Endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation (EH) is the abnormal growth of the uterine endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development. This abnormal growth may be due to estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy stimulation or genetic mutationsGenetic MutationsCarcinogenesis leading to uncontrolled proliferation. Endometrial carcinoma (EC) is the most common gynecologic malignancyMalignancyHemothorax in the developed world, and it has several histologic types. Endometrioid carcinoma (known as type 1Type 1Spinal Muscular Atrophy EC) typically develops from atypical endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation, is hormonally responsive, and carries a favorable prognosisPrognosisA prediction of the probable outcome of a disease based on a individual's condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas. Other histologic types are known as type 2Type 2Spinal Muscular Atrophy EC; they tend to present at more advanced stages, are not hormonally responsive, and carry a far worse prognosisPrognosisA prediction of the probable outcome of a disease based on a individual's condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas. Women with both EH and EC tend to present with postmenopausal or irregular menstrual bleeding. Diagnosis is histologic. Management most often involves progestin therapy, surgery, and adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund's adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.VaccinationradiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy (for advanced disease).
Endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation (EH) is a state of excessive proliferation of endometrial cells, resulting in an increased gland-to-stroma ratio.
Endometrial carcinoma (EC) refers to excessive proliferation of endometrial cells that are capable of invading surrounding tissues and metastasizing to distant sites.
Epidemiology
Endometrial cancer is the most common gynecologic cancer in the developed world (cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer is most common in developing countries).
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
EH: 133 per 100,000 woman-years
EC: 25 per 100,000 woman-years
Lifetime risk of EC in U.S. women: approximately 2%
Both are most common in perimenopausal or early postmenopausal individuals.
Histologic classification of endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation
There are 2 primary classification systems for endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation:
2014 World Health Organization (WHO)
Endometrial intraepithelial neoplasia (EIN) classification system
Table: Classification of endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation
WHO system terminology
EIN system terminology
Characteristics
Normal endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Normal endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Proliferative phaseProliferative phaseMenstrual Cycle (prior to ovulationOvulationThe discharge of an ovum from a rupturing follicle in the ovary.Menstrual Cycle with estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy alone): no crowding of the glands within the stroma (gland-to-stroma ratio < 2:1)
Secretory phaseSecretory phaseMenstrual Cycle (after ovulationOvulationThe discharge of an ovum from a rupturing follicle in the ovary.Menstrual Cycle with estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy + progesteroneProgesteroneThe major progestational steroid that is secreted primarily by the corpus luteum and the placenta. Progesterone acts on the uterus, the mammary glands and the brain. It is required in embryo implantation; pregnancy maintenance, and the development of mammary tissue for milk production. Progesterone, converted from pregnenolone, also serves as an intermediate in the biosynthesis of gonadal steroid hormones and adrenal corticosteroids.Gonadal Hormones):
EndometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development may display some crowding
Glands remain well organized
No mitotic activity
HyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation without atypiaAtypiaFibrocystic Change
BenignBenignFibroadenoma endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation
Changes seen with prolonged estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy exposure
Diffuse changes throughout the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Abnormal chromatinChromatinThe material of chromosomes. It is a complex of dna; histones; and nonhistone proteins found within the nucleus of a cell.DNA Types and Structure
Prominent nucleoli
Mitotic activity is present.
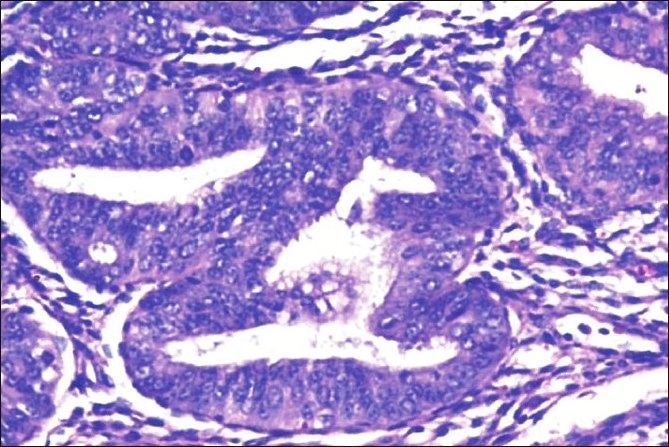
Histopathology of endometrial intraepithelial neoplasia/atypical hyperplasia: The image shows closely packed endometrial glands with sparse intervening stroma and stratification of the lining epithelium Epithelial cells show cytologic atypia with high nucleocytoplasmic ratio, irregular clumping of nuclear chromatin, and mitotic figures (hematoxylin and eosin stain, ×200)
Image: “Histopathology of complex hyperplasia with atypia” by Shalinee Rao, Sandhya Sundaram, Raghavan Narasimhan. License: CC BY 2.0
Not estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy dependent
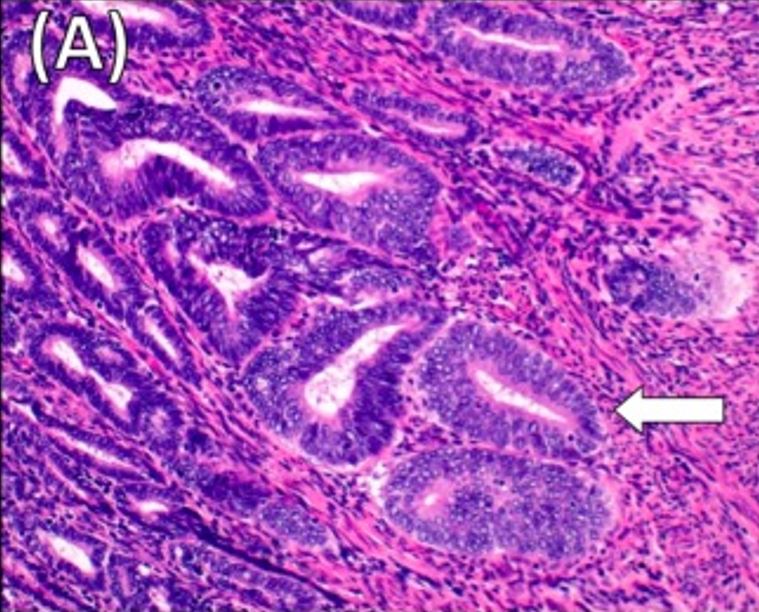
Histology of moderately differentiated grade 2 endometrioid adenocarcinoma: Note the superficial myometrial invasion of the tumor (arrow). H&E stain x20
Image: “Histology of the primary endometrial cancer and the ileum recurrence” by Frontiers in Oncology. License: CC BY 4.0, cropped by Lecturio.
GradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis endometrial carcinoma
The grade describes the amount of solid glandular growth. Endometrial cancer is classified into 1 of 3 grades.
Table: Endometrial cancer gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis
Grade
Definition
Histology
I
Well differentiated
≤ 5% of the tissue exhibits a solid growth pattern
II
Moderately differentiated
6%–50% of the tissue exhibits a solid growth pattern
III
Poorly differentiated
> 50% of the tissue exhibits a solid growth pattern
StagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis endometrial carcinoma
The stage describes the extent of tumorTumorInflammation spread. StagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis takes into account the size of the tumorTumorInflammation, extent of local invasion, lymphLymphThe interstitial fluid that is in the lymphatic system.Secondary Lymphatic Organs node involvement, and metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis. There are 4 major stages in EC. Disease is staged based on the “highest” findings. For example, a tumorTumorInflammation confined to the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy but with positive lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy is classified as stage III. Similarly, direct tumorTumorInflammation invasion into the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess mucosa is stage IV regardless of lymphLymphThe interstitial fluid that is in the lymphatic system.Secondary Lymphatic Organs node involvement.
Table: Endometrial cancer stagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis
TumorTumorInflammation invades into cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy stroma, but does not extend beyond the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy.
None
III
TumorTumorInflammation invades into adnexa, vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, or parametrium.
Direct tumorTumorInflammation invasion into the mucosa of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess or rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
MetastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis to distant structures
BenignBenignFibroadenoma endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation: chronic estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy exposure that is unopposed by progesteroneProgesteroneThe major progestational steroid that is secreted primarily by the corpus luteum and the placenta. Progesterone acts on the uterus, the mammary glands and the brain. It is required in embryo implantation; pregnancy maintenance, and the development of mammary tissue for milk production. Progesterone, converted from pregnenolone, also serves as an intermediate in the biosynthesis of gonadal steroid hormones and adrenal corticosteroids.Gonadal Hormones.
In many cases, prolonged unopposed estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy exposure also contributes.
Risk factors
Most of the risk factors for both EH and EC include anything that increases unopposed estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy exposure.
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity: Adipose tissueAdipose tissueAdipose tissue is a specialized type of connective tissue that has both structural and highly complex metabolic functions, including energy storage, glucose homeostasis, and a multitude of endocrine capabilities. There are three types of adipose tissue, white adipose tissue, brown adipose tissue, and beige or “brite” adipose tissue, which is a transitional form.Adipose Tissue: Histology converts androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens to estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy.
Polycystic ovary syndrome (PCOSPCOSPolycystic ovarian syndrome (PCOS) is the most common endocrine disorder of reproductive-age women, affecting nearly 5%-10% of women in the age group. It is characterized by hyperandrogenism, chronic anovulation leading to oligomenorrhea (or amenorrhea), and metabolic dysfunction.Polycystic Ovarian Syndrome): a condition of chronic anovulationAnovulationSuspension or cessation of ovulation in animals or humans with follicle-containing ovaries (ovarian follicle). Depending on the etiology, ovulation may be induced with appropriate therapy.Polycystic Ovarian Syndrome → ↓ opposing progesteroneProgesteroneThe major progestational steroid that is secreted primarily by the corpus luteum and the placenta. Progesterone acts on the uterus, the mammary glands and the brain. It is required in embryo implantation; pregnancy maintenance, and the development of mammary tissue for milk production. Progesterone, converted from pregnenolone, also serves as an intermediate in the biosynthesis of gonadal steroid hormones and adrenal corticosteroids.Gonadal Hormones
Nulliparity
Early menarcheMenarcheThe first menstrual cycle marked by the initiation of menstruation.Menstrual Cycle/late menopauseMenopauseMenopause is a physiologic process in women characterized by the permanent cessation of menstruation that occurs after the loss of ovarian activity. Menopause can only be diagnosed retrospectively, after 12 months without menstrual bleeding. Menopause: more menstrual cycles = ↑ estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy exposure
Postmenopausal hormone replacement therapyHormone Replacement TherapyHormone replacement therapy (HRT) is used to treat symptoms associated with female menopause and in combination to suppress ovulation. Risks and side effects include uterine bleeding, predisposition to cancer, breast tenderness, hyperpigmentation, migraine headaches, hypertension, bloating, and mood changes.Noncontraceptive Estrogen and Progestins (HRTHRTHormone replacement therapy (HRT) is used to treat symptoms associated with female menopause and in combination to suppress ovulation. Risks and side effects include uterine bleeding, predisposition to cancer, breast tenderness, hyperpigmentation, migraine headaches, hypertension, bloating, and mood changes.Noncontraceptive Estrogen and Progestins) without adequate progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives
TamoxifenTamoxifenOne of the selective estrogen receptor modulators with tissue-specific activities. Tamoxifen acts as an anti-estrogen (inhibiting agent) in the mammary tissue, but as an estrogen (stimulating agent) in cholesterol metabolism, bone density, and cell proliferation in the endometrium.Antiestrogens: estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy antagonist in breast, but has estrogenic activity in endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Estrogen-secreting ovarian tumors (e.g., granulosa cellGranulosa cellSupporting cells for the developing female gamete in the ovary. They are derived from the coelomic epithelial cells of the gonadal ridge. Granulosa cells form a single layer around the oocyte in the primordial ovarian follicle and advance to form a multilayered cumulus oophorus surrounding the ovum in the graafian follicle. The major functions of granulosa cells include the production of steroids and LH receptors.Puberty tumors)
Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome:
Also known as hereditary nonpolyposis colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy cancer (HNPCCHNPCCLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome)
Carries up to a 60% lifetime risk of EC
Protective factors
The following factors decrease the risk of EH/EC:
Use of combination oral contraceptives
Cigarette smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Pathogenesis of benignBenignFibroadenoma endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation
EstrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy naturally stimulates proliferation of endometrial tissueEndometrial tissueThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Endometriosis
ProgesteroneProgesteroneThe major progestational steroid that is secreted primarily by the corpus luteum and the placenta. Progesterone acts on the uterus, the mammary glands and the brain. It is required in embryo implantation; pregnancy maintenance, and the development of mammary tissue for milk production. Progesterone, converted from pregnenolone, also serves as an intermediate in the biosynthesis of gonadal steroid hormones and adrenal corticosteroids.Gonadal Hormones (produced by the corpus luteumCorpus LuteumThe yellow body derived from the ruptured ovarian follicle after ovulation. The process of corpus luteum formation, luteinization, is regulated by luteinizing hormone.Ovaries: Anatomy only after ovulationOvulationThe discharge of an ovum from a rupturing follicle in the ovary.Menstrual Cycle) counteracts estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy/has a protective effect on the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Excess estrogenic stimulation → diffuse hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation throughout the cavity
Altering the hormonal milieu (e.g., treating with progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives and/or removing estrogenic stimulation) can lead to resolution of hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation.
Pathogenesis of endometrial intraepithelial neoplasia and endometrial carcinoma
Uncontrolled proliferation starting from a single location
Absence of programmed cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death
POLE geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics: involved in DNA replicationDNA replicationThe entire DNA of a cell is replicated during the S (synthesis) phase of the cell cycle. The principle of replication is based on complementary nucleotide base pairing: adenine forms hydrogen bonds with thymine (or uracil in RNA) and guanine forms hydrogen bonds with cytosine. DNA Replication and repair
Lynch syndromeLynch syndromeLynch syndrome, also called hereditary non-polyposis colorectal cancer (HNPCC), is the most common inherited colon cancer syndrome, and carries a significantly increased risk for endometrial cancer and other malignancies. Lynch syndrome has an autosomal dominant inheritance pattern involving pathogenic variants in one of the mismatch repair (MMR) genes or epithelial cell adhesion molecule (EpCAM). Lynch syndrome mutations (DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structuremismatch repairMismatch repairA DNA repair pathway involved in correction of errors introduced during DNA replication when an incorrect base, which cannot form hydrogen bonds with the corresponding base in the parent strand, is incorporated into the daughter strand. Exonucleases recognize the base pair mismatch and cause a segment of polynucleotide chain to be excised from the daughter strand, thereby removing the mismatched base.Lynch syndromegenesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure)
Distant metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis via lymphatic and hematologic spread
Clinical Presentation
About ¾ of women diagnosed with EC are postmenopausal. The classic presentation is a 60-something-year-old obese woman with postmenopausal bleeding.
Abnormal uterine bleedingAbnormal Uterine BleedingAbnormal uterine bleeding is the medical term for abnormalities in the frequency, volume, duration, and regularity of the menstrual cycle. Abnormal uterine bleeding is classified using the acronym PALM-COEIN, with PALM representing the structural causes and COEIN indicating the non-structural causes. Abnormal Uterine Bleeding (most common presenting symptom):
Postmenopausal bleeding
Abnormal menstrual cycles in premenopausal individuals
Vaginal discharge (clear or white) in postmenopausal women
Abdominal or pelvic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways/pressure
DyspareuniaDyspareuniaRecurrent genital pain occurring during, before, or after sexual intercourse in either the male or the female.Primary Ovarian Insufficiency (painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways during intercourse)
Thickened endometrial lining on pelvic imaging done for other indications in a postmenopausal woman
Identified on specimen from a hysterectomy done for other indications (e.g., fibroidsFibroidsA benign tumor derived from smooth muscle tissue, also known as a fibroid tumor. They rarely occur outside of the uterus and the gastrointestinal tract but can occur in the skin and subcutaneous tissue, probably arising from the smooth muscle of small blood vessels in these tissues.Infertility)
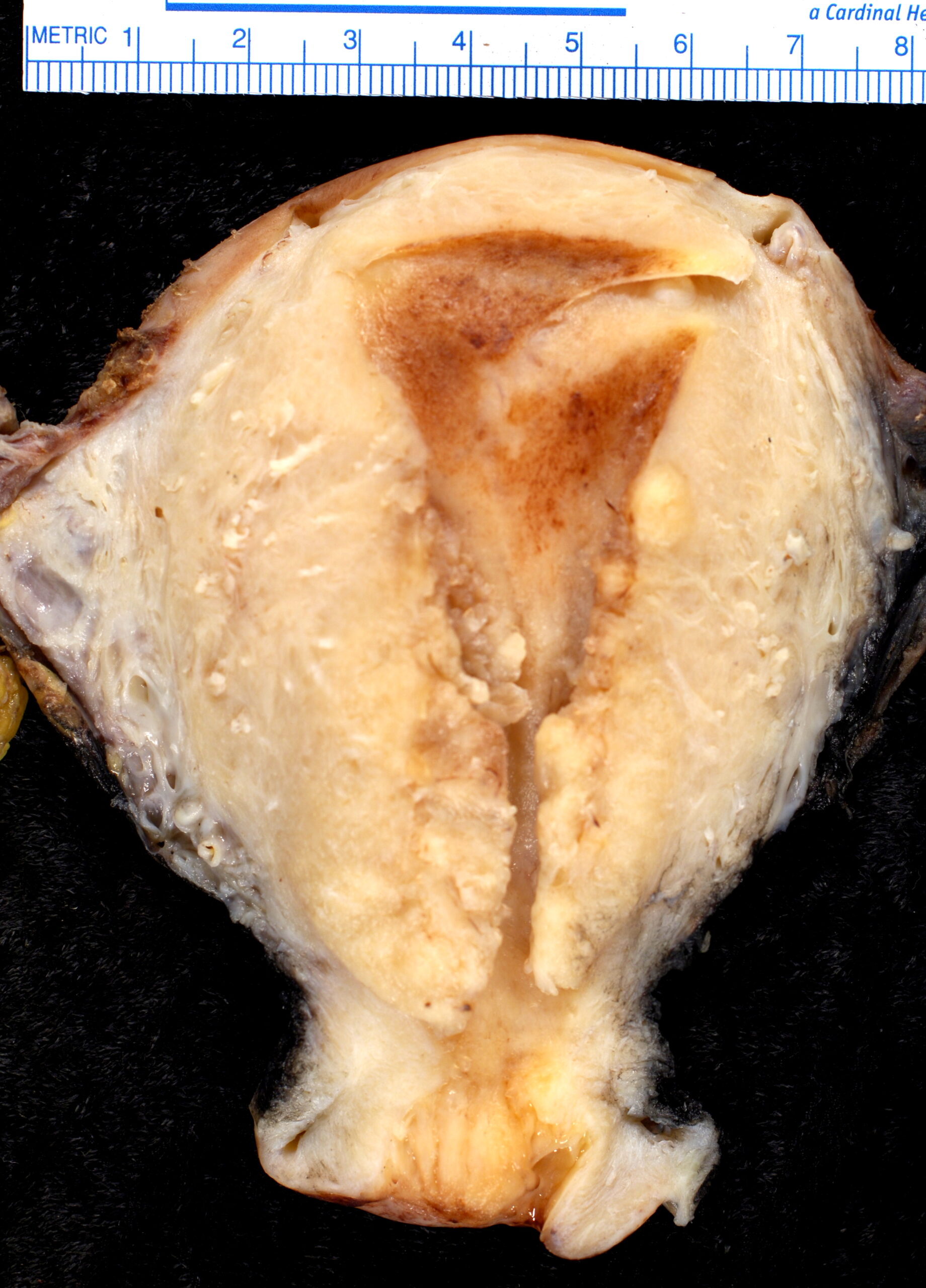
Endometrioid adenocarcinoma, gross specimen: Note the tumor primarily in the lower half of the specimen and invading into the surrounding myometrium.
Image: “Endometrioid adenocarcinoma of the uterus FIGO grade III” by Ed Uthman. License: CC BY 2.0
Diagnosis
BiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma is required for definitive diagnosis of EH and EC. The pelvic exam is usually normal. All women who present with abnormal bleeding (especially postmenopausal bleeding) should be assessed with pelvic ultrasonography and/or biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
BiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma
Gold standard for diagnosing both EH and EC
Methods:
In-office biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma with an endometrial pipelle (most reliable when ≥ 50% of the cavity is affected → may miss focal lesions)
Surgical biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma with dilation and curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors (D&C)
Histologic findings:
Back-to-back glands with no intervening stroma
Glands have smooth, luminal contour
May see cribriform patterns (gland within a gland)
Imaging
Methods:
Transvaginal pelvic ultrasound: imaging method of choice
Saline is injected into the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy while real-time sonographySonographyThe visualization of deep structures of the body by recording the reflections or echoes of ultrasonic pulses directed into the tissues. Use of ultrasound for imaging or diagnostic purposes employs frequencies ranging from 1. 6 to 10 megahertz.Diagnostic Procedures in Gynecology is performed.
Distends the cavity to allow assessment of intrauterine pathology
Can differentiate diffusely thickened endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development (a concern for EH/EC) from endometrial polyp
Pelvic MRI: may be indicated if ultrasound is unclear or to assess extent of disease.
Chest radiography: to look for metastasisMetastasisThe transfer of a neoplasm from one organ or part of the body to another remote from the primary site.Grading, Staging, and Metastasis
Findings worrisome for EH/EC:
Endometrial thickness ≥ 5 mmMMMultiple myeloma (MM) is a malignant condition of plasma cells (activated B lymphocytes) primarily seen in the elderly. Monoclonal proliferation of plasma cells results in cytokine-driven osteoclastic activity and excessive secretion of IgG antibodies.Multiple Myeloma in a postmenopausal woman
Heterogeneity of the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
Loss of a distinct border between the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development and myometrium
CysticCysticFibrocystic Change lesions in the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development
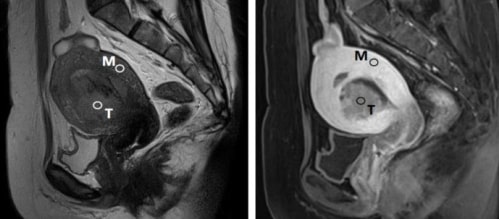
Endometrial cancer seen on sagittal view Left: T2-weighted MRI Right: contrast-enhanced T1-weighted MRI T: tumor M: myometrium
Image: “Use of Myometrium as an Internal Reference for Endometrial and Cervical Cancer on Multiphase Contrast-Enhanced MRI” by Lin CN, Liao YS, Chen WC, Wang YS, Lee LW. License: CC BY 4.0, cropped by Lecturio.
Other assessments
Pelvic exam:
Typically normal
Findings in more advanced disease:
Diffusely enlarged uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy
Fixed (nonmobile) pelvic structures
Pap smearPap smearCytological preparation of cells collected from a mucosal surface and stained with Papanicolaou stain.Cervical Cancer Screening (should be up to date)
CA-125CA-125A carbohydrate antigen that occurs in tumors of the ovary as well as in breast, kidney, and gastrointestinal tract tumors and normal tissue. While it is tumor-associated, it is not tumor-specific and may have a protective function against particles and infectious agents at mucosal surfaces.Serum Tumor Markers:
Management for benignBenignFibroadenoma endometrial hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation (hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation without atypiaAtypiaFibrocystic Change)
Observation (instead of progestin therapy) may be considered in premenopausal women with:
Normal weight
Known inciting factor removed (e.g., anovulatory woman has now become ovulatory)
Medical management:
Candidates:
Premenopausal women (1st-line)
Can be considered in postmenopausal women
Because benignBenignFibroadenoma EH is an estrogen-driven process, treatment is typically with progestin therapy(which naturally opposes the effects of estrogens).
Progestin therapy options include:
LevonorgestrelLevonorgestrelA synthetic progestational hormone with actions similar to those of progesterone and about twice as potent as its racemic or (+-)-isomer (norgestrel). It is used for contraception, control of menstrual disorders, and treatment of endometriosis.Hormonal Contraceptives intrauterine device (IUD) (1st-line)
Oral progestin therapy: megestrol acetateMegestrol acetateMegestrol acetate is a progestogen with actions and uses similar to those of the progestogens in general. It also has anti-androgenic properties. It is given by mouth in the palliative treatment or as an adjunct to other therapy in endometrial carcinoma and in breast cancer.Noncontraceptive Estrogen and Progestins, medroxyprogesterone
Combined oral contraceptives pills (for women who also desire contraception)
Hysterectomy: preferred treatment in all individuals
Progestin therapy can be an alternative in women who:
Desire future fertility
Are at high risk for surgical complicationsSurgical complicationsSurgical complications are conditions, disorders, or adverse events that occur following surgical procedures. The most common general surgical complications include bleeding, infections, injury to the surrounding organs, venous thromboembolic events, and complications from anesthesia.Surgical Complications
Management for endometrial carcinoma
Management is primarily surgical, with potential for adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.VaccinationradiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy. Management of advanced disease is highly individualized.
Surgical management:
Indicated in women who are able to undergo an operation
Procedure:
Hysterectomy with a bilateral salpingo-oophorectomy
Possible lymphadenectomy of the pelvic and para-aortic nodes (higher stage/grade)
Surgery is often curative in low-risk disease (defined as type 1Type 1Spinal Muscular Atrophy EC confined to the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development).
Individuals with locally advanced or metastatic cancer may have cytoreductive or palliative surgery.
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy:
Often prescribed for individuals with intermediate- or high-risk disease
Pelvic radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy (↑ toxicityToxicityDosage Calculation, including long-term bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and bowel complications)
PaclitaxelPaclitaxelA cyclodecane isolated from the bark of the pacific yew tree, taxus brevifolia. It stabilizes microtubules in their polymerized form leading to cell death.Microtubule and Topoisomerase Inhibitors
Hormone therapy (progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives): may be considered in some cases
Can consider following CA-125CA-125A carbohydrate antigen that occurs in tumors of the ovary as well as in breast, kidney, and gastrointestinal tract tumors and normal tissue. While it is tumor-associated, it is not tumor-specific and may have a protective function against particles and infectious agents at mucosal surfaces.Serum Tumor Markers levels
Imaging for any suspicion of recurrence:
PETPETAn imaging technique that combines a positron-emission tomography (PET) scanner and a ct X ray scanner. This establishes a precise anatomic localization in the same session.Nuclear Imaging/CT (preferred)
MRI
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
EIN (hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation with atypiaAtypiaFibrocystic Change): 15%–40% will progress to EC within 20 years
EC prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas by type:
Carries a good prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
Surgery is often curative
Type 2Type 2Spinal Muscular Atrophy disease acts more like ovarian cancerOvarian cancerOvarian cancer is a malignant tumor arising from the ovarian tissue and is classified according to the type of tissue from which it originates. The 3 major types of ovarian cancer are epithelial ovarian carcinomas (EOCs), ovarian germ cell tumors (OGCTs), and sex cord-stromal tumors (SCSTs). Ovarian Cancer:
Generally presents at a higher stage
Worse prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
Higher rates of recurrence
5-year survival rates based on EC stage:
Stage I: approximately 80%–90%
Stage II: approximately 80%
Stage III: approximately 50%–65%
Stage IV: approximately 20%
Differential Diagnosis
AdenomyosisAdenomyosisAdenomyosis is a benign uterine condition characterized by the presence of ectopic endometrial glands and stroma within the myometrium. Adenomyosis is a common condition, affecting 20%-35% of women, and typically presents with heavy menstrual bleeding and dysmenorrhea. Adenomyosis: very common benignBenignFibroadenoma uterine condition characterized by the presence of ectopic endometrial glands and stroma within the myometrium. AdenomyosisAdenomyosisAdenomyosis is a benign uterine condition characterized by the presence of ectopic endometrial glands and stroma within the myometrium. Adenomyosis is a common condition, affecting 20%-35% of women, and typically presents with heavy menstrual bleeding and dysmenorrhea. Adenomyosis typically presents with heavy menstrual bleedingHeavy menstrual bleedingExcessive menstrual blood loss (objectively defined as > 80 mL blood loss/cycle). Can be based on heavy flow, as determined by the patientAbnormal Uterine Bleeding and dysmenorrhea. Diagnosis is either clinical or assisted with pelvic imaging, usually transvaginal ultrasonography or, occasionally, MRI. Management is based on the woman’s preference regarding future childbearing and may include hysterectomy, other surgical options, or medical hormonal suppressionSuppressionDefense Mechanisms with progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives.
Endometrial atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation: benignBenignFibroadenoma condition in which the endometrial lining becomes thin and atrophic because of prolonged states of low estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy. With little to no fluid in the cavity, friction may lead to micro-erosions and a subsequent inflammatory reaction that typically presents with postmenopausal light bleeding or spotting. Endometrial atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation is diagnosed on ultrasonography (which shows a thin endometrial lining) in the setting of a negative endometrial biopsyEndometrial BiopsyDiagnostic Procedures in Gynecology. No treatment is required.
Endometrial or cervical polyps: pedunculated or sessile projections of the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development that result from overgrowth of endometrial glands and stroma around a central vascular stalk. Although these polyps are usually benignBenignFibroadenoma, they can be malignant, particularly in postmenopausal women. Endometrial or cervical polyps present with abnormal uterine or postmenopausal bleeding, though many are asymptomatic. Endometrial polypsEndometrial polypsEndometrial polyps are pedunculated or sessile projections of the endometrium that result from overgrowth of endometrial glands and stroma around a central vascular stalk. Endometrial polyps are a few millimeters to a few centimeters in size, can occur anywhere within the uterine cavity, and, while usually benign, can be malignant, particularly in postmenopausal women. Endometrial Polyps are best diagnosed with saline-infusion sonographySaline-Infusion SonographyCongenital Malformations of the Female Reproductive System (SISSISInfertility) and are usually treated with hysteroscopic resection.
Leiomyomas (uterine fibroidsUterine FibroidsGynecological Imaging): common, benignBenignFibroadenoma tumors arising from smooth muscle cells in the uterine myometrium. Leiomyomas typically present with abnormal bleeding, pelvic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and/or bulk symptoms. FibroidsFibroidsA benign tumor derived from smooth muscle tissue, also known as a fibroid tumor. They rarely occur outside of the uterus and the gastrointestinal tract but can occur in the skin and subcutaneous tissue, probably arising from the smooth muscle of small blood vessels in these tissues.Infertility are identified as a hypoechoicHypoechoicA structure that produces a low-amplitude echo (darker grays)Ultrasound (Sonography), well-circumscribed, round massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast on pelvic ultrasonography. Leiomyomas of the vaginal wall are also possible, though extremely rare.
LeiomyosarcomaLeiomyosarcomaUterine leiomyomas (or uterine fibroids) are benign tumors arising from smooth muscle cells in the uterine myometrium. Leiomyosarcomas, however, are malignant tumors, arising de novo (not from fibroids). Uterine Leiomyoma and Leiomyosarcoma: rare,malignant tumors of uterine smooth muscle that arise de novo (i.e., not from the malignant transformationTransformationChange brought about to an organism’s genetic composition by unidirectional transfer (transfection; transduction, genetic; conjugation, genetic, etc.) and incorporation of foreign DNA into prokaryotic or eukaryotic cells by recombination of part or all of that DNA into the cell’s genome.Bacteriology of fibroidsFibroidsA benign tumor derived from smooth muscle tissue, also known as a fibroid tumor. They rarely occur outside of the uterus and the gastrointestinal tract but can occur in the skin and subcutaneous tissue, probably arising from the smooth muscle of small blood vessels in these tissues.Infertility). They present similarly to benignBenignFibroadenoma leiomyomas (with abnormal bleeding, pelvic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and bulk symptoms), making diagnosis difficult. They are usually diagnosed on post-operative hysterectomy specimens done for suspected fibroidsFibroidsA benign tumor derived from smooth muscle tissue, also known as a fibroid tumor. They rarely occur outside of the uterus and the gastrointestinal tract but can occur in the skin and subcutaneous tissue, probably arising from the smooth muscle of small blood vessels in these tissues.Infertility. Management involves surgical excision (if not already done) and possibly adjuvantAdjuvantSubstances that augment, stimulate, activate, potentiate, or modulate the immune response at either the cellular or humoral level. The classical agents (freund’s adjuvant, bcg, corynebacterium parvum, et al.) contain bacterial antigens. Some are endogenous (e.g., histamine, interferon, transfer factor, tuftsin, interleukin-1). Their mode of action is either non-specific, resulting in increased immune responsiveness to a wide variety of antigens, or antigen-specific, i.e., affecting a restricted type of immune response to a narrow group of antigens. The therapeutic efficacy of many biological response modifiers is related to their antigen-specific immunoadjuvanticity.VaccinationchemotherapyChemotherapyOsteosarcoma.
Cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer: invasive cancer of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy (and the most common gynecologic cancer worldwide). There are 2 major histologic types of cervical cancerCervical cancerCervical cancer, or invasive cervical carcinoma (ICC), is the 3rd most common cancer in women in the world, with > 50% of the cases being fatal. In the United States, ICC is the 13th most common cancer and the cause of < 3% of all cancer deaths due to the slow progression of precursor lesions and, more importantly, effective cancer screening. Cervical Cancer: SCC and adenocarcinoma, the vast majority of which are caused by high-risk HPVHPVHuman papillomavirus (HPV) is a nonenveloped, circular, double-stranded DNA virus belonging to the Papillomaviridae family. Humans are the only reservoir, and transmission occurs through close skin-to-skin or sexual contact. Human papillomaviruses infect basal epithelial cells and can affect cell-regulatory proteins to result in cell proliferation. Papillomavirus (HPV)infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease. Early cervical neoplasia is asymptomatic, though more advanced disease may present with abnormal bleeding (especially bleeding on contact). Diagnosis is made by Pap testing with cytology, HPV testingHPV testingCervical Cancer Screening, and biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
Smith, R.A., et al.; ACS Prostate Cancer Advisory Committee, ACS Colorectal Cancer Advisory Committee, ACS Endometrial Cancer Advisory Committee. (2001). American Cancer Society guidelines for the early detection of cancer: update of early detection guidelines for prostate, colorectal, and endometrial cancers. CA Cancer J Clin. 51(1), 38–75. https://pubmed.ncbi.nlm.nih.gov/11577479/
Khati, N.J., et al. (2014). Expert Panel on Women’s Imaging. ACR Appropriateness Criteria: abnormal vaginal bleeding. Reston, VA: American College of Radiology, pp. 1–13.
Trimble, C.L., et al., Society of Gynecologic Oncology Clinical Practice Committee. (2012). Management of endometrial precancers. Obstet Gynecol 120:1160–1175. https://pubmed.ncbi.nlm.nih.gov/23090535/
Create your free account or log in to continue reading!