Adrenal Insufficiency and Addison Disease (Clinical)
Adrenal Insufficiency and Addison Disease (Clinical)
Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease (AI) is the inadequate production of adrenocortical hormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types: glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids, mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids, and adrenal androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens. Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease, also called Addison disease, is caused by adrenal gland disorder (autoimmune disease, infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, and malignancyMalignancyHemothorax, among others). Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease can also occur because of decreased production of adrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones (ACTH) from disease in the pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland (secondary) or hypothalamic disorders and prolonged glucocorticoid therapy (tertiary). Diagnosis is by demonstrating hypocortisolism (via cortisolCortisolGlucocorticoids and ACTH levels and ACTH-stimulation testActh-Stimulation TestAdrenal Insufficiency and Addison Disease) and determining the etiology (adrenal autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques, imaging). Glucocorticoid replacement is needed in all forms of AI. Additionally, in primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease, mineralocorticoid is given to prevent volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration, salt loss, and hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia. Adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease is a medical emergency; management requires prompt IV hydrationIv HydrationCrush Syndrome and administration of IV glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids without waiting for initial hormone results.
Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease (AI) is the deficiency in adrenal production of glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids, adrenal androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens, and mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids.
Forms of adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease[6,7]
Primary (Addison disease): dysfunction or destruction of the adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy
Secondary: conditions that cause deficiency in pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Typesadrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones (ACTH) secretionSecretionCoagulation Studies
Tertiary: conditions that cause deficiency in the hypothalamic secretionSecretionCoagulation Studies of corticotropin-releasing hormoneCorticotropin-releasing hormoneA peptide of about 41 amino acids that stimulates the release of adrenocorticotropic hormone. Crh is synthesized by neurons in the paraventricular nucleus of the hypothalamus. After being released into the pituitary portal circulation, crh stimulates the release of acth from the pituitary gland. Crh can also be synthesized in other tissues, such as placenta; adrenal medulla; and testis.Hypothalamic and Pituitary Hormones (CRH)
Epidemiology[6,7]
Annual incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 4–6 cases per million people
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are diagnosed in the 6th decade of life.
Hospitalizations have increased in recent decades:[8]
Admissions for AI (mostly secondary): ↑ 62% between 2000 and 2019 (from 36.8/million to 59.6/million)
Admissions for adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease: ↑ 90% (from 10.7/million to 20.4/million)
Adrenal glands:
Small, triangular glands that sit on top of the kidneys (suprarenal glands)
Etiology of primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease[2,5,14]
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease is caused by processes that affect the adrenal gland’s ability to produce cortisolCortisolGlucocorticoids. The most common cause is idiopathicIdiopathicDermatomyositis autoimmune destruction (adrenalitis).
Autoimmune polyendocrine syndrome type IAutoimmune polyendocrine syndrome type IAdrenal Insufficiency and Addison Disease (APECED (autoimmune polyendocrinopathy, candidiasisCandidiasisCandida is a genus of dimorphic, opportunistic fungi. Candida albicans is part of the normal human flora and is the most common cause of candidiasis. The clinical presentation varies and can include localized mucocutaneous infections (e.g., oropharyngeal, esophageal, intertriginous, and vulvovaginal candidiasis) and invasive disease (e.g., candidemia, intraabdominal abscess, pericarditis, and meningitis). Candida/Candidiasis, ectodermal dystrophy) syndrome):
Addison disease
Chronic mucocutaneous candidiasisChronic mucocutaneous candidiasisA clinical syndrome characterized by development, usually in infancy or childhood, of a chronic, often widespread candidiasis of skin, nails, and mucous membranes. It may be secondary to one of the immunodeficiency syndromes, inherited as an autosomal recessive trait, or associated with defects in cell-mediated immunity, endocrine disorders, dental stomatitis, or malignancy.Adaptive Immune Response
HypoparathyroidismHypoparathyroidismHypoparathyroidism is defined as reduced parathyroid hormone (PTH) levels due to poor function of the parathyroid glands. The cause of hypoparathyroidism is most commonly iatrogenic following neck surgery, but it can also be associated with genetic or autoimmune disorders as well as infiltrative diseases causing destruction of the normal parathyroid tissue. Hypoparathyroidism
Primary gonadal failure
HypoplasiaHypoplasiaHypoplastic Left Heart Syndrome (HLHS) of the dental enamelEnamelA hard thin translucent layer of calcified substance which envelops and protects the dentin of the crown of the tooth. It is the hardest substance in the body and is almost entirely composed of calcium salts. Under the microscope, it is composed of thin rods (enamel prisms) held together by cementing substance, and surrounded by an enamel sheath.Teeth: Anatomy
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus type 1Type 1Spinal Muscular Atrophy
Pernicious anemiaPernicious anemiaA megaloblastic anemia occurring in children but more commonly in later life, characterized by histamine-fast achlorhydria, in which the laboratory and clinical manifestations are based on malabsorption of vitamin B12 due to a failure of the gastric mucosa to secrete adequate and potent intrinsic factor.Megaloblastic Anemia
VitiligoVitiligoVitiligo is the most common depigmenting disorder and is caused by the destruction of melanocytes. Patients present with hypo- or depigmented macules or patches which often occur on the face, hands, knees, and/or genitalia. Vitiligo
Celiac diseaseCeliac diseaseCeliac disease (also known as celiac sprue or gluten enteropathy) is an autoimmune reaction to gliadin, which is a component of gluten. Celiac disease is closely associated with HLA-DQ2 and HLA-DQ8. The immune response is localized to the proximal small intestine and causes the characteristic histologic findings of villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis. Celiac Disease
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease that replace adrenal tissue (15%):
TuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
Fungal infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (coccidioidomycosisCoccidioidomycosisCoccidioidomycosis, commonly known as San Joaquin Valley fever, is a fungal disease caused by Coccidioides immitis or Coccidioides posadasii. When Coccidioides spores are inhaled, they transform into spherules that result in infection. Coccidioidomycosis is also a common cause of community-acquired pneumonia and can cause severe disease in the immunocompromised.Coccidioides/Coccidioidomycosis, histoplasmosisHistoplasmosisHistoplasmosis is an infection caused by Histoplasma capsulatum, a dimorphic fungus. Transmission is through inhalation, and exposure to soils containing bird or bat droppings increases the risk of infection. Most infections are asymptomatic; however, immunocompromised individuals generally develop acute pulmonary infection, chronic infection, or even disseminated disease.Histoplasma/Histoplasmosis)
CytomegalovirusCytomegalovirusCMV is a ubiquitous double-stranded DNA virus belonging to the Herpesviridae family. CMV infections can be transmitted in bodily fluids, such as blood, saliva, urine, semen, and breast milk. The initial infection is usually asymptomatic in the immunocompetent host, or it can present with symptoms of mononucleosis. Cytomegalovirus
Infiltrative disease of the adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy:
SarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis
Amyloid
HemochromatosisHemochromatosisA disorder of iron metabolism characterized by a triad of hemosiderosis; liver cirrhosis; and diabetes mellitus. It is caused by massive iron deposits in parenchymal cells that may develop after a prolonged increase of iron absorption.Hereditary Hemochromatosis
Malignancies affecting the adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy:
Metastases from lung, breast, renal, or GI primary tumors
Intra-adrenal hemorrhageIntra-adrenal hemorrhageA condition of hemorrhage and necrosis of the adrenal gland. It is characterized by rapidly developing adrenal insufficiency; hypotension; and widespread cutaneous purpura.Adrenal Insufficiency and Addison Disease:
Waterhouse–Friderichsen syndromeWaterhouse–Friderichsen syndromeA condition of hemorrhage and necrosis of the adrenal gland. It is characterized by rapidly developing adrenal insufficiency; hypotension; and widespread cutaneous purpura.Adrenal Insufficiency and Addison Disease after meningococcal septicemia
Antiphospholipid syndromeAntiphospholipid syndromeAntiphospholipid syndrome (APLS) is an acquired autoimmune disorder characterized by the persistent presence of antiphospholipid antibodies, which create a hypercoagulable state. These antibodies are most commonly discovered during a workup for a thrombotic event or recurrent pregnancy loss, which are the 2 most common clinical manifestations.Antiphospholipid Syndrome
Adrenoleukodystrophies: rare X-linkedX-linkedGenetic diseases that are linked to gene mutations on the X chromosome in humans or the X chromosome in other species. Included here are animal models of human X-linked diseases.Common Variable Immunodeficiency (CVID) condition (1:25,000)
Congenital adrenal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation:
Mutations of the 21-hydroxylase (CYP21A2) or 11 beta-hydroxylase (CYP11B1) genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure → nearly complete deficiency of an enzyme required for cortisolCortisolGlucocorticoidssynthesisSynthesisPolymerase Chain Reaction (PCR)
Presents in infancy with adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease and salt-wasting crisis
ACTH resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing syndromes (familial glucocorticoid resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing)
KetoconazoleKetoconazoleBroad spectrum antifungal agent used for long periods at high doses, especially in immunosuppressed patients.Azoles
FluconazoleFluconazoleTriazole antifungal agent that is used to treat oropharyngeal candidiasis and cryptococcal meningitis in aids.Azoles
EtomidateEtomidateImidazole derivative anesthetic and hypnotic with little effect on blood gases, ventilation, or the cardiovascular system. It has been proposed as an induction anesthetic.Intravenous Anesthetics
Secondary and tertiary AITertiary AIDeficiency in the hypothalamic secretion of corticotropin-releasing hormone (CRH).Adrenal Insufficiency and Addison Disease are a consequence of dysfunction of the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus and pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland. Secondary AISecondary AIDeficiency in pituitary adrenocorticotropic hormone (ACTH) secretion.Adrenal Insufficiency and Addison Disease is most often due to glucocorticoid therapy in greater than physiologic doses, used for treating rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis, inflammatory bowel disease, and severe asthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma.
Secondary:
HypopituitarismHypopituitarismHypopituitarism is a condition characterized by pituitary hormone deficiency. This condition primarily results from a disease of the pituitary gland, but it may arise from hypothalamic dysfunction. Pituitary tumors are one of the most common causes. The majority of cases affect the anterior pituitary lobe (adenohypophysis), which accounts for 80% of the gland. Hypopituitarism
Pituitary tumorsPituitary tumorsNeoplasms which arise from or metastasize to the pituitary gland. The majority of pituitary neoplasms are adenomas, which are divided into non-secreting and secreting forms. Hormone producing forms are further classified by the type of hormone they secrete. Pituitary adenomas may also be characterized by their staining properties. Pituitary tumors may compress adjacent structures, including the hypothalamus, several cranial nerves, and the optic chiasm. Chiasmal compression may result in bitemporal hemianopsia.Pituitary Adenomas, irradiation, and surgery
Granulomatous/infiltrative disease (tuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis, sarcoid, eosinophilic granuloma)
Postpartum pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types infarction (Sheehan’s syndromeSheehan’s syndromePostpartum pituitary necrosis caused by blood loss during childbirth.Hypopituitarism)
Medications:
Exogenous glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Long-term and high-dose opiatesOpiatesOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates.Opioid Analgesics
NivolumabNivolumabA genetically engineered, fully humanized immunoglobulin g4 monoclonal antibody that binds to the pd-1 receptor, activating an immune response to tumor cells. It is used as monotherapy or in combination with ipilimumab for the treatment of advanced malignant melanoma. It is also used in the treatment of advanced or recurring non-small cell lung cancer; renal cell carcinoma; and Hodgkin’s lymphoma.Melanoma
High-dose progestinsProgestinsCompounds that interact with progesterone receptors in target tissues to bring about the effects similar to those of progesterone. Primary actions of progestins, including natural and synthetic steroids, are on the uterus and the mammary gland in preparation for and in maintenance of pregnancy.Hormonal Contraceptives (e.g., megestrol acetateMegestrol acetateMegestrol acetate is a progestogen with actions and uses similar to those of the progestogens in general. It also has anti-androgenic properties. It is given by mouth in the palliative treatment or as an adjunct to other therapy in endometrial carcinoma and in breast cancer.Noncontraceptive Estrogen and Progestins for metastatic breast cancerBreast cancerBreast cancer is a disease characterized by malignant transformation of the epithelial cells of the breast. Breast cancer is the most common form of cancer and 2nd most common cause of cancer-related death among women. Breast Cancer)
POMC geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics mutations
TPITgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics mutations
Familial cortisol-binding globulin deficiency
Tertiary:
Prolonged high-dose glucocorticoid use
Effect of Cushing syndromeCushing syndromeA condition caused by prolonged exposure to excess levels of cortisol (hydrocortisone) or other glucocorticoids from endogenous or exogenous sources. It is characterized by upper body obesity; osteoporosis; hypertension; diabetes mellitus; hirsutism; amenorrhea; and excess body fluid. Endogenous Cushing syndrome or spontaneous hypercortisolism is divided into two groups, those due to an excess of adrenocorticotropin and those that are acth-independent.Paraneoplastic Syndromes treatment:
Chronic elevation of glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids (e.g., from tumorTumorInflammation effects) has suppressed the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus–pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types–adrenal axis.
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease due to autoimmune destruction is most often caused by serum antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against steroidogenic enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes, most commonly P450c21 (CYP21A2, 21-hydroxylase) and occasionally others. The pathophysiology in all cases involves the lack of mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids and glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids needed to promote sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia retention and enhance vasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure.
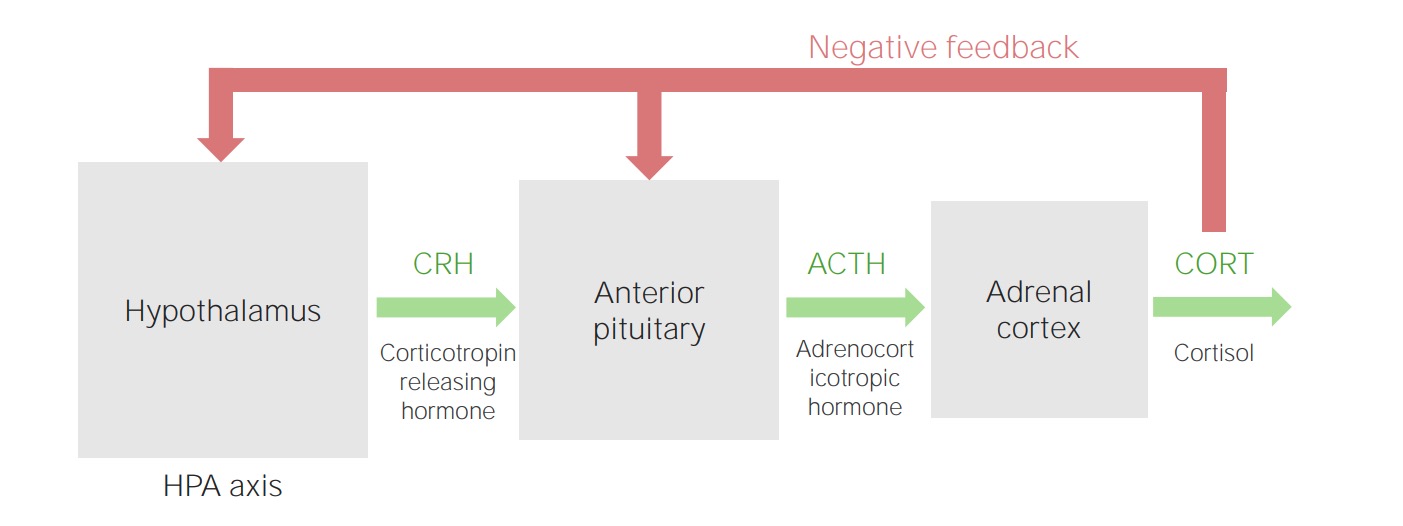
Hormonal regulation[1,6,7]
Hypothalamic–pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types–adrenal (HPA) axis:
HypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus secretes CRH → release of ACTH from the anterior pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland
ACTH release:
Like CRH, release is pulsatile, following the circadian rhythmCircadian RhythmThe regular recurrence, in cycles of about 24 hours, of biological processes or activities, such as sensitivity to drugs or environmental and physiological stimuli.Cranial Nerve Palsies.
↑ in the early morning hours (before awakening), with peak levels in the morning (approximately 8:30 a.m.) and ↓ in the evening
Adrenal gland (cortex):
ACTH mainly stimulates the zona fasciculataZona FasciculataThe wide middle zone of the adrenal cortex. This zone produces a series of enzymes that convert pregnenolone to cortisol (hydrocortisone) via 17-alpha-hydroxyprogesterone.Adrenal Glands: Anatomy (cortisolCortisolGlucocorticoids) and zona reticularisZona ReticularisThe inner zone of the adrenal cortex. This zone produces the enzymes that convert pregnenolone, a 21-carbon steroid, to 19-carbon steroids (dehydroepiandrosterone; and androstenedione) via 17-alpha-hydroxypregnenolone.Adrenal Glands: Anatomy (androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens).
The zona glomerulosaZona GlomerulosaThe narrow subcapsular outer zone of the adrenal cortex. This zone produces a series of enzymes that convert pregnenolone to aldosterone. The final steps involve three successive oxidations by cytochrome p-450 cyp11b2.Adrenal Glands: Anatomy (aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia) is primarily regulated by the reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation–angiotensin system and potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia levels.
↓ GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance uptake by cells and ↑ gluconeogenesisGluconeogenesisGluconeogenesis is the process of making glucose from noncarbohydrate precursors. This metabolic pathway is more than just a reversal of glycolysis. Gluconeogenesis provides the body with glucose not obtained from food, such as during a fasting period. The production of glucose is critical for organs and cells that cannot use fat for fuel. Gluconeogenesis
↑ LipolysisLipolysisThe metabolic process of breaking down lipids to release free fatty acids, the major oxidative fuel for the body. Lipolysis may involve dietary lipids in the digestive tract, circulating lipids in the blood, and stored lipids in the adipose tissue or the liver. A number of enzymes are involved in such lipid hydrolysis, such as lipase and lipoprotein lipase from various tissues.Metabolic Dysfunction-associated Steatotic Liver Disease (MASLD) → release of fatty acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance into the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment
↑ Smooth muscle (vasculature) sensitivity to catecholaminesCatecholaminesA general class of ortho-dihydroxyphenylalkylamines derived from tyrosine.Adrenal Hormones and angiotensin IIAngiotensin IIAn octapeptide that is a potent but labile vasoconstrictor. It is produced from angiotensin I after the removal of two amino acids at the c-terminal by angiotensin converting enzyme. The amino acid in position 5 varies in different species. To block vasoconstriction and hypertension effect of angiotensin II, patients are often treated with ace inhibitors or with angiotensin II type 1 receptor blockers.Renal Sodium and Water Regulation (producing ↑ blood pressure)
Antiinflammatory actions:
ApoptosisApoptosisA regulated cell death mechanism characterized by distinctive morphologic changes in the nucleus and cytoplasm, including the endonucleolytic cleavage of genomic DNA, at regularly spaced, internucleosomal sites, I.e., DNA fragmentation. It is genetically-programmed and serves as a balance to mitosis in regulating the size of animal tissues and in mediating pathologic processes associated with tumor growth.Ischemic Cell Damage of T cellsT cellsLymphocytes responsible for cell-mediated immunity. Two types have been identified – cytotoxic (t-lymphocytes, cytotoxic) and helper T-lymphocytes (t-lymphocytes, helper-inducer). They are formed when lymphocytes circulate through the thymus gland and differentiate to thymocytes. When exposed to an antigen, they divide rapidly and produce large numbers of new T cells sensitized to that antigen.T cells: Types and Functions
↓ Antibody production
↓ Neutrophil migration
AndrogensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens:
DehydroepiandrosteroneDehydroepiandrosteroneA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (DHEA) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens (DHEADHEAA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (dhea) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens) and DHEADHEAA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (dhea) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens sulfate (DHEA-S) from the adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy: major source of androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens in women and prepubertal children
Some forms of AI may include androgen deficiency.
Exception is congenital adrenal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation in children:
21-hydroxylase deficiency21-hydroxylase deficiencyCongenital Adrenal Hyperplasia or 11-beta-hydroxylase deficiency causes disrupted steroid biosynthesisBiosynthesisThe biosynthesis of peptides and proteins on ribosomes, directed by messenger RNA, via transfer RNA that is charged with standard proteinogenic amino acids.Virology; signals an increase in ACTH
Results in adrenal insufficiency but adrenal androgen excess
DHEADHEAA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (dhea) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens:
Weak androgenic activity
Precursor can be peripherally converted to more potent androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens (e.g., testosteroneTestosteroneA potent androgenic steroid and major product secreted by the leydig cells of the testis. Its production is stimulated by luteinizing hormone from the pituitary gland. In turn, testosterone exerts feedback control of the pituitary LH and FSH secretion. Depending on the tissues, testosterone can be further converted to dihydrotestosterone or estradiol.Androgens and Antiandrogens) and estrogens (e.g., estradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins).
In postpubertal males, the testesTestesGonadal Hormones are the main source of androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens.
MineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids:
Regulation of renal sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia and water reabsorption
Regulation of potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia excretion
Hypothalamic–pituitary–adrenal cortex axis
Image by Lecturio.
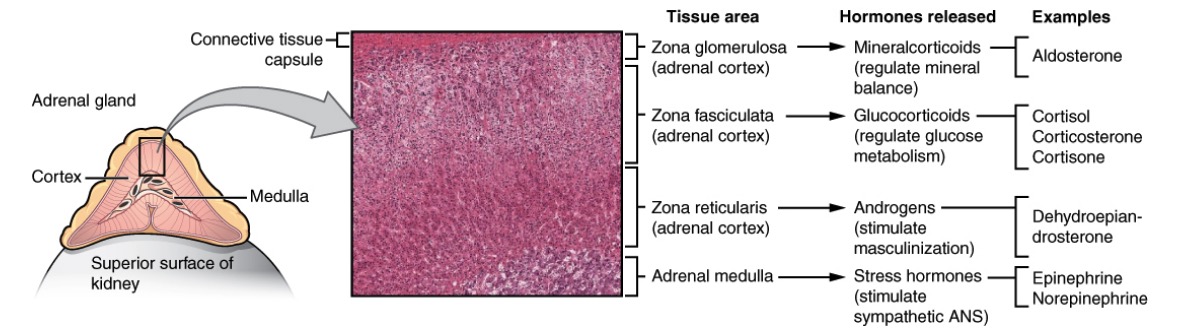
Anatomy, histology, and physiology of different zones of the adrenal gland: The cortex has zona glomerulosa that produces mineralocorticoids (salt), zona fasciculata that produces glucocorticoids (sugar), and zona reticularis that produces androgens (sex). The adrenal medulla produces epinephrine and norepinephrine (stress).
Image: “Adrenal Glands” by OpenStax College, Anatomy and Physiology. OpenStax CNX. License: CC BY 4.0
Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease[6,7]
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease:
Manifestations emerge when > 90% of the adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy (zona glomerulosaZona GlomerulosaThe narrow subcapsular outer zone of the adrenal cortex. This zone produces a series of enzymes that convert pregnenolone to aldosterone. The final steps involve three successive oxidations by cytochrome p-450 cyp11b2.Adrenal Glands: Anatomy, fasciculata, and reticularis) is destroyed.
Hypocortisolism, hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism, and hypoandrogenism (men still produce androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens in testesTestesGonadal Hormones)
Compensatory ↑ ACTH:
Leads to hyperpigmentationHyperpigmentationExcessive pigmentation of the skin, usually as a result of increased epidermal or dermal melanin pigmentation, hypermelanosis. Hyperpigmentation can be localized or generalized. The condition may arise from exposure to light, chemicals or other substances, or from a primary metabolic imbalance.Malassezia Fungi
Both ACTH and ɑ-melanin-stimulating hormone are derived from pro-opiomelanocortin (POMC) → melanocytesMelanocytesMammalian pigment cells that produce melanins, pigments found mainly in the epidermis, but also in the eyes and the hair, by a process called melanogenesis. Coloration can be altered by the number of melanocytes or the amount of pigment produced and stored in the organelles called melanosomes. The large non-mammalian melanin-containing cells are called melanophores.Skin: Structure and Functions stimulated
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia production preserved (as primary regulation is through the reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation–angiotensin system)
No hyperpigmentationHyperpigmentationExcessive pigmentation of the skin, usually as a result of increased epidermal or dermal melanin pigmentation, hypermelanosis. Hyperpigmentation can be localized or generalized. The condition may arise from exposure to light, chemicals or other substances, or from a primary metabolic imbalance.Malassezia Fungi, as ACTH is not increased
↓ CRH → ↓ ACTH→ hypocortisolism and hypoandrogenism
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia production preserved
Normal adrenal function
Image by Lecturio.
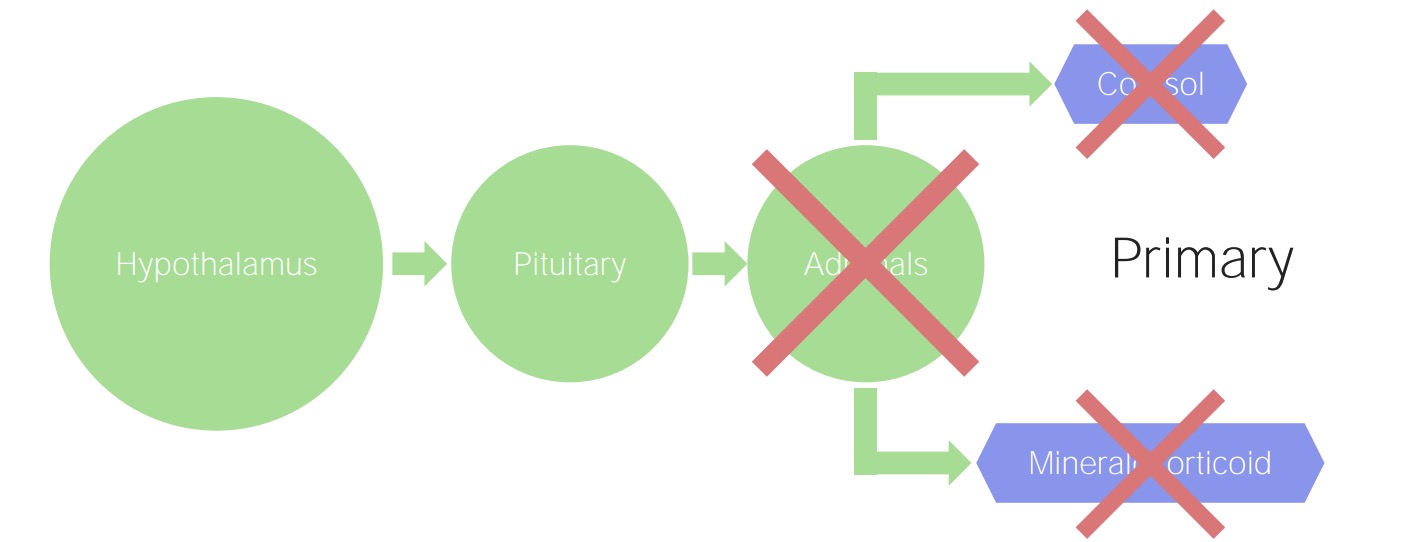
Primary adrenal insufficiency: The adrenals are damaged, regardless of the etiology. Consequently, there is a decline in the production of cortisol and mineralocorticoids.
Image by Lecturio.
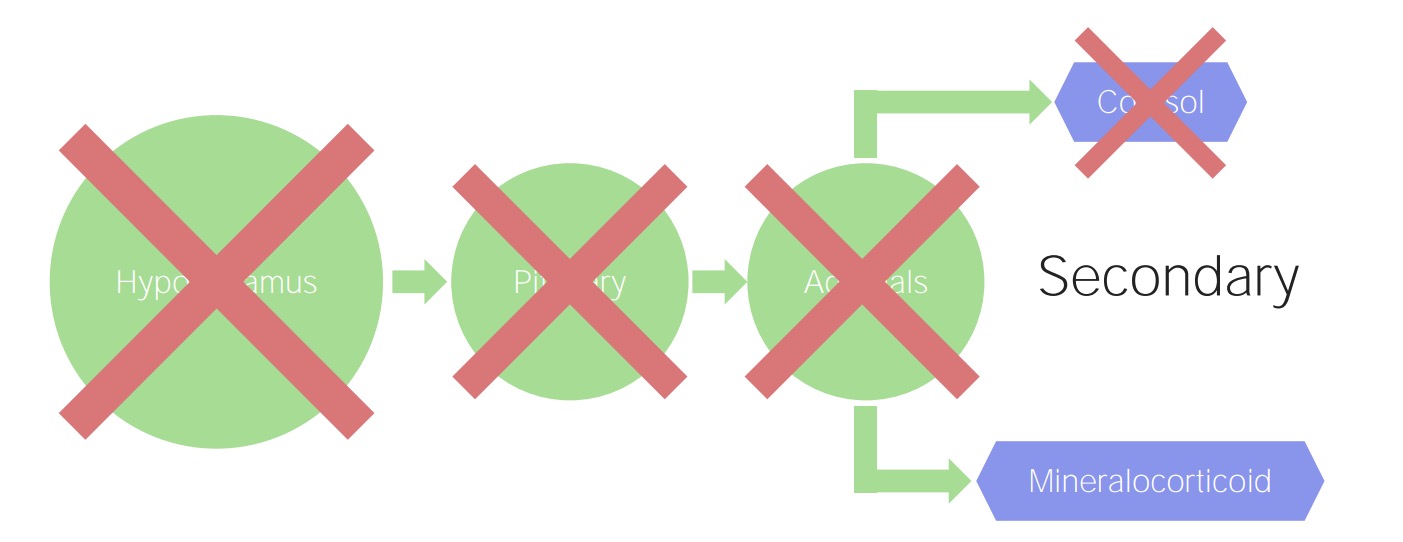
Secondary and tertiary adrenal insufficiency: A pituitary (secondary) or hypothalamic (tertiary) problem results in decreased stimulation of cortisol. However, mineralocorticoid production is regulated by the renin–angiotensin–aldosterone system, so this adrenal function remains preserved.
Image by Lecturio.
Clinical Presentation
The signs and symptoms of AI depend on the rate at which it develops and the degree of loss of adrenal hormonesAdrenal hormonesThere are 2 primary portions of the adrenal glands, the adrenal medulla and the adrenal cortex. The adrenal medulla is the inner portion of the gland, secreting epinephrine and, to a lesser degree, norepinephrine. The adrenal cortex is the outer portion of the gland and secretes mineralocorticoids, glucocorticoids, and androgens. Adrenal Hormones. Many symptoms are similar in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with different types of AI. Still, the clinical presentation varies depending on whether AI is acute (adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease) or chronic (primary, secondary, or tertiary).
Primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease[2,6,7]
Signs and symptoms of primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease relate to glucocorticoid, mineralocorticoid, and androgen deficiency.
↓GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids:
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
Weight lossWeight lossDecrease in existing body weight.Bariatric Surgery/anorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
Abdominal painAbdominal PainAcute Abdomen/diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (including orthostatic hypotensionOrthostatic hypotensionA significant drop in blood pressure after assuming a standing position. Orthostatic hypotension is a finding, and defined as a 20-mm hg decrease in systolic pressure or a 10-mm hg decrease in diastolic pressure 3 minutes after the person has risen from supine to standing. Symptoms generally include dizziness, blurred vision, and syncope.Hypotension)
HypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (due to ↑ antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia)
↓ MineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids:
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (including orthostatic hypotensionOrthostatic hypotensionA significant drop in blood pressure after assuming a standing position. Orthostatic hypotension is a finding, and defined as a 20-mm hg decrease in systolic pressure or a 10-mm hg decrease in diastolic pressure 3 minutes after the person has risen from supine to standing. Symptoms generally include dizziness, blurred vision, and syncope.Hypotension)
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
LethargyLethargyA general state of sluggishness, listless, or uninterested, with being tired, and having difficulty concentrating and doing simple tasks. It may be related to depression or drug addiction.Hyponatremia
Salt craving
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
↓ AndrogensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens:
Dry skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
HyperpigmentationHyperpigmentationExcessive pigmentation of the skin, usually as a result of increased epidermal or dermal melanin pigmentation, hypermelanosis. Hyperpigmentation can be localized or generalized. The condition may arise from exposure to light, chemicals or other substances, or from a primary metabolic imbalance.Malassezia Fungi from ↑ ACTH
Manifestation of primary adrenal insufficiency: Patient presents initially with hyperpigmentation (left). Note the change in skin tone after treatment is administered (right).
Image: “69-year-old female with tiredness and a persistent tan” by Freeman Hospital, Newcastle upon Tyne, United Kingdom. License: CC BY 4.0
Hyperpigmentation: Patient with adrenal insufficiency presents with hyperpigmentation of the oral mucosa.
Image: “Classic hyperpigmentation of Addison’s disease” by FlatOut. License: CC0
Glucocorticoid + androgen deficiency → associated signs/symptoms similar to primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Mineralocorticoid production preserved → associated signs/symptoms not present
No hyperpigmentationHyperpigmentationExcessive pigmentation of the skin, usually as a result of increased epidermal or dermal melanin pigmentation, hypermelanosis. Hyperpigmentation can be localized or generalized. The condition may arise from exposure to light, chemicals or other substances, or from a primary metabolic imbalance.Malassezia Fungi (ACTH not elevated)
Adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease[2,6,10,14]
Adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation (hyperthyroidismHyperthyroidismHypersecretion of thyroid hormones from the thyroid gland. Elevated levels of thyroid hormones increase basal metabolic rate.Thyrotoxicosis and Hyperthyroidism).
Presentation:
Hypovolemic shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock(from reduced volume and mineralocorticoid deficiency)
Can mimic acute abdomenAcute AbdomenAcute abdomen, which is in many cases a surgical emergency, is the sudden onset of abdominal pain that may be caused by inflammation, infection, perforation, ischemia, or obstruction. The location of the pain, its characteristics, and associated symptoms (e.g., jaundice) are important tools that help narrow the differential diagnosis.Acute Abdomen (abdominal tenderness, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever)
Nonspecific symptoms:
Weakness
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
Confusion or decreased responsiveness progressing to comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Precipitating factors:
Severe infection or other acute major stress in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with chronic primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Abrupt withdrawal from supraphysiologic doses of glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids used for other systemic diseases (e.g., asthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma)
Under-replacement of glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids/mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with primary or secondary AISecondary AIDeficiency in pituitary adrenocorticotropic hormone (ACTH) secretion.Adrenal Insufficiency and Addison Disease
Acute adrenal destruction (e.g., hemorrhage)
PituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types infarction
Diagnosis
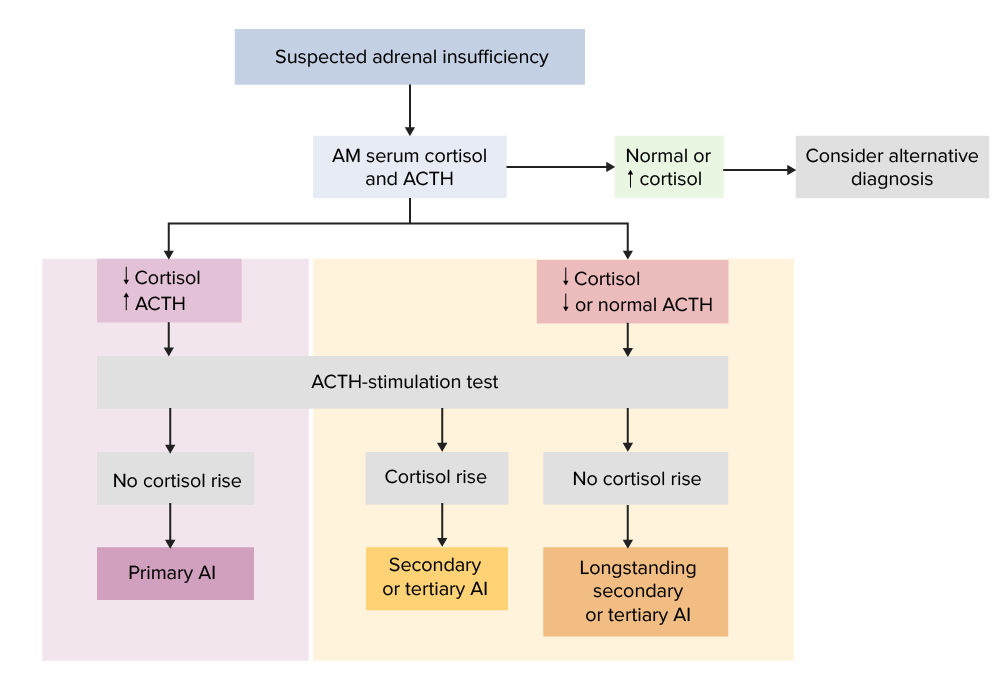
The diagnosis of AI is confirmed by laboratory testing results showing a morning (8 AM) serum cortisolCortisolGlucocorticoids level of < 3 µg/dL. AI is virtually excluded if the cortisolCortisolGlucocorticoids level is > 18 µg/dL, but patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with indeterminate results of 3–18 µg/dL require additional testing. All patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with acute AI should be evaluated for sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, adrenal hemorrhage, and metastatic disease.
Further testing with the cosyntropin stimulation test is needed if the diagnosis is unclear.
ACTH levels:[2,7]
Obtain baseline plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products ACTH level simultaneously with morning cortisolCortisolGlucocorticoids
Interpretation:
↑ ACTH (> 300 ng/L or > 2-fold the upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal; with low cortisolCortisolGlucocorticoids): suggests primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease[6]
With ↑ baseline ACTH → primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Newer monoclonal antibody immune assays or liquid chromatography–massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast spectrometry (LC-MS) assays are more specific; a stimulated cortisolCortisolGlucocorticoids level of 14–15 µg/dL is considered normal.
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductscortisolCortisolGlucocorticoids is protein-bound; falsely ↓ levels can be seen with significant hypoalbuminemiaHypoalbuminemiaA condition in which albumin level in blood (serum albumin) is below the normal range. Hypoalbuminemia may be due to decreased hepatic albumin synthesis, increased albumin catabolism, altered albumin distribution, or albumin loss through the urine (albuminuria).Nephrotic Syndrome in Children.
Simplified diagnostic algorithm for adrenal insufficiency (AI)
ACTH: adrenocorticotropic hormone
Image by Lecturio.
Basal reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation, aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia, and electrolyte levels help in interpretation, especially in primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease:[6,7]
↑ ReninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation → primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
↓ AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia levels → primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
ElectrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes:
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia → more suggestive of primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
Nonanion gap metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis → more suggestive of primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Other laboratory findings[2,6]
Due to glucocorticoid deficiency:
AnemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
HypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia (more common in children)
Due to mineralocorticoid deficiency:
↑ Creatinine (from volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration)
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Table: Summary of diagnostic testing results for adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease[7,12]
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
ReninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation concentration
↑
Normal
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia
↓
Normal
ElectrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes
↑ potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia (hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia)
↓ sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia)
Normal potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia
↓ SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia and increased intravascular volume may be from “inappropriate” increase in vasopressin secretionSecretionCoagulation Studies/SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH))
AI: adrenal insufficiency ACTH: adrenocorticotropic hormone
*In prolonged secondary/tertiary adrenal insufficiency, chronically decreased ACTH leads to adrenal atrophy (low cortisol). This results in no or little increase in cortisol.
ACTH: adrenocorticotropic hormone
AI: adrenal insufficiency
Additional tests for hypothalamic–pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types–adrenal function[7]
The following tests may be performed when initial testing is indeterminate. However, they are typically not required and should be done only in conjunction with specialist consultation.
MetyraponeMetyraponeAn inhibitor of the enzyme steroid 11-beta-monooxygenase. It is used as a test of the feedback hypothalamic-pituitary mechanism in the diagnosis of Cushing syndrome.Adrenal Insufficiency and Addison Disease test:
MetyraponeMetyraponeAn inhibitor of the enzyme steroid 11-beta-monooxygenase. It is used as a test of the feedback hypothalamic-pituitary mechanism in the diagnosis of Cushing syndrome.Adrenal Insufficiency and Addison Disease blocks conversion of 11-deoxycortisol to cortisolCortisolGlucocorticoids.
Oral metyraponeMetyraponeAn inhibitor of the enzyme steroid 11-beta-monooxygenase. It is used as a test of the feedback hypothalamic-pituitary mechanism in the diagnosis of Cushing syndrome.Adrenal Insufficiency and Addison Disease given, followed by obtaining 11-deoxycortisol and cortisolCortisolGlucocorticoids after 24 hours
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease: ↑ ACTH but no increase in 11-deoxycortisol and cortisolCortisolGlucocorticoids
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin causes ↓ glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance, which in turn, triggers cortisolCortisolGlucocorticoidssecretionSecretionCoagulation Studies in normal circumstances.
Inject insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin.
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance, ACTH, and cortisolCortisolGlucocorticoids are measured in intervals.
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease: ↑ ACTH without increase in cortisolCortisolGlucocorticoids despite hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
Secondary AISecondary AIDeficiency in pituitary adrenocorticotropic hormone (ACTH) secretion.Adrenal Insufficiency and Addison Disease: Inadequate ↑ in cortisolCortisolGlucocorticoids and ACTH at the onset of hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
Contraindicated in cardiovascular disease and seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
Corticotropin-releasing hormoneCorticotropin-releasing hormoneA peptide of about 41 amino acids that stimulates the release of adrenocorticotropic hormone. Crh is synthesized by neurons in the paraventricular nucleus of the hypothalamus. After being released into the pituitary portal circulation, crh stimulates the release of acth from the pituitary gland. Crh can also be synthesized in other tissues, such as placenta; adrenal medulla; and testis.Hypothalamic and Pituitary Hormones test differentiates secondary from tertiary adrenal insufficiencyTertiary adrenal insufficiencyDeficiency in the hypothalamic secretion of corticotropin-releasing hormone (CRH).Adrenal Insufficiency and Addison Disease.
In suspected primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease:
Review medications (rule out drug-induced AI).
Adrenocortical antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions or antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against 21-hydroxylase:
Autoimmune adrenalitis
Autoimmune polyendocrine syndrome (proceed with other tests for hypoparathyroidismHypoparathyroidismHypoparathyroidism is defined as reduced parathyroid hormone (PTH) levels due to poor function of the parathyroid glands. The cause of hypoparathyroidism is most commonly iatrogenic following neck surgery, but it can also be associated with genetic or autoimmune disorders as well as infiltrative diseases causing destruction of the normal parathyroid tissue. Hypoparathyroidism, diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy disease)
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products very-long-chain fatty acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance (VLCFAs):
In male patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with isolated Addison disease and negative autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques
Elevated in adrenoleukodystrophy (genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies required)
In children in whom AI presents in infancy or childhood:
CT of the adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy:
Tuberculous adrenalitis: spotty calcifications late in the disease
Adrenal infiltration (sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis, amyloidosisAmyloidosisAmyloidosis is a disease caused by abnormal extracellular tissue deposition of fibrils composed of various misfolded low-molecular-weight protein subunits. These proteins are frequently byproducts of other pathological processes (e.g., multiple myeloma). Amyloidosis, hemochromatosisHemochromatosisA disorder of iron metabolism characterized by a triad of hemosiderosis; liver cirrhosis; and diabetes mellitus. It is caused by massive iron deposits in parenchymal cells that may develop after a prolonged increase of iron absorption.Hereditary Hemochromatosis)
Workup of hypopituitarismHypopituitarismHypopituitarism is a condition characterized by pituitary hormone deficiency. This condition primarily results from a disease of the pituitary gland, but it may arise from hypothalamic dysfunction. Pituitary tumors are one of the most common causes. The majority of cases affect the anterior pituitary lobe (adenohypophysis), which accounts for 80% of the gland. Hypopituitarism (e.g., thyroid-stimulating hormoneThyroid-stimulating hormoneA glycoprotein hormone secreted by the adenohypophysis. Thyrotropin stimulates thyroid gland by increasing the iodide transport, synthesis and release of thyroid hormones (thyroxine and triiodothyronine).Thyroid Hormones (TSH))
MRI of the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus and pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland
CT of adrenal hemorrhage: Contrast imaging of the abdomen and pelvis showing bilateral adrenal hemorrhage (yellow arrows) in a patient presenting with sepsis
Image: “Bilateral adrenal hemorrhages” by Jahanzaib Khwaja. License: CC BY 4.0
Optimal dosing for glucocorticoid replacement therapy for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with primary and secondary AISecondary AIDeficiency in pituitary adrenocorticotropic hormone (ACTH) secretion.Adrenal Insufficiency and Addison Disease is not well agreed on. Still, insufficient replacement can result in adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease, and chronic excess doses may cause cardiovascular disease and increased mortalityMortalityAll deaths reported in a given population.Measures of Health Status.[10]Specialty referral (e.g., endocrinology) is indicated in most cases.
The following information was gleaned from US, UK, and European literature and guidelines.
Adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease
Background:[6,12]
Acute AI is a life-threatening emergency!
Clinical suspicion of adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease requires immediate therapy even before diagnosis is established.
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia
ReninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation
Give rapid infusion of 0.9% saline (start with 1 L within 1 hour)
Add 50 g/L of dextroseDextroseIntravenous Fluids (5%) to fluids if hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia is present.
Amount and rate of fluids should be guided by clinical course and urine output.
Avoid hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation solution → can worsen hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
IV hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants (has mineralocorticoid activity):
100 mg IV every 6–8 hours (IM administration possible if IV access not available)
Can also do continuous infusion
Should see clinical improvement within 4–6 hours[6]
Alternative: prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants
If the diagnosis of AI is yet not established:
May consider a single dose of dexamethasoneDexamethasoneAn anti-inflammatory 9-fluoro-glucocorticoid.Antiemetics 10 mg IV (instead of hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants) → does not interfere with test results
Start rapid infusion of IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids as above.
Perform cosyntropin stimulation test (any time of day), then start IV hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants
Treat hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia, as needed
Once stabilized:[6,12–14]
May slow IV fluid rate, maintain for 24–48 hours
Search for underlying condition and treat accordingly.
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants adjustment:
After 24 hours, can reduce to 50 mg IV every 6 hours
Taper IV dose over the next few days
Eventual dose:
10 mg in the AM
5 mg at lunch
5–10 mg in afternoon
Adjust to the lowest dose that provides symptom relief
Once IV saline is discontinued and daily hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants dose is < 50 mg/day → fludrocortisoneFludrocortisoneA synthetic mineralocorticoid with anti-inflammatory activity.Mineralocorticoids should be started for primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Dose: 0.1 mg daily
Adjust dose (usual range, 0.05–0.2 mg) as needed to maintain:
Normal blood pressure supine and standing
Normal potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level
Start when IV hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants dose has been decreased to < 100 mg.
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 5 mg orally daily in the morning
Adjust to the lowest dose that provides symptom relief (usually 4–7.5 mg daily).
Alternative: hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants 10 mg orally in the morning and 5 mg in the afternoon
Higher doses may be needed concomitantly with drugs that accelerate glucocorticoid metabolism.
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease also require aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia replacement:
Adjust dose (usual range, 0.05–0.2 mg) as needed to maintain:
Normal blood pressure supine and standing
Normal potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level
Chronic adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease
Primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease:[6,10,12,13]
Glucocorticoid replacement:
Oral hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants (in 2–3 divided doses to mimic diurnal rhythm)
Alternatives: prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants/prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants
Situations of stress require escalated doses (e.g., surgery, infection).
Monitor:
Body weight
Symptoms
Blood pressure
Energy
Mineralocorticoid replacement:
Prevention of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, loss of fluids and sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia
Dose increased in warm weather due to salt loss in perspiration
Monitor BP, electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation → adjust dose as needed
Adrenal androgen replacement:
In women, the adrenal gland is the main source of androgensAndrogensAndrogens are naturally occurring steroid hormones responsible for development and maintenance of the male sex characteristics, including penile, scrotal, and clitoral growth, development of sexual hair, deepening of the voice, and musculoskeletal growth. Androgens and Antiandrogens.
DHEADHEAA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (dhea) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens may improve loss of libidoLoss of libidoMale Sexual Dysfunction and/or low energy levels in women.
Discontinue if no benefit after 6-month trial
Underlying causes must be treated (e.g., resection of tumors, antibiotics for infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease).
Similar to primary AIPrimary AIAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease
Options:
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants/prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants
ACTH not used for monitoring and titration of glucocorticoid dose
Mineralocorticoid replacement rarely required
Replacement of other anterior pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and TypeshormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types, if indicated (e.g., thyroxineThyroxineThe major hormone derived from the thyroid gland. Thyroxine is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines (diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood.Thyroid Hormones, growth hormone) → may affect glucocorticoid dosing
Table: Treatment options for chronic adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease[6,10]
Replacement category
Medication
Common dose*
Glucocorticoid
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants
2-dose regimen:
10 mg in AM
5 mg in afternoon
3-dose regimen:
10 mg in AM
5 mg at lunchtime
5 mg in afternoon
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants/prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants
DHEADHEAA major C19 steroid produced by the adrenal cortex. It is also produced in small quantities in the testis and the ovary. Dehydroepiandrosterone (dhea) can be converted to testosterone; androstenedione; estradiol; and estrone.Androgens and Antiandrogens
25–50 mg in AM
*Dose will vary depending on the patient and circumstances.
AM: in the morning
DHEA:dehydroepiandrosterone
Follow-up:[6,10]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be followed closely by endocrinology specialist.
Follow-up should be scheduled annually, at a minimum.
Illness or surgery[6,10,12,13]
Minor illness:
Double the usual dose of glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids for 2–3 days, then resume the maintenance doseMaintenance DoseDosage Calculation
No change to mineralocorticoid dosing needed
Illness with vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia:
Give IV glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids and IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be given a 4-mg vial of dexamethasoneDexamethasoneAn anti-inflammatory 9-fluoro-glucocorticoid.Antiemetics and taught to self-administer IM if medical careMedical careConflict of Interest is not immediately available.
Severe illness:
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants 100 mg for 1 dose
Followed by either:
50 mg IV/IM every 6–8 hours
Continuous infusion (200 mg in 24 hours)
Taper with recovery
Surgery:
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants 50–100 mg IV preoperatively
If major surgery with anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts, follow up with either:
Continuous infusion (200 mg in 24 hours)
50 mg IV every 6 hours
Taper to usual maintenance therapy over 2–3 days if the patient is tolerating oral intake.
Critical illness–related corticosteroid insufficiency (CIRCI) with septic shockSeptic shockSepsis associated with hypotension or hypoperfusion despite adequate fluid resuscitation. Perfusion abnormalities may include, but are not limited to lactic acidosis; oliguria; or acute alteration in mental status.Sepsis and Septic Shock:
Start hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants IV (< 400 mg/day) for ≥ 3 days.
HypopituitarismHypopituitarismHypopituitarism is a condition characterized by pituitary hormone deficiency. This condition primarily results from a disease of the pituitary gland, but it may arise from hypothalamic dysfunction. Pituitary tumors are one of the most common causes. The majority of cases affect the anterior pituitary lobe (adenohypophysis), which accounts for 80% of the gland. Hypopituitarism:pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types hormone deficiency, resulting from a disease of the pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland (commonly tumors), but may arise from hypothalamic dysfunction: The anterior lobeAnterior lobeCerebellum: Anatomy produces growth hormone, follicle-stimulating hormone, luteinizing hormone, TSH, ACTH, and prolactinProlactinA lactogenic hormone secreted by the adenohypophysis. It is a polypeptide of approximately 23 kd. Besides its major action on lactation, in some species prolactin exerts effects on reproduction, maternal behavior, fat metabolism, immunomodulation and osmoregulation.Breasts: Anatomy. Loss of antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia and oxytocin occurs in posterior lobePosterior lobeCerebellum: Anatomy damage. Diagnosis is via hormone levels, provocation tests, and brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification imaging. Treatment is hormonal replacement.
Syndrome of inappropriate antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)): disorder of impaired water excretion due to the inability to suppress the secretionSecretionCoagulation Studies of ADH/vasopressin: This disorder can be due to disease, medications, ectopic secretionSecretionCoagulation Studies by cancer, or hereditary causes (nephrogenic SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)). SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) also occurs in cortisolCortisolGlucocorticoids deficiency. Loss of cortisolCortisolGlucocorticoids results in absence of negative feedbackNegative feedbackHypothalamic and Pituitary Hormones on ADH secretionSecretionCoagulation Studies, increasing ADH. Low cortisolCortisolGlucocorticoids also triggers increased CRH, an ADH secretagogue. HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia and hypoosmolality are findings. Management depends on the underlying etiology.
Congenital adrenal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation (CAHCAHCongenital adrenal hyperplasia (CAH) consists of a group of autosomal recessive disorders that cause a deficiency of an enzyme needed in cortisol, aldosterone, and androgen synthesis. The most common subform of cah is 21-hydroxylase deficiency, followed by 11β-hydroxylase deficiency.Congenital Adrenal Hyperplasia): inherited autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance disease characterized by enzyme deficiency that impairs adrenal hormone production, which results in the overproduction of the hormone precursor. 95% of CAHCAHCongenital adrenal hyperplasia (CAH) consists of a group of autosomal recessive disorders that cause a deficiency of an enzyme needed in cortisol, aldosterone, and androgen synthesis. The most common subform of cah is 21-hydroxylase deficiency, followed by 11β-hydroxylase deficiency.Congenital Adrenal Hyperplasia is due to the absence of the enzyme 21-hydroxylase, leading to inability to produce cortisolCortisolGlucocorticoids, and often accompanied by salt wasting. Females exhibit atypical genitalia from virilizing effects (increased androgen from hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation). Neonatal screeningScreeningPreoperative Care is by measurement of 17-OHP (elevated hydroxyprogesterone). Management involves glucocorticoid and mineralocorticoid therapy.
Adrenoleukodystrophy: a rare X-linkedX-linkedGenetic diseases that are linked to gene mutations on the X chromosome in humans or the X chromosome in other species. Included here are animal models of human X-linked diseases.Common Variable Immunodeficiency (CVID) genetic disorder caused by a mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in the ABCD1geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics and associated with buildup of VLCFAs (very-long-chain fatty acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance): This buildup causes destruction of the myelin sheath of nerves, adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy, and testesTestesGonadal Hormones. Children have learning disabilitiesLearning disabilitiesConditions characterized by a significant discrepancy between an individual’s perceived level of intellect and their ability to acquire new language and other cognitive skills. These may result from organic or psychological conditions. Relatively common subtypes include dyslexia, dyscalculia, and dysgraphia.DiGeorge Syndrome, behavior problems, and quadriparesis. Adrenoleukodystrophy can present in adulthood, with young adults having spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy and gonadal dysfunction. Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease is one of the manifestations. Diagnosis is via a VLCFA panel. Treatment options include glucocorticoid therapy, hematopoietic–cell transplantation, and supportive interventions.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease. Addison’s disease refers specifically to primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease, while other codes cover secondary (pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types) and other forms.
This code is for an ACTH stimulation test, the definitive test for diagnosing primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease. It measures the adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy‘ ability to produce cortisolCortisolGlucocorticoids in response to an injection of synthetic ACTH.
Coding System
Code
Description
CPT
80400
ACTH stimulation panel; for adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease
Medications:
These codes are for the essential hormone replacement therapyHormone Replacement TherapyHormone replacement therapy (HRT) is used to treat symptoms associated with female menopause and in combination to suppress ovulation. Risks and side effects include uterine bleeding, predisposition to cancer, breast tenderness, hyperpigmentation, migraine headaches, hypertension, bloating, and mood changes.Noncontraceptive Estrogen and Progestins for Addison’s disease, which includes a glucocorticoid like hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants and, in primary insufficiency, a mineralocorticoid like fludrocortisoneFludrocortisoneA synthetic mineralocorticoid with anti-inflammatory activity.Mineralocorticoids.
Coding System
Code
Description
RxNorm
5482
HydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants (ingredient)
This code is for an adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease, a life-threatening emergency in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease characterized by profound shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock, hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia, and electrolyte abnormalities, often precipitated by stress or illness.
Coding System
Code
Description
ICD-10-CM
E27.2
Addisonian crisisAddisonian crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease
References
Angelousi, A., Margioris, A. N., Tsatsanis, C. (2020). ACTH action on the adrenals. Endotext. Retrieved February 20, 2023, from http://www.ncbi.nlm.nih.gov/books/NBK279118/
Arlt, W. (2018). Disorders of the adrenal cortex. In Jameson, J. et al. (Eds.), Harrison’s Principles of Internal Medicine (20th ed.) McGraw-Hill.
Carroll, T. B., et al. (2017). Glucocorticoids and adrenal androgens. In Gardner, D. G., Shoback, D. (Eds.), Greenspan’s Basic & Clinical Endocrinology (10th ed.) McGraw-Hill.
Nieman, L. K. (2019). Adrenal cortex. In Crow, M.K., et al. (Eds.), Goldman-Cecil Medicine (26th ed., vol. 1, pp. 1476–1483).
Rushworth, R. L., Torpy, D. J. (2023). The changing epidemiology of adrenal insufficiency: iatrogenic factors predominate. Journal of the Endocrine Society, 7(3), bvad017. https://doi.org/10.1210/jendso/bvad017
Choudhury, S., Lightman, S., Meeran, K. (2019). Improving glucocorticoid replacement profiles in adrenal insufficiency. Clinical Endocrinology, 91(3), 367–371. https://doi.org/10.1111/cen.13999
Husebye, E. S., et al. (2013). Consensus statement on the diagnosis, treatment and follow-up of patients with primary adrenal insufficiency. Journal of Internal Medicine, 275, 104–115. https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.12162
Adamson, S. E., et al. (2023). Endocrine/adrenal failure. In Ancha, S., et al. (Eds.), The Washington Manual of Medical Therapeutics (37th ed., pp. 883–886.)
Fitzgerald, P. A. (2023). Endocrine disorders/primary adrenal insufficiency (Addison disease). In Papadakis, M. A., et al. (Eds.), Current Medical Diagnosis & Treatment (62nd ed., pp. 1156–1160).