Hyperkalemia is defined as serum potassium (K+) concentration ≥5.5 mEq/L (cutoff ranges between 5.0 and 5.5 mEq/L, depending on the source). Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and5.0 mEq/L, despite marked variations in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia is usually asymptomatic if minor in severity; however, acute elevations or severe hyperkalemia can lead to potentially fatal cardiac arrhythmias. Management is guided by severity and includes measures to stabilize the myocardial membrane potential, transiently shifting K+ intracellularly, removing K+ from the body, and treating the underlying predisposing conditions.
K+ is the main intracellular cation in all cells and is distributed unevenly between the intracellular fluidIntracellular fluidThe fluid inside cells.Body Fluid Compartments (98%) and extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (2%).
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia causes partial depolarizationDepolarizationMembrane Potential (i.e., decrease) of the resting membrane potentialResting membrane potentialMembrane Potential
With prolonged depolarizationDepolarizationMembrane Potential, the cell membraneCell MembraneA cell membrane (also known as the plasma membrane or plasmalemma) is a biological membrane that separates the cell contents from the outside environment. A cell membrane is composed of a phospholipid bilayer and proteins that function to protect cellular DNA and mediate the exchange of ions and molecules. The Cell: Cell Membrane will become more refractory and less likely to fully depolarize/decreased excitabilityExcitabilitySkeletal Muscle Contraction of cardiac cells → predisposition for arrhythmias
The kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy are responsible for 90%–95% of the overall K+ regulation.
The GI tract secretes 5%–10% of absorbed K+ daily.
Movement of potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia in the kidney[2,4,11]
Glomerulus: K+ is freely filtered.
Proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System: 65%–70% of filtered K+ is reabsorbed.
Thick ascending limbThick ascending limbRenal Sodium and Water Regulation of the loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System: 10%–25% of filtered K+ is reabsorbed.
Principal cell (cortical collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma): K+ is secreted.
𝛼-intercalated cell (collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma): K+ is reabsorbed (final fine-tuning mechanism).
Normal response to ingested K+[2,4,14]
A normal Western diet contains approximately 70–150 mmol of K+ per day. This diet is unlikely to lead to the development of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia from increased intake only, owing to the following mechanisms:
Gut absorbs dietary K+ into the bloodstream.
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift prevents excessive increase in extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (ECF) K+ concentration.
Insulin- and β2-mediated
K+ shifts primarily into muscle and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy cells.
Increased ECF K+ concentration triggers mechanisms for renal K+ excretion.
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting into muscle/liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy cells gradually reverses.
The etiologies of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia can be grouped into 5 categories: transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifts, tissue breakdown, inadequate renal excretion, drug-induced, and pseudohyperkalemia.
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifts[2,4,10,11]
Certain factors cause K+ to move transiently into or out of cells.
The effect of this shift can be significant enough to decrease or increase the measured serum K+.
The total body K+ does not change.
Factors that cause shifting out of the cell (→ raises the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+):
AcidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis: H+/K+ exchange maintains electroneutrality → moves H+ into cell to help balance extracellular pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance in exchange for K+ moving out of the cell
Hyperosmolality (hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus, IV contrast, mannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics):
High ECF osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation → shift of water into ECF → decreases ECF K+ concentration → more favorable gradient for diffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis of K+ out of cells
Solvent drag on K+ as water leaves the cell may also contribute.
Common mechanism in hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus (i.e., diabetic ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis (DKADKADiabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are serious, acute complications of diabetes mellitus. Diabetic ketoacidosis is characterized by hyperglycemia and ketoacidosis due to an absolute insulin deficiency. Hyperglycemic Crises))
Exercise: K+ is intentionally released by muscle cells to act as a local vasodilator.
Factors that cause shifting into the cell (→ lowers the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+):
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin: stimulates Na+/K+ ATPase → 3 Na+ move out of cell, 2 K+ move into cell
β2-Adrenergic agonist (i.e., albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs; stimulates Na+/K+ ATPase)
AlkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis: H+/K+ exchanger moves H+ out of cell to help balance extracellular pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance in exchange for K+ moving into cell
Transcellular shift of K+:
Extracellular shift of K+:
1. Acidosis (increased H+) causes blockage of the Na+/H+ exchanger, which causes a decrease in intracellular Na+, in turn blocking Na+/K+ ATPase. On the other hand, acidosis activates the H+/K+ exchanger. Both cause an increase in extracellular K+.
2. Increased osmolarity in extracellular space (hyperglycemia, IV contrast, mannitol) shifts water outside the cell, decreasing K+ concentration. Increased gradient causes K+ diffusion outside.
Intracellular shift of K+:
1. Alkalosis (decreased H+) causes activation of the Na+/H+ exchanger, which causes an increase in intracellular Na+, in turn activating Na+/K+ ATPase. On the other hand, alkalosis blocks the H+/K+ exchanger. Both cause a decrease in extracellular K+.
2. Insulin and β2 adrenergic agonists activate Na+/K+ ATPase, lowering plasma K+ concentration.
Image by Lecturio.
Tissue breakdown[2,4,14,17]
Similar to transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift, but the shift is not reversible
Damage to a cell results in release of the highly concentrated intracellular K+:
Tumor lysisTumor LysisTumor Lysis Syndrome syndrome (high-volume malignant cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death after chemotherapyChemotherapyOsteosarcoma)
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis (muscle cells; trauma, crush injuries, prolonged immobilizationImmobilizationDelirium, associated with malignant hyperthermiaMalignant hyperthermiaAn important complication of anesthesia is malignant hyperthermia, an autosomal dominant disorder of the regulation of calcium transport in the skeletal muscles resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high fever, muscle rigidity, rhabdomyolysis, and respiratory and metabolic acidosis. Malignant Hyperthermia)
Transfusion of multiple units of packed red blood cellsRed blood cellsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology and/or older stored red blood cellsRed blood cellsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology are used (RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology lyse over time in storage)
GI bleeding (RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology metabolized by GI tract → intracellular K+ released)
Large hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception (RBC reabsorbed and metabolized → intracellular K+ released)
BurnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns
OliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation plus excess K+ load or aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia blocker (ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors/ARB, spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics) will result in hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.
OliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation by itself may not cause hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.
Type IV renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis):
A syndrome of decreased urinary secretionSecretionCoagulation Studies of K+ and H+, resulting in a non–anion gapAnion gapMetabolic Acidosis metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis, and hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Common causes include:
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration:
Also occurs in states of total body fluid overload, but with effective arterial blood volumeEffective arterial blood volumeRenal Sodium and Water Regulation depletion (heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis)
Volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration can also cause acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury (AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury) → hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia from oliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation
Functional hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism:
Mineralocorticoid deficiency:
Primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease (Addison disease)
Tubulointerstitial disease: sickle cell diseaseSickle cell diseaseSickle cell disease (SCD) is a group of genetic disorders in which an abnormal Hb molecule (HbS) transforms RBCs into sickle-shaped cells, resulting in chronic anemia, vasoocclusive episodes, pain, and organ damage.Sickle Cell Disease, urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy obstruction
Drugs (see table below)
Drug-induced hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia[2,4,14,17]
Drugs are a very common cause of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia and cause it by a variety of the previously mentioned mechanisms. A key part of the diagnosis of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia is to review all the recent drugs and medications that a patient has received.
Table: Drug-induced hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Medication class (examples)
Mechanism
ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors (e.g., lisinoprilLisinoprilOne of the angiotensin-converting enzyme inhibitors (ACE inhibitors), orally active, that has been used in the treatment of hypertension and congestive heart failure.Renin-Angiotensin-Aldosterone System Inhibitors, captoprilCaptoprilA potent and specific inhibitor of peptidyl-dipeptidase a. It blocks the conversion of angiotensin I to angiotensin II, a vasoconstrictor and important regulator of arterial blood pressure. Captopril acts to suppress the renin-angiotensin system and inhibits pressure responses to exogenous angiotensin.Hypertension Drugs)
Inhibits angiotensin IIAngiotensin IIAn octapeptide that is a potent but labile vasoconstrictor. It is produced from angiotensin I after the removal of two amino acids at the c-terminal by angiotensin converting enzyme. The amino acid in position 5 varies in different species. To block vasoconstriction and hypertension effect of angiotensin II, patients are often treated with ace inhibitors or with angiotensin II type 1 receptor blockers.Renal Sodium and Water Regulation formation → decreases aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies → decreases renal K+secretionSecretionCoagulation Studies
ARB (e.g., losartanLosartanAn antagonist of angiotensin type 1 receptor with antihypertensive activity due to the reduced pressor effect of angiotensin II.Hypertension Drugs, valsartanValsartanA tetrazole derivative and angiotensin II type 1 receptor blocker that is used to treat hypertension.Hypertension Drugs)
Blocks angiotensin receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors → ↓ aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies → ↓ renal K+secretionSecretionCoagulation Studies
Blocks reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation from converting angiotensinogen to angiotensin l → decreases aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiasecretionSecretionCoagulation Studies → ↓ renal K+ excretion
K+-sparing diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication (e.g., amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome, triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics, spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics)
Block epithelial sodium channelEpithelial sodium channelSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome (ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome) (amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome, triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics) or the aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.HyperkalemiareceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors (spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics, eplerenoneEplerenoneA spironolactone derivative and selective aldosterone receptor antagonist that is used in the management of hypertension and congestive heart failure, post-myocardial infarction.Potassium-sparing Diuretics) → ↓ renal K+ excretion
Cardiac glycosidesCardiac glycosidesCardiac glycosides are a class of drugs reversibly inhibiting the sodium-potassium ATPase pump in myocardial cells and increasing vagal tone, which results in increased cardiac contractility and slowed conduction through the atrioventricular node. Cardiac Glycosides (digoxinDigoxinA cardiotonic glycoside obtained mainly from digitalis lanata; it consists of three sugars and the aglycone digoxigenin. Digoxin has positive inotropic and negative chronotropic activity. It is used to control ventricular rate in atrial fibrillation and in the management of congestive heart failure with atrial fibrillation. Its use in congestive heart failure and sinus rhythm is less certain. The margin between toxic and therapeutic doses is small.Cardiac Glycosides)
Decreases reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia → ↓ renal K+secretionSecretionCoagulation Studies
Calcineurin inhibitorsCalcineurin InhibitorsCompounds that inhibit or block the phosphatase activity of calcineurin.Immunosuppressants (e.g., cyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants, tacrolimusTacrolimusA macrolide isolated from the culture broth of a strain of streptomyces tsukubaensis that has strong immunosuppressive activity in vivo and prevents the activation of T-lymphocytes in response to antigenic or mitogenic stimulation in vitro.Immunosuppressants)
Multifactorial/incompletely understood: ↓ aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia release, ↓ aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia sensitivity, inhibition of Na+/K+ ATPase pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols, blocking of ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome channel
SuccinylcholineSuccinylcholineA quaternary skeletal muscle relaxant usually used in the form of its bromide, chloride, or iodide. It is a depolarizing relaxant, acting in about 30 seconds and with a duration of effect averaging three to five minutes. Succinylcholine is used in surgical, anesthetic, and other procedures in which a brief period of muscle relaxation is called for.Cholinomimetic Drugs
Causes extracellular leakage of K+ through acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS receptor-gated channelsChannelsThe Cell: Cell Membrane
Antimicrobials (e.g., trimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim, pentamidine)
Block ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome
ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome: epithelial sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiachannelsChannelsThe Cell: Cell Membrane
Pseudohyperkalemia[2,4,10,14,17]
False positiveFalse positiveAn FP test result indicates that a person has the disease when they do not.Epidemiological Values of Diagnostic TestshyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia:
Related to blood draw → damaged RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology lyse and release their intracellular K+:
Prolonged tourniquet time
Excessive fist clenching
Venipuncture trauma
Related to blood sample processing:
Severe thrombocytosis or leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus
More likely if blood sample analysis is delayed
Intracellular K+ is released from plateletsPlateletsPlatelets are small cell fragments involved in hemostasis. Thrombopoiesis takes place primarily in the bone marrow through a series of cell differentiation and is influenced by several cytokines. Platelets are formed after fragmentation of the megakaryocyte cytoplasm. Platelets: Histology after clotting in the test tube.
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia is a medical emergency due to its arrhythmic effects on the heart. Cardiac symptoms are more likely to occur with increasing severity and acuity of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia; however, even relatively severe hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia can be asymptomatic. Weakness and paralysis of skeletal muscle may also be observed.
Cardiac symptoms[2,10,11,17]
Cardiac symptoms are the most important symptoms of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, as they can be rapidly fatal.
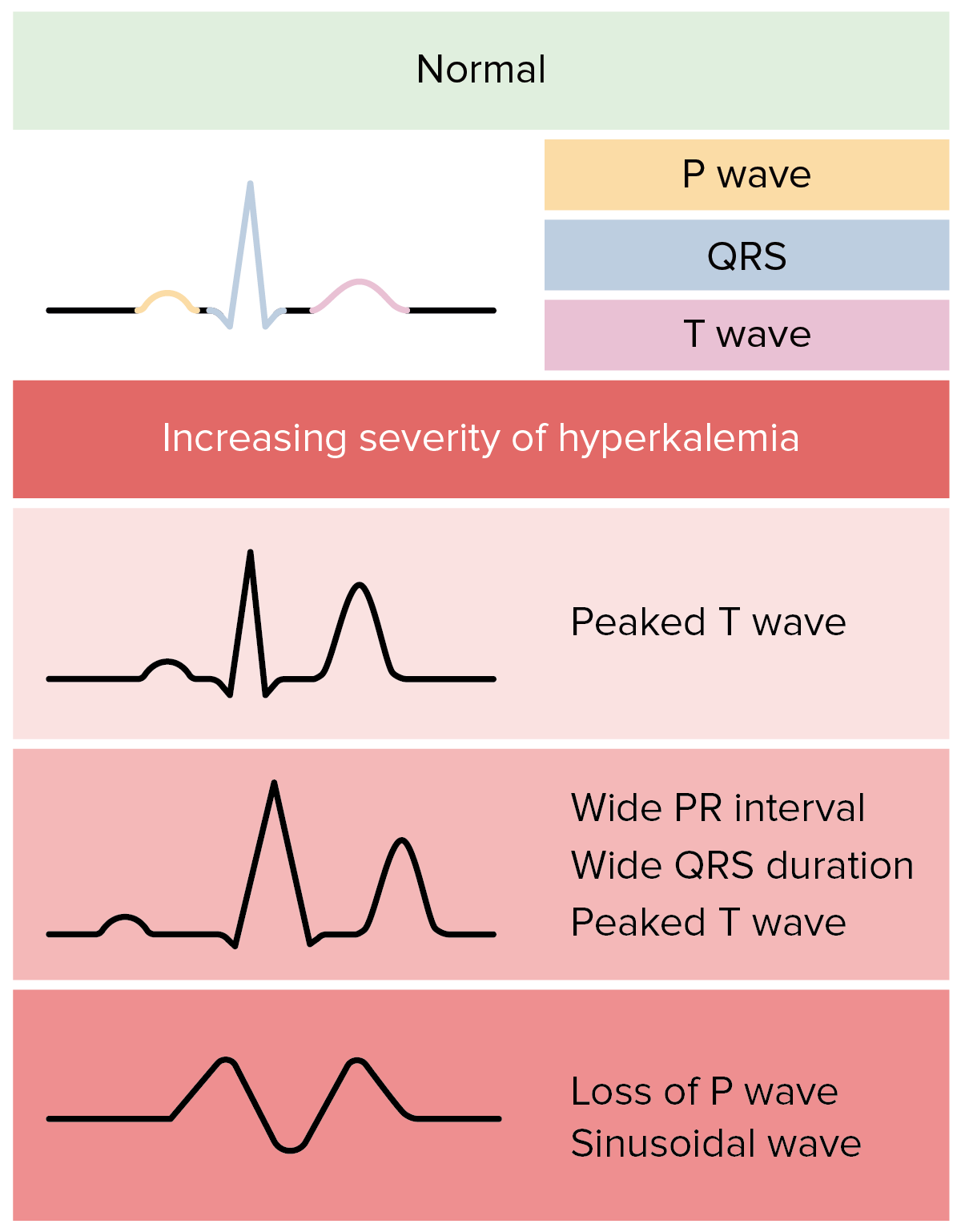
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes follow a characteristic progression with increasing K+:
Peaked T waves and short QTShort QTHyperkalemia interval → PR intervalPR intervalElectrocardiogram (ECG) prolongation and QRS widening → loss of P waves → QRS widens to sine wave → asystoleAsystoleNo discernible electrical activity, flatline on electrocardiogram (P waves and QRS complexes are not present).Cardiac Arrest
This classic progression is often not observed clinically.
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) findings are helpful if present but are not sensitive for hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia overall.
Arrhythmias and cardiac conduction abnormalities:
Cardiac conduction abnormalities (e.g., advanced atrioventricular blockAtrioventricular blockAtrioventricular (AV) block is a bradyarrhythmia caused by delay, or interruption, in the electrical conduction between the atria and the ventricles. Atrioventricular block occurs due to either anatomic or functional impairment, and is classified into 3 types. Atrioventricular block (AV block), bundle branch blockBundle branch blockA form of heart block in which the electrical stimulation of heart ventricles is interrupted at either one of the branches of bundle of His thus preventing the simultaneous depolarization of the two ventricles.Bundle Branch and Fascicular Blocks)
Sinus arrestSinus arrestThe omission of atrial activation that is caused by transient cessation of impulse generation at the sinoatrial node. It is characterized by a prolonged pause without P wave in an electrocardiogram. Sinus arrest has been associated with sleep apnea (rem sleep-related sinus arrest).Bradyarrhythmias
Slow idioventricular rhythm
Ventricular tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children, ventricular fibrillationVentricular fibrillationVentricular fibrillation (VF or V-fib) is a type of ventricular tachyarrhythmia (> 300/min) often preceded by ventricular tachycardia. In this arrhythmia, the ventricle beats rapidly and sporadically. The ventricular contraction is uncoordinated, leading to a decrease in cardiac output and immediate hemodynamic collapse. Ventricular Fibrillation (V-fib), and/or asystoleAsystoleNo discernible electrical activity, flatline on electrocardiogram (P waves and QRS complexes are not present).Cardiac Arrest if severe
Monitoring:
Important at all levels of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Can be done with repeat ECGs and/or continuous cardiac monitoring
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will not have ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes or arrhythmias, even with severe hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.
ECG changes in hyperkalemia: In reality, ECG changes in hyperkalemia are more variable and less predictable.
IleusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Unlikely to have respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure due to respiratory muscle weaknessRespiratory muscle weaknessRespiratory Acidosis
The management of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia often takes precedence over the diagnosis because of the possibility of life-threatening arrhythmias and is guided by determining the level of urgency needed for treatment. Usually, the etiology of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia is not difficult to determine and is not impeded by treating it first.
The following recommendations are based on current US and UK guidelines for acute hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia management.
For all cases of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia[10–14,17,19]
Ensure lab result is accurate:
Hemolyzed specimen:
Very common type of pseudohyperkalemia
Most labs will routinely indicate if specimen is hemolyzed.
Redraw lab prior to making treatment decisions.
Less common causes of pseudohyperkalemia:
Severe thrombocytosis (i.e., > 1000 × 109/L)
Severe leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus (i.e., > 50,000 × 109/L)
Measure plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ (rather than routine serum K+) to obtain an accurate level.
Identify and treat any contributing underlying diseases.
Stop potentially causative medications.
Recognition and management of hyperkalemic emergency
A hyperkalemic emergency exists if the serum K+ > 6.5–7 mEq/L (cutoff differs in the literature) OR if there are clinical signs or symptoms of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia:[10‒13]
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes (arrhythmias or cardiac conduction abnormalities)
Severe muscle weakness or paralysis
Significant kidney impairment and ongoing tissue breakdown (e.g., rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis)
Options for emergency treatment:[10‒19]
Stabilize myocardiumMyocardiumThe muscle tissue of the heart. It is composed of striated, involuntary muscle cells connected to form the contractile pump to generate blood flow.Heart: Anatomy → lower risk of ventricular fibrillationVentricular fibrillationVentricular fibrillation (VF or V-fib) is a type of ventricular tachyarrhythmia (> 300/min) often preceded by ventricular tachycardia. In this arrhythmia, the ventricle beats rapidly and sporadically. The ventricular contraction is uncoordinated, leading to a decrease in cardiac output and immediate hemodynamic collapse. Ventricular Fibrillation (V-fib):
IV calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes
Calcium gluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia, OR
Calcium chlorideCalcium chlorideA salt used to replenish calcium levels, as an acid-producing diuretic, and as an antidote for magnesium poisoning.Hypocalcemia (can cause injection site irritation)
Administer immediately if ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes noted[17]
If ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) not immediately available, still give if K+ > 6.5 mEq/L[16,17]
Note: CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes can worsen cardiac effects in digoxin toxicityDigoxin ToxicityCardiac Glycosides → slow infusion over 20 minutes is recommended).[14,19]
Shift K+ into cells (Note: Effects are temporary.):
IV insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin plus glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance:
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin is provided as a bolus.
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance is given as a bolus (not necessary if serum glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance is ≥ 250 mg/dL).[14,16]
HypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia can occur → glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance infusion often recommended to prevent this[12,14]
β2 agonist (e.g., albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs nebulizer) → has potential additive effect with insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin/glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance[17]
IV sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes:
Use is controversial (limited efficacy in studies)[16]
Potentially helpful when metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis is present[10,17]
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes polystyrene sulfonate is used in Europe.[12]
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia polystyrene sulfonate is used in the US.
Newer potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia binders: patiromer and sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia zirconium cyclosilicate[17]
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome:
Option of choice for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with end-stage renal disease[17]
Consider in:
Therapy-refractory cases
Severe hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia with acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury[18]
Additional considerations:[10‒14]
Continuous cardiac monitoring and/or repeat ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) while treating
If insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin is given, close glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance monitoring is required → risk of hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
Consult nephrology early, particularly if dialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis may be needed.
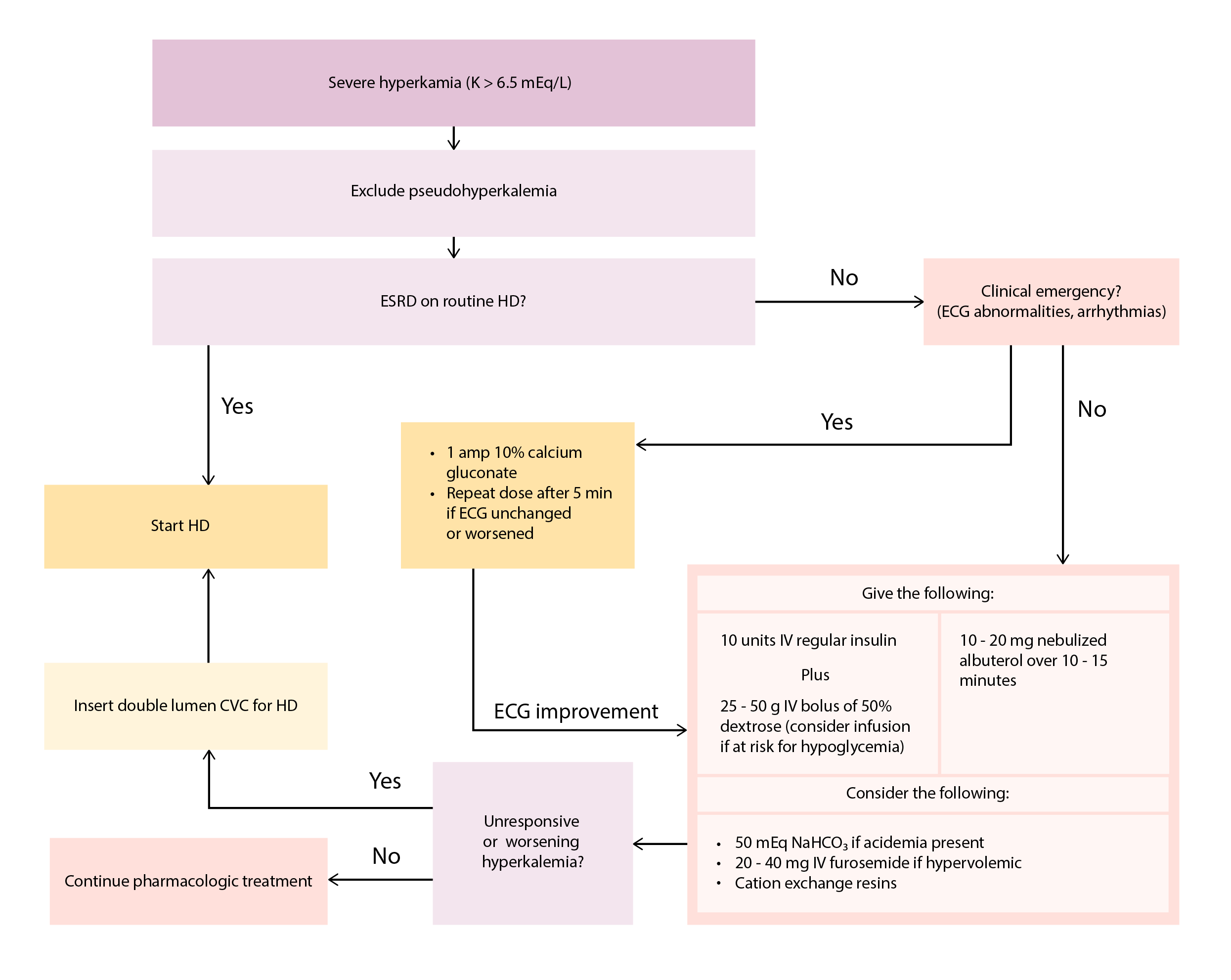
Algorithm for the management of severe hyperkalemia.
CKD: chronic kidney disease; CVC: central venous catheter; HD: hemodialysis; K: serum potassium; SPS: sodium polystyrene sulfonate
Image by Lecturio.
Recognition and management of mild and moderate hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
Moderate hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia with high risk:[10‒13]
Features:
Generally asymptomatic and without ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes
Serum K+ 5.5–6.5 mEq/L with high-risk factor:
Sudden increase (e.g., 3.7 mEq/L to 6 mEq/L overnight)
Ongoing K+ release (e.g., tumor lysisTumor LysisTumor Lysis Syndrome, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis)
Ongoing K+absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption (e.g., GI bleeding)
Kidney dysfunction
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
Treat similarly to hyperkalemic emergency, but no need for IV calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes.
Moderate hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia without high risk:[10‒13]
Features:
Serum K+ 5.5–6.5 mEq/L without any of the above risk factors
Generally asymptomatic and without ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes
Treat urgently:
Cation exchange resin +/– loop diuretic +/– hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome to remove K+
Differences with emergent treatment:
Do not need IV calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes
Do not necessarily need shifting measures
Monitor serum K+ frequently
Continuous cardiac monitoring and/or repeat ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) while treating
Mild hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia:[10‒13]
Features:
Serum K+ < 5.5 mEq/L
Generally asymptomatic and without ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes
Does not require urgent treatment
Management is primarily risk-factor modification:
Dietary K+ restriction if renal dysfunction
Stop/adjust offending medications (e.g., ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors/ARB, NSAIDsNSAIDSPrimary vs Secondary Headaches, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).).
Start/adjust loop or thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication.
Start/adjust oral sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes.
Start/adjust cation exchange resin.
Table: Pharmacologic interventions for hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia[10,12‒15,17]
Medication
Dose
Effects
Notes
Stabilize myocardiumMyocardiumThe muscle tissue of the heart. It is composed of striated, involuntary muscle cells connected to form the contractile pump to generate blood flow.Heart: Anatomy
10% calcium gluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia
10% calcium chlorideCalcium chlorideA salt used to replenish calcium levels, as an acid-producing diuretic, and as an antidote for magnesium poisoning.Hypocalcemia
Can cause tissue necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage if extravasation occurs (central venous access preferred)
Shift K+ into cells
RegularRegularInsulininsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin + dextroseDextroseIntravenous Fluids (bolus)
IV regularRegularInsulininsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin: 10 units
Monitor for hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia.
Consider dextroseDextroseIntravenous Fluids infusion for those at risk for hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia (10% @ 50 mL/hr for 5 hours)[12]sup>
AlbuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs (also known as salbutamol)
Nebulized: 10–20 mg over 10–15 minutes
Repeated up to 8 times in 120 minutes
Expected ↓ in K+: 0.5–1 mEq/L
Onset of action: 15–30 minutes
Duration: 2–4 hours/li>
Side effects may include tremorTremorCyclical movement of a body part that can represent either a physiologic process or a manifestation of disease. Intention or action tremor, a common manifestation of cerebellar diseases, is aggravated by movement. In contrast, resting tremor is maximal when there is no attempt at voluntary movement, and occurs as a relatively frequent manifestation of parkinson disease.Myotonic Dystrophies, tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children, and anxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder.
Potentially additive effect with insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin/dextroseDextroseIntravenous Fluids
Use with caution in those with ischemic heart diseaseIschemic heart diseaseCoronary heart disease (CHD), or ischemic heart disease, describes a situation in which an inadequate supply of blood to the myocardium exists due to a stenosis of the coronary arteries, typically from atherosclerosis. Coronary Heart Disease.
Beta blockers may diminish effect.
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
IV: 50 mEq over 5 minutes OR
IV: 8.4% 100–250 mL over 20 minutes[18]
Expected ↓ in K+: variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Onset of action: 5–10 minutes
Duration: 2 hours
Use only if metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis present
Risk of hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia, volume overload
Remove K+
FurosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics
IV: 20–40 mg
Expected ↓ in K+: variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Onset of action: 15–60 minutes
Duration: 4–6 hours
Avoid in hypovolemiaHypovolemiaSepsis in Children or oliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation
Higher doses may be required in CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease.
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia polystyrene sulfonate
Oral: 25‒50 g
Rectal enema: 25‒50 g
Expected ↓ in K+: variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Onset of action: 1‒2 hours
Duration: ≥ 4‒6 hours
SorbitolSorbitolA polyhydric alcohol with about half the sweetness of sucrose. Sorbitol occurs naturally and is also produced synthetically from glucose. It was formerly used as a diuretic and may still be used as a laxative and in irrigating solutions for some surgical procedures. It is also used in many manufacturing processes, as a pharmaceutical aid, and in several research applications.Laxatives solution is associated with ↑ risk of colonic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis must be ruled out before administration.
Can cause electrolyte abnormalities
Caution in heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) (due to potential for sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia overload)
Patiromer
Oral: 8.4‒25.2 g
Expected ↓ in K+: variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Information adapted from recommendations by the American Academy of Family Practice, American Italian Society of Nephrology, The Renal Association, The American Heart Association, National Kidney Foundation, and Kidney Disease: Improving Global Outcomes (KDIGO).
CKD: chronic kidney disease
Diagnosis[10–14,17]
The subsequent evaluation should focus on the cause of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.
AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury or CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease present?
Recent process that could cause transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift?
New or worsening metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (including DKADKADiabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are serious, acute complications of diabetes mellitus. Diabetic ketoacidosis is characterized by hyperglycemia and ketoacidosis due to an absolute insulin deficiency. Hyperglycemic Crises)
Recent intense exercise
Recent surgery
Other predisposing disease processes present?
HypovolemiaHypovolemiaSepsis in Children or other states of decreased effective arterial blood volumeEffective arterial blood volumeRenal Sodium and Water Regulation (heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis)
High cell turnover (tumor lysisTumor LysisTumor Lysis Syndrome syndrome, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, burnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns)
RBC absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption (RBC transfusion, GI bleeding, large hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception reabsorption)
Review medication list carefully.
Check plasma renin activityPlasma renin activityRenal Artery Stenosis and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia if etiology is still not identified.
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis: large-scale muscle cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death, which can result from many possible etiologies (trauma, drugs, toxins, infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease): Serum K+ can increase suddenly if rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis is unrecognized or inadequately treated or if AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury develops (common complication). RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis is diagnosed by a serum CK level > 5 times the upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal and treated with IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids.
Tumor lysisTumor LysisTumor Lysis Syndrome syndrome: large-scale malignant cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death, often sudden and brought on by the initiation of chemotherapyChemotherapyOsteosarcoma: Large amounts of intracellular K+, phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes, and uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis are released when malignant cells die. Treated with rasburicaseRasburicaseGout Drugs (for hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout), calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes supplementation, and dialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis, if necessary.
Digoxin toxicityDigoxin ToxicityCardiac Glycosides: DigoxinDigoxinA cardiotonic glycoside obtained mainly from digitalis lanata; it consists of three sugars and the aglycone digoxigenin. Digoxin has positive inotropic and negative chronotropic activity. It is used to control ventricular rate in atrial fibrillation and in the management of congestive heart failure with atrial fibrillation. Its use in congestive heart failure and sinus rhythm is less certain. The margin between toxic and therapeutic doses is small.Cardiac Glycosides is the only commonly used cardiac glycoside. ToxicityToxicityDosage Calculation is common, as the therapeutic windowTherapeutic WindowDosage Calculation is narrow and excretion is renal. Clinical presentation includes arrhythmias, hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, and characteristic visionVisionOphthalmic Exam changes, including increased yellow colors in visionVisionOphthalmic Exam (xanthopsia). Treated with digoxin-specific antibody (FabFabUnivalent antigen-binding fragments composed of one entire immunoglobulin light chain and the amino terminal end of one of the immunoglobulin heavy chains from the hinge region, linked to each other by disulfide bonds. Fab contains the immunoglobulin variable regions, which are part of the antigen-binding site, and the first immunoglobulin constant regions. This fragment can be obtained by digestion of immunoglobulins with the proteolytic enzyme papain.Immunoglobulins: Types and Functions) fragments, which bindBINDHyperbilirubinemia of the Newborn to and thereby inactivate the circulating drug.
Malignant hyperthermiaMalignant hyperthermiaAn important complication of anesthesia is malignant hyperthermia, an autosomal dominant disorder of the regulation of calcium transport in the skeletal muscles resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high fever, muscle rigidity, rhabdomyolysis, and respiratory and metabolic acidosis. Malignant Hyperthermia: a life-threatening syndrome characterized by hyperthermia, muscle rigidityMuscle rigidityContinuous involuntary sustained muscle contraction which is often a manifestation of basal ganglia diseases. When an affected muscle is passively stretched, the degree of resistance remains constant regardless of the rate at which the muscle is stretched. This feature helps to distinguish rigidity from muscle spasticity.Motor Neuron Lesions, and hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia (via rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis): Malignant hyperthermiaMalignant hyperthermiaAn important complication of anesthesia is malignant hyperthermia, an autosomal dominant disorder of the regulation of calcium transport in the skeletal muscles resulting in a hypermetabolic crisis. Malignant hyperthermia is marked by high fever, muscle rigidity, rhabdomyolysis, and respiratory and metabolic acidosis. Malignant Hyperthermia is triggered by volatile anesthetic and/or succinylcholineSuccinylcholineA quaternary skeletal muscle relaxant usually used in the form of its bromide, chloride, or iodide. It is a depolarizing relaxant, acting in about 30 seconds and with a duration of effect averaging three to five minutes. Succinylcholine is used in surgical, anesthetic, and other procedures in which a brief period of muscle relaxation is called for.Cholinomimetic Drugs use in genetically predisposed patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship. Treatment includes dantroleneDantroleneSkeletal muscle relaxant that acts by interfering with excitation-contraction coupling in the muscle fiber. It is used in spasticity and other neuromuscular abnormalities. Although the mechanism of action is probably not central, dantrolene is usually grouped with the central muscle relaxants.Spasmolytics (skeletal muscle reluctant) and supportive care.
Primary adrenal insufficiencyPrimary adrenal insufficiencyAn adrenal disease characterized by the progressive destruction of the adrenal cortex, resulting in insufficient production of aldosterone and hydrocortisone. Clinical symptoms include anorexia; nausea; weight loss; muscle weakness; and hyperpigmentation of the skin due to increase in circulating levels of acth precursor hormone which stimulates melanocytes.Adrenal Insufficiency and Addison Disease (Addison’s diseaseAddison’s DiseaseAdrenal insufficiency (AI) is the inadequate production of adrenocortical hormones: glucocorticoids, mineralocorticoids, and adrenal androgens. Primary AI, also called Addison’s disease, is caused by autoimmune disease, infections, and malignancy, among others.Adrenal Insufficiency and Addison Disease): a rare, autoimmune type of destruction of the adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy: Addison’s diseaseAddison’s DiseaseAdrenal insufficiency (AI) is the inadequate production of adrenocortical hormones: glucocorticoids, mineralocorticoids, and adrenal androgens. Primary AI, also called Addison’s disease, is caused by autoimmune disease, infections, and malignancy, among others.Adrenal Insufficiency and Addison Disease is diagnosed by measuring aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia (low), reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation (high), serum cortisolCortisolGlucocorticoids (low), and ACTH (low) and ACTH stimulation test. Addison’s diseaseAddison’s DiseaseAdrenal insufficiency (AI) is the inadequate production of adrenocortical hormones: glucocorticoids, mineralocorticoids, and adrenal androgens. Primary AI, also called Addison’s disease, is caused by autoimmune disease, infections, and malignancy, among others.Adrenal Insufficiency and Addison Disease leads to hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia primarily through hypoaldosteronismHypoaldosteronismHypoaldosteronism is a hormonal disorder characterized by low levels of aldosterone. These low levels can be caused by decreased aldosterone production or a peripheral resistance to aldosterone. When hypoaldosteronism occurs as a result of an acquired decrease in renin production, the condition is more commonly referred to as renal tubular acidosis (RTA) type 4. Hypoaldosteronism. The disease manifests acutely as adrenal crisisAdrenal crisisAdrenal crisis is the acute decompensation of adrenal function that can be triggered by another disease, surgery, stress, or increased glucocorticoid inactivation.Adrenal Insufficiency and Addison Disease, which is an emergency because of circulatory shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock. Acute treatment is high-dose glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids and supportive care. Long-term treatment is by substituting glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids (hydrocortisoneHydrocortisoneThe main glucocorticoid secreted by the adrenal cortex. Its synthetic counterpart is used, either as an injection or topically, in the treatment of inflammation, allergy, collagen diseases, asthma, adrenocortical deficiency, shock, and some neoplastic conditions.Immunosuppressants) and mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids (fludrocortisoneFludrocortisoneA synthetic mineralocorticoid with anti-inflammatory activity.Mineralocorticoids).
Diabetic ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis (DKADKADiabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are serious, acute complications of diabetes mellitus. Diabetic ketoacidosis is characterized by hyperglycemia and ketoacidosis due to an absolute insulin deficiency. Hyperglycemic Crises): severe acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis caused by insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin deficiency, usually in the setting of type 1Type 1Spinal Muscular AtrophydiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus: Presents with total body K+ deficit (urinary losses from osmotic diuresisOsmotic diuresisVolume Depletion and Dehydration/polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation); however, serum K+ will be normal or high. Treatment is by insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin replacement followed by K+ supplementation once the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products level falls. If there is even mild hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia on presentation, this represents severe total body K+ deficit, and the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ will decrease even further once an insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin drip is started. In this situation, K+ must be replaced until the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products level is at least 3.3 mEq/L prior to starting insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin.
Hyperkalemic periodic paralysisHyperkalemic Periodic ParalysisIon Channel Myopathy: a rare genetic disease with autosomal dominant inheritanceAutosomal dominant inheritanceAutosomal Recessive and Autosomal Dominant Inheritance: Hyperkalemic periodic paralysisHyperkalemic Periodic ParalysisIon Channel Myopathy is characterized by acute attacks of muscle weakness and/or paralysis due to hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia from severe transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting of K+. Attacks are precipitated by cold temperatures, rest after exercise, and/or K+ ingestion. If recovery is not spontaneous, treatment is with inhaled β2 agonists and K+-removing therapies (e.g., furosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics, cation exchange resins, dialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis).
Type IV renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis): a syndrome of decreased urinary secretionSecretionCoagulation Studies of K+ and H+ at the principal cell, resulting in a non–anion gapAnion gapMetabolic Acidosis metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis, and hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia: Common causes include diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, NSAIDsNSAIDSPrimary vs Secondary Headaches, calcineurin inhibitorsCalcineurin InhibitorsCompounds that inhibit or block the phosphatase activity of calcineurin.Immunosuppressants, heparin, and Addison’s diseaseAddison’s DiseaseAdrenal insufficiency (AI) is the inadequate production of adrenocortical hormones: glucocorticoids, mineralocorticoids, and adrenal androgens. Primary AI, also called Addison’s disease, is caused by autoimmune disease, infections, and malignancy, among others.Adrenal Insufficiency and Addison Disease. Diagnosed by history and measuring serum cortisolCortisolGlucocorticoids, reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation, and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia. Treatment is by mineralocorticoid replacement (e.g., fludrocortisoneFludrocortisoneA synthetic mineralocorticoid with anti-inflammatory activity.Mineralocorticoids). HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia is usually not severe unless concurrent predisposing factors are present.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, a condition of an elevated potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level in the blood, which can be life-threatening due to its effects on cardiac conduction.
Coding System
Code
Description
ICD-10-CM
E87.5
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
SNOMED CT
11123008
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia (disorder)
Evaluation & Workup:
This CPT code is for an ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG), which is the most important initial test in a patient with hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia to assess for cardiotoxicity, such as peaked T waves, widened QRS, and sine wave patterns.
Coding System
Code
Description
CPT
93000
ElectrocardiogramElectrocardiogramAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG), routine ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) with at least 12 leads
CPT
80048
Basic metabolic panelBasic Metabolic PanelPrimary vs Secondary Headaches (to confirm potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level)
Medications:
These codes are for the emergent medical treatments for severe hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia. Calcium gluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia is given to stabilize the cardiac membrane, while insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin (with glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance) and albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs shift potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia into the cells.
Coding System
Code
Description
RxNorm
1898
Calcium GluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia (ingredient)
RxNorm
5797
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin, RegularRegularInsulin, Human (ingredient)
RxNorm
435
AlbuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs (ingredient)
Kasper, D. L., Fauci, A. S., Hauser, S. L., Longo, D. L., Jameson, J. L., Loscalzo, J. (2015). Harrison’s principles of internal medicine (19th ed..). New York: McGraw Hill Education.
Bianchi, S., Aucella, F., De Nicola, L., et al. (2019). Management of hyperkalemia in patients with kidney disease: a position paper endorsed by the Italian Society of Nephrology. Journal of Nephrology, 32(4), 499–516. https://doi.org/10.1007/s40620-019-00617-y
Palmer, B. F., Carrero, J. J., Clegg, D. J., Colbert, G. B., Emmett, M., Fishbane, S., Hain, D. J., Lerma, E., Onuigbo, M., Rastogi, A., Roger, S. D., Spinowitz, B. S., Weir, M. R. (2021). Clinical management of hyperkalemia. Mayo Clinic Proceedings, 96(3), 744–762. https://doi.org/10.1016/j.mayocp.2020.06.014