Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) (Clinical)
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) (Clinical)
Thesyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). There are many causes of SIADH, including increased pituitary production of ADH (related to trauma, disease, or medications), ectopic production of ADH by a tumor, and hereditary disorders. SIADH is characterized by impaired water excretion, leading to dilutional hyponatremia. This condition is usually asymptomaticbut may cause neurologic symptoms. SIADH should be suspected in any patient with hyponatremia, hypo-osmolality, and high urine osmolality.
Synthesized in the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus:
Supraoptic nuclei
Paraventricular nuclei
Stored and secreted by the posterior pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types
Secreted in response to[1,10,13]
Increased serum osmolarityOsmolarityThe concentration of osmotically active particles in solution expressed in terms of osmoles of solute per liter of solution. Osmolality is expressed in terms of osmoles of solute per kilogram of solvent.Hypernatremia:
Detected by osmoreceptorsOsmoreceptorsRenal Sodium and Water Regulation (hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus)
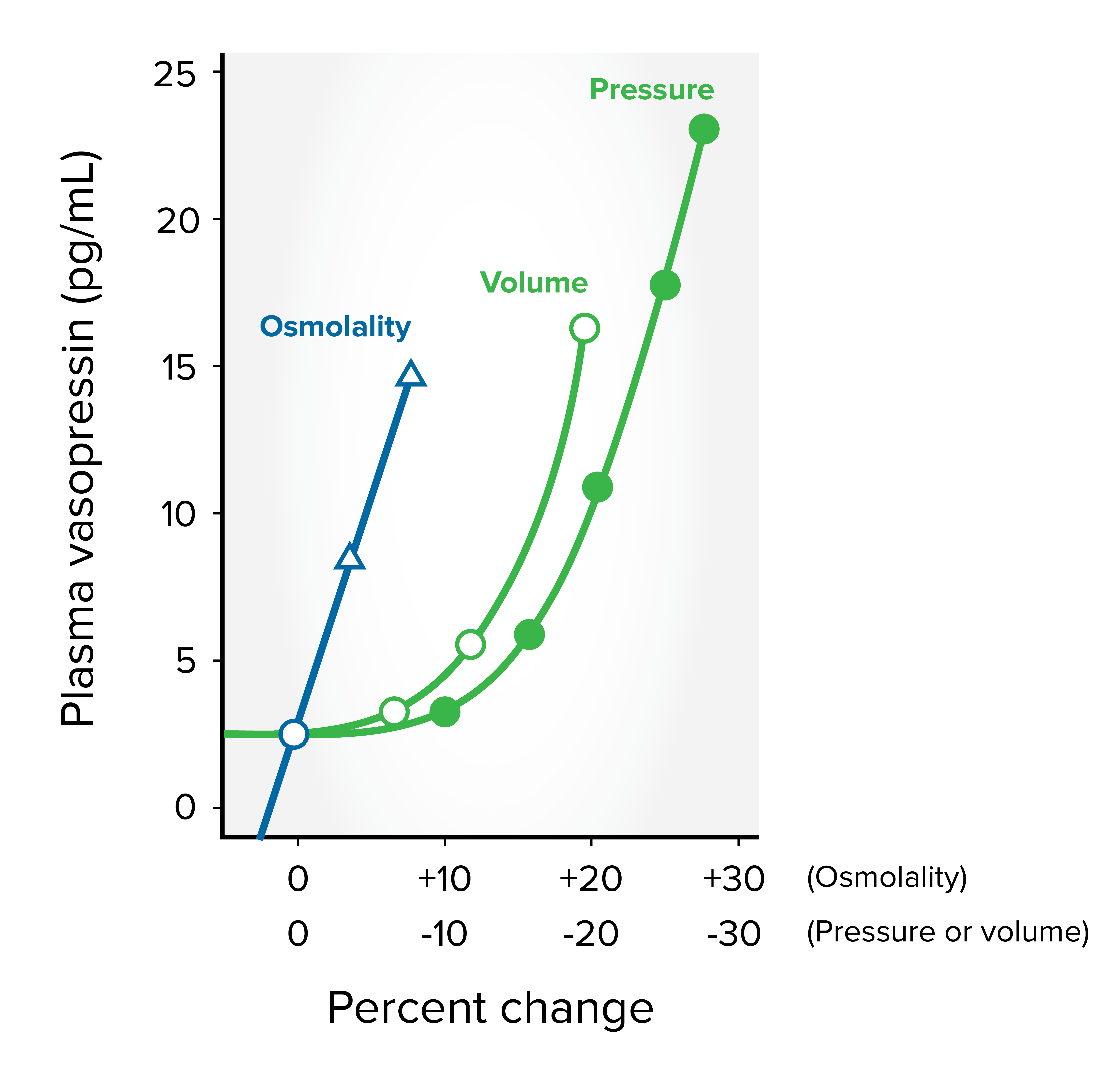
ADH is very sensitive to osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation, responding to as little as a 1% increase.
ADH is less sensitive to blood pressure and volume, requiring a change of 10%–15% to stimulate its release.
Function[3,4,10,13]
Increases free water absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption (via V2 receptorsV2 receptorsRenal Sodium and Water Regulation in the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy):
↓ Serum osmolarityOsmolarityThe concentration of osmotically active particles in solution expressed in terms of osmoles of solute per liter of solution. Osmolality is expressed in terms of osmoles of solute per kilogram of solvent.Hypernatremia
↑ Urine osmolarityOsmolarityThe concentration of osmotically active particles in solution expressed in terms of osmoles of solute per liter of solution. Osmolality is expressed in terms of osmoles of solute per kilogram of solvent.Hypernatremia
↑ Intravascular volume
VasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure (via V1 receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors)
Release of von Willebrand’s factor from endothelial cells
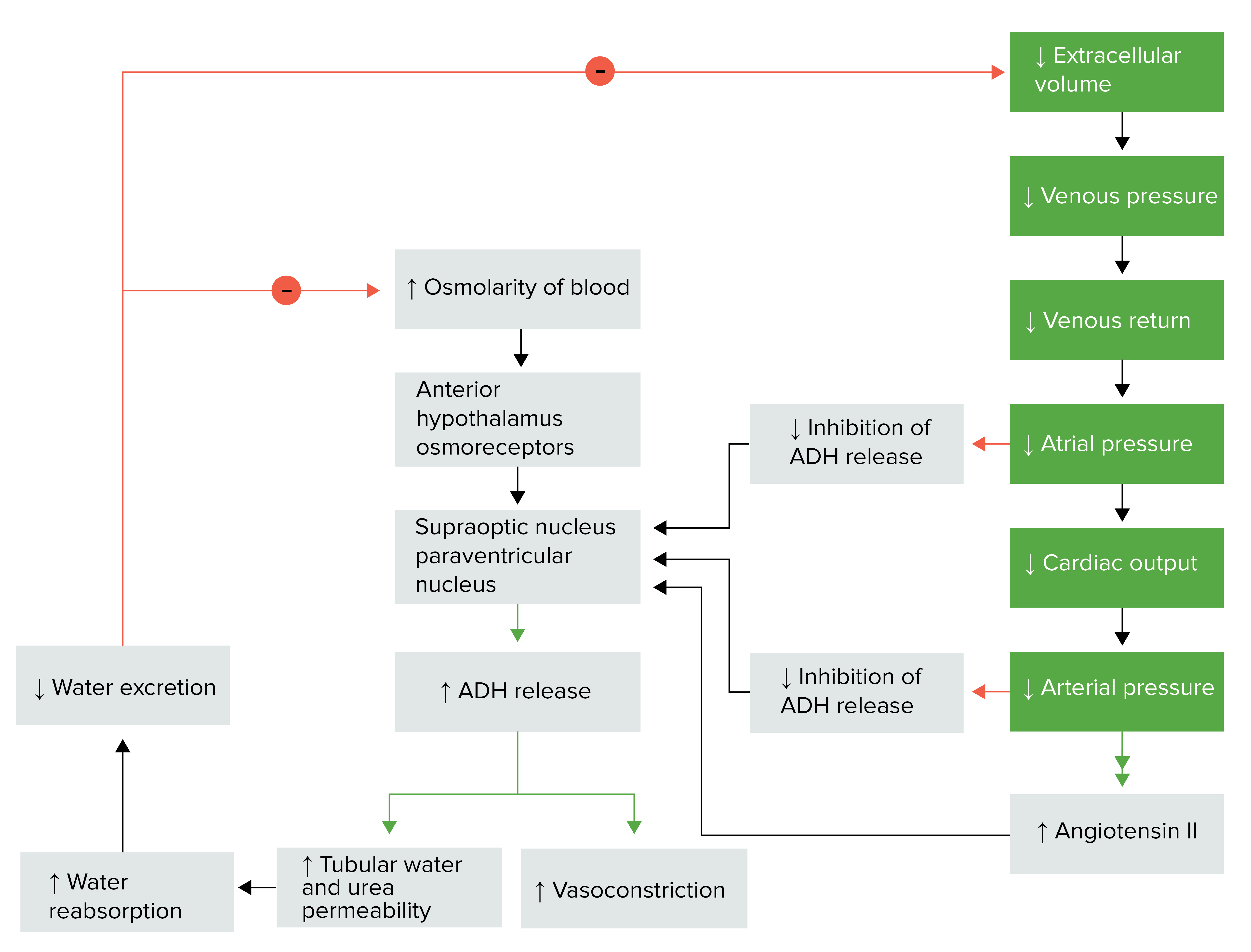
Antidiuretic hormone regulation
Image by Lecturio.
Antidiuretic hormone secretion: directly related to plasma osmolality, blood pressure, and blood volume
Image by Lecturio.
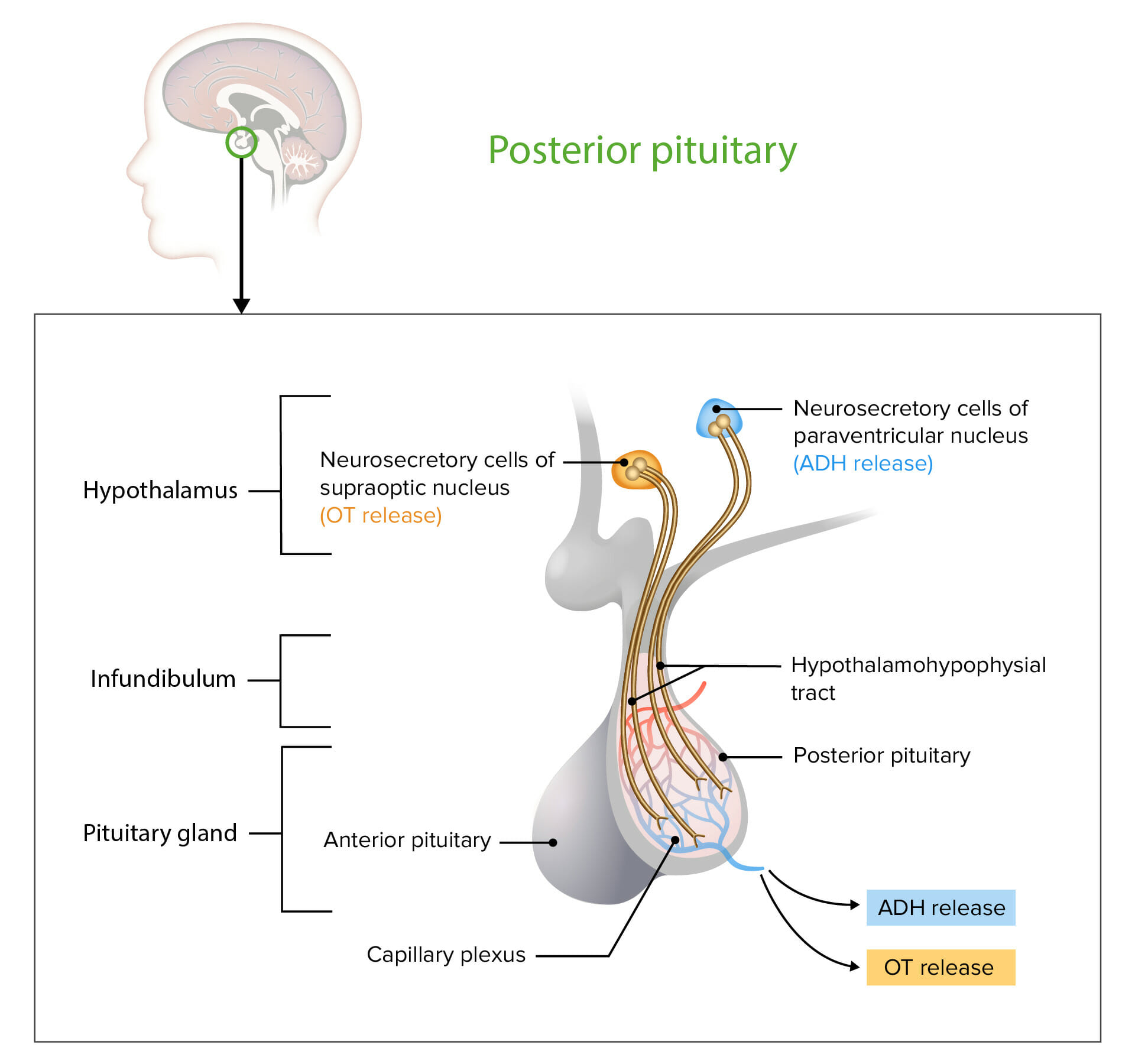
Neurosecretory cells in the hypothalamus release OT or ADH into the posterior lobe of the pituitary gland. The hormones are stored or released into the blood via the capillary plexus.
OT: oxytocin
ADH: antidiuretic hormone
ADH levels normally rise when plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration exceeds 280 mOsm/kg; this mechanism is impaired with SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH).
A mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations affects the geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics for the renal V2 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors
Both types cause free-water absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption and retention → dilutional hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia → cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP) and neurologic symptoms
Due to the combination of ADH-induced water retention and secondary solute loss
Overall solute loss is more prominent than water retention with chronic SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH).
Etiology[1,4,10]
The major causes of SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) are medications, malignancies, or infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease affecting the CNS or lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy.
Subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage
Infection:
MeningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis
EncephalitisEncephalitisEncephalitis is inflammation of the brain parenchyma caused by an infection, usually viral. Encephalitis may present with mild symptoms such as headache, fever, fatigue, and muscle and joint pain or with severe symptoms such as seizures, altered consciousness, and paralysis.Encephalitis
Trauma
NeoplasmsNeoplasmsNew abnormal growth of tissue. Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms.Benign Bone Tumors
Small cell lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung Cancer
Head and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess cancers
Pulmonary causes
PneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
TuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis
AtelectasisAtelectasisAtelectasis is the partial or complete collapse of a part of the lung. Atelectasis is almost always a secondary phenomenon from conditions causing bronchial obstruction, external compression, surfactant deficiency, or scarring. Atelectasis
Medications
CarbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs, oxcarbazepineOxcarbazepineA carbamazepine derivative that acts as a voltage-gated sodium channel blocker. It is used for the treatment of partial seizures with or without secondary generalization. It is also an inducer of cytochrome p-450 cyp3a4.First-Generation Anticonvulsant Drugs
VincristineVincristineAn antitumor alkaloid isolated from vinca rosea.Microtubule and Topoisomerase Inhibitors, vinblastineVinblastineAntitumor alkaloid isolated from vinca rosea.Microtubule and Topoisomerase Inhibitors, vinorelbineVinorelbineA vinca alkaloid related to vinblastine that is used as a first-line treatment for non-small cell lung cancer, or for advanced or metastatic breast cancer refractory to treatment with anthracyclines.Microtubule and Topoisomerase Inhibitors, cisplatinCisplatinAn inorganic and water-soluble platinum complex. After undergoing hydrolysis, it reacts with DNA to produce both intra and interstrand crosslinks. These cross links appear to impair replication and transcription of DNA. The cytotoxicity of cisplatin correlates with cellular arrest in the g2 phase of the cell cycle.Alkylating Agents and Platinum
MAOIsMAOIsMonoamine oxidase inhibitors are a class of antidepressants that inhibit the activity of monoamine oxidase (MAO), thereby increasing the amount of monoamine neurotransmitters (particularly serotonin, norepinephrine, and dopamine). The increase of these neurotransmitters can help in alleviating the symptoms of depression.Monoamine Oxidase Inhibitors
HaloperidolHaloperidolA phenyl-piperidinyl-butyrophenone that is used primarily to treat schizophrenia and other psychoses. It is also used in schizoaffective disorder, delusional disorders, ballism, and tourette syndrome (a drug of choice) and occasionally as adjunctive therapy in intellectual disability and the chorea of huntington disease. It is a potent antiemetic and is used in the treatment of intractable hiccups.First-Generation Antipsychotics
AmphetaminesAmphetaminesAnalogs or derivatives of amphetamine. Many are sympathomimetics and central nervous system stimulators causing excitation, vasopressin, bronchodilation, and to varying degrees, anorexia, analepsis, nasal decongestion, and some smooth muscle relaxation.Stimulants
Surgery
Occurs in surgeries of the abdominal and thoracic regions
Mechanism of release is mediated through painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways afferents.
Symptoms do not always correlate with the severity or the rapidity of onset of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, and some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with profound hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia may be relatively asymptomatic.[1,7,10]
Note: “EuvolemiaEuvolemiaVolume Depletion and Dehydration” in SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) is a bit misleading, as patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship actually have subclinical volume expansion from H2O and NaCl retention.[1]
Patient presentation depends on:
The rate and severity of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (acute and chronic)
The degree of cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP) is the main problem.
Symptoms are mostly neurologic and include:
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
The cells adapt to the osmotic shift/dilutional hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia by losing organic osmolytes (inositol, betaine, glutamateGlutamateDerivatives of glutamic acid. Included under this heading are a broad variety of acid forms, salts, esters, and amides that contain the 2-aminopentanedioic acid structure.Synthesis of Nonessential Amino Acids); therefore, cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP) will be reduced.
The following should be evaluated to determine an etiology for SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH):
Thorough medication review
Risk factors for (or history of):
Cardiac disease
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
HemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis
Abnormal neurologic findings in addition to those of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (listed below under “Clinical Presentation”)
Laboratory results[1,5,10,11,13,14,16]
Laboratory results showing hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, serum hypo-osmolality, and urine hyperosmolality indicate only that ADH is acting on the kidney, not whether its secretionSecretionCoagulation Studies is “inappropriate.”
Blood tests:
Serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (Na+) < 135 mEq/L (hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia)
Serum osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation < 280 mOsm/kg (hypo-osmolality)
Other findings with SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH):
Normal potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia
↓ Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis
↑ ADH level (but may be variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables)
Urine studies (Note: Urine studies will be affected by diuretic use.):
Urine sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia > 20–40 mEq/L (unless on a low-sodium diet)
Urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation > 100 mOsm/kg (inappropriately concentrated)
Fractional excretion of urate (FEUrate):[14]
Can help in cases where diuretic use may cloud typical urine studies
≥ 12% is indicative of SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Additional studies to rule out another diagnosis:
ElectrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes → abnormalities may point to another etiology (e.g., adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease, GI losses)
BUN and creatinine → renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance → pseudohyponatremia
Thyroid-stimulating hormoneThyroid-stimulating hormoneA glycoprotein hormone secreted by the adenohypophysis. Thyrotropin stimulates thyroid gland by increasing the iodide transport, synthesis and release of thyroid hormones (thyroxine and triiodothyronine).Thyroid Hormones (TSH) → hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism
B-type natriuretic peptide (BNPBNPA peptide that is secreted by the brain and the heart atria, stored mainly in cardiac ventricular myocardium. It can cause natriuresis; diuresis; vasodilation; and inhibits secretion of renin and aldosterone. It improves heart function. It contains 32 amino acids.Renal Sodium and Water Regulation) → heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
Other causes of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia to consider:
Salt-wasting renal disease
PituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types insufficiency
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Primary polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus)
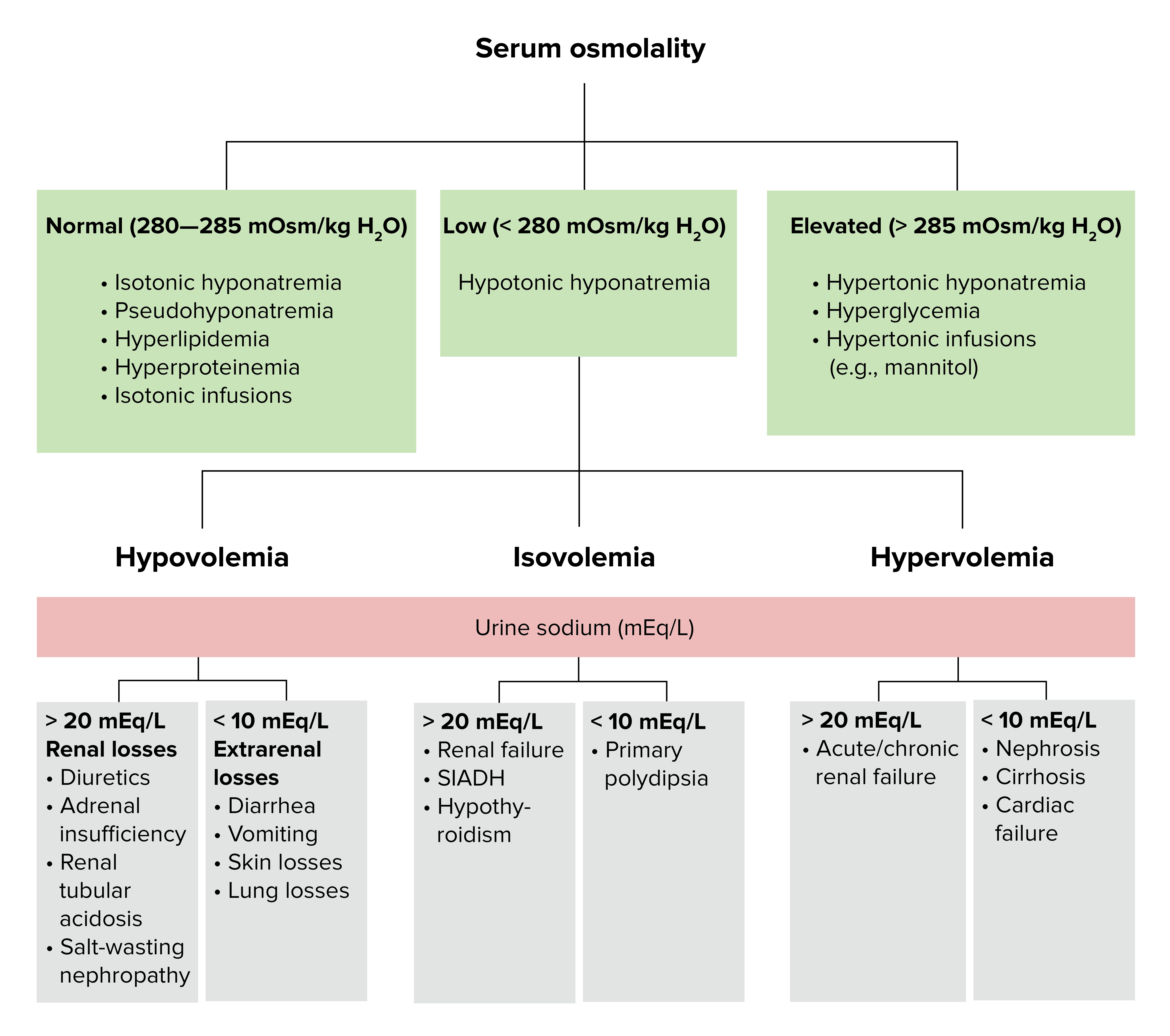
Diagnostic algorithm for volemic and sodium alterations
Absence of other causes for euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) hypo-osmolar hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (e.g., hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism, adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease)
Imaging[10,11]
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests: for underlying pulmonary diseasePulmonary diseaseDiseases involving the respiratory system.Blastomyces/Blastomycosis
CT or MRI brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification to detect:
CNS disease causing SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP) as a complication
Management may vary depending on practice location. The following information is derived from US and European literature and guidelines for adults. See local practice guidelines for additional information.
Overall, treatment includes correction of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia and its underlying cause, if possible. Important note: IsotonicIsotonicSolutions having the same osmotic pressure as blood serum, or another solution with which they are compared.Renal Sodium and Water Regulation saline should be avoided, as it can worsen hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia in SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH).
Treat the underlying disease[1,10,11,15,16]
This is the only definitive treatment for SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), but it may not always be possible (e.g., incurable malignancyMalignancyHemothorax, unknown etiology).
Treat infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., meningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis, pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
Replace hormonesHormonesHormones are messenger molecules that are synthesized in one part of the body and move through the bloodstream to exert specific regulatory effects on another part of the body. Hormones play critical roles in coordinating cellular activities throughout the body in response to the constant changes in both the internal and external environments. Hormones: Overview and Types in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease or hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism
Indications for hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium and specialist referral[12]
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia of uncertain cause
Refractory cases
Need for aggressive therapies (e.g., hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia or vasopressin receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonists)
Severe heart or liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage (SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage)
Restrict to 500‒800 mL/day, if possible: keep in mind that this involves all fluid intake (including IV medications and parenteral and enteral nutritionEnteral nutritionNutritional support given via the alimentary canal or any route connected to the gastrointestinal system (i.e., the enteral route). This includes oral feeding, sip feeding, and tube feeding using nasogastric, gastrostomy, and jejunostomy tubes.Short Bowel Syndrome).
Level of patient complianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology
IV hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia (3% NaCl)
General considerations:[1,6,10,13–15]
Goals of correction:
Initial: Increase serum Na+ by 4‒6 mEq/L within the first 6 hours (maximum, 7 mEq/L in 24 hours).
Subsequent: Increase Na+ by < 8‒10 mEq/L in the first 24 hours.
Maintain serum Na+ at a constant level for the remainder of the 24-hour period.
Alleviation of symptoms
Requires closer monitoring of:
Serum Na+ levels every 2–4 hours (some articles recommend every 1–2 hours)
Fluid status (risk of volume overload, particularly with underlying heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) or cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis)
May lead to iatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome osmotic demyelinationDemyelinationMultiple Sclerosis syndrome (ODS)
Acute (< 48 hours) severe hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (< 130 mOsm/kg):[1,8,10,13–15,17–19]
Asymptomatic:
IV bolus 50–100 mL over 10 minutes
Reassess serum Na+ every 1–2 hours.
Symptomatic:
IV bolus 100–150 mL over 10–20 minutes
May repeat up to 2 additional times in 30 minutes to relieve symptoms.
Severe hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia < 120 mEq/L (mild-to-moderate symptoms):
Initial: 15‒30 mL/hour
Alternative: 50‒100 mL bolus over 10 minutes every 6 hours, as needed
Either rapid intermittent bolus or slow continuous infusion is safe and effective[6]
Severe symptoms (e.g., seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures, comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma) or known intracranial pathology:
Similar to management of acute, symptomatic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
IV bolus 100 mL over 10–20 minutes
May repeat up to 2 additional times in 30 minutes to relieve symptoms.
Alternative:
150 mL over 20 minutes up to 2 total doses
Check serum Na+ between infusions
Stop administration once symptoms resolve.
Other interventions
The following medications may be needed to increase serum Na+ and lower urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation, but they should be started only under the guidance of a specialist.
FurosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics 20 mg orally twice daily
TorsemideTorsemideA pyridine and sulfonamide derivative that acts as a sodium-potassium chloride symporter inhibitor. It is used for the treatment of edema associated with congestive heart failure; chronic renal insufficiency; and liver diseases. It is also used for the management of hypertension.Loop Diuretics 10 mg orally once daily
Note: Higher doses may be needed in cases of renal insufficiency.
Monitor serum potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia.
Oral solute tablets:[1,14]
May be needed in combination with a loop diuretic as 2nd-line treatment (after fluid restriction) → counteracts natriuresis of diuretic
Options:
NaCl
UreaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea Cycle
Usually tolerated poorly
Vasopressin receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonists (vaptans):[1,10,13,16]
Augment free water excretion
European guidelines do not encourage use.[21]
Fluid restriction is generally avoided with vaptan therapy.
Close Na+ monitoring (at least every 6–8 hours, more frequently in those at high risk of ODS)
TolvaptanTolvaptanA benzazepine derivative and selective vasopressin v2 receptor antagonist that is used to treat euvolemic and hypervolemic hyponatremia. It is also used in the treatment of rapidly progressing autosomal dominant polycystic kidney disease to slow the rate of cyst development and renal insufficiency.Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH):
Available in oral form
Dose:
Initial: 15 mg orally once daily
Can be increased by 30 mg at 24-hour intervals
Maximum: 60 mg
Avoid use for > 30 days
Contraindicated in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Beware of drug interactions (metabolized by cytochrome P450Cytochrome P450A superfamily of hundreds of closely related hemeproteins found throughout the phylogenetic spectrum, from animals, plants, fungi, to bacteria. They include numerous complex monooxygenases (mixed function oxygenases). In animals, these p450 enzymes serve two major functions: (1) biosynthesis of steroids, fatty acids, and bile acids; (2) metabolism of endogenous and a wide variety of exogenous substrates, such as toxins and drugs (biotransformation). They are classified, according to their sequence similarities rather than functions, into cyp gene families (>40% homology) and subfamilies (>59% homology). For example, enzymes from the cyp1, cyp2, and cyp3 gene families are responsible for most drug metabolism.Drug-Induced Liver Injury 3A4 (CYP3A4CYP3A4Class 3 Antiarrhythmic Drugs (Potassium Channel Blockers)))
The differential diagnosis of SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)includes other hyponatremic conditions:
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: a low sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration in the blood. Generally defined as sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration < 135 mEq/L, with severe hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia being < 120 mEq/L. The disorders that cause hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia can be divided into:
Disorders that cause impairment in urinary water excretion:
Gastrointestinal (GI) losses (vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea)
Renal losses (diuretic therapy, adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease)
Disorders with edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema (chronic heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis, nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome)
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome (acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury and chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease)
Other causes of excess ADH (cortisolCortisolGlucocorticoids deficiency, hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism, administration of ADH derivatives)
Disorders in which renal handling of water is normal:
Primary polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus)
Cerebral salt wasting
Cerebral salt wasting: renal loss of Na+ with an intracranial disease, which leads to hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia and a decrease in extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments volume. Presents with volume contraction and SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will be euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). The treatment is salt and volume replacement.
Adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease (Addison’s diseaseAddison’s DiseaseAdrenal insufficiency (AI) is the inadequate production of adrenocortical hormones: glucocorticoids, mineralocorticoids, and adrenal androgens. Primary AI, also called Addison’s disease, is caused by autoimmune disease, infections, and malignancy, among others.Adrenal Insufficiency and Addison Disease): glucocorticoid and mineralocorticoid insufficiency due to the destruction or dysfunction of the entire adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy. CortisolCortisolGlucocorticoids has a negative feedbackNegative feedbackHypothalamic and Pituitary Hormones effect on ADH and adrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones (ACTH). The absence of cortisolCortisolGlucocorticoids thus removes this inhibitory effect, increasing the release of ADH.
Psychogenic polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus): increase in water intake attributed to a defect in the thirst mechanism, mostly in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with psychosis.
Hypervolemic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: a deficit of free water excretion that leads to inappropriate water retention in relation to the sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration. This osmotic imbalance results in an expanded extracellular volume and dilutional hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia. It can be seen in cases ofchronic heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis, and nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome. Easy to diagnose based on the significant symptoms and laboratory values of the underlying disease.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), a condition where the body produces too much antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (ADH), leading to water retention and a dilutional hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Coding System
Code
Description
ICD-10-CM
E22.2
Syndrome of inappropriate secretionSecretionCoagulation Studies of antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia
SNOMED CT
52667002
Syndrome of inappropriate secretionSecretionCoagulation Studies of antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (disorder)
Evaluation & Workup:
These codes are for the essential lab tests to diagnose SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), which involve simultaneous measurement of serum and urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation and electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes to demonstrate inappropriately concentrated urine in the face of low serum osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation.
These codes are for medications used to treat SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). FurosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics can be used with saline to increase free water excretion, while vasopressin receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonists like tolvaptanTolvaptanA benzazepine derivative and selective vasopressin v2 receptor antagonist that is used to treat euvolemic and hypervolemic hyponatremia. It is also used in the treatment of rapidly progressing autosomal dominant polycystic kidney disease to slow the rate of cyst development and renal insufficiency.Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) directly counteract the effect of ADH.
Coding System
Code
Description
RxNorm
4603
FurosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics (ingredient)
RxNorm
486095
TolvaptanTolvaptanA benzazepine derivative and selective vasopressin v2 receptor antagonist that is used to treat euvolemic and hypervolemic hyponatremia. It is also used in the treatment of rapidly progressing autosomal dominant polycystic kidney disease to slow the rate of cyst development and renal insufficiency.Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) (ingredient)
Complications:
This code is for hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, the hallmark and primary complication of SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). Severe or rapidly developing hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia can lead to life-threatening cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP).
Coding System
Code
Description
ICD-10-CM
E87.1
Hypo-osmolality and hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
ICD-10-CM
G93.6
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
References
Jameson, J. L., et al. (Ed.). (2015). Harrison’s Principles of Internal Medicine (20th ed., pp. 299–303, 610, 2281).
Verbalis, J. G. (2019). Posterior pituitary. In Crow, M. K., et al. (Eds.), Goldman-Cecil Medicine (26th ed., vol. 2, pp. 1456–1462).
Qais, A.-A. (2019). Disorders of sodium and water. In Crow, M. K., et al. (Eds.), Goldman-Cecil Medicine (26th ed., vol. 1, pp. 712–723).
Baek, S. H., et al. (2021). Risk of overcorrection in rapid intermittent bolus vs slow continuous infusion therapies of hypertonic saline for patients with symptomatic hyponatremia: the SALSA randomized clinical trial. JAMA Internal Medicine, 181(1), 81–92. https://doi.org/10.1001/jamainternmed.2020.5519
Garrahy, A., et al. (2020). Fluid restriction therapy for chronic SIAD: results of a prospective randomized controlled trial. Journal of Clinical Endocrinology and Metabolism, 105(12), dgaa619. https://doi.org/10.1210/clinem/dgaa619
Mentrasti, G., et al. (2020). Syndrome of inappropriate antidiuretic hormone secretion (SIADH: optimal management. Therapeutics and Clinical Risk Management, 16, 663–672. https://doi.org/10.2147/TCRM.S206066
Adrogué, H. J., Tucker, B. M., Madias, N. E. (2022). Diagnosis and management of hyponatremia: a review. JAMA, 328(3), 280–291. https://doi.org/10.1001/jama.2022.11176
Arora, N., Jefferson, J. A. (2023). Electrolyte & acid-base disorders. In Papadakis, M.A., et al. (Eds.), Current Medical Diagnosis & Treatment (62nd ed., pp. 879–880).
Ball, S., Barth, J., Levy, M., Society for Endocrinology Clinical Committee. (2016). Society for Endocrinology Endocrine Emergency Guidance: emergency management of severe symptomatic hyponatraemia in adult patients. Endocrine Connections, 5(5), G4–G6. https://ec.bioscientifica.com/view/journals/ec/5/5/G4.xml
Vaidya, C., Ho, W., Freda, B. J. (2010). Management of hyponatremia: providing treatment and avoiding harm. Cleveland Clinic Journal of Medicine, 77(10): 715–726. https://www.ccjm.org/content/ccjom/77/10/715.full.pdf
Spasovski, G., et al. (2014). Clinical practice guideline on diagnosis and treatment of hyponatremia. European Journal of Endocrinology, 170, G1–G47. https://doi.org/10.1530/EJE-13-1020