Small bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine; it is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is postsurgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. The diagnosis is established via imaging. Up to 80% of all cases will resolve with supportive management (bowel rest, intravenous (IV) hydration, and nasogastric decompression). However, surgery is required for persistent or complicated cases.
Small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis (SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction) is the interruption of the flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of intraluminal contents through the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy (duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy, jejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy, or ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy).
Epidemiology[1]
Average age of onset is 64 years.
Similar incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in men and women
Accounts for 2%–4% of emergency department visits in the United States
Constitutes 80% of mechanical intestinal obstructions
Etiology[3,6,7]
Mechanical:
Adhesions (postsurgical):
Most common cause in the Western countries
Open surgery: Prior open abdominal surgery significantly increases lifetime risk of adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction (estimated 5%–20%, depending on procedure), with lower risk observed after laparoscopic approaches.
Tumors
Hernias:
External hernias: noted in sites of abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen weakness
Internal hernias: noted in congenital/acquired mesenteric defects or from surgeries such as Roux-en-Y gastric bypassGastric bypassSurgical procedure in which the stomach is transected high on the body. The resulting small proximal gastric pouch is joined to any parts of the small intestine by an end-to-side surgical anastomosis, depending on the amounts of intestinal surface being bypasses. This procedure is used frequently in the treatment of morbid obesity by limiting the size of functional stomach, food intake, and food absorption.Gastroesophageal Reflux Disease (GERD)
Crohn’s disease (inflammatory strictures or adhesions)
GallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis (gallstone ileusGallstone IleusCholelithiasis)
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
PeritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
Serious intra-abdominal infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease and/or inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation:
Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis
Pelvic inflammatory diseasePelvic inflammatory diseasePelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and Gardnerella vaginalis. Pelvic Inflammatory Disease
Trauma
Intestinal ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
Medications (opiatesOpiatesOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates.Opioid Analgesics, calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes channel blockers, diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication)
Electrolyte imbalance
Mnemonics
3 most common causes of SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction: ABC
Adhesions
Bulge (hernias)
Cancer (neoplasm)
Causes of SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction: SHAVING
Mechanical: results from intrinsic (tumors) or extrinsic(adhesions, hernias) compressionCompressionBlunt Chest Trauma
Functional (ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction):
Results from impaired motilityMotilityThe motor activity of the gastrointestinal tract.Gastrointestinal Motility (non-mechanical cause of bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis symptoms)
Can be limited to the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy or include the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy as well
By degree of obstruction:
Complete: no passage of luminal contents beyond the obstruction point
Partial: Some intestinal contents pass through.
Closed loop:
Segment of intestine is obstructed proximally and distally.
Seen in volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
IschemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage, necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, and perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis can develop rapidly.
By associated complication:
Simple: obstruction without ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
Complicated: CirculationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment is compromised, with associated ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage, infarction, and/or perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
Pathophysiology[1,3,10]
Early:
Intrinsic obstruction or extrinsic compressionCompressionBlunt Chest Trauma causes interrupted flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of bowel contents, leading to:
Increased migrating clustered contractions (MCCs) proximal to the obstruction → abdominal crampsCrampsIon Channel Myopathy
Accumulation of swallowed air and gas from bacterial fermentation
Loss of normal intestinal absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption (including water)
Emesis leads to loss of fluid and electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes (Na+, K+, H+, Cl–) → hypovolemiaHypovolemiaSepsis in Children and metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis follow
Late:
Luminal flora changes → bacterial breakdown of stagnant contents results in feculent fluid
Persistent edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema of the bowel wall → bowel ischemiaBowel ischemiaMesenteric ischemia is a rare, life-threatening condition caused by inadequate blood flow through the mesenteric vessels, which results in ischemia and necrosis of the intestinal wall. Mesenteric ischemia can be either acute or chronic.Mesenteric Ischemia from compressionCompressionBlunt Chest Trauma of intramural vesselsIntramural vesselsLarge Bowel Obstruction
With ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage → lactic acid accumulates → metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Ischemic bowel can lead to gut translocation of bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology, necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, and perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
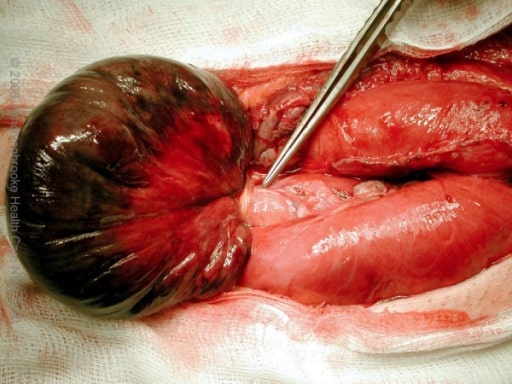
Gangrenous small bowel with closed-loop obstruction caused by an omental band adhesion
Image: “Intra-operative photograph” by the Department of Surgery, Hinchingbrooke Hospital, Hinchingbrooke Healthcare NHS Trust, Huntingdon, Cambridgeshire, UK. License: CC BY 2.0.
Can be temporarily relieved by vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Severe constant painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways may indicate ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage or perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and biliousvomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Proximal SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction → early, frequent vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Distal SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction → later vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, more distention
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Intermittent nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
May not have nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics or vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Physical examination[1,7]
Signs of dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration (hallmark of SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction):
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (orthostatic)
High-pitched bowel sounds (early SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction)
Decreased/absent bowel sounds (late SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction or adynamic ileusAdynamic ileusSmall Bowel Obstruction)
PercussionPercussionAct of striking a part with short, sharp blows as an aid in diagnosing the condition beneath the sound obtained.Pulmonary Examination: tympany or hyper-resonanceHyper-ResonancePneumothorax; dullness if fluid filled
PalpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination:
Look for hernias and masses.
Tenderness on minimal palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination, rebound, and/or guarding indicates possible peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury (indicative of complications such as ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage or perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis).
Digital rectal exam:
To rule out fecal impaction as a cause of symptoms
Presence of blood would raise suspicion for a tumorTumorInflammation/malignancyMalignancyHemothorax, ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage, or inflammatory pathology.
Diagnosis
History[1,7]
Risk factors for adhesions:
Prior abdominal surgeries (most important): ↑ risk of adhesions
Inflammatory conditions (Crohn’s disease, diverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease)
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma exposure
Other risk factors for mechanical SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction:
Risk factors for functional SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction:
Medications
Acute or chronic systemic illness (i.e. pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
Acute intra-abdominal infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Abdominal trauma
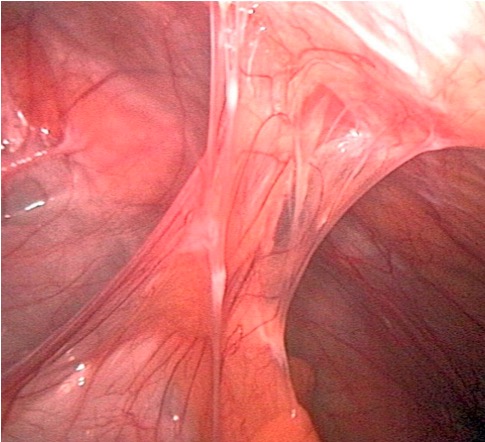
Adhesions that can develop after surgery are the most common cause of bowel obstruction
Image by Kevin Pei, PD.
Laboratory tests
Minimum lab tests to order when SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction is suspected:[13]
CBC
ElectrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes with BUN/creatinine
Lactate
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test in women of reproductive age
Findings consistent with SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction:[6]
Electrolyte abnormalities (commonly seen in acute onset due to vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and dehydrationDehydrationThe condition that results from excessive loss of water from a living organism.Volume Depletion and Dehydration):
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
High blood ureaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea CyclenitrogenNitrogenAn element with the atomic symbol n, atomic number 7, and atomic weight [14. 00643; 14. 00728]. Nitrogen exists as a diatomic gas and makes up about 78% of the earth’s atmosphere by volume. It is a constituent of proteins and nucleic acids and found in all living cells.Urea Cycle (BUN)/creatinine
Metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis from vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia (high bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes)
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis at late stages
AnemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types: if with associated etiology (Crohn’s, cancer)
Other:
Lactate: Elevated lactate suggests bowel ischemiaBowel ischemiaMesenteric ischemia is a rare, life-threatening condition caused by inadequate blood flow through the mesenteric vessels, which results in ischemia and necrosis of the intestinal wall. Mesenteric ischemia can be either acute or chronic.Mesenteric Ischemia or hypoperfusion.
C-reactive protein (CRP) correlates with inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation severity (> 75 may indicate peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury). [13]
Blood cultures: in the setting of bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides
Imaging studies[1,3,6–9,12,13]
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests:
Often obtained first (wide availability, low cost, low exposure to radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma)
Abdominal X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests performed in supine and upright or lateral decubitus positions
Performed with upright chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
Air–fluid levels (with stacked small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy loops) in upright films (stepladder signStepladder signSmall Bowel Obstruction)
Paucity of air in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Gasless abdomenGasless AbdomenPediatric Gastrointestinal Abnormalities (if all the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy loops are filled with fluid)
IleusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction: can show diffuse small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy and colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy dilatation
Free air in case of perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis (under the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy) → an indication for immediate surgical intervention
An X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests can be used to diagnose SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction in > 60% of cases,[3,6] but:
Etiology of the obstruction cannot be determined.
Imaging may be normal in early or proximal obstruction.
Computed tomography (CT) scan:
Recommended in all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship when acute SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction is suspected[6,8]
Intravenous (IV) contrast recommended (for signs of inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation, ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage)
Oral contrast is not necessary if high-grade or complete obstruction is suspected.
Helps identify:
Site of obstruction
Etiology (e.g., herniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias, volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus, tumorTumorInflammation)
Severity (must exclude bowel compromise)
SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction findings:
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy has little gas or fluid.
Signs of bowel compromise (which are indications for immediate surgical intervention):
Closed-loop obstruction findings:
U-shaped or C-shaped dilated bowel loop
Mesenteric vessels converging toward a torsion point (CT whirl signWhirl signVolvulus)
2 collapsed bowel loops adjacent to the obstruction
PneumoperitoneumPneumoperitoneumA condition with trapped gas or air in the peritoneal cavity, usually secondary to perforation of the internal organs such as the lung and the gastrointestinal tract, or to recent surgery. Pneumoperitoneum may be purposely introduced to aid radiological examination.Perforated Viscus (indicative of perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis):
Free air over the spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy or liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
Free air adjacent to the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (retroperitoneum)
“Football signFootball signOutlining the whole abdomen by gasImaging of the Intestines” (gas from the perforated bowel surrounds the abdominal cavity): supine CT
Pneumatosis intestinalisPneumatosis intestinalisA condition characterized by the presence of multiple gas-filled cysts in the intestinal wall, the submucosa and/or subserosa of the intestine. The majority of the cysts are found in the jejunum and the ileum.Necrotizing Enterocolitis (air in the bowel wall)
Mesenteric haziness or edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema (mesenteric stranding)
IV contrast has poor uptake into the wall of the affected bowel.
AscitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites
GastrografinGastrografinComputed Tomography (CT) (water-soluble contrast) is used in case perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis exists. Use with caution (aspiration risk).
Serial abdominal radiographic images are taken, tracking the movement of contrast through the GI tract.
Generally inferior to a CT scan in acute settings but helpful in partial SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Exclusions:
Complete or closed-loop obstructions
Bowel ischemiaBowel ischemiaMesenteric ischemia is a rare, life-threatening condition caused by inadequate blood flow through the mesenteric vessels, which results in ischemia and necrosis of the intestinal wall. Mesenteric ischemia can be either acute or chronic.Mesenteric Ischemia, necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, or perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Because of its iodineIodineA nonmetallic element of the halogen group that is represented by the atomic symbol I, atomic number 53, and atomic weight of 126. 90. It is a nutritionally essential element, especially important in thyroid hormone synthesis. In solution, it has anti-infective properties and is used topically.Thyroid Hormones component, gastrografinGastrografinComputed Tomography (CT) is contraindicated in hyperthyroidismHyperthyroidismHypersecretion of thyroid hormones from the thyroid gland. Elevated levels of thyroid hormones increase basal metabolic rate.Thyrotoxicosis and Hyperthyroidism.
Radiograph obtained 24 hours after administration: If the contrast agent reaches the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy, SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction is likely resolving without surgery.
Used as therapeutic agent in adhesive mechanical SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction: HypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water RegulationgastrografinGastrografinComputed Tomography (CT) reduces intestinal wall edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, thus helping peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility.
Speeds up resolution of adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction in cases that would have resolved without surgical correction (i.e., does not improve success rate of nonoperative management)
Decreases length of hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
Less effective in those with SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction from recent abdominal surgery (< 6 weeks)
Magnetic resonance imaging (MRI): if CT is contraindicated (children, pregnant women)
Bedside imaging (abdominal US):
Utilized in those with contrast allergiesAllergiesA medical specialty concerned with the hypersensitivity of the individual to foreign substances and protection from the resultant infection or disorder.Selective IgA Deficiency (cannot undergo CT scanning) and in those who are pregnant
Easily accessible; thus can be used in the ED or in critical care at the bedside to evaluate abdominal painAbdominal PainAcute Abdomen
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
Pelvic disease
GallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy disease
X-ray showing intestinal loops with air-fluid levels consistent with SBO
Image: “X-ray” by the Department of Surgery, University Hospital of Ioannina, Greece. License: CC BY 2.0.
Abdominal X-ray showing dilated small bowel loops consistent with SBO
Image: “Abdominal X-ray” by the Department of General Surgery, Sunderland Royal Hospital, Kayll Road, Sunderland SR4 7TP, UK. License: CC BY 2.0.
A CT scan showing the transition zone (arrow) with proximal bowel dilation and distal bowel decompression
Image: “Abdominal CT Scan” by the 2nd Department of Surgery, Athens University School of Medicine, Aretaieion Hospital, Athens, Greece. License: CC BY 2.0.
A CT scan showing a hernia causing a small obstruction with air-fluid levels
Image: “Abdominal CT scan” by the Service des Urgences Chirurgicales Viscérales, Centre Hospitalier Universitaire Ibn Rochd, Casablanca, Morocco. License: CC BY 2.0.
Diagnosing adhesive versus nonadhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction[1]
Adhesions form because of prior abdominal surgeries or previous abdominal inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation (e.g., pelvic inflammatory diseasePelvic inflammatory diseasePelvic inflammatory disease (PID) is defined as a polymicrobial infection of the upper female reproductive system. The disease can affect the uterus, fallopian tubes, ovaries, and adjacent structures. Pelvic inflammatory disease is closely linked with sexually transmitted diseases, most commonly caused by Chlamydia trachomatis, Neisseria gonorrhoeae, and Gardnerella vaginalis. Pelvic Inflammatory Disease, acute appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis).
Adhesions cannot be seen on imaging.
Etiologies of nonadhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction typically can be seen on imaging.
Therefore, diagnosis of adhesive versus nonadhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction can typically be made by combining history and imaging.
Note: Adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction is more common in developed countries.
Severity assessment[1]
The American Association for the Surgery of Trauma (AAST) has developed gradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis criteria for SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction.
A higher grade means:
More critical care services are needed.
Longer hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium is expected.
Increased complications
Table: AAST GradingGradingMethods which attempt to express in replicable terms the level of cell differentiation in neoplasms as increasing anaplasia correlates with the aggressiveness of the neoplasm.Grading, Staging, and Metastasis Criteria for SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Grade
Description
Radiographic
Operative criteria
I
Partial SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Minimal bowel distention
Minimal bowel distention with no evidence of obstruction
II
Complete SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with viable bowel (not compromised)
Bowel distention with transition point without bowel compromise
Bowel distention with transition point without bowel compromise
III
Complete SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with compromised but viable bowel
Bowel distention with transition point associated with impending bowel compromise, complete obstruction, and/or no distal contrast flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure
Bowel distention with impending bowel compromise
IV
Complete SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with:
Nonviable bowel
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis (local spillage)
Complete SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with:
Nonviable bowel
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis (local spillage)
Bowel distention with localized perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis or free fluid
V
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis with diffuse peritoneal contamination
Bowel perforationBowel perforationPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall.Perforated Viscus with free air and free fluid
Bowel distention with perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, free fluid, and evidence of diffuse peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
General diagnostic checklist for initial assessment[1–3,6-11,13]
Check for symptoms of SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction: abdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and (bilious) vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation/obstipationObstipationLarge Bowel Obstruction
Medical and surgical history
Exam findings consistent with SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Testing to rule out other causes of abdominal/pelvic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways: e.g., urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children, lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion, pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care test if indicated
Imaging:
Upright chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests and supine abdominal X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
CT of the abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy with IV contrast (without oral contrast)
EMERGENT surgical consult if patient has hemodynamic instability, peritoneal signs and/or signs of bowel compromise (free air, pneumatosis on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests)
Indicated in suspected adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Check for contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation for gastrografinGastrografinComputed Tomography (CT): pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care, abdominal surgery in the past 6 weeks (in those with contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation, proceed with medical management)
Abdominal X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests in 6–24 hours:
Contrast in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy → resolving SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction, continue with medical management
Without contrast in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy → SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction is not resolving; may influence the decision to operate
Involve other services as indicated (e.g., surgery, gastroenterology, oncology)
Management and Prognosis
The general principles of diagnostic evaluation are summarized below from US sources. Additional international recommendations can be reviewed from the World Society of Emergency Surgery.
Medical management[2,3,6–8,10]
For both adhesive and nonadhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction, without indications for immediate surgery
Management needed for ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction (functional SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction)
75%–80% of adhesive mechanical SBOs resolve with medical management alone:
Correction of electrolyte abnormalities (caution with potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia supplementation in case of acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury)
Not warranted in uncomplicated SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Given in bowel compromise and as a standard prophylaxisProphylaxisCephalosporins in cases where surgery is anticipated
Administered if etiology is an infectious cause
GastrografinGastrografinComputed Tomography (CT) challenge in cases of adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction (Passage of contrast to the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy within 24 hours predicts successful nonoperative resolution.)
Duration of medical management:
Up to 3 days, with plans for surgery if:[13]
Patient’s condition clinically deteriorates
SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction persists longer than 3–5 days despite treatment
For SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction associated with recent abdominal surgery (≤ 6 weeks):
Nonoperative treatment is usually longer (dense adhesions from recent operation will make surgery difficult).
Parenteral nutritionParenteral nutritionThe administering of nutrients for assimilation and utilization by a patient who cannot maintain adequate nutrition by enteral feeding alone. Nutrients are administered by a route other than the alimentary canal (e.g., intravenously, subcutaneously).Central Venous Catheter is given in these cases.
For older adults, earlier intervention (if no improvement is seen) is associated with decreased mortalityMortalityAll deaths reported in a given population.Measures of Health Status.
Factors that predict eventual need for bowel resection after nonoperative management (≥ 3 highly predicts surgery):
Guarding on exam
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways > 4 days
> 500 mL free intra-abdominal fluid on CT
Decreased wall contrast enhancement on CT
CRP > 75 mg/L
WBC > 10
Surgery[3,6–8,13]
Emergent:
Closed-loop obstruction
Intestinal ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage/necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
HerniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception/volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
For failure of medical management:
If SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction does not resolve in 3–5 days, on average
At any point if the patient shows clinical deterioration
Procedures (depend on specific etiologies):
Lysis of adhesions
HerniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias repair
Small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy resection:
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Crohn’s disease
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
< 5% perioperative mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate for non-strangulating SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Higher perioperative mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate for strangulating or complicated SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction has a risk of recurrence after both operative and nonoperative management. Surgical intervention may reduce short-term recurrence but may increase long-term adhesionAdhesionThe process whereby platelets adhere to something other than platelets, e.g., collagen; basement membrane; microfibrils; or other ‘foreign’ surfaces.Coagulation Studies formation.
General management checklist[2,3,6–8,10,13]
Indications for surgery:
SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with bowel compromise (ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage, necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis) → immediate/emergent surgery
SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction with surgically correctable causes (except adhesions) → urgent surgery:
Closed-loop obstruction
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
IntussusceptionIntussusceptionIntussusception occurs when a part of the intestine (intussusceptum) telescopes into another part (intussuscipiens) of the intestine. The condition can cause obstruction and, if untreated, progress to bowel ischemia. Intussusception is most common in the pediatric population, but is occasionally encountered in adults. Intussusception
Small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: AnatomytumorTumorInflammation (localized)
History of Roux-en-Y gastric bypassGastric bypassSurgical procedure in which the stomach is transected high on the body. The resulting small proximal gastric pouch is joined to any parts of the small intestine by an end-to-side surgical anastomosis, depending on the amounts of intestinal surface being bypasses. This procedure is used frequently in the treatment of morbid obesity by limiting the size of functional stomach, food intake, and food absorption.Gastroesophageal Reflux Disease (GERD) (↑ risk of internal herniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias)
Initial medical management:
Nothing by mouth
IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids
NG decompression (can be placed on suction if recommended by the surgical team)
Electrolyte monitoring and correction
Minimize opioidOpioidCompounds with activity like opiate alkaloids, acting at opioid receptors. Properties include induction of analgesia or narcosis.Constipation use
AntiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics as needed
Serial abdominal exams
Urine output monitoring (Foley catheter can be placed)
IV antibiotics if indicated
GastrografinGastrografinComputed Tomography (CT) challenge (if no contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation) for adhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Targeted treatment for nonadhesive SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction
Monitor response to treatment and progression of symptoms; look for:
↓ NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
↓ NG output
Passing flatus
If worsening (↑ abdominal painAbdominal PainAcute Abdomen, sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, bowel compromise) → surgery
Signs of improvement over the next 24–48 hours:
May remove NGT
Advance the diet
No signs of improvement over the next 24–48 hours:
Continue nothing-by-mouth status and NG decompression
Consider additional imaging
Consult surgery and assess surgical candidacy
Typical wait for improvement is over 3–5 days, then consider surgery if SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction persists.
Irritable bowel syndromeIrritable bowel syndromeIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome (IBSIBSIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome): a functional bowel disorder without a clear anatomic abnormality.Irritable bowel syndromeIrritable bowel syndromeIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome can present with abdominal painAbdominal PainAcute Abdomen and constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, but the sudden onset of symptoms is not a feature of IBSIBSIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome. Imaging and laboratory tests are usually normal in IBSIBSIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome.
GastroenteritisGastroenteritisGastroenteritis is inflammation of the stomach and intestines, commonly caused by infections from bacteria, viruses, or parasites. Transmission may be foodborne, fecal-oral, or through animal contact. Common clinical features include abdominal pain, diarrhea, vomiting, fever, and dehydration.Gastroenteritis: an acute self-limited illness usually caused by a virusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology.GastroenteritisGastroenteritisGastroenteritis is inflammation of the stomach and intestines, commonly caused by infections from bacteria, viruses, or parasites. Transmission may be foodborne, fecal-oral, or through animal contact. Common clinical features include abdominal pain, diarrhea, vomiting, fever, and dehydration.Gastroenteritis can also present with crampy abdominal painAbdominal PainAcute Abdomen, but the typical presentation also involves diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea (watery or bloody), which is infrequent with acute SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction.
Peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease (PUDPUDPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease): mucosal ulcerationUlcerationCorneal Abrasions, Erosion, and Ulcers of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy or duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy. Peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease presents with upper abdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease is typically not associated with distention and constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation. VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia is usually non-bilious.
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy. Early appendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis can present with diffuse colicky painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, but painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and tenderness eventually localize to the right lower quadrantRight lower quadrantAnterior Abdominal Wall: Anatomy. Diagnosis is established by a CT scan.
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy. PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis presents with epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear), nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Blood work will show elevated amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption/lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion. A CT scan may show pancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation.
DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the colonic diverticula. DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease presents with crampy lower abdominal painAbdominal PainAcute Abdomen, many times with constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation. DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease frequently is also associated with feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever and leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus. A CT scan shows the characteristic findings.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose a small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis (SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction), a blockage in the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy. The codes can further specify the cause, such as adhesions or herniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias.
Coding System
Code
Description
ICD-10-CM
K56.609
Unspecified intestinal obstructionIntestinal obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis, unspecified as to partial versus complete obstruction
ICD-10-CM
K56.50
Intestinal adhesions [bands] with obstruction (postprocedural) (postinfection)
Evaluation & Workup:
These codes are for the imaging studies used to diagnose an SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction. An abdominal X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests may show dilated loops of small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy and air-fluid levels, while a CT scan can better define the location and cause of the obstruction.
Coding System
Code
Description
CPT
74022
Radiologic examination, abdomen; 2 views
CPT
74177
Computed tomography, abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy; with contrast material(s)
Procedures/Interventions:
This code is for the placement of a nasogastric (NG) tube for decompression, a primary non-operative management for SBOSBOSmall bowel obstruction (SBO) is an interruption of the flow of the intraluminal contents through the small intestine, and is classified as mechanical (due to physical blockage) or functional (due to disruption of normal motility). The most common cause of SBO in the Western countries is post-surgical adhesions. Small bowel obstruction typically presents with nausea, vomiting, abdominal pain, distention, constipation, and/or obstipation. Small Bowel Obstruction. Surgical intervention, such as lysis of adhesions, may be required if conservative management fails.
Coding System
Code
Description
CPT
44005
Enterolysis (freeing of intestinal adhesionAdhesionThe process whereby platelets adhere to something other than platelets, e.g., collagen; basement membrane; microfibrils; or other ‘foreign’ surfaces.Coagulation Studies) (separate procedure)
Kulaylat, M. N., Doerr, R. J., Holzheimer, R. G., Mannick, J. A. (Eds.) (2001) Small bowel obstruction. In Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt. https://www.ncbi.nlm.nih.gov/books/NBK6873/
Tavakkoli, A., Ashley, S. W., Zinner, M. J. (2019). Small intestine. In Brunicardi, F., Andersen, D. K., Billiar, T. R., Dunn, D. L., Kao, L. S., Hunter, J. G., Matthews, J. B., Pollock, R. E. (Eds.), Schwartz’s Principles of Surgery (11th ed.). McGraw-Hill.
Vercruysse, G., Busch, R., Dimcheff, D., et al. (2021). Evaluation and management of mechanical small bowel obstruction in adults. Ann Arbor (MI): Michigan Medicine, University of Michigan. https://www.ncbi.nlm.nih.gov/books/NBK572336/
Maung, A. A., Johnson, D. C., Piper, G. L., Barbosa, R. R., Rowell, S. E., Bokhari, F., Collins, J. N., Gordon, J. R., Ra, J. H., Kerwin, A. J. (2012). Evaluation and management of small-bowel obstruction, Journal of Trauma and Acute Care Surgery, 73(5), S362–S369.
Choi, H. K., Chu, K. W., Law, W. L. (2002). Therapeutic value of Gastrografin in adhesive small bowel obstruction after unsuccessful conservative treatment: a prospective randomized trial. Annals of Surgery, 236(1), 1–6. https://doi.org/10.1097/00000658-200207000-00002
Cohen, R. B., Olafson, S. N., Krupp, J., Parsikia, A., Kaplan, M. J., Moran, B., Leung, P. S. (2021). Timing of Gastrografin administration in the management of adhesive small bowel obstruction (ASBO): does it matter? Surgery, 170(2), 596–602. https://doi.org/10.1016/j.surg.2021.03.008
ten Broek, R.P.G., Krielen, P., Di Saverio, S., et al. (2018). Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group. World Journal of Emergency Surgery, 13(24). https://doi.org/10.1186/s13017-018-0185-2