Appendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting. The diagnosis can frequently be established clinically, but imaging is used in uncertain cases. Computed tomography (CT) scan provides the highest diagnostic accuracy. Perforation occurs in 13%–20% of cases and can present as localized (abscess/phlegmon) or free perforation with generalized peritonitis. The standard treatment is appendectomy, but localized perforations are frequently managed non-operatively with antibiotics.
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitisis the inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the vermiform appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy.
Epidemiology[1,4,5]
Lifetime risk: approximately 8%
6% of the population gets appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis.
Peak incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 10–19 years of age
Males > females
The most common acute surgical problem in the pediatric population
Etiology[1,4,18]
Obstruction of appendiceal orifice (implicated, but not often proven)
Cause of obstruction varies with age.
Children and young adults: lymphoid follicular hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation secondary to infection
Older adults:
Fecaliths
Calculi
FibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans
Escherichia coliEscherichia coliThe gram-negative bacterium Escherichia coli is a key component of the human gut microbiota. Most strains of E. coli are avirulent, but occasionally they escape the GI tract, infecting the urinary tract and other sites. Less common strains of E. coli are able to cause disease within the GI tract, most commonly presenting as abdominal pain and diarrhea. Escherichia coli
PeptostreptococcusPeptostreptococcusA genus of gram-positive, anaerobic, coccoid bacteria that is part of the normal flora of humans. Its organisms are opportunistic pathogens causing bacteremias and soft tissue infections.Perianal and Perirectal Abscess
PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas
Bacteroides fragilisBacteroides fragilisGram-negative bacteria occurring in the lower intestinal tracts of man and other animals. It is the most common species of anaerobic bacteria isolated from human soft tissue infections.Bacteroides
Increase in transmural pressure → thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus and occlusion of small vessels
IschemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage and necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage (gangreneGangreneDeath and putrefaction of tissue usually due to a loss of blood supply.Small Bowel Obstruction)
Eventual perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Vague periumbilical painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways develops.
Late:
Usually after 24 hours
Invasion of appendiceal wall by bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology + ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
PropagationPropagationPropagation refers to how the electrical signal spreads to every myocyte in the heart.Cardiac Physiology of neutrophilic exudateExudateExudates are fluids, cells, or other cellular substances that are slowly discharged from blood vessels usually from inflamed tissues.Pleural Effusion → fibropurulent reaction involving serosal surface
Peritoneal irritation → localized painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and tenderness
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis:
Affects 13%–20% of cases
In 65% of cases, symptoms last longer than 48 hours.
In 20% of cases, symptoms last less than 24 hours.
More likely with calculus as the obstructing culprit:
Walled-off perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis: abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease formation
Free perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis: generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
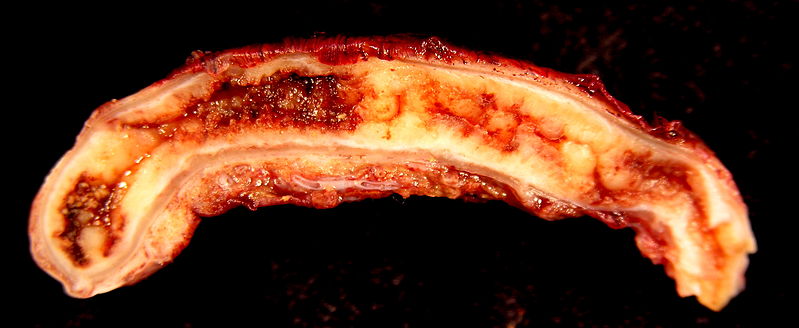
Acute appendicitis
Image: “Acute Appendicitis” by Ed Uthman. License: CC BY 2.0
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Atypical:
Indigestion
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Anterior appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy (most common): pronounced localized RLQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Pelvic: dysuriaDysuriaPainful urination. It is often associated with infections of the lower urinary tract.Urinary Tract Infections (UTIs), diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, tenesmus (from bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and rectal irritation)
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea/constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation may or may not be present.
Symptoms may be vague/atypical in the elderly.
Adults (eliminate other causes):
History of inflammatory bowel disease
History of colorectal cancerColorectal cancerColorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Colorectal Cancer/previous colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening
Reproductive/sexually transmitted diseases in women (rule out pelvic inflammatory diseasePelvic inflammatory diseasePelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and Gardnerella vaginalis. Pelvic Inflammatory Disease (PIDPIDPelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and gardnerella vaginalis.Pelvic Inflammatory Disease), ectopic pregnancyEctopic pregnancyEctopic pregnancy refers to the implantation of a fertilized egg (embryo) outside the uterine cavity. The main cause is disruption of the normal anatomy of the fallopian tube. Ectopic Pregnancy)
Children:
Most common in 5–12-year-olds
Very rare in neonates
Rule out viral illness:
History of concurrent or preceding respiratory symptoms
High feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever may indicate late appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis/necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage/perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
Desire to lie still, with difficulty ambulating (common in children)
Signs of dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration if prolonged vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia/anorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa:
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Orthostatic hypotensionOrthostatic hypotensionA significant drop in blood pressure after assuming a standing position. Orthostatic hypotension is a finding, and defined as a 20-mm hg decrease in systolic pressure or a 10-mm hg decrease in diastolic pressure 3 minutes after the person has risen from supine to standing. Symptoms generally include dizziness, blurred vision, and syncope.Hypotension
Rovsing’s signRovsing’s signA positive sign when there is pain in the RLQ with palpation of the left lower quadrantAppendicitis:painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the RLQ with palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination of the left lower quadrantLeft Lower quadrantAnterior Abdominal Wall: Anatomy
Obturator signObturator signWhen there is RLQ pain with internal hip rotation with a flexed knee (pelvic appendix)Appendicitis: RLQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways with internal hip rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays with a flexed knee (pelvic appendixPelvic appendixAppendicitis)
Generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury suggests perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
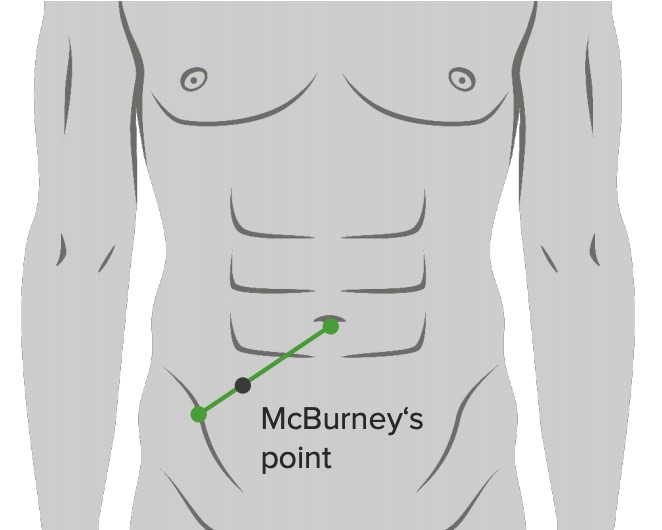
Location of the McBurney’s point: 2/3 from umbilicus on a straight line from the umbilicus to ASIS (anterior superior iliac spine)
Image by Lecturio.
Location of the McBurney’s point: 2/3 from umbilicus on a straight line from the umbilicus to ASIS (anterior superior iliac spine)
Image: “McBurney’s point” by Department of Basic Sciences, School of Medicine. Universidad de Caldas. Manizales, Colombia. License: CC BY 2.5
Rectal exam:
Not helpful for establishing appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis diagnosis
May be helpful if an alternative diagnosis is suspected
Pelvic exam:
May be needed in a female if PIDPIDPelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and gardnerella vaginalis.Pelvic Inflammatory Disease is suspected
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis (especially pelvic) may also produce tenderness on pelvic exam.
Chemistry may show dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration pattern: low K (potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia), low Na (sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia), metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children: may show mild pyuriaPyuriaThe presence of white blood cells (leukocytes) in the urine. It is often associated with bacterial infections of the urinary tract. Pyuria without bacteriuria can be caused by tuberculosis, stones, or cancer.Urinary Tract Infections (UTIs) due to proximity of the right ureter
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test: Perform on all females of reproductive age.
A numerical scaleScaleDermatologic Examination for predicting the likelihood of appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis based on clinical and laboratory findings
Migratory painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the right iliac fossa
1
Anorexia
1
Nausea and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
1
Signs
Tenderness in the right iliac fossa
2
Rebound tenderness
1
Elevated temperature
1
Laboratory findings
Leukocytosis
2
Shift to left
1
Total
10
Interpretation:
0–4: Appendicitis is less likely.
5–6: Appendicitis is possible; imaging evaluation needed
7–8: Appendicitis is probable → surgical consultation
9–10: Appendicitis is highly likely → surgical consultation
Imaging[2,5–7,9,16]
Imaging is not required for diagnosis if the Alvarado scoreAlvarado scoreAppendicitis is very low (< 3) or high (> 7).
Computed tomography (CT) scan:
Highest diagnostic accuracy
Should be performed with intravenous contrast unless contraindicated (renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome, allergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction)
Findings of appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis:
Appendiceal diameter > 6 mm (0.24 in) with occluded lumen
Preferred test in children and pregnant women as it avoids radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma
Signs of appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis:
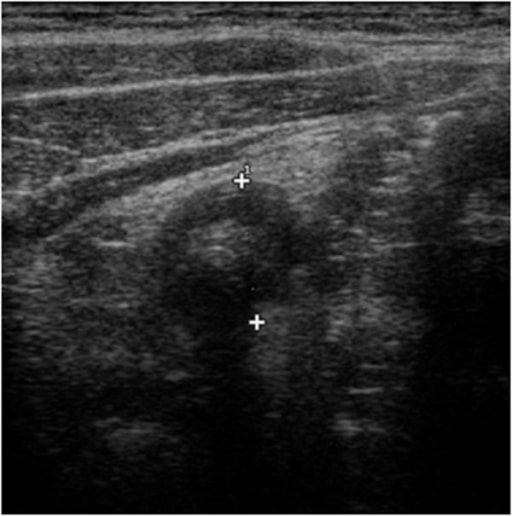
Focal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways with pressure from US probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography)
Ultrasound features of appendicitis: “target sign” characterized by a fluid-filled center and surrounded by an echogenic mucosa and submucosa and hypo-echoic muscularis
Image: “Ultrasound features of appendicitis” by Second University of Naples, Department of Clinical and Experimental Internistic F, Magrassi, Naples, Italy. License: CC BY 2.0
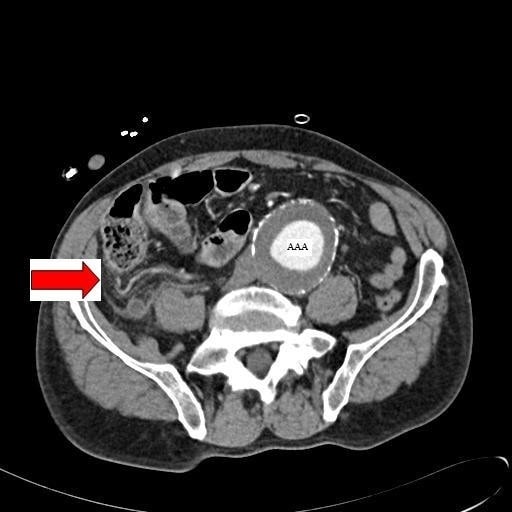
Abdominal CT image with contrast showing an inflamed appendix (marked by the red arrow) in a patient with a concomitant abdominal aortic aneurysm (AAA)
Image: “Abdominal CT” by Department of General Surgery, Queen Elizabeth Hospital, Queen Elizabeth Avenue, Sheriff Hill, Gateshead, Tyne & Wear, NE9 6SX, UK. License: CC BY 2.0
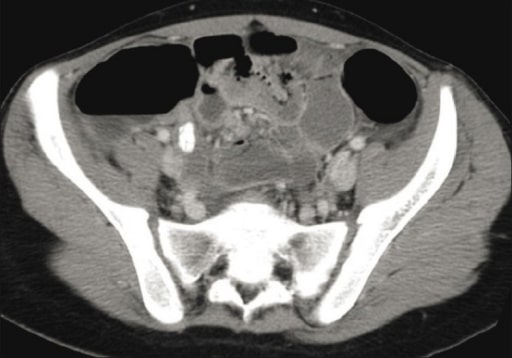
Pelvic CT image showing an inflamed appendix with an appendicolith
Image: “CT scan” by Department of Radiology, King Khalid University Hospital, King Saud University, Saudi Arabia. License: CC BY 2.0
Intravenous fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome (hydrate and replace electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes)
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics control
Uncomplicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
Definition: acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis without clinical or radiographic signs of perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Non-operative management (NOM):[5-7,10]
Growing evidence that non-perforated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis can be managed with antibiotics alone
90% will initially respond to antibiotics.
Indications:[10]
Localized appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis, without signs of diffuse peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
No imaging evidence of abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, or tumorTumorInflammation
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are unfit for surgery (multiple comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus) or who accept the risk of recurrence
The following are generally not candidates for NOM:
ImmunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are hemodynamically unstable or have sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Pregnant women:[19]
AppendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy is recommended owing to morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status, risk of preterm laborPreterm laborPreterm labor refers to regular uterine contractions leading to cervical change prior to 37 weeks of gestation; preterm birth refers to birth prior to 37 weeks of gestation. Preterm birth may be spontaneous due to preterm labor, preterm prelabor rupture of membranes (PPROM), or cervical insufficiency. Preterm Labor and Birth, and fetal loss.
NOM can serve as a bridge to surgery in remote areas or where skilled surgical staff is not available.
Adult antibiotic regimens:[5,8,11,16]
Single-agent regimen:
Cefoxitin
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam
MoxifloxacinMoxifloxacinA fluoroquinolone that acts as an inhibitor of DNA topoisomerase II and is used as a broad-spectrum antibacterial agent.Fluoroquinolones
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins (for high-severity infection)
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess PLUS 1 of the following:
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins
Cefuroxime
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins PLUS metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins
Penicillin-allergic: ciprofloxacinCiprofloxacinA broad-spectrum antimicrobial carboxyfluoroquinoline.Fluoroquinolones PLUS metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
Antibiotics course:
7–10 days
1–3 days IV, if on a nothing-by-mouth regimen or unable to tolerate oral intake
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are typically able to tolerate oral doses after 48 hours.
Switch to oral doses once able to tolerate
Recurrence rate of 20%–30% in the 1st year, and up to 39% in 5 years
Table: Adult antibiotic options for uncomplicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis[5,8,11,16]
Regimen
Antibiotic
Typical adult dose
Single-agent
Cefoxitin
1 g IV daily
ErtapenemErtapenemA carbapenem derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of gram-positive and gram-negative bacterial infections including intra-abdominal infections, acute gynecological infections, complicated urinary tract infections, skin infections, and respiratory tract infections. It is also used to prevent infection in colorectal surgery.Carbapenems and Aztreonam
1 g IV daily
MoxifloxacinMoxifloxacinA fluoroquinolone that acts as an inhibitor of DNA topoisomerase II and is used as a broad-spectrum antibacterial agent.Fluoroquinolones
400 mg orally or IV daily
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins
3.375g IV every 6 hours
Multi-agent (metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess + 1 additional agent)
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
500 mg orally or IV every 8 hours
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins
1–2 g IV every 8 hours
Cefuroxime
1.5 g IV every 8 hours
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins
Table: Pediatric antibiotic options for uncomplicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis[8,14]
Regimen
Antibiotic
Typical adult dose
Single-agent
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins
Patient over 9 months of age and ≤ 40 kg:
100 mg/kg/dose IV every 8 hours
Maximum: 3 g of piperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins/dose
Patient > 40 kg:
3 g IV every 6 hours
Maximum dose: 16 g piperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins/day
Multi-agent (metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess + 1 additional agent)
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
Either:
10 mg/kg/dose IV every 8 hours
30 mg/kg/dose IV daily*
Maximum: 1,500 mg/day
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins
AppendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy:[5,6]
Timing:
Delay of 12–24 hours does not increase morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status or risk for complicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis.
Delay beyond 24 hours, however, increases adverse outcomes.
Performed in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are fit for surgery and do not accept the risks of possible recurrence.
Preoperative antibiotics are indicated and should be given within 60 min of the start of the procedure.[12]
Cefoxitin 2 g IV every 2 hours if redose needed; OR
Cefotetan 2 g IV every 6 hours if redose needed; OR
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess 500 mg IV plus cefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins:
For < 120 kg, give 2 g IV every 4 hours (if redose needed)
For 120 kg, give 3 g IV every 4 hours (if redose needed)
Penicillin- or cephalosporin-allergic: clindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides 900 mg IV one dose, PLUS 1 of the following:
CiprofloxacinCiprofloxacinA broad-spectrum antimicrobial carboxyfluoroquinoline.Fluoroquinolones 400 mg IV, one dose
AztreonamAztreonamThe carbapenems and aztreonam are both members of the bactericidal beta-lactam family of antibiotics (similar to penicillins). They work by preventing bacteria from producing their cell wall, ultimately leading to bacterial cell death. Carbapenems and Aztreonam 2 g IV, one dose
Cefoxitin 40 mg/kg IV; maximum dose: 2 g every 2 hours if redose needed, OR
Cefotetan 40 mg/kg IV; maximum dose: 2 g every 6 hours if redose needed, OR
CeftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins 50–75 mg/kg IV
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins:
Over 9 months and ≤ 40 kg: 100 mg/kg IV; maximum dose: 3 g piperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins/dose
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess 15 mg/kg; maximum dose: 500 mg
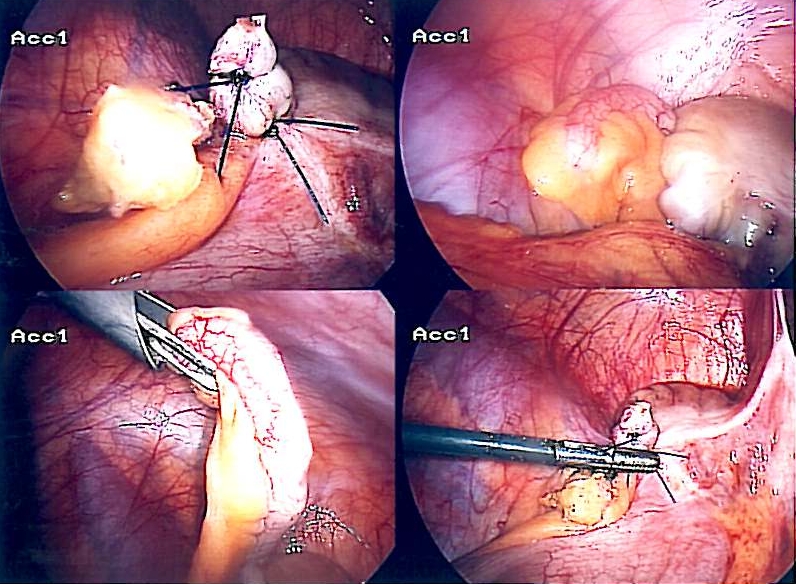
Approach:
Laparoscopic:
Lower rate of wound infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Less painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways on postoperative day 1
Shorter hospital stay
Open:
Lower rate of intra-abdominal infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Image: “Appendix-Entfernung” by Life-of-hannes.de. License: Public Domain
Complicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
Definition: appendiceal rupture with or without phlegmon or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease formation
Initial non-operative management:[5,7,8]
Preferred approach as immediate surgery has high risk of complications:
More extensive surgery (ileocecectomy) may be required.
Risk of postoperative abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula
Indicated for contained perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis:
Cecal phlegmon or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease > 3 cm (1.18 in) on CT scan
Stable patient without diffuse peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
Components of management:
Radiologically guided drainage of an abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease
IV antibiotics: broad-spectrumBroad-SpectrumFluoroquinolones enteric coverageincluding EnterobacteriaceaeEnterobacteriaceaeA family of gram-negative, facultatively anaerobic, rod-shaped bacteria that do not form endospores. Its organisms are distributed worldwide with some being saprophytes and others being plant and animal parasites. Many species are of considerable economic importance due to their pathogenic effects on agriculture and livestock.Cephalosporins (nonresistant), streptococci, and anaerobesAnaerobesLincosamides (See NOM section for antibiotics)
IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids and bowel rest
Successful (patient is discharged home with 7–10-day course of oral antibiotics):
↓ PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
↓ FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Unsuccessful: rescue appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy during the same admission
Interval appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy:[5,6,17]
Generally performed 6–8 weeks after successful nonoperative management:
To prevent recurrence of appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
To exclude appendiceal neoplasm
If not performed, proponents of interval appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy cite the following risks:
Although there are benefits, some argue against routine interval appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy (after NOM for complicated appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis) in those who are < 40 years old and in children, citing:
High rate of resolution after NOM
High incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of no future events in majority of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Shared decision-making is recommended regarding the procedure.
ColonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening should also be considered for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship > 40 years of age because of the increased risk of malignancyMalignancyHemothorax in this age group.
Immediate appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy:[5,18]
Always indicated for unstable patient with generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury/free perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
May require more extensive resection (ileocecectomy)
Requires washout and drainage of peritoneal cavityPeritoneal CavityThe space enclosed by the peritoneum. It is divided into two portions, the greater sac and the lesser sac or omental bursa, which lies behind the stomach. The two sacs are connected by the foramen of winslow, or epiploic foramen.Peritoneum: Anatomy
Can also be performed for contained perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis with small phlegmon or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease (< 3 cm (1.18 in))
Postoperative antibiotics are recommended:
Duration:
Adults, 3–5-day course (see NOM section for antibiotic regimens)
Children, < 7-day course (see NOM section for antibiotic regimens)
Longer course may be needed in cases of:
Incomplete drainage
Presence of catheters
Surgical complicationsSurgical complicationsSurgical complications are conditions, disorders, or adverse events that occur following surgical procedures. The most common general surgical complications include bleeding, infections, injury to the surrounding organs, venous thromboembolic events, and complications from anesthesia.Surgical Complications
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[5,6]
Complications of appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy:
Wound infection: 3.3%–10.3%
Pelvic/abdominal abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease: 9.4%
GastroenteritisGastroenteritisGastroenteritis is inflammation of the stomach and intestines, commonly caused by infections from bacteria, viruses, or parasites. Transmission may be foodborne, fecal-oral, or through animal contact. Common clinical features include abdominal pain, diarrhea, vomiting, fever, and dehydration.Gastroenteritis: acute self-limited viral illness presenting with abdominal painAbdominal PainAcute Abdomen, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, and diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea. Imaging and labs may be largely normal. Condition is treated supportively with bowel rest and intravenous hydration.
Mesenteric lymphadenitisMesenteric LymphadenitisInflammation of lymph nodes in the mesentery.Pediatric Gastrointestinal Abnormalities: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of mesenteric lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy associated with acute or chronic abdominal painAbdominal PainAcute Abdomen. Mesenteric lymphadenitisMesenteric LymphadenitisInflammation of lymph nodes in the mesentery.Pediatric Gastrointestinal Abnormalities commonly localizes to RLQ because of a large number of lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy in that area. Computed tomography scan/US will show lymphadenopathyLymphadenopathyLymphadenopathy is lymph node enlargement (> 1 cm) and is benign and self-limited in most patients. Etiologies include malignancy, infection, and autoimmune disorders, as well as iatrogenic causes such as the use of certain medications. Generalized lymphadenopathy often indicates underlying systemic disease. Lymphadenopathy.
Epiploic appendagitis: ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage/infarction of the colonic fatty appendages. Epiploic appendagitis presents with acute or subacute lower abdominal painAbdominal PainAcute Abdomen. Computed tomography scan can confirm the diagnosis. Usually, this self-limited illness is treated with oral anti-inflammatory medications.
Meckel’s diverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of Meckel’s diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease. The condition may be impossible to clinically distinguish from acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis as the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is similar; however, it may be more central or left-sided. Occasionally, there is a history of intermittent lower gastrointestinal bleedingGastrointestinal bleedingGastrointestinal bleeding (GIB) is a symptom of multiple diseases within the gastrointestinal (GI) tract. Gastrointestinal bleeding is designated as upper or lower based on the etiology’s location to the ligament of Treitz. Depending on the location of the bleeding, the patient may present with hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (fresh blood in stools). Gastrointestinal Bleeding. Computed tomography scan may or may not be diagnostic. Sometimes, diagnosis is made during surgery.
Right-sided diverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of colonic diverticula. Usually left-sided, but right-sided presentation can also occur, especially in young patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship and in Asian populations. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with RLQ painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and change in bowel habits. Diagnosis is made by CT scan.
Terminal ileitis:inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy that can have an antecedent history of abdominal crampingAbdominal crampingNorovirus, weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, and diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea. The ileitis may be non-specific, due to Crohn’s disease or YersiniaYersiniaYersinia is a genus of bacteria characterized as gram-negative bacilli that are facultative anaerobic with bipolar staining. There are 2 enteropathogenic species that cause yersiniosis, Y. enterocolitica and Y. pseudotuberculosis. Infections are manifested as pseudoappendicitis or mesenteric lymphadenitis, and enterocolitis. Yersinia spp./Yersiniosis infection. Diagnosis is made acutely by CT scan. ColonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening (Crohn’s) and serum antibody titers (YersiniaYersiniaYersinia is a genus of bacteria characterized as gram-negative bacilli that are facultative anaerobic with bipolar staining. There are 2 enteropathogenic species that cause yersiniosis, Y. enterocolitica and Y. pseudotuberculosis. Infections are manifested as pseudoappendicitis or mesenteric lymphadenitis, and enterocolitis. Yersinia spp./Yersiniosis) can help establish the etiology.
Genitourinary
Right ureteric colic: obstructive stone in the right ureter that presents as intermittent (colicky) painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways of the right flankRight FlankSurgical Anatomy of the Abdomen/groinGroinThe external junctural region between the lower part of the abdomen and the thigh.Male Genitourinary Examination. UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children will show the presence of red blood cellsRed blood cellsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology. Diagnosis is established by non-contrast CT scan.
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection: bacterial infection of the urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy in the form of cystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs) (bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess infection) or right-sided acute pyelonephritisAcute pyelonephritisInflammation of the kidney involving the renal parenchyma (the nephrons); kidney pelvis; and kidney calices. It is characterized by abdominal pain; fever; nausea; vomiting; and occasionally diarrhea.Imaging of the Urinary System (kidney involvement). Presents with suprapubic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and dysuriaDysuriaPainful urination. It is often associated with infections of the lower urinary tract.Urinary Tract Infections (UTIs) (cystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs)) or right costovertebral angle tenderness and feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever (pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess). Diagnosis is made by urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children and CT scan.
Gynecologic
Right-sided ectopic pregnancyEctopic pregnancyEctopic pregnancy refers to the implantation of a fertilized egg (embryo) outside the uterine cavity. The main cause is disruption of the normal anatomy of the fallopian tube. Ectopic Pregnancy:pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care in the right fallopian tubeFallopian TubeA pair of highly specialized canals extending from the uterus to its corresponding ovary. They provide the means for ovum transport from the ovaries and they are the site of the ovum’s final maturation and fertilization. The fallopian tube consists of an interstitium, an isthmus, an ampulla, an infundibulum, and fimbriae. Its wall consists of three layers: serous, muscular, and an internal mucosal layer lined with both ciliated and secretory cells.Uterus, Cervix, and Fallopian Tubes: Anatomy. Presents with right-sided abdominal painAbdominal PainAcute Abdomen. When ruptured, can present with feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, and peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury. Usually, there is a history of a missed menstrual period. Findings include a positive pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways with cervical manipulation (pelvic exam). Diagnosis is confirmed with pelvic US.
PIDPIDPelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and gardnerella vaginalis.Pelvic Inflammatory Disease:sexually transmitted infectionSexually Transmitted InfectionSexually transmitted infections (STIs) are infections that spread either by vaginal intercourse, anal sex, or oral sex. Symptoms and signs may include vaginal discharge, penile discharge, dysuria, skin lesions (e.g., warts, ulcers) on or around the genitals, and pelvic pain. Some infections can lead to infertility and chronic debilitating disease.Sexually Transmitted Infections (STIs) involving internal reproductive organs, usually in a young adult woman. Pelvic inflammatory diseasePelvic inflammatory diseasePelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and Gardnerella vaginalis. Pelvic Inflammatory Disease presents with lower abdominal painAbdominal PainAcute Abdomen (mostly bilateral), feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and vaginal discharge. Diagnosis is established with pelvic exam and US.
Ovarian and fallopian tubeFallopian TubeA pair of highly specialized canals extending from the uterus to its corresponding ovary. They provide the means for ovum transport from the ovaries and they are the site of the ovum’s final maturation and fertilization. The fallopian tube consists of an interstitium, an isthmus, an ampulla, an infundibulum, and fimbriae. Its wall consists of three layers: serous, muscular, and an internal mucosal layer lined with both ciliated and secretory cells.Uterus, Cervix, and Fallopian Tubes: Anatomy torsion: causes acute ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage of the ovary/fallopian tubeFallopian TubeA pair of highly specialized canals extending from the uterus to its corresponding ovary. They provide the means for ovum transport from the ovaries and they are the site of the ovum’s final maturation and fertilization. The fallopian tube consists of an interstitium, an isthmus, an ampulla, an infundibulum, and fimbriae. Its wall consists of three layers: serous, muscular, and an internal mucosal layer lined with both ciliated and secretory cells.Uterus, Cervix, and Fallopian Tubes: Anatomy. Torsion presents with abdominal painAbdominal PainAcute Abdomen (RLQ if on the right), feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. When suspected, a DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography) pelvic US (looking at the blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure) should be performed. The condition can affect females of both adult and pediatric age.
Ruptured ovarian cyst (right): fluid or blood released from the cyst causes peritoneal irritation and acute onset of RLQ abdominal painAbdominal PainAcute Abdomen. Diagnosis is made by pelvic US.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis, an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy. It is critical to specify if there is perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis or an abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, as this changes management.
Coding System
Code
Description
ICD-10-CM
K35.80
Unspecified acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
ICD-10-CM
K35.2
Acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis with generalized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
ICD-10-CM
K35.32
Acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis with perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis and localized peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury, without abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease
Evaluation & Workup:
A CT scan of the abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy with contrast is the most accurate imaging study for confirming the diagnosis of appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis in adults and assessing for complications like perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
Coding System
Code
Description
CPT
74177
Computed tomography, abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy; with contrast material(s)
LaparoscopyLaparoscopyLaparoscopy is surgical exploration and interventions performed through small incisions with a camera and long instruments. Laparotomy and Laparoscopy, surgical, appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy
Di Saverio, S., et al. (2020). Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World Journal of Emergency Surgery, 15(1), 27. https://doi.org/10.1186/s13017-020-00306-3
Fugazzola, P., et al. (2020). The SIFIPAC/WSES/SICG/SIMEU guidelines for diagnosis and treatment of acute appendicitis in the elderly (2019 edition). World Journal of Emergency Surgery, 15(1), 19. https://doi.org/10.1186/s13017-020-00298-0
Moris, D., Paulson, E. K., Pappas, T. N. (2021). Diagnosis and management of acute appendicitis in adults: a review. JAMA, 326(22), 2299–2311. https://doi.org/10.1001/jama.2021.20502
Bom, W. J., Scheijmans, J., Salminen, P., Boermeester, M. A. (2021). Diagnosis of uncomplicated and complicated appendicitis in adults. Scandinavian Journal of Surgery, 110(2), 170–179. https://doi.org/10.1177/14574969211008330
Talan, D. A., Di Saverio, S. (2021). Treatment of acute uncomplicated appendicitis. New England Journal of Medicine, 385(12), 1116–1123. https://doi.org/10.1056/NEJMcp2107675
Talan, D. A., Saltzman, D. J., DeUgarte, D. A., Moran, G. J. (2019). Methods of conservative antibiotic treatment of acute uncomplicated appendicitis: a systematic review. Journal of Trauma and Acute Care Surgery, 86(4), 722–736. https://doi.org/10.1097/TA.0000000000002137
Andersen, B. R., Kallehave, F. L., Andersen, H. K. (2005). Antibiotics versus placebo for prevention of postoperative infection after appendicectomy. Cochrane Database of Systematic Reviews, 2005(3), CD001439. https://doi.org/10.1002/14651858.CD001439.pub2
Berríos-Torres, S. I., Umscheid, C. A., Bratzler, D. W., Leas, B., Stone, E. C., Kelz, R. R., Reinke, C. E., Morgan, S., Solomkin, J. S., Mazuski, J. E., Dellinger, E. P., Itani, K., Berbari, E. F., Segreti, J., Parvizi, J., Blanchard, J., Allen, G., Kluytmans, J., Donlan, R., Schecter, W. P., … Healthcare Infection Control Practices Advisory Committee. (2017). Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surgery, 152(8), 784–791. https://doi.org/10.1001/jamasurg.2017.0904
Minneci, P. C., Hade, E. M., Lawrence, A. E., et al. (2020). Association of nonoperative management using antibiotic therapy vs laparoscopic appendectomy with treatment success and disability days in children with uncomplicated appendicitis. JAMA,324(6), 581–593. doi: 10.1001/jama.2020.10888 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7385674/
Bratzler, D. W., Dellinger, E. P., Olsen, K. M., Perl, T. M., Auwaerter, P. G., Bolon, M. K., Fish, D. N., Napolitano, L. M., Sawyer, R. G., Slain, D., Steinberg, J. P., Weinstein, R. A., American Society of Health-System Pharmacists (ASHP), Infectious Diseases Society of America (IDSA), Surgical Infection Society (SIS), & Society for Healthcare Epidemiology of America (SHEA) (2013). Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surgical Infections, 14(1), 73–156. https://doi.org/10.1089/sur.2013.9999
Solomkin, J. S., Mazuski, J. E., Bradley, J. S., Rodvold, K. A., Goldstein, E. J., Baron, E. J., O’Neill, P. J., Chow, A. W., Dellinger, E. P., Eachempati, S. R., Gorbach, S., Hilfiker, M., May, A. K., Nathens, A. B., Sawyer, R. G., Bartlett, J. G. (2010). Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clinical Infectious Diseases, 50(2), 133–164. https://doi.org/10.1086/649554
Hayes, D., Reiter, S., Hagen, E., Lucas, G., Chu, I., Muñiz, T., Martinez, R. (2021). Is interval appendectomy really needed? A closer look at neoplasm rates in adult patients undergoing interval appendectomy after complicated appendicitis. Surgical Endoscopy, 35(7), 3855–3860. https://doi.org/10.1007/s00464-020-07798-9
Dahdaleh, F .S., Heidt, D., Turaga K. K. (2019). The appendix. In Brunicardi, F., Andersen, D. K., Billiar, T. R., Dunn, D. L., Kao, L. S., Hunter, J. G., Matthews, J. B., Pollock, R. E. (Eds.), Schwartz’s Principles of Surgery (11th ed.). McGraw-Hill. https://accessmedicine.mhmedical.com/content.aspx?bookid=2576§ionid=216215350
Carstens, A. K., Fensby, L., Penninga, L. (2018). Nonoperative treatment of appendicitis during pregnancy in a remote area. AJP Reports, 8(1), e37–e38. https://doi.org/10.1055/s-0037-1620279
Create your free account or log in to continue reading!