or rhinorrheaRhinorrheaExcess nasal drainage.Respiratory Syncytial Virus (may indicate occult basilar skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: AnatomyfractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures).
Check cervical spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy in all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with suspected head injury (immobilize until injury is ruled out)
Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma)
NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant[3,6,10,11]
Noncontrast head CT:
Imaging method of choice (1st line):
For acute head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma
For acute loss of consciousness
For suspected SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage (and other intracranial bleeds)
Characteristic findings:
Morphology:
Crescent-shaped, concave collection of blood along the convexity of the affected hemisphere
Can cross cranial suture lines
Does not cross the midline (subdural spaceSubdural spacePotential cavity which separates the arachnoid mater from the dura mater.Subdural Hemorrhage is bound by the falx cerebri)
Can cause midline shift if unilateral
Density depends on duration:
Acute: hyperdense
Subacute: heterogeneously hyperdense/isodense
Chronic: hypodense
Acute on chronic: hyperdense regions superimposed on hypodense or isodense regions
Unilateral SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage creates an obvious distortionDistortionDefense Mechanisms of cerebral contours.
Bilateral SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage may create symmetric distortionDistortionDefense Mechanisms of cerebral contours and be less obvious.
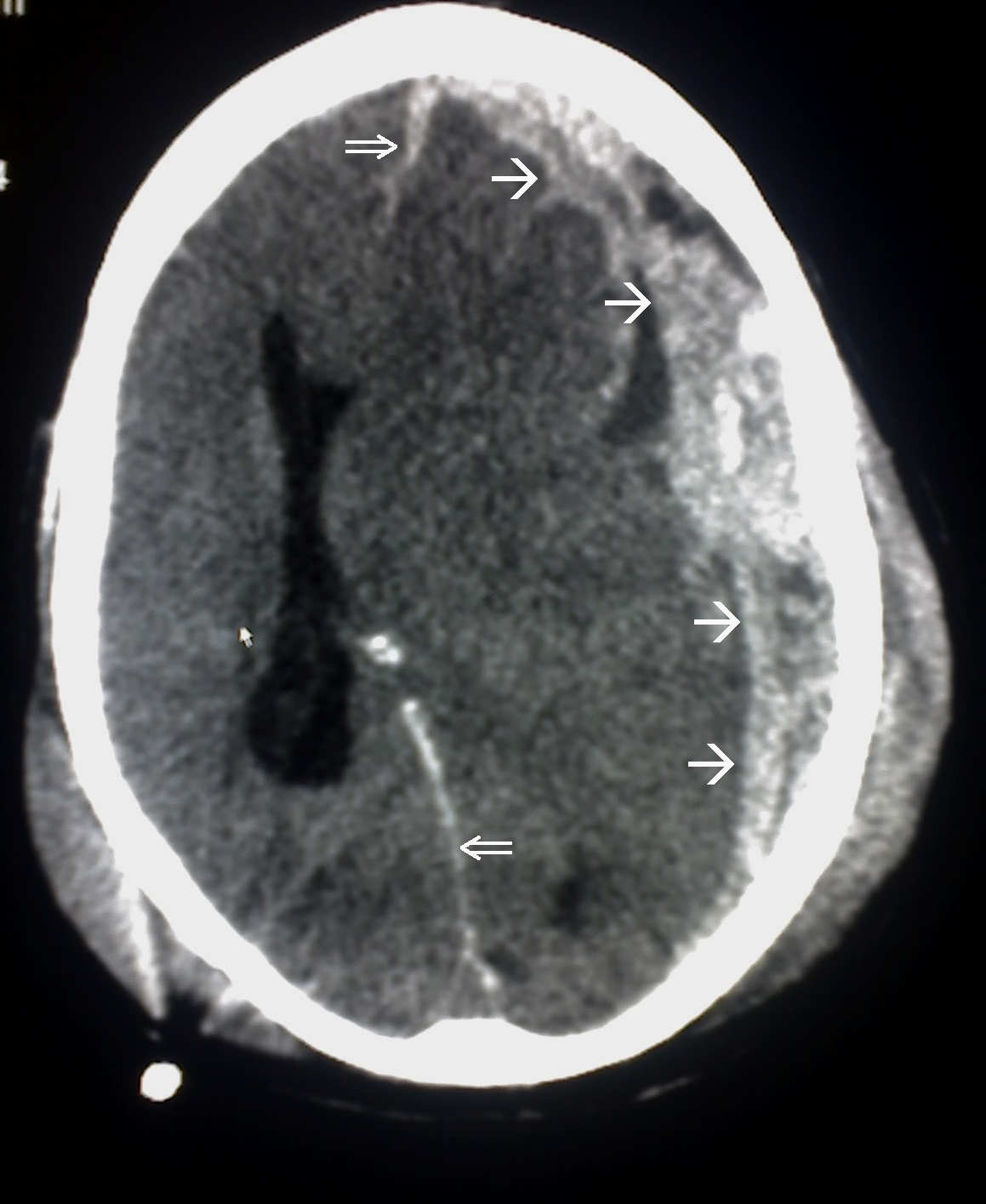
Subdural hemorrhage: Note the convexity of the hematoma and associated midline shift (with distortion of cerebral anatomy and obliteration of the lateral ventricle).
Image: “This CT scan is an example of Subdural haemorrhage caused by trauma. Single arrow marked the spread of the subdural haematoma. Double arrow marked the midline shift” by Glitzy queen00. License: Public Domain
Head MRI:
Indicated if neurologic features are not accounted for by CT head:
Sensitivity is superior to that of noncontrast CT in the detection of intracranial hemorrhageIntracranial hemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most sahs originate from a saccular aneurysm in the circle of willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use.Subarachnoid Hemorrhage.
May detect small SDHs that may be missed on noncontrast CT
May detect dural lesions (e.g., dural tears, neoplasm) missed on noncontrast CT
Can be used to elucidate the degree of brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification injury, including parenchymal microhemorrhages, diffuse axonal injuryDiffuse axonal injuryA relatively common sequela of blunt head injury, characterized by a global disruption of axons throughout the brain. Associated clinical features may include neurobehavioral manifestations; persistent vegetative state; dementia; and other disorders.Head Trauma, and areas of ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
Not as readily available as CT
AngiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery:
Used to determine the etiology of a nontraumatic/idiopathicIdiopathicDermatomyositisSDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage
Options include digital subtraction, MRMRCalculated as the ratio of the total number of people who die due to all causes over a specific time period to the total number of people in the selected population.Measures of Health Status, and CT angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery.
Noninvasive MRAMRAImaging of the Heart and Great Vessels or CTACTAA non-invasive method that uses a ct scanner for capturing images of blood vessels and tissues. A contrast material is injected, which helps produce detailed images that aid in diagnosing vascular diseases.Pulmonary Function Tests:
Indicated for evaluation of nontraumatic or idiopathicIdiopathicDermatomyositisSDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage
May reveal small intracranial aneurysms or other vascular lesions
Conventional angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery may be considered if a vascular lesion is suspected but not detected by noninvasive angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery.
Contraindicated when SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage is suspected
Increased ICPIncreased ICPExcessive accumulation of cerebrospinal fluid within the cranium which may be associated with dilation of cerebral ventricles, intracranial.Subarachnoid Hemorrhage due to expanding hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception increases risk of herniationHerniationOmphalocele and death.
Acute SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage, especially that presenting with neurologic compromise or comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma, is an emergent neurologic situation often requiring surgical intervention. Failure to promptly stabilize, diagnose, evaluate, and intervene could result in hemorrhagic expansion, parenchymal brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification injury, elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and ClassificationherniationHerniationOmphalocele, and death.[1,3,6,7]
Stabilization[6,7.9–11]
Individual should be evaluated and stabilized using advanced trauma life support/advanced cardiac life support (ATLS/ACLS) protocols.
Address life-threatening injuries.
Immediately discontinue (and possibly reverse) antiplateletsAntiplateletsDrugs or agents which antagonize or impair any mechanism leading to blood platelet aggregation, whether during the phases of activation and shape change or following the dense-granule release reaction and stimulation of the prostaglandin-thromboxane system.Heart Failure and Chronic Coronary Syndrome Medication/anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants.
Monitor serial labs:
Prothrombin timeProthrombin timeClotting time of plasma recalcified in the presence of excess tissue thromboplastin. Factors measured are fibrinogen; prothrombin; factor V; factor VII; and factor X.Hemostasis, partial thromboplastin timePartial thromboplastin timeThe time required for the appearance of fibrin strands following the mixing of plasma with phospholipid platelet substitute (e.g., crude cephalins, soybean phosphatides). It is a test of the intrinsic pathway (factors VIII, IX, XI, and XII) and the common pathway (fibrinogen, prothrombin, factors V and X) of blood coagulation.Hemostasis, and international normalized ratioInternational normalized ratioSystem established by the world health organization and the international committee on thrombosis and hemostasis for monitoring and reporting blood coagulation tests. Under this system, results are standardized using the international sensitivity index for the particular test reagent/instrument combination used.Hemostasis
Platelet count
FibrinogenFibrinogenPlasma glycoprotein clotted by thrombin, composed of a dimer of three non-identical pairs of polypeptide chains (alpha, beta, gamma) held together by disulfide bonds. Fibrinogen clotting is a sol-gel change involving complex molecular arrangements: whereas fibrinogen is cleaved by thrombin to form polypeptides a and b, the proteolytic action of other enzymes yields different fibrinogen degradation products.Hemostasis levels
Options for warfarinWarfarinAn anticoagulant that acts by inhibiting the synthesis of vitamin K-dependent coagulation factors. Warfarin is indicated for the prophylaxis and/or treatment of venous thrombosis and its extension, pulmonary embolism, and atrial fibrillation with embolization. It is also used as an adjunct in the prophylaxis of systemic embolism after myocardial infarction. Warfarin is also used as a rodenticide.Anticoagulants reversal:
ProthrombinProthrombinA plasma protein that is the inactive precursor of thrombin. It is converted to thrombin by a prothrombin activator complex consisting of factor Xa, factor V, phospholipid, and calcium ions.Hemostasis complex concentrate
Vitamin KVitamin KA lipid cofactor that is required for normal blood clotting. Several forms of vitamin K have been identified: vitamin K 1 (phytomenadione) derived from plants, vitamin K 2 (menaquinone) from bacteria, and synthetic naphthoquinone provitamins, vitamin K 3 (menadione). Vitamin k 3 provitamins, after being alkylated in vivo, exhibit the antifibrinolytic activity of vitamin k. Green leafy vegetables, liver, cheese, butter, and egg yolk are good sources of vitamin k.Fat-soluble Vitamins and their Deficiencies
Consult hematology on reversal options in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship taking direct oral anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants.
ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus admission
Serial neurologic examination
Head elevation 30–45°
Maintain SpO2 ≥ 94% (mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing when indicated)
Avoid hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (maintain SBPSBPAscites at ≥ 100 mm Hg for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship 50–69 years old or at ≥ 110 mm Hg for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship 15–49 or > 70 years old).
Manage temperature to prevent feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever.
AnalgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts and sedation as indicated (to reduce agitationAgitationA feeling of restlessness associated with increased motor activity. This may occur as a manifestation of nervous system drug toxicity or other conditions.St. Louis Encephalitis Virus)
Additional interventions:
Central line insertion
End-tidal CO₂ monitoring
Consider antiseizure medication (e.g., levetiracetamLevetiracetamA pyrrolidinone and acetamide derivative that is used primarily for the treatment of seizures and some movement disorders, and as a nootropic agent.Second-Generation Anticonvulsant Drugs or phenytoinPhenytoinAn anticonvulsant that is used to treat a wide variety of seizures. The mechanism of therapeutic action is not clear, although several cellular actions have been described including effects on ion channels, active transport, and general membrane stabilization. Phenytoin has been proposed for several other therapeutic uses, but its use has been limited by its many adverse effects and interactions with other drugs.First-Generation Anticonvulsant Drugs):
If seizure occurs beyond the 1st 7 days, consult neurology.
Consider arterial line for continuous blood pressure monitoring.
Avoid hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Maintain hemoglobin > 7 g/dL.
Manage raised intracranial pressureIntracranial PressureIdiopathic Intracranial Hypertension (ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP)):
ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitoring with ventriculostomyVentriculostomySurgical creation of an opening in a cerebral ventricle.Neurosurgery, subarachnoid bolt, or intraparenchymal monitor in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score < 9.
ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) < 20 mm Hg (in adults)
Emergent neurosurgical consultation:
Surgical clinical decision-making
Placement of ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitoring device
Stratification[1,6]
Clinical decision tools used to determine operative or nonoperative management include:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score
Head CT findings:
Clot thickness
Degree of midline shift
Presence of associated brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification lesion
Neurologic examination
Presence of pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Acuity of SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage
Presence of comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus
Severity of associated trauma
Age
Nonoperative management[6,10,11]
May be appropriate for:
Clinically stable individuals (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score > 9)
Small hematomas (< 10 mm thickness on CT)
Absence of brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and ClassificationherniationHerniationOmphalocele signs by clinical and/or radiographic evaluation:
Absence of physical examination findings of elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) (e.g., patient has reactive, symmetric pupils)
Absence of elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) on neuromonitoring (should be < 20 mm Hg)
Should be monitored in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus with continuous ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitoring:
Perform serial neurologic examination at least every 1–2 hours in the 1st 24 hours.
Monitor mental status (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma), pupillary function, and sensorimotor function.
Serial head CT every 6–8 hours for 36 hours
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception may resolve through resorption over weeks.
Operative management[6,10,12]
May be appropriate for:
SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage of < 10 mm and midline shift < 5 mm but clinically unstable individuals:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score < 9, reduced by ≥ 2 from the time of injury to the time of evaluation
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score < 9,with pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies (fixed, or asymmetric pupils)
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score < 9 with ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) > 20 mm Hg (suspect in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with Cushing triad: hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, respiratory depression, bradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias)
Large hematomas (> 10 mm thickness on CT), regardless of GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score
Midline shift on CT > 5 mm, regardless of GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score
Structural lesion such as arteriovenous malformationArteriovenous malformationAbnormal formation of blood vessels that shunt arterial blood directly into veins without passing through the capillaries. They usually are crooked, dilated, and with thick vessel walls. A common type is the congenital arteriovenous fistula. The lack of blood flow and oxygen in the capillaries can lead to tissue damage in the affected areas.Erysipelas or fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures in the setting of SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage
Surgical indications for chronic SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage are similar to above, with post-operative recurrence also included.
Should be undertaken as soon as clinically feasible for individuals meeting these criteria (within 2–4 hours after onset of neurologic deterioration)
Surgical techniques:
CraniotomyCraniotomySurgical incision into the cranium.Neurosurgery with hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception evacuation: most commonly performed
Decompressive craniectomyDecompressive CraniectomyExcision of part of the skull. This procedure is used to treat elevated intracranial pressure that is unresponsive to conventional treatment.Neurosurgery
Subdural evacuation port system
Culprit vessel identificationIdentificationDefense Mechanisms and tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis may be undertaken simultaneously:
Traditional tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis with ligatures
Endovascular embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding of the middle meningeal arteryMiddle Meningeal ArteryEpidural Hemorrhage
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[1,6,10,11]
Approximately 50% in SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage requiring surgery
Approximately 40% if surgical intervention is prompt (2–4 hours after injury)
Approximately 85% if surgical intervention is delayed
Approximately 60%–70% in SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage presenting with comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma prior to evaluation
Age and GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score are the most important prognostic indicators.
Management after discharge[6,10]
Follow-up CT:
2–3 weeks after discharge
ASAP if with new neurologic symptoms (headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, dizzinessDizzinessAn imprecise term which may refer to a sense of spatial disorientation, motion of the environment, or lightheadedness.Lateral Medullary Syndrome (Wallenberg Syndrome), vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia)
NeurosurgeryNeurosurgeryNeurosurgery is a specialized field focused on the surgical management of pathologies of the brain, spine, spinal cord, and peripheral nerves. General neurosurgery includes cases of trauma and emergencies. There are a number of specialized neurosurgical practices, including oncologic neurosurgery, spinal neurosurgery, and pediatric neurosurgery. Neurosurgery follow-up
In patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship requiring anticoagulationAnticoagulationPulmonary Hypertension Drugs (e.g., atrial fibrillationAtrial fibrillationAtrial fibrillation (AF or Afib) is a supraventricular tachyarrhythmia and the most common kind of arrhythmia. It is caused by rapid, uncontrolled atrial contractions and uncoordinated ventricular responses. Atrial Fibrillation, venous thromboembolismThromboembolismObstruction of a blood vessel (embolism) by a blood clot (thrombus) in the blood stream.Systemic Lupus Erythematosus), discussion with cardiologist and/or hematologist is recommended to decide on restarting medication.
Differential Diagnosis
Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke: ischemic infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage of the cerebral parenchyma caused by occlusion of a cerebral artery by atherosclerotic lesions or cardioembolic emboli. Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke presents with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/altered level of consciousnessAltered Level of ConsciousnessIntracerebral Hemorrhage that depends on the size and location of infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage. Diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management includes initial stabilization, possible cerebrovascular intervention, addressing identifiable underlying etiologies (severe hypertensionSevere hypertensionA confirmed blood pressure ≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic.Uncontrolled Hypertension, embolus), and management of cardiovascular risk factors.
Other hemorrhagic cerebral conditions: Carotid/cerebral artery dissection, epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage, and intraparenchymal hemorrhage are other hemorrhagic manifestations of the cerebral vasculature that can present with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/altered level of consciousnessAltered Level of ConsciousnessIntracerebral Hemorrhage. Diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management depends on the hemorrhagic etiology and includes initial stabilization, neurosurgical/endovascular consultation, management of ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), and monitoring in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus.
These codes are used to diagnose a traumatic subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage, a bleed between the dura and arachnoid materArachnoid materA delicate membrane enveloping the brain and spinal cord. It lies between the pia mater and the dura mater. It is separated from the pia mater by the subarachnoid cavity which is filled with cerebrospinal fluid.Meninges: Anatomy, typically from tearing of bridging veinsBridging VeinsSubdural Hemorrhage. Codes specify acuity (acute, subacute, chronic).
Coding System
Code
Description
ICD-10-CM
S06.5X0A
Traumatic subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage without loss of consciousness, initial encounter
ICD-10-CM
I62.00
Nontraumatic subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage, unspecified
Evaluation & Workup:
A non-contrast CT scan of the head is the primary imaging modality for diagnosis, which shows a characteristic crescent-shaped hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception that conforms to the surface of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification.
Coding System
Code
Description
CPT
70450
Computed tomography, head or brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification; without contrast material
Procedures/Interventions:
Surgical treatment depends on the size and acuity of the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception. This code is for the creation of burr holes, a common procedure to drain a chronic subdural hematomaChronic Subdural HematomaAccumulation of blood in the subdural space with delayed onset of neurological symptoms. Symptoms may include loss of consciousness, severe headache, and deteriorating mental status.Subdural Hemorrhage.
Coding System
Code
Description
CPT
61108
Twist drill hole(s) for subdural or ventricular puncture
CPT
61312
Craniectomy or craniotomyCraniotomySurgical incision into the cranium.Neurosurgery for evacuation of hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception, supratentorial; extradural or subdural
Yang, A. I., Balser, D. S., Mikheev, A., et al. (2012). Cerebral atrophy is associated with development of chronic subdural haematoma. Brain Injury, 26, 1731–1736. https://doi.org/10.3109/02699052.2012.698364
Lee, K. S., Shim, J. J., Yoon, S. M., Doh, J. W., Yun, I. G., Bae, H. G. (2011). Acute-on-chronic subdural hematoma: not uncommon events. Journal of Korean Neurosurgical Society, 50(6), 512–516. https://doi.org/10.3340/jkns.2011.50.6.512
Hawryluk, G. W. J., Aguilera, S., Buki, A., Bulger, E., Citerio, G., Cooper, D. J., Arrastia, R. D., Diringer, M., Figaji, A., Gao, G., Geocadin, R., Ghajar, J., Harris, O., Hoffer, A., Hutchinson, P., Joseph, M., Kitagawa, R., Manley, G., Mayer, S., Menon, D. K., … Chesnut, R. M. (2019). A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Medicine, 45(12), 1783–1794. https://doi.org/10.1007/s00134-019-05805-9