Hashimoto's thyroiditis, or chronic autoimmune thyroiditis, is the most common cause of hypothyroidism in iodine-sufficient regions, including the US. The condition is an autoimmune disorder leading to destruction of the thyroid cells and thyroid failure. The gradual clinical course of Hashimoto's thyroiditis starts with a transient hyperthyroid state (“hashitoxicosis”) followed by subclinical hypothyroidism. Eventually, progression to overt hypothyroidism occurs, which is permanent. Patients may have a painless goiter, but in later stages, the gland is atrophic. Diagnosis is by laboratory tests showing elevated thyroid-stimulating hormone (TSH), low free thyroxine (T4), and positive antibodies against thyroglobulin and thyroid peroxidase. In uncertain cases, imaging is required. Radioactive iodine uptake will show low iodine uptake and ultrasonography demonstrates either diffuse symmetric enlargement or atrophic reduction (depending on the phase). Biopsy shows lymphocytic infiltration with Hürthle cells. Treatment of the eventual hypothyroid state is lifelong thyroid hormone replacement.
Hashimoto’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditisis an autoimmune thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy disease resulting in the destruction and failure of the thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy gland.
Epidemiology
Age at onset is usually between 30 and 50 years.
More common in women than men: 7–10:1 ratio
Most common cause of hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism in iodine-sufficient regions
2nd-most common cause of hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism worldwide, after iodineIodineA nonmetallic element of the halogen group that is represented by the atomic symbol I, atomic number 53, and atomic weight of 126. 90. It is a nutritionally essential element, especially important in thyroid hormone synthesis. In solution, it has anti-infective properties and is used topically.Thyroid Hormones deficiency
Etiology
Exact cause unknown, although genetic and environmental factors play a role:
Genetic risk factors:
↑ Risk with polymorphisms in immunoregulatory genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure including CTLA4, PTPN22, IL2RA (all encoding T cell regulatory responses)
Associated with HLA-DR3, DR4, and DR5
Disease clusters found in families suggest genetic susceptibility.
↑ IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with Down’s syndrome and Turner’s syndrome
Non-genetic risk factors possibly precipitate the disease:
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
IodineIodineA nonmetallic element of the halogen group that is represented by the atomic symbol I, atomic number 53, and atomic weight of 126. 90. It is a nutritionally essential element, especially important in thyroid hormone synthesis. In solution, it has anti-infective properties and is used topically.Thyroid Hormones and amiodaroneAmiodaroneAn antianginal and class III antiarrhythmic drug. It increases the duration of ventricular and atrial muscle action by inhibiting potassium channels and voltage-gated sodium channels. There is a resulting decrease in heart rate and in vascular resistance.Pulmonary Fibrosis
Stress
Irradiation
SexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender DysphoriasteroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
Associated with other autoimmune diseasesAutoimmune diseasesDisorders that are characterized by the production of antibodies that react with host tissues or immune effector cells that are autoreactive to endogenous peptides.Selective IgA Deficiency:
Type 1Type 1Spinal Muscular AtrophydiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
Systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus
When thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: AnatomyautoimmunityAutoimmunityAutoimmunity is a pathologic immune response toward self-antigens, resulting from a combination of factors: immunologic, genetic, and environmental. The immune system is equipped with self-tolerance, allowing immune cells such as T cells and B cells to recognize self-antigens and to not mount a reaction against them. Defects in this mechanism, along with environmental triggers (such as infections) and genetic susceptibility factors (most notable of which are the HLA genes) can lead to autoimmune diseases. Autoimmunity is induced, progressive depletion of thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy epithelial cells ensues.
ThyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cell destruction mediated by:
T cell–mediated cytotoxicity: CD8+ cytotoxicCytotoxicParvovirus B19T cellsT cellsLymphocytes responsible for cell-mediated immunity. Two types have been identified – cytotoxic (t-lymphocytes, cytotoxic) and helper T-lymphocytes (t-lymphocytes, helper-inducer). They are formed when lymphocytes circulate through the thymus gland and differentiate to thymocytes. When exposed to an antigen, they divide rapidly and produce large numbers of new T cells sensitized to that antigen.T cells: Types and Functions destroy thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cells.
Local production of cytokinesCytokinesNon-antibody proteins secreted by inflammatory leukocytes and some non-leukocytic cells, that act as intercellular mediators. They differ from classical hormones in that they are produced by a number of tissue or cell types rather than by specialized glands. They generally act locally in a paracrine or autocrine rather than endocrine manner.Adaptive Immune Response:
TumorTumorInflammationnecrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage factor and interferon-ɣ impair cell function.
RecruitmentRecruitmentSkeletal Muscle Contraction of macrophagesMacrophagesThe relatively long-lived phagocytic cell of mammalian tissues that are derived from blood monocytes. Main types are peritoneal macrophages; alveolar macrophages; histiocytes; kupffer cells of the liver; and osteoclasts. They may further differentiate within chronic inflammatory lesions to epithelioid cells or may fuse to form foreign body giant cells or langhans giant cells.Innate Immunity: Phagocytes and Antigen Presentation
AntibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions to thyroglobulinThyroglobulinThyroid Hormones (TgTgThyroid Hormones) and thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy peroxidase (TPO): secondary role in thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomycell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death but are markers of thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: AnatomyautoimmunityAutoimmunityAutoimmunity is a pathologic immune response toward self-antigens, resulting from a combination of factors: immunologic, genetic, and environmental. The immune system is equipped with self-tolerance, allowing immune cells such as T cells and B cells to recognize self-antigens and to not mount a reaction against them. Defects in this mechanism, along with environmental triggers (such as infections) and genetic susceptibility factors (most notable of which are the HLA genes) can lead to autoimmune diseases. Autoimmunity
Lymphocytic infiltration and fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans of thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cells → follicles are disrupted and release thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: AnatomyhormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types:
Transient ↑ of thyroxineThyroxineThe major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood.Thyroid Hormones (T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones) and triiodothyronineTriiodothyronineA T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones (T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones): “hashitoxicosis”
Compensatory ↓ thyroid-stimulating hormoneThyroid-stimulating hormoneA glycoprotein hormone secreted by the adenohypophysis. Thyrotropin stimulates thyroid gland by increasing the iodide transport, synthesis and release of thyroid hormones (thyroxine and triiodothyronine).Thyroid Hormones (TSH) follows → T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones/T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones stores gradually decline
End result: ↑ TSH + hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism (often permanent)
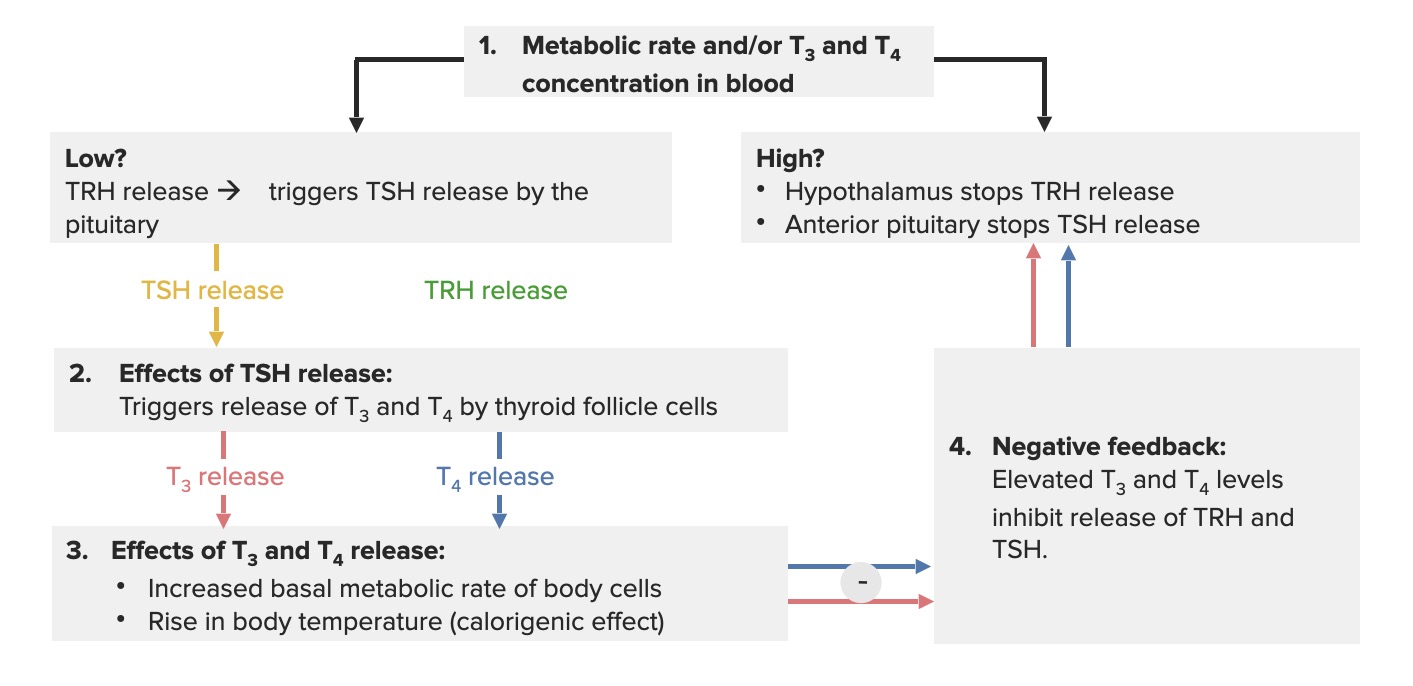
Hypothalamic-pituitary-thyroid axis feedback loop: When the thyroid hormones are low, the hypothalamus releases thyrotropin-releasing hormone (TRH), which triggers the pituitary gland to secrete TSH. The effect of this process is that the thyroid gland produces thyroxine (T4) and triiodothyronine (T3) (more T4 is produced, as it gets converted to T3). An increase in thyroid hormones (free or unbound T3/T4) creates a negative feedback, inhibiting the release of TRH and TSH.
Image: “Classic Negative Feedback Loop” by OpenStax College. License: CC BY 3.0, edited by Lecturio.
Pathology
Immunologic response seen histologically as:
Infiltrates of lymphocytesLymphocytesLymphocytes are heterogeneous WBCs involved in immune response. Lymphocytes develop from the bone marrow, starting from hematopoietic stem cells (HSCs) and progressing to common lymphoid progenitors (CLPs). B and T lymphocytes and natural killer (NK) cells arise from the lineage.Lymphocytes: Histology and plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products cells
Well-developed germinal centers
ThyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cell destruction:
Oncocytic cells with abundant eosinophilic granular cytoplasm
Metaplastic change resulting from chronic injury
Increased connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology/fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans (limited within the capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides)
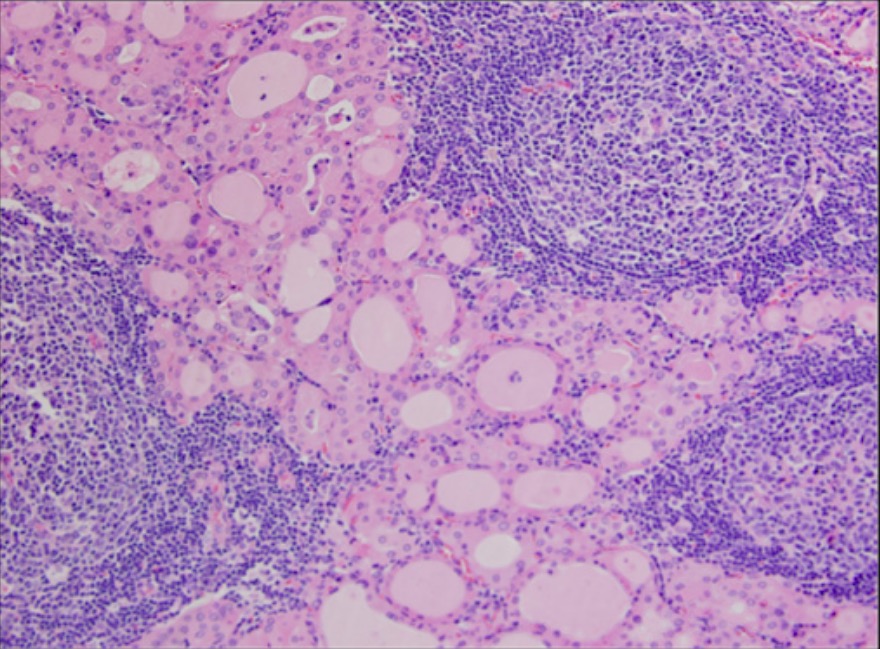
Florid Hashimoto’s thyroiditis: reactive lymphoid tissue with germinal center (hematoxylin and eosin stain, 200x magnification)
Image: “Florid Hashimoto’s thyroiditis” by Division of Endocrinology and Metabolism, University of Connecticut Health Center, 263 Farmington Avenue, Farmington, CT 06030, USA. License: CC BY 2.0
Clinical Presentation
Clinical course
ThyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis typically presents with a triphasic clinical course.
Hashimoto’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis presents similarly, without the final euthyroidEuthyroidThyroiditis phase.
Phases:
Hashitoxicosis: initial transient hyperthyroidismHyperthyroidismHypersecretion of thyroid hormones from the thyroid gland. Elevated levels of thyroid hormones increase basal metabolic rate.Thyrotoxicosis and Hyperthyroidism
Gradual loss of thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy function
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism common symptoms:
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, cold intolerance, weight gain
Dry skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions, hair loss
Difficulty concentrating and poor memoryMemoryComplex mental function having four distinct phases: (1) memorizing or learning, (2) retention, (3) recall, and (4) recognition. Clinically, it is usually subdivided into immediate, recent, and remote memory.Psychiatric Assessment
Hoarse voice
Impaired hearing
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
ParesthesiasParesthesiasSubjective cutaneous sensations (e.g., cold, warmth, tingling, pressure, etc.) that are experienced spontaneously in the absence of stimulation.Posterior Cord Syndrome
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism common signs:
+/- GoiterGoiterA goiter is a chronic enlargement of the thyroid gland due to nonneoplastic growth occurring in the setting of hypothyroidism, hyperthyroidism, or euthyroidism. Morphologically, thyroid enlargement can be diffuse (smooth consistency) or nodular (uninodular or multinodular). Goiter (some glands are atrophic in later stages)
Dry, coarse skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions; alopeciaAlopeciaAlopecia is the loss of hair in areas anywhere on the body where hair normally grows. Alopecia may be defined as scarring or non-scarring, localized or diffuse, congenital or acquired, reversible or permanent, or confined to the scalp or universal; however, alopecia is usually classified using the 1st 3 factors.Alopecia; cool extremities
Puffy face, hands, and feet (nonpitting edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema/myxedemaMyxedemaA condition characterized by a dry, waxy type of swelling (edema) with abnormal deposits of mucopolysaccharides in the skin and other tissues. It is caused by a deficiency of thyroid hormones. The skin becomes puffy around the eyes and on the cheeks. The face is dull and expressionless with thickened nose and lips.Edema)
BradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias
Delayed relaxation of tendon reflexes
Carpal tunnelCarpal TunnelThe carpal tunnel is formed by the transverse carpal ligament (flexor retinaculum) superiorly and the carpal bones inferiorly.Carpal Tunnel Syndrome syndrome
ThyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy hormone levels will differ in each phase:
Hashitoxicosis: ↓ TSH + ↑ free T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones/T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones
Subclinical hypothyroidismSubclinical HypothyroidismHypothyroidism: ↑ TSH + normal free T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones/T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones
Overt hypothyroidismOvert HypothyroidismHypothyroidism: ↑ TSH + ↓ free T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones/T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones
Positive anti-thyroid peroxidase (TPO) and anti-thyroglobulin antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions (TgTgThyroid Hormones):
Noted in > 95% of cases of Hashimoto’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis
AntibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions may predict the progression to overt hypothyroidismOvert HypothyroidismHypothyroidism.
Obtained in cases of asymmetric goiterGoiterA goiter is a chronic enlargement of the thyroid gland due to nonneoplastic growth occurring in the setting of hypothyroidism, hyperthyroidism, or euthyroidism. Morphologically, thyroid enlargement can be diffuse (smooth consistency) or nodular (uninodular or multinodular). Goiter and/or + suspicion of nodules
Shows Hürthle cells and lymphocytic infiltration with germinal centers
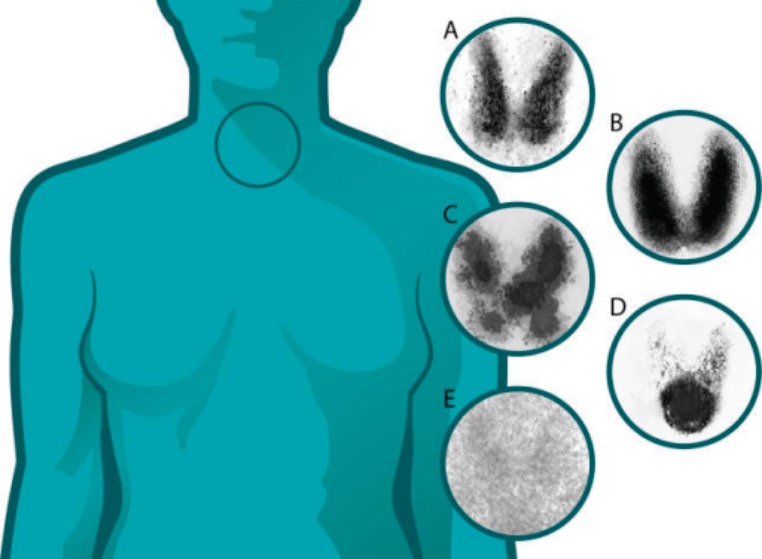
Thyroid uptake scans (thyroiditis versus other thyroid diseases): A: normal B: Graves’ disease: diffuse increased uptake in both thyroid lobes C: toxic multinodular goiter: “hot” and “cold” areas of uneven uptake D: toxic adenoma: increased uptake in a single nodule with suppression of the surrounding thyroid E: thyroiditis: decreased or absent uptake
Image: “Technetium 99” by Endocrine Unit, Freeman Hospital, Newcastle upon Tyne, United Kingdom. License: CC BY 4.0
Management and Complications
Thyroid-replacement therapy
LevothyroxineLevothyroxineThyroid Replacement Therapy: synthetic form of T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones that is peripherally converted to T3T3A T3 thyroid hormone normally synthesized and secreted by the thyroid gland in much smaller quantities than thyroxine (T4). Most T3 is derived from peripheral monodeiodination of T4 at the 5′ position of the outer ring of the iodothyronine nucleus. The hormone finally delivered and used by the tissues is mainly t3.Thyroid Hormones
1.6 µg/kg body weight per day in young and healthy patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Starting dose of 25 µg per day in the elderly
Different dose for pediatric population
Duration: lifetime
AbsorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption reduced by antacids, ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements, calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes
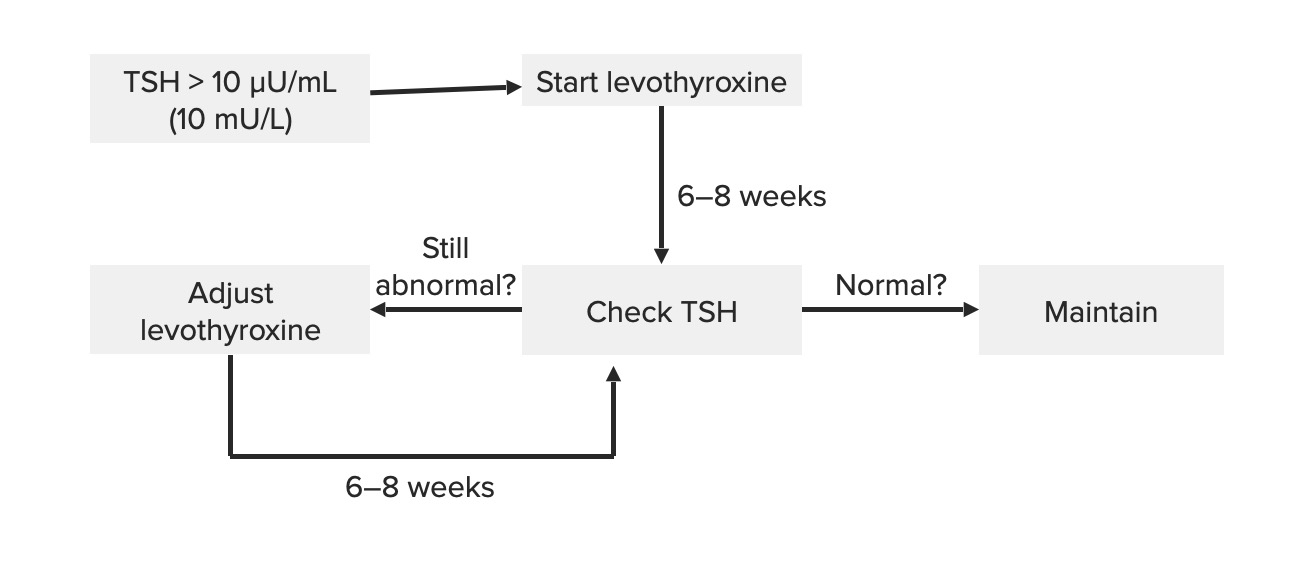
Measure TSH after 6 weeks, and adjust the dose.
Schematic diagram of the management of Hashimoto’s thyroiditis: Note that the adjustments depend on TSH levels.
Image by Lecturio.
Complications
Myxedema comaMyxedema ComaHypothyroidism: severehypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism characterized by slowing function of multiple organs
Considered a medical emergency
Can lead to shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock and death (mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate up to 50%)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with Hashimoto’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis have increased risk of:
Other autoimmune disease (e.g., type 1Type 1Spinal Muscular AtrophydiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus, autoimmune adrenalitis)
B cell lymphomaLymphomaA general term for various neoplastic diseases of the lymphoid tissue.Imaging of the Mediastinum of the thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy gland
Differential Diagnosis
Granulomatous thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis (de Quervain’s syndrome): thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: AnatomyinflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation usually associated with a previous viral infection and the most common cause of thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: AnatomypainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways. Presentation includes neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess tenderness with goiterGoiterA goiter is a chronic enlargement of the thyroid gland due to nonneoplastic growth occurring in the setting of hypothyroidism, hyperthyroidism, or euthyroidism. Morphologically, thyroid enlargement can be diffuse (smooth consistency) or nodular (uninodular or multinodular). Goiter. Work-up shows low TSH, elevated free T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones, increased sedimentation rate, and a low or absent radioactive iodine uptakeRadioactive Iodine UptakeThyrotoxicosis and Hyperthyroidism. Often a self-limited course that can go through a hyperthyroid state and then a euthyroidEuthyroidThyroiditis state followed by hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism. Recovery to normal thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy function takes months.
Subacute lymphocytic thyroiditisSubacute lymphocytic thyroiditisThyroiditis (painless thyroiditisPainless ThyroiditisThyroiditis): an autoimmune disease with diffuse enlargement of the thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy gland. The same process occurs in postpartum thyroiditisPostpartum thyroiditisTransient autoimmune thyroiditis occurring in the postpartum period. It is characterized by the presence of high titers of autoantibodies against thyroid peroxidase and thyroglobulin. Clinical signs include the triphasic thyroid hormone pattern: beginning with thyrotoxicosis, followed with hypothyroidism, then return to euthyroid state by 1 year postpartum.Postpartum Complications. Laboratory tests depend on the phase of the disease but the initial hyperthyroidismHyperthyroidismHypersecretion of thyroid hormones from the thyroid gland. Elevated levels of thyroid hormones increase basal metabolic rate.Thyrotoxicosis and Hyperthyroidism shows low TSH and elevated T4T4The major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine which exerts a broad spectrum of stimulatory effects on cell metabolism.Thyroid Hormones. The condition is associated with a low radioactive iodine uptakeRadioactive Iodine UptakeThyrotoxicosis and Hyperthyroidism. The disease pattern is a transient hyperthyroid state and then hypothyroid followed by recovery. Some cases do not become euthyroidEuthyroidThyroiditis, however.
Riedel’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis: rare form of thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis characterized by extensive fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans of the thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy gland and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess area. Riedel’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis differs from Hashimoto’s thyroiditisThyroiditisThyroiditis is a catchall term used to describe a variety of conditions that have inflammation of the thyroid gland in common. It includes pathologies that cause an acute illness with severe thyroid pain (e.g., subacute thyroiditis and infectious thyroiditis) as well as conditions in which there is no clinically evident inflammation and the manifestations primarily reflect thyroid dysfunction or a goiter (e.g., painless thyroiditis and fibrous Riedel’s thyroiditis). Thyroiditis, in which fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans does not extend beyond the capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides. Examination will show a hard, fixed thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy gland, which is associated with other sites of fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans in the body.
HypopituitarismHypopituitarismHypopituitarism is a condition characterized by pituitary hormone deficiency. This condition primarily results from a disease of the pituitary gland, but it may arise from hypothalamic dysfunction. Pituitary tumors are one of the most common causes. The majority of cases affect the anterior pituitary lobe (adenohypophysis), which accounts for 80% of the gland. Hypopituitarism: a disorder characterized by a deficiency in the pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types hormone production, which results from disease of the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus or the pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland itself. Hypofunction results in reduced secretionSecretionCoagulation Studies of growth hormone, TSH, gonadotropins, prolactinProlactinA lactogenic hormone secreted by the adenohypophysis. It is a polypeptide of approximately 23 kd. Besides its major action on lactation, in some species prolactin exerts effects on reproduction, maternal behavior, fat metabolism, immunomodulation and osmoregulation.Breasts: Anatomy, and adrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones, which produces a complex syndrome depending on the hormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types affected.