Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome (SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome is characterized by keratinocyte necrosisKeratinocyte NecrosisStevens-Johnson Syndrome and separation of the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions from the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will present with a flu-like prodromeProdromeSymptoms that appear 24–48 hours prior to migraine onset.Migraine Headache, followed by cutaneous bullaeBullaeErythema Multiforme and sloughing on the face, thorax, and mucous membranes. Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome is considered a medical emergency, and management is largely supportive. Withdrawal of the causative agent is required. Monitoring for, and treating, superinfection is essential due to the high risk of associated death in these patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome (SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome) and toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome (TEN) are severe mucocutaneous reactions.
Considered a continuum of the same disease
Classified based on the percentage of body surface affected by blisters, erosionsErosionsCorneal Abrasions, Erosion, and Ulcers, and skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions detachment:
Table: Classification of Stevens-Johnson SyndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome and Toxic Epidermal NecrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome
Subtype
Involved BSA
Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome
<10% of BSA
Overlapping SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN
BSA: body surface area
SJS: Stevens-Johnson syndrome
TEN: toxic epidermal necrolysis
Epidemiology[1‒5]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
1–7 cases per million people per year
Higher in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with HIVHIVAnti-HIV Drugs and active cancer
SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome is more common.
SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome: 10%
TEN: 50%
More common in women than men, with a ratio of 2:1
Can occur at any age
Etiology[1,3,4,6,7,10]
Medications
Approximately 70% of cases
Occurs within 8 weeks of medication onset
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Ultraviolet lightUltraviolet lightThat portion of the electromagnetic spectrum immediately below the visible range and extending into the x-ray frequencies. The longer wavelengths (near-uv or biotic or vital rays) are necessary for the endogenous synthesis of vitamin D and are also called antirachitic rays; the shorter, ionizing wavelengths (far-uv or abiotic or extravital rays) are viricidal, bactericidal, mutagenic, and carcinogenic and are used as disinfectants.Bullous Pemphigoid and Pemphigus Vulgaris stimulus
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy
Table: Major common medication and infectious causes of SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN
Types
Examples
Medications
Antiepileptics
LamotrigineLamotrigineA phenyltriazine compound, sodium and calcium channel blocker that is used for the treatment of seizures and bipolar disorder.Second-Generation Anticonvulsant Drugs, phenobarbitalPhenobarbitalA barbituric acid derivative that acts as a nonselective central nervous system depressant. It potentiates gamma-aminobutyric acid action on gaba-a receptors, and modulates chloride currents through receptor channels. It also inhibits glutamate induced depolarizations.First-Generation Anticonvulsant Drugs, carbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs, valproateValproateA fatty acid with anticonvulsant and anti-manic properties that is used in the treatment of epilepsy and bipolar disorder. The mechanisms of its therapeutic actions are not well understood. It may act by increasing gamma-aminobutyric acid levels in the brain or by altering the properties of voltage-gated sodium channels.First-Generation Anticonvulsant Drugs, phenytoinPhenytoinAn anticonvulsant that is used to treat a wide variety of seizures. The mechanism of therapeutic action is not clear, although several cellular actions have been described including effects on ion channels, active transport, and general membrane stabilization. Phenytoin has been proposed for several other therapeutic uses, but its use has been limited by its many adverse effects and interactions with other drugs.First-Generation Anticonvulsant Drugs
Sulfa
Cotrimoxazole, sulfasalazineSulfasalazineA drug that is used in the management of inflammatory bowel diseases. Its activity is generally considered to lie in its metabolic breakdown product, 5-aminosalicylic acid released in the colon.Sulfonamides and Trimethoprim
Other antibiotics
AminopenicillinsAminopenicillinsPenicillins, fluoroquinolonesFluoroquinolonesFluoroquinolones are a group of broad-spectrum, bactericidal antibiotics inhibiting bacterial DNA replication. Fluoroquinolones cover gram-negative, anaerobic, and atypical organisms, as well as some gram-positive and multidrug-resistant (MDR) organisms. Fluoroquinolones, cephalosporinsCephalosporinsCephalosporins are a group of bactericidal beta-lactam antibiotics (similar to penicillins) that exert their effects by preventing bacteria from producing their cell walls, ultimately leading to cell death. Cephalosporins are categorized by generation and all drug names begin with “cef-” or “ceph-.” Cephalosporins
MeloxicamMeloxicamA benzothiazine and thiazole derivative that acts as a nsaid and cyclooxygenase-2 (cox-2) inhibitor. It is used in the treatment of rheumatoid arthritis; osteoarthritis; and ankylosing spondylitis.Nonsteroidal Antiinflammatory Drugs (NSAIDs), piroxicamPiroxicamA cyclooxygenase inhibiting, non-steroidal anti-inflammatory agent (nsaid) that is well established in treating rheumatoid arthritis and osteoarthritis and used for musculoskeletal disorders, dysmenorrhea, and postoperative pain. Its long half-life enables it to be administered once daily.Nonsteroidal Antiinflammatory Drugs (NSAIDs)
Antiretrovirals
NevirapineNevirapineA potent, non-nucleoside reverse transcriptase inhibitor used in combination with nucleoside analogues for treatment of HIV infections and aids.Anti-HIV Drugs
Miscellaneous
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs, chlormezanone
Infectious
Viral
Herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology, HIVHIVAnti-HIV Drugs, coxsackievirusCoxsackievirusCoxsackievirus is a member of a family of viruses called Picornaviridae and the genus Enterovirus. Coxsackieviruses are single-stranded, positive-sense RNA viruses, and are divided into coxsackie group A and B viruses. Both groups of viruses cause upper respiratory infections, rashes, aseptic meningitis, or encephalitis. Coxsackievirus, hepatitis, influenzaInfluenzaInfluenza viruses are members of the Orthomyxoviridae family and the causative organisms of influenza, a highly contagious febrile respiratory disease. There are 3 primary influenza viruses (A, B, and C) and various subtypes, which are classified based on their virulent surface antigens, hemagglutinin (HA) and neuraminidase (NA). Influenza typically presents with a fever, myalgia, headache, and symptoms of an upper respiratory infection. Influenza Viruses/Influenza, mumpsMumpsMumps is caused by a single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae. Mumps is typically a disease of childhood, which manifests initially with fever, muscle pain, headache, poor appetite, and a general feeling of malaise, and is classically followed by parotitis. Mumps Virus/Mumps, Epstein-Barr virusEpstein-Barr VirusEpstein-Barr virus (EBV) is a linear, double-stranded DNA virus belonging to the Herpesviridae family. This highly prevalent virus is mostly transmitted through contact with oropharyngeal secretions from an infected individual. The virus can infect epithelial cells and B lymphocytes, where it can undergo lytic replication or latency. Epstein-Barr Virus, enteroviruses
Bacterial
Group A beta-hemolytic streptococci, brucellosisBrucellosisBrucellosis (also known as undulant fever, Mediterranean fever, or Malta fever) is a zoonotic infection that spreads predominantly through ingestion of unpasteurized dairy products or direct contact with infected animal products. Clinical manifestations include fever, arthralgias, malaise, lymphadenopathy, and hepatosplenomegaly. Brucella/Brucellosis, mycobacteriaMycobacteriaMycobacterium is a genus of the family Mycobacteriaceae in the phylum Actinobacteria. Mycobacteria comprise more than 150 species of facultative intracellular bacilli that are mostly obligate aerobes. Mycobacteria are responsible for multiple human infections including serious diseases, such as tuberculosis (M. tuberculosis), leprosy (M. leprae), and M. avium complex infections.Mycobacterium, Mycoplasma pneumoniaeMycoplasma pneumoniaeShort filamentous organism of the genus mycoplasma, which binds firmly to the cells of the respiratory epithelium. It is one of the etiologic agents of non-viral primary atypical pneumonia in man.Mycoplasma, rickettsiaRickettsiaRickettsiae are a diverse collection of obligate intracellular, gram-negative bacteria that have a tropism for vascular endothelial cells. The vectors for transmission vary by species but include ticks, fleas, mites, and lice. Rickettsia, tularemia
The exact mechanism is unknown, but there are several theories:[1,3,4,6]
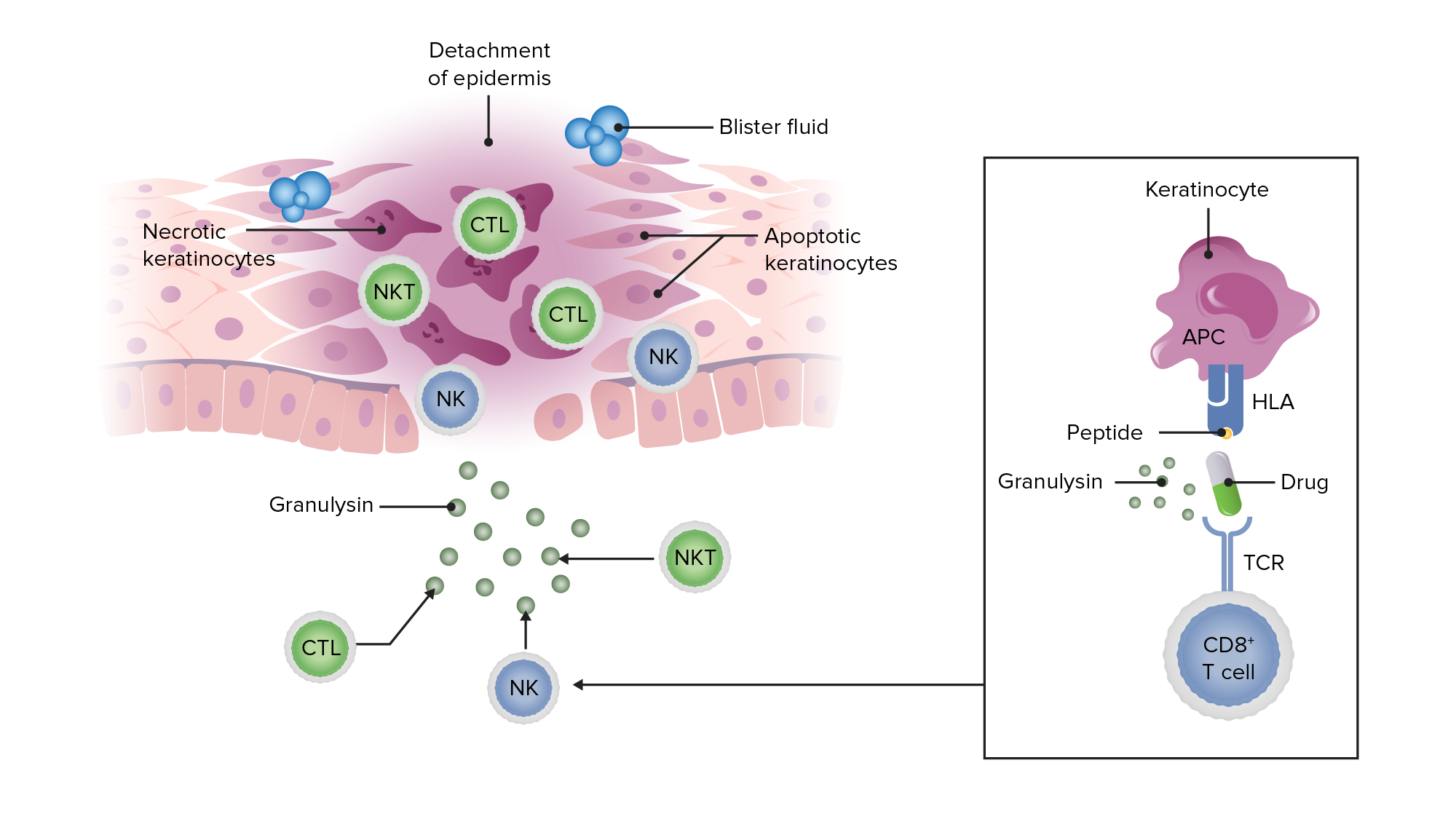
Drug, or infectious, antigenAntigenSubstances that are recognized by the immune system and induce an immune reaction.Vaccination in the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions tissue → stimulates cytotoxicCytotoxicParvovirus B19T cellsT cellsLymphocytes responsible for cell-mediated immunity. Two types have been identified – cytotoxic (t-lymphocytes, cytotoxic) and helper T-lymphocytes (t-lymphocytes, helper-inducer). They are formed when lymphocytes circulate through the thymus gland and differentiate to thymocytes. When exposed to an antigen, they divide rapidly and produce large numbers of new T cells sensitized to that antigen.T cells: Types and Functions, natural killer T cellsNatural killer T cellsA specialized subset of T-lymphocytes that exhibit features of innate immunity similar to that of natural killer cells. They are reactive to glycolipids presented in the context of the major histocompatibility complex (MHC) class i-like molecule, cd1d antigen.T cells: Types and Functions (NKT), and natural killer (NK) cells → granulysinGranulysinStevens-Johnson Syndrome release → keratinocyteKeratinocyteEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Erythema Multiforme death
ApoptosisApoptosisA regulated cell death mechanism characterized by distinctive morphologic changes in the nucleus and cytoplasm, including the endonucleolytic cleavage of genomic DNA, at regularly spaced, internucleosomal sites, I.e., DNA fragmentation. It is genetically-programmed and serves as a balance to mitosis in regulating the size of animal tissues and in mediating pathologic processes associated with tumor growth.Ischemic Cell Damage of keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions → epidermal separation from the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions → characteristic skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions detachment of SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN
Dying cells and necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage → ↑ antigen loadAntigen LoadStevens-Johnson Syndrome → triggers T cellsT cellsLymphocytes responsible for cell-mediated immunity. Two types have been identified – cytotoxic (t-lymphocytes, cytotoxic) and helper T-lymphocytes (t-lymphocytes, helper-inducer). They are formed when lymphocytes circulate through the thymus gland and differentiate to thymocytes. When exposed to an antigen, they divide rapidly and produce large numbers of new T cells sensitized to that antigen.T cells: Types and Functions to continue the inflammatory response → development of fluid-filled blisters
This impaired skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions integrity can lead to:[1,3,4,6]
Water loss
Secondary bacterial infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease and sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
Schematic showing how a peptide antigen (in this case, from a drug) presented on keratinocytes can lead to a cytotoxic inflammatory response resulting in granulysin release, keratinocyte apoptosis and necrosis, detachment of the epidermis, and blister formation in SJS and TEN.
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever (often > 39°C)
KeratoconjunctivitisKeratoconjunctivitisSimultaneous inflammation of the cornea and conjunctiva.Stevens-Johnson Syndrome (inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the corneaCorneaThe transparent anterior portion of the fibrous coat of the eye consisting of five layers: stratified squamous corneal epithelium; bowman membrane; corneal stroma; descemet membrane; and mesenchymal corneal endothelium. It serves as the first refracting medium of the eye.Eye: Anatomy and conjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy)
Sore throatSore throatPharyngitis is an inflammation of the back of the throat (pharynx). Pharyngitis is usually caused by an upper respiratory tract infection, which is viral in most cases. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, and hoarseness.Pharyngitis
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
1‒3 days after the prodromeProdromeSymptoms that appear 24–48 hours prior to migraine onset.Migraine Headache
Lasts 8‒12 days
Cutaneous lesions:
Begin as ill-defined, coalescing macules with purpuric centers or diffuse erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion:
Start on the face and thorax, then spread symmetrically
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions begins to slough within days
Nikolsky signNikolsky SignDermatologic Examination: extensionExtensionExamination of the Upper Limbs of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions sloughing by applying pressure
Oral lesions from SJS seen in a patient on an antiretroviral medication (nevirapine).
Image: “Oral lesions associated with nevirapine-related Stevens Johnson syndrome: A report of four cases.” by lasundaram S, Ranganathan K, Umadevi K, Gunaseelan R, Kumaraswamy N, Solomon S, Devaleenol B, Ambrose P – Journal of oral and maxillofacial pathology : JOMFP (2011). License: CC BY 2.0
Characteristic lesions of SJS/TEN in a patient with accompanying erythema and sloughing.
Image: “Oral lesions associated with nevirapine-related Stevens Johnson syndrome: A report of four cases” by Balasundaram S, Ranganathan K, Umadevi K, Gunaseelan R, Kumaraswamy N, Solomon S, Devaleenol B, Ambrose P – Journal of oral and maxillofacial pathology : JOMFP (2011) . License: CC BY 2.0
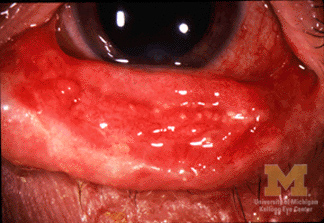
Keratoconjunctivitis in a patient with SJS/TEN.
Image: “Conjunctivitis in SJS” by Jonathan Trobe, M.D., University of Michigan Kellogg Eye Center. License: CC BY 3.0
Demonstration of Nikolsky’s sign by causing skin sloughing with the application of pressure.
Image: “Curcumin in stevens-johnsons syndrome: culprit or bystander?” by Irani C, Haddad F, Maalouly G, Nemnoum R. License: CC BY 2.0
Drug-induced toxic epidermal necrolysis with peeled skin over the back and buttocks.
Image: “Drug induced toxic epidermal necrolysis: two case reports” by Qadir SN, Raza N, Qadir F. License: CC BY 3.0
Photograph of a patient with widespread denudation of the epidermis in sheets, consistent with toxic epidermal necrolysis.
Image: “Review of Toxic Epidermal Necrolysis” by International Journal of Molecular Sciences. License: CC BY 4.0
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Bacterial infection:
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock and septic shockSeptic shockSepsis associated with hypotension or hypoperfusion despite adequate fluid resuscitation. Perfusion abnormalities may include, but are not limited to lactic acidosis; oliguria; or acute alteration in mental status.Sepsis and Septic Shock are the main cause of death in SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Most often caused by Staphylococcus aureusStaphylococcus aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Brain Abscessand Pseudomonas aeruginosaPseudomonas aeruginosaA species of gram-negative, aerobic, rod-shaped bacteria commonly isolated from clinical specimens (wound, burn, and urinary tract infections). It is also found widely distributed in soil and water. P. Aeruginosa is a major agent of nosocomial infection.Pseudomonas
Tracheobronchial epithelial involvement:
PneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
Acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS)
Protein loss: edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Electrolyte imbalances
Epithelial necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of the gastrointestinal tract:
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Colonic perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: AnatomyintussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
Diagnosis
The diagnosis is clinical, based on history and physical exam findings.
Apoptotic keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions are scattered in the basal layer of the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions in early lesions.
Full-thickness epidermal necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage and subepidermal bullaeBullaeErythema Multiforme later in the disease
Lymphocytic inflammatory infiltration
Direct immunofluorescence is negative.
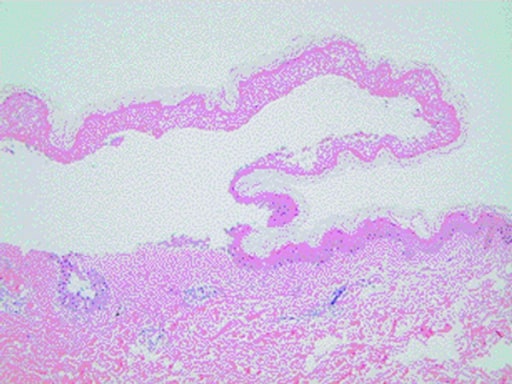
Histopathology of a skin biopsy taken from a patient with SJS/TEN showing characteristic epidermal detachment and lymphocyte infiltration in the dermis
Image: “Curcumin in stevens-johnsons syndrome: culprit or bystander?” by Irani C, Haddad F, Maalouly G, Nemnoum R. License: CC BY 2.0
Supporting workup[6,7,10]
The following studies aid in monitoring treatment and complications:
Basic metabolic panelBasic Metabolic PanelPrimary vs Secondary Headaches → evaluate for electrolyte imbalance and renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Complete blood count → significant leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus may signal an infection
Coagulation studiesCoagulation studiesCoagulation studies are a group of hematologic laboratory studies that reflect the function of blood vessels, platelets, and coagulation factors, which all interact with one another to achieve hemostasis. Coagulation studies are usually ordered to evaluate patients with bleeding or hypercoagulation disorders.Coagulation Studies
Bacterial and fungal culturesFungal culturesDermatophytes/Tinea Infections → bacterial superinfection and sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
MycoplasmaMycoplasmaMycoplasma is a species of pleomorphic bacteria that lack a cell wall, which makes them difficult to target with conventional antibiotics and causes them to not gram stain well. Mycoplasma bacteria commonly target the respiratory and urogenital epithelium. Mycoplasma pneumoniae (M. pneumoniae), the causative agent of atypical or “walking” pneumonia.Mycoplasma and chlamydiaChlamydiaChlamydiae are obligate intracellular gram-negative bacteria. They lack a peptidoglycan layer and are best visualized using Giemsa stain. The family of Chlamydiaceae comprises 3 pathogens that can infect humans: Chlamydia trachomatis, Chlamydia psittaci, and Chlamydia pneumoniae.ChlamydiaserologySerologyThe study of serum, especially of antigen-antibody reactions in vitro.Yellow Fever Virus → if an infectious cause is suspected
HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2 swab → if an infectious cause is suspected
Chest radiograph → pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia or interstitial pneumonitisPneumonitisHuman Herpesvirus 6 and 7
Management
Management may vary based on local protocols. The following recommendations are based on the most recent UK, European, and US guidelines.
General management
Withdrawal of causative agent is required.[5‒7]The treatment goal of SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN is supportive until the epidermal layer can be replaced and to prevent complications related to the lack of an epidermal barrier.
Management should be a multidisciplinary approach coordinated by a specialist in skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions failure.
Potential consultants:
Dermatology
Plastic surgeon
Burn surgeon
Critical care
Ophthalmology
Wound care nursing
Ensure:
Private room, controlled for humidity
Room temperature, 25‒28℃ (may also need body warmers)
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children ≥ 120/min
1
Serum ureaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea Cycle > 10 mmol/L
1
Serum glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance > 14 mmol/L
1
Serum bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes < 20 mmol/L
1
The SCORTEN scoreSCORTEN scoreStevens-Johnson Syndrome is used to help determine the severity, prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas, and appropriate setting for management in SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Score 0‒1: 94% survival, may be treated in non-specialized wards
Score 2: 87% survival, should be transferred to an intensive care unit, burn unitBurn unitSpecialized hospital facilities which provide intensive care for burn patients.Staphylococcal Scalded Skin Syndrome (SSSS), or specialized dermatology unit
Score 3: 53% survival, should be transferred to an intensive care unit, burn unitBurn unitSpecialized hospital facilities which provide intensive care for burn patients.Staphylococcal Scalded Skin Syndrome (SSSS), or specialized dermatology unit
Score 4: 25% survival, should be transferred to an intensive care unit, burn unitBurn unitSpecialized hospital facilities which provide intensive care for burn patients.Staphylococcal Scalded Skin Syndrome (SSSS), or specialized dermatology unit
Score 5‒7: 17% survival, should be transferred to an intensive care unit, burn unitBurn unitSpecialized hospital facilities which provide intensive care for burn patients.Staphylococcal Scalded Skin Syndrome (SSSS), or specialized dermatology unit
AirwayAirwayABCDE Assessment involvement is visualized on direct laryngoscopy (should be performed if patient is hypoxic, dyspneic, or tachypneic).
VentilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing management should follow ARDS guidelines.
Fluid and electrolyte management:[5‒7]
Encourage oral intake, if possible.
Obtain peripheral venous access through nonlesional skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.
Place urinary catheter to monitor urinary output → target 0.5‒1 mL/kg/hr
A target of 2 mL/kg/% BSA involved in the 1st 24 hrsHRSHepatorenal syndrome (HRS) is a potentially reversible cause of acute kidney injury that develops secondary to liver disease. The main cause of hrs is hypovolemia, often as a result of forced diuresis or drainage of ascites. This leads to renal vasoconstriction resulting in hypoperfusion of the kidneys.Hepatorenal Syndrome may be needed for adequate for fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome.[9]
Nutritional support:[5‒7]
Enteral feeding should be encouraged.
Place nasogastric tubeNasogastric tubeMalnutrition in children in resource-limited countries for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia and odynophagiaOdynophagiaEpiglottitis.
Caloric goal: 30‒35 kcal/kg/day
Parenteral nutritionParenteral nutritionThe administering of nutrients for assimilation and utilization by a patient who cannot maintain adequate nutrition by enteral feeding alone. Nutrients are administered by a route other than the alimentary canal (e.g., intravenously, subcutaneously).Central Venous Catheter for those whose enteral nutritionEnteral nutritionNutritional support given via the alimentary canal or any route connected to the gastrointestinal system (i.e., the enteral route). This includes oral feeding, sip feeding, and tube feeding using nasogastric, gastrostomy, and jejunostomy tubes.Short Bowel Syndrome is unable to meet daily caloric needs
Transition to oral feeding when tolerated.
Maintain tight glycemic control (serum glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance, 110‒180 mg/dL)
Topical steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors (potent or ultrapotent) ointment up to 4 times daily
Viscous lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics 2%, 15-mL swish and spit every 3 hours for painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
Topical corticosteroid may decrease ocular surface damage.
Antibiotic eyedrops should be considered with corneal involvement (seen on fluoresceinFluoresceinA phthalic indicator dye that appears yellow-green in normal tear film and bright green in a more alkaline medium such as the aqueous humor.Pseudomonas staining) or if frank ulcerationUlcerationCorneal Abrasions, Erosion, and Ulcers is present.
Coat urogenital skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions with ointment or ointment gauze.
An intravaginal lubricated moldMoldMycology or dilator can be placed to help treat vaginal disease (replace every 24 hours).
Topical lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics 5% can be applied at the vaginal introitus to help with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and help reduce discomfort due to vaginal dilators.
Petroleum jelly can be applied 2‒4 times daily as barrier protection.
Potent topical corticosteroidsCorticosteroidsChorioretinitis may be considered with involved, but not eroded, skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions; taper with clinical improvement.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control:[5,6]
Assess every 4 hours with validated painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways tool.
AcetaminophenAcetaminophenAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen for mild painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Patient-controlled analgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts with opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics for severe painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Adjuvants for opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics for sparing painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief:
GabapentinGabapentinA cyclohexane-gamma-aminobutyric acid derivative that is used for the treatment of partial seizures; neuralgia; and restless legs syndrome.Second-Generation Anticonvulsant Drugs/pregabalinPregabalinA gamma-aminobutyric acid (gaba) derivative that functions as a calcium channel blocker and is used as an anticonvulsant as well as an anti-anxiety agent. It is also used as an analgesic in the treatment of neuropathic pain and fibromyalgia.Second-Generation Anticonvulsant Drugs
Low-dose ketamineKetamineA cyclohexanone derivative used for induction of anesthesia. Its mechanism of action is not well understood, but ketamine can block NMDA receptors (n-methyl-d-aspartate receptors) and may interact with sigma receptors.Intravenous Anesthetics
Monitor for signs of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions infection
Bacterial and fungal culturesFungal culturesDermatophytes/Tinea Infections of blood, wounds, and mucosal lesions should be performed if there is suspicion of infection (routine cultures are not recommended).
Prophylactic antibiotics are not recommended.
Initiate appropriate antibiotics and antifungals only if:
Signs and symptoms of sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock are present OR
ProphylaxisProphylaxisCephalosporins with low-molecular-weight heparin is recommended (especially if the patient is immobile).
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with high bleeding risk should have graduated compressionCompressionBlunt Chest Trauma stockings or intermittent pneumatic devices in place.
LimitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation dressing changes.
Leave detached or detachable skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions in place to act as a biologic barrier.
Use an air bed to minimize potential shearing.
Gently cleanse lesional area with warmed sterileSterileBasic Procedures water, normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids, or dilute chlorhexidine solution (0.05%).
Lyse or drain wounds only for patient comfort.
Apply topical greasy emollientsEmollientsOleaginous substances used topically to soothe, soften or protect skin or mucous membranes. They are used also as vehicles for other dermatologic agents.Pityriasis Rosea to entire epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions → minimizes water loss:
Secondary absorptive dressing may be necessary to control exudateExudateExudates are fluids, cells, or other cellular substances that are slowly discharged from blood vessels usually from inflamed tissues.Pleural Effusion
Surgical debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome:[6,7]
Cleansing lesions with an antimicrobial agent under general anesthesiaGeneral anesthesiaProcedure in which patients are induced into an unconscious state through use of various medications so that they do not feel pain during surgery.Anesthesiology: History and Basic Concepts
Covering denuded dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions with a dressing:
Xenograft (pigskin)
Allograft (cadaveric skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions)
Synthetic dressing
Discharge[6]
Educate patient about future drug avoidance, including closely related agents.
Document the causative drug in the patient’s chart.
Notify patient’s outpatient care team.
Follow-up appointment with a dermatologist and ophthalmologist (if ocular involvement) should be scheduled.
Notify patient that they may experience fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia for several weeks.
Controversial treatments[6,7]
CyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants
PlasmapheresisPlasmapheresisProcedure whereby plasma is separated and extracted from anticoagulated whole blood and the red cells retransfused to the donor. Plasmapheresis is also employed for therapeutic use.Stevens-Johnson Syndrome
TumorTumorInflammationnecrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage factor (TNFTNFTumor necrosis factor (TNF) is a major cytokine, released primarily by macrophages in response to stimuli. The presence of microbial products and dead cells and injury are among the stimulating factors. This protein belongs to the TNF superfamily, a group of ligands and receptors performing functions in inflammatory response, morphogenesis, and cell proliferation. Tumor Necrosis Factor (TNF)) inhibitors
Granulocyte colony-stimulating factorGranulocyte colony-stimulating factorA glycoprotein of mw 25 kda containing internal disulfide bonds. It induces the survival, proliferation, and differentiation of neutrophilic granulocyte precursor cells and functionally activates mature blood neutrophils. Among the family of colony-stimulating factors, G-CSF is the most potent inducer of terminal differentiation to granulocytes and macrophages of leukemic myeloid cell lines.White Myeloid Cells: Histology (for acquired neutropeniaAcquired NeutropeniaNeutropenia)
Differential Diagnosis
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme: an acute, immune-mediated skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions eruption with typical targetoid lesions; may be accompanied by systemic symptoms and mucosal involvement. Etiology is usually due to infection from the herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology, unlike SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN, which is usually caused by a medication. Diagnosis is clinical and will differentiate this condition from SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome. Treatment includes supportive care.
Staphylococcal scalded skin syndromeStaphylococcal Scalded Skin SyndromeStaphylococcal scalded skin syndrome (SSSS), also known as Ritter disease and staphylococcal epidermal necrolysis, is a toxin-mediated condition caused by Staphylococcus aureus. The exfoliative toxin produced disseminates and cleaves desmoglein 1 in the epidermis, causing separation and detachment of the skin. Staphylococcal Scalded Skin Syndrome (SSSS)(SSSSSSSSStaphylococcal scalded skin syndrome (SSSS), also known as Ritter disease and staphylococcal epidermal necrolysis, is a toxin-mediated condition caused by Staphylococcus aureus. The exfoliative toxin produced disseminates and cleaves desmoglein 1 in the epidermis, causing separation and detachment of the skin. Staphylococcal Scalded Skin Syndrome (SSSS)): presents with a painful, desquamative skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsrashRashRocky Mountain Spotted Fever, especially around the noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal), mouth, and anus. The condition results from a staphylococcal toxin and is usually seen in children. Unlike SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN, there is no mucosal involvement. Diagnosis is clinical and confirmed with bacterial cultures. A biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma will show noninflammatory, superficial splittingSplittingDefense Mechanisms of the epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions. Treatment includes antibiotics, wound care, and supportive care.
Exfoliative dermatitisDermatitisAny inflammation of the skin.Atopic Dermatitis (Eczema): a generalized, symmetric, erythematous rashRashRocky Mountain Spotted Fever caused by an underlying cutaneous disease (psoriasisPsoriasisPsoriasis is a common T-cell-mediated inflammatory skin condition. The etiology is unknown, but is thought to be due to genetic inheritance and environmental triggers. There are 4 major subtypes, with the most common form being chronic plaque psoriasis. Psoriasis, atopic dermatitisDermatitisAny inflammation of the skin.Atopic Dermatitis (Eczema)), medications, and malignancyMalignancyHemothorax (lymphomaLymphomaA general term for various neoplastic diseases of the lymphoid tissue.Imaging of the Mediastinum). The condition can mimic the early stages of SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome; however, there is no mucosal involvement (which will differentiate the condition from SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome). Diagnosis is made clinically, and treatment focuses on treating the underlying cause, withdrawal of implicated medications, and supportive care.
Toxic shock syndromeToxic Shock SyndromeToxic shock syndrome (TSS) is an acute, multi-systemic disease caused by the toxin-producing bacteria, Staphylococcus aureus and Streptococcus pyogenes. Staphylococcal TSS is more common and associated with tampons and nasal packing. Toxic Shock Syndrome: a systemic syndrome caused by staphylococcusStaphylococcusStaphylococcus is a medically important genera of Gram-positive, aerobic cocci. These bacteria form clusters resembling grapes on culture plates. Staphylococci are ubiquitous for humans, and many strains compose the normal skin flora.Staphylococcus or streptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.StreptococcusendotoxinsEndotoxinsToxins closely associated with the living cytoplasm or cell wall of certain microorganisms, which do not readily diffuse into the culture medium, but are released upon lysis of the cells.Bacteriology. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock, and multisystem organ dysfunction. Cutaneous manifestations include a diffuse, erythematous rashRashRocky Mountain Spotted Fever and desquamationDesquamationStaphylococcal Scalded Skin Syndrome (SSSS). Diagnosis is based on blood culture results, clinical history, and exam, which will differentiate this condition from SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome. Treatment includes hemodynamic support, fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome, and antibiotics.
Pemphigus vulgarisPemphigus vulgarisBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In pemphigus vulgaris, autoantibodies attack the desmosomal proteins, which connect the keratinocytes to one another. This attack results in a more severe, potentially fatal condition with fragile, flaccid blisters, usually with significant mucosal involvement. Bullous Pemphigoid and Pemphigus Vulgaris: an autoimmune disorderAutoimmune DisorderSeptic Arthritis causing intraepidermal blistering and erosionsErosionsCorneal Abrasions, Erosion, and Ulcers of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and mucous membranes. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will have cutaneous bullaeBullaeErythema Multiforme appearing on normal-appearing skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and painful mucocutaneous erosionsErosionsCorneal Abrasions, Erosion, and Ulcers. Diagnosis involves a biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma with immunofluorescence testing showing immunoglobulin G (IgGIgGThe major immunoglobulin isotype class in normal human serum. There are several isotype subclasses of igg, for example, igg1, igg2a, and igg2b.Hypersensitivity Pneumonitis) antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against keratinocytesKeratinocytesEpidermal cells which synthesize keratin and undergo characteristic changes as they move upward from the basal layers of the epidermis to the cornified (horny) layer of the skin. Successive stages of differentiation of the keratinocytes forming the epidermal layers are basal cell, spinous or prickle cell, and the granular cell.Skin: Structure and Functions, differentiating this condition from SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome. Treatment includes corticosteroidsCorticosteroidsChorioretinitis, immunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants, and IVIGIVIGDermatomyositis.
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris: an autoimmune skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions disorder causing pruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema), erythematous plaques, and tense, bullous lesions. Mucous membraneMucous membraneAn epithelium with mucus-secreting cells, such as goblet cells. It forms the lining of many body cavities, such as the digestive tract, the respiratory tract, and the reproductive tract. Mucosa, rich in blood and lymph vessels, comprises an inner epithelium, a middle layer (lamina propria) of loose connective tissue, and an outer layer (muscularis mucosae) of smooth muscle cells that separates the mucosa from submucosa.Barrett Esophagus involvement is rare. Triggers include medications, trauma, skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions conditions, and systemic disease. BiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma with immunofluorescence shows IgGIgGThe major immunoglobulin isotype class in normal human serum. There are several isotype subclasses of igg, for example, igg1, igg2a, and igg2b.Hypersensitivity Pneumonitis and complement deposits along the basement membraneBasement membraneA darkly stained mat-like extracellular matrix (ecm) that separates cell layers, such as epithelium from endothelium or a layer of connective tissue. The ecm layer that supports an overlying epithelium or endothelium is called basal lamina. Basement membrane (bm) can be formed by the fusion of either two adjacent basal laminae or a basal lamina with an adjacent reticular lamina of connective tissue. Bm, composed mainly of type IV collagen; glycoprotein laminin; and proteoglycan, provides barriers as well as channels between interacting cell layers.Thin Basement Membrane Nephropathy (TBMN), which differentiates the condition from SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome. Treatment includes steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors, immunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants, and anti-inflammatory medications.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome (SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome), Toxic Epidermal NecrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome (TEN), and the overlap between them. These are severe, life-threatening skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions reactions, often triggered by medications.
Coding System
Code
Description
ICD-10-CM
L51.1
Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome (SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome)
This CPT code is for a skin biopsySkin BiopsySecondary Skin Lesions, which is the definitive test to confirm the diagnosis by showing full-thickness epidermal necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, distinguishing SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN from other skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions conditions.
Coding System
Code
Description
CPT
11102
Tangential biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions (eg, shave, scoop, saucerize, curette); single lesion
Procedures/Interventions:
This code represents admission to a critical care unit, as patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome/TEN require intensive supportive care similar to that of a burn patient, including fluid management, wound care, and nutritional support.
Coding System
Code
Description
CPT
99291
Critical care, evaluation and management of the critically ill or critically injured patient; first 30-74 minutes
Seminario-Vidal, L., Kroshinsky, D., Malachowski, S. J., et al.(2020). Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. Journal of the American Academy of Dermatology, 82(6), 1553–1567. https://doi.org/10.1016/j.jaad.2020.02.066
Creamer, D., Walsh, S. A., Dziewulski, P., et al. (2016). U.K. guidelines for the management of Stevens–Johnson syndrome/toxic epidermal necrolysis in adults 2016. British Journal of Dermatology, 174(6), 1194–1227. https://doi.org/10.1111/bjd.14530
McPherson, T., Exton, L. S., Biswas, S., et al. (2019). British Association of Dermatologists’ guidelines for the management of Stevens–Johnson syndrome/toxic epidermal necrolysis in children and young people, 2018. British Journal of Dermatology, 181(1), 37–54. https://doi.org/10.1111/bjd.17841
Shiga, S., Cartotto, R. (2010). What are the fluid requirements in toxic epidermal necrolysis? Journal of Burn Care & Research, 31(1), 100–104. https://doi.org/10.1097/BCR.0b013e3181cb8cb8
Guegan, S., et al. (2006). Performance of the SCORTEN during the first five days of hospitalization to predict the prognosis of epidermal necrolysis. Journal of Investigative Dermatology, 126(2), 272–276. https://www.jidonline.org/article/S0022-202X(15)32753-6/fulltext
Create your free account or log in to continue reading!