Botulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum(C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism presents with blurred vision, respiratory failure, and symmetric, descending flaccid paralysis. Characterization includes intact sensorium, normal heart rate and blood pressure, absence of fever, and absence of sensory deficits. Diagnosis is made on clinical grounds and can be confirmed by the isolation of bacteria or toxins from stool, wound specimens, or food sources. The approach to managing a case of botulism should include prompt management of respiratory failure, administration of antitoxin, and supportive care for paralysis.
BotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism is a rare, neuroparalytic syndrome caused by the bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. BacteriologyClostridium botulinumClostridium botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia (C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia), which releases a fatal neurotoxin (botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism), resulting in varying degrees of muscle paralysis and distinct clinical syndromes.
Epidemiology[1–4]
Approximately 110 cases per year in the US (rare disease)
Can occur in any age group
No person-to-person transmission
C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridiais found in soil and marine sediments worldwide.
The most common types are foodborne and infantile botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism.
The least common type is adult intestinal toxemiaAdult Intestinal ToxemiaBotulism (adult intestinal colonizationColonizationBacteriologybotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism).
Etiology[1–4]
Pathogen C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia:
Gram-positiveGram-PositivePenicillinsbacillusBacillusBacillus are aerobic, spore-forming, gram-positive bacilli. Two pathogenic species are Bacillus anthracis (B. anthracis) and B. cereus. Bacillus
Anaerobic, spore-forming bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology
Found in soil and marine sediments worldwide
4 distinct phenotypic groups: I–IV (group I causes most adult human cases)
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism:
Neurotoxic protein produced by C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia
Classified into 7 serotypes: A–G
A, B, E, and F cause disease in humans.
A and B are used commercially and medically.
Blocks the release of the neurotransmitter acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS (AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS) at the neuromuscular junctionNeuromuscular junctionThe synapse between a neuron and a muscle.Skeletal Muscle Contraction (NMJ)
Conditions favorable for pathogen growth and sporeSporeThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Microsporidia/Microsporidiosis formation:
Low O2 or no O2 (anaerobic conditions)
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance of > 4.5 (ideal is 7 and above)
Ideal temperature range: 25℃–37℃
Survive in temperatures as low as 4℃
Survive 100℃ (heatHeatInflammation resistant sporesSporesThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Anthrax) for at least 5 hours (destruction requires 120℃ for 5 minutes)
Mode of infection: ingestion of C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.ClostridiasporesSporesThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Anthrax
The toxin is produced in vivo (bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology germinate in the GI tract).
Typically occurs in infants < 6 months of age (natural defenses have not yet developed in the intestine)
Mode of infection: ingestion of food contaminated with C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridiatoxin
Commonly found in inadequately canned foods with low-acid content and lightly preserved food products (e.g., fermented, salted, or smoked meat/fishFISHA type of in situ hybridization in which target sequences are stained with fluorescent dye so their location and size can be determined using fluorescence microscopy. This staining is sufficiently distinct that the hybridization signal can be seen both in metaphase spreads and in interphase nuclei.Chromosome Testing products)
Dangerous: may infect many people at once who consume food from the same source
Mode of infection: SporesSporesThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Anthrax of C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia enter an open wound and thrive under anaerobic conditions.
Rare form of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism
Can result from contamination of the wound by soil, gravel, or inappropriately treated open fractures
Commonly associated with substance abuse of black tar heroinHeroinA narcotic analgesic that may be habit-forming. It is a controlled substance (opium derivative) listed in the U.S. Code of federal regulations, title 21 parts 329. 1, 1308. 11 (1987). Sale is forbidden in the United States by federal statute.Nephrotic Syndrome
Mode of infection: botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism injections for cosmetic or therapeutic/medical purposes (e.g., migraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine Headache, contracturesContracturesProlonged shortening of the muscle or other soft tissue around a joint, preventing movement of the joint.Wound Healing, spasticitySpasticitySpinal Disk Herniation)
Another rare form of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism
Mode of infection: ingestion of sporesSporesThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Anthrax of C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia
Least common form of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism
Similar to infantile botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism but occurs in older children and adults with bowel abnormalities or disruption of the normal intestinal flora (e.g., inflammatory bowel disease)
Inhalation botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism[2–4]
Does not occur naturally
Associated with the accidental or intentional release of toxin in aerosolsAerosolsColloids with a gaseous dispersing phase and either liquid (fog) or solid (smoke) dispersed phase; used in fumigation or in inhalation therapy; may contain propellant agents.Coxiella/Q Fever (bioterrorismBioterrorismThe use of biological agents in terrorism. This includes the malevolent use of bacteria; viruses; or other biological toxins against people, animals; or plants.Anthrax associated botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism)
The means of exposure to the toxin will determine the type of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism; the toxin is not absorbed through intact skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.[3,4]
Exposure can occur through the following mechanisms:
Ingestion of preformed toxin
Inhalation of preformed toxin
Production of toxin by C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia in the GI tract
Production of toxin byC. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia in devitalized tissue at the site of a wound
Exposure to the toxin by injection for cosmetic or therapeutic/medical purposes
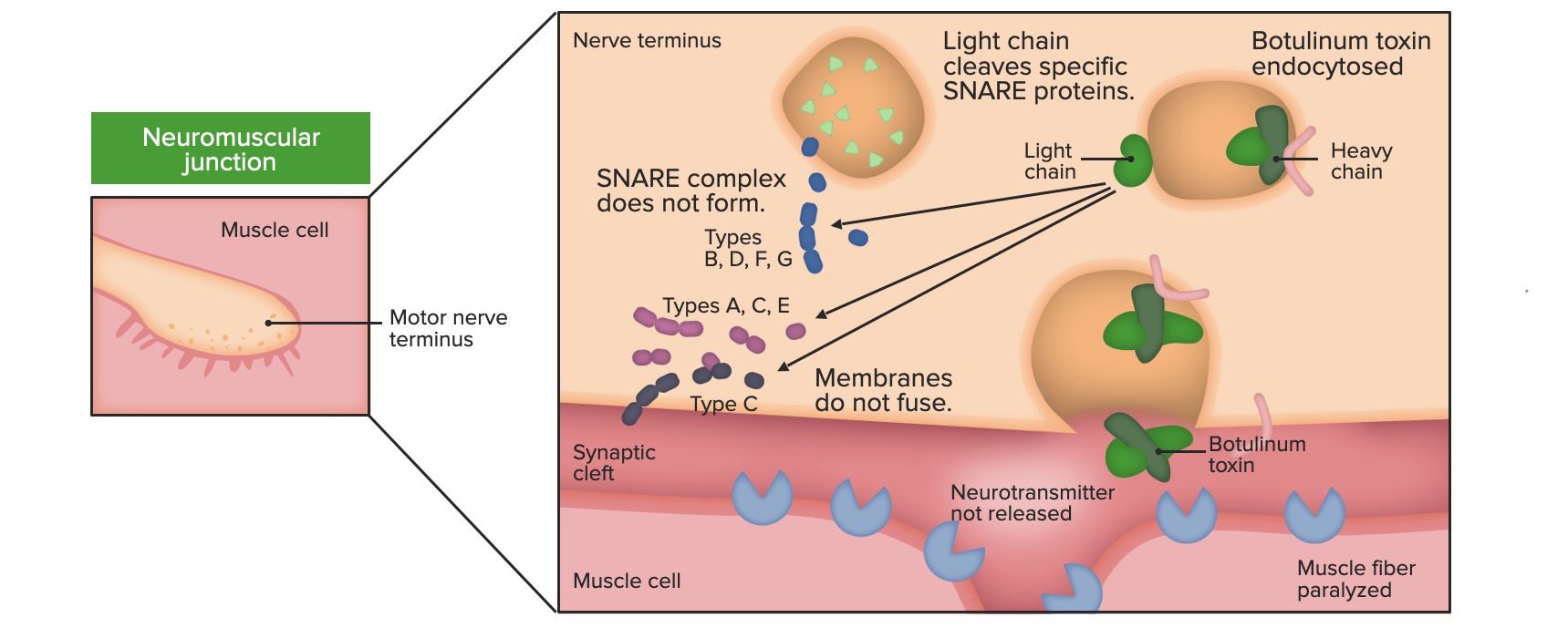
Mechanism of pathogenesis:
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism is activated by bacterial proteasesProteasesProteins and Peptides which cleave the precursor polypepetide chain; the toxin is then transported to the neuromuscular junctionNeuromuscular junctionThe synapse between a neuron and a muscle.Skeletal Muscle Contraction (NMJ).
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism exists in the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment as a polymer of a light chain and a heavy chain.
The heavy chain of the toxin binds to receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors on the presynaptic neuronPresynaptic neuronSynapses and Neurotransmission and enters the presynaptic neuronPresynaptic neuronSynapses and Neurotransmission via receptor-mediated endocytosisEndocytosisCellular uptake of extracellular materials within membrane-limited vacuoles or microvesicles. Endosomes play a central role in endocytosis.The Cell: Cell Membrane.
Once in the cytoplasm, the light chain binds SNARE/SNAP proteinsSNAP proteinsA superfamily of small proteins which are involved in the membrane fusion events, intracellular protein trafficking and secretory processes. They share a homologous snare motif. The snare proteins are divided into subfamilies: qa-snares; qb-snares; qc-snares; and r-snares. The formation of a snare complex (composed of one each of the four different types snare domains (qa, qb, qc, and r)) mediates membrane fusion. Following membrane fusion snare complexes are dissociated by the nsfs (n-ethylmaleimide-sensitive factors), in conjunction with soluble nsf attachment protein, i.e., snaps (no relation to snap 25).Botulism, which are involved in the release of AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS from the presynaptic vesiclesVesiclesFemale Genitourinary Examination where it is stored.
The inhibition of AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS release prevents AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS from binding to the AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNSreceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors, which halts muscle contraction and leads to weakness/paralysis.
Effect of botulinum toxin at the level of the NMJ: inhibition of ACh release
The classic presentation of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism includes symmetric cranial nerve palsiesCranial Nerve PalsiesCranial nerve palsy is a congenital or acquired dysfunction of 1 or more cranial nerves that will, in turn, lead to focal neurologic abnormalities in movement or autonomic dysfunction of its territory. Head/neck trauma, mass effect, infectious processes, and ischemia/infarction are among the many etiologies for these dysfunctions. Diagnosis is initially clinical and supported by diagnostic aids. Management includes both symptomatic measures and interventions aimed at correcting the underlying cause.Cranial Nerve Palsies and descending paralysisDescending ParalysisBotulism. The 5 key features of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism include:
Absence of feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Symmetric, descending flaccid paralysis of voluntary muscles:
Often starts with ocular, bulbar, and facial musclesFacial musclesThe facial muscles (also called mimetic muscles) control facial expression and are supplied by the facial nerve. Most of them originate from the skull and attach to the skin around the facial openings, which serve as a method to group or classify them.Facial Muscles: Anatomy
Progress downward to involve the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess, upper extremities and trunk
Ultimately lead to respiratory weakness and difficulty breathing
Eventually affect the lower extremities
Intact sensorium and mental status
Normal or slow heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology and normal blood pressure
Dysphagia (difficulty swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility)
BotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism also presents with autonomic findings:
Pupillary (dilated, fixed pupils)
Reduced salivation (dry mouth)
Reduced lacrimation (dry eyes)
Paralytic ileusParalytic ileusSmall Bowel Obstruction/severe constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Gastric dilatation
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess distention/urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Orthostatic hypotensionOrthostatic hypotensionA significant drop in blood pressure after assuming a standing position. Orthostatic hypotension is a finding, and defined as a 20-mm hg decrease in systolic pressure or a 10-mm hg decrease in diastolic pressure 3 minutes after the person has risen from supine to standing. Symptoms generally include dizziness, blurred vision, and syncope.Hypotension
IncubationIncubationThe amount time between exposure to an infectious agent and becoming symptomatic.Rabies Virus period: 3–30 days after sporeSporeThe reproductive elements of lower organisms, such as bacteria; fungi; and cryptogamic plants.Microsporidia/Microsporidiosis entry
Typically occurs in infants < 6 months of age
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation: often the 1st sign
General weakness/lethargyLethargyA general state of sluggishness, listless, or uninterested, with being tired, and having difficulty concentrating and doing simple tasks. It may be related to depression or drug addiction.Hyponatremia
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures (rare, but can occur with hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage due to respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure)
An important presentation in infant botulism: floppy baby syndrome
IncubationIncubationThe amount time between exposure to an infectious agent and becoming symptomatic.Rabies Virus period: 12–36 hours after toxin consumption
In addition to the typical disease features, prodromal symptoms are common:
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, and abdominal crampsCrampsIon Channel Myopathy
Initial diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea (thought to be from local toxin effect in GI endotheliumEndotheliumA layer of epithelium that lines the heart, blood vessels (vascular endothelium), lymph vessels (lymphatic endothelium), and the serous cavities of the body.Arteries: Histology or early autonomic dysfunctionAutonomic DysfunctionAnterior Cord Syndrome) progresses to constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation (as systemic NMJ manifestations dominate).
IncubationIncubationThe amount time between exposure to an infectious agent and becoming symptomatic.Rabies Virus period difficult to estimate (timing of exposure usually uncertain), but likely longer than that for foodborne disease
Symptoms are similar to foodborne botulismFoodborne BotulismBotulism (including typical features), except:
Prodromal symptoms are absent.
Wound botulismWound BotulismBotulismpresents with feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever and leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus in around 50% of cases
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation at the site of the wound
Ptosis in a child with botulism: The patient is alert and oriented.
Image: “Botulism1and2” by Herbert L. Fred, MD and Hendrik A. van Dijk. License: CC BY 2.0
Other forms of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism[2–4]
After injection of botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism for cosmetic or therapeutic/medical purposes
Inhalation botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism:
Typical features are generally present.
Can develop early (short incubationIncubationThe amount time between exposure to an infectious agent and becoming symptomatic.Rabies Virus period) and quickly progress to respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
In many cases, a presumptive diagnosis of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism may be made with history and physical exam alone. Clinical pearl: Consider botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism in the differential diagnosis when also considering myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis or Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome.
History[2,4–7]
Consumption of canned foods (especially foods canned at home)
Similar symptoms in individuals with similar exposure
History of injectable drug abuse
History of cosmetic/medical use of botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism
Absence of feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Alert and conscious patient with neurologic symptoms
May be intact initially (different from Guillain-Barré)
Diminished when the associated muscle groups are paralyzed
No ticksTicksBlood-sucking acarid parasites of the order ixodida comprising two families: the softbacked ticks (argasidae) and hardbacked ticks (ixodidae). Ticks are larger than their relatives, the mites. They penetrate the skin of their host by means of highly specialized, hooked mouth parts and feed on its blood. Ticks attack all groups of terrestrial vertebrates. In humans they are responsible for many tick-borne diseases, including the transmission of rocky mountain spotted fever; tularemia; babesiosis; african swine fever; and relapsing fever.Coxiella/Q Fever identified on a dedicated “tick check”
Laboratory, imaging, and other diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests[2,4–7]
Confirmatory tests to identify/isolate C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia or its toxin:
Mouse bioassay (gold standard):
Can detect toxin in serum, stool, gastric fluid, or a food source (10 to 20 g)
Mice are injected with the sample and followed for symptoms.
Results typically available in 24‒48 hours.
May not detect low levels of toxin.
Isolation of C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia via anaerobic culture:
From stool, wound specimen, or food source
Results can take up to 6 days.
ELISAELISAAn immunoassay utilizing an antibody labeled with an enzyme marker such as horseradish peroxidase. While either the enzyme or the antibody is bound to an immunosorbent substrate, they both retain their biologic activity; the change in enzyme activity as a result of the enzyme-antibody-antigen reaction is proportional to the concentration of the antigen and can be measured spectrophotometrically or with the naked eye. Many variations of the method have been developed.St. Louis Encephalitis Virus or PCRPCRPolymerase chain reaction (PCR) is a technique that amplifies DNA fragments exponentially for analysis. The process is highly specific, allowing for the targeting of specific genomic sequences, even with minuscule sample amounts. The PCR cycles multiple times through 3 phases: denaturation of the template DNA, annealing of a specific primer to the individual DNA strands, and synthesis/elongation of new DNA molecules.Polymerase Chain Reaction (PCR) detection of toxin:
In serum, stool, gastric fluid, or food source
Results can take 1‒4 days.
Testing can be performed only in specific labs (typically, public health labs).
Note: Because there is a delay in obtaining results, antitoxin should be administered based on a presumptive clinical diagnosis (rather than waiting for confirmatory results).
Other tests:
MRI or CT: to rule out other reasons for neurologic symptoms (e.g., stroke)
Serum testing for autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques against the acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNSreceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors: typically present in myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis
CSF exam:[5]
CSF exam is typically normal in botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism.
↑ Protein concentrations often present in Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome
ElectromyographyElectromyographyRecording of the changes in electric potential of muscle by means of surface or needle electrodes.Becker Muscular Dystrophy (EMG):[5]
Can differentiate botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism from Lambert-Eaton syndrome
Findings in botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism may include:
To rule out myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis
Not conducted at present (unavailable in the US) because of a high occurrence of false positiveFalse positiveAn FP test result indicates that a person has the disease when they do not.Epidemiological Values of Diagnostic Tests results
CDC criteria for suspecting botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism[5,8]
The following criteria were developed by the US Centers for Disease Control and Prevention (CDC). In a crisis setting, these criteria may be used alone to make a presumptive diagnosis of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism and to administer antitoxin. In standard settings, a more detailed evaluation (with the testing outlined above) should be completed.
Suspect botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism when all 3 of the following criteria are metMETPreoperative Care:
DiplopiaDiplopiaA visual symptom in which a single object is perceived by the visual cortex as two objects rather than one. Disorders associated with this condition include refractive errors; strabismus; oculomotor nerve diseases; trochlear nerve diseases; abducens nerve diseases; and diseases of the brain stem and occipital lobe.Myasthenia Gravis
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia, pooling of secretions, or droolingDroolingPeritonsillar Abscess
Thick tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy
Extraocular palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies/fatigability: seen as the inability to avert eyes when a light is shone repeatedly into the eye (used for infants)
Facial paresisParesisA general term referring to a mild to moderate degree of muscular weakness, occasionally used as a synonym for paralysis (severe or complete loss of motor function). In the older literature, paresis often referred specifically to paretic neurosyphilis. ‘general paresis’ and ‘general paralysis’ may still carry that connotation. Bilateral lower extremity paresis is referred to as paraparesis.Spinal Disk Herniation, which may be seen as:
Loss of facial expression
Pooling of secretions
In young children: poor feeding/fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia while eating, poor sucking on breast or pacifier
Descending paralysisDescending ParalysisBotulism, beginning with cranial nervesCranial nervesThere are 12 pairs of cranial nerves (CNs), which run from the brain to various parts of the head, neck, and trunk. The CNs can be sensory or motor or both. The CNs are named and numbered in Roman numerals according to their location, from the front to the back of the brain.The 12 Cranial Nerves: Overview and Functions
Management may vary based on practice location. The following information is based on US and UK guidelines.
A detailed clinical history and diagnosis are important in botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism, as the tests take time. If a case history is highly suggestive of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism, treatment should not be delayed.
General approach[5–7]
Notify public health officials if botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism is suspected.[5,6]
HospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium, with frequent serial examinations focusing on:
Development/progression of cranial nerve palsiesCranial Nerve PalsiesCranial nerve palsy is a congenital or acquired dysfunction of 1 or more cranial nerves that will, in turn, lead to focal neurologic abnormalities in movement or autonomic dysfunction of its territory. Head/neck trauma, mass effect, infectious processes, and ischemia/infarction are among the many etiologies for these dysfunctions. Diagnosis is initially clinical and supported by diagnostic aids. Management includes both symptomatic measures and interventions aimed at correcting the underlying cause.Cranial Nerve Palsies
Ability to swallow
Extremity strength
Respiratory status
Monitor for signs of respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure:
Mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing can allow most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship to survive even without antitoxin (though it typically requires prolonged intensive care resources for weeks to months).[5]
For supportive care, provide nasogastric feeding in small amounts to prevent aspiration.
Administration of antitoxin
If botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism is suspected, contact local public health office for consultation and to acquire antitoxin.
Do not delay antitoxin administration while awaiting definitive diagnosis (should be given as soon as possible).
Antitoxin
Antitoxin is the mainstay of botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism treatment.
The antitoxin cannot reverse paralysis but can prevent paralysis progression.
Antitoxin administration within 24 hours after the onset of symptoms is preferred.
Local health department specialists can/should assist in dosing, since dosing varies based on the strength of the antitoxin available (which can vary by country).
Two major forms are available in the United States and elsewhere:
Heptavalent botulinum antitoxinBotulinum antitoxinAntiserum given therapeutically in botulism.Botulism(HBAT):[5,9]
Equine serum heptavalent antitoxin: contains antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against 7 types of botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism (A‒G)
Binds to and neutralizes circulating neurotoxins in the blood → prevents NMJ binding
Adults ≥ 17 years of age:
1 vial, IV infusion to start at 0.5 mL/min
Rate may be doubled every 30 minutes, if tolerated, to a maximum infusion rate of 2 mL/min.
Children 1–17 years of age:
20%–100% of the adult dose
IV infusion of 0.01 mL/kg/min
May increase by 0.01 mL/kg/min every 30 minutes, to a maximum infusion rate of 0.03 mL/kg/min (not to exceed maximum adult rate of 2 mL/min)
Infants < 1 year of age:
10% of the adult dose
IV infusion of 0.01 mL/kg/min
May increase by 0.01 mL/kg/min every 30 minutes, to a maximum infusion rate of 0.03 mL/kg/min
AnaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction is an adverse effect:
Rate of anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction: 1%–2%
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions testing before administration is not recommended by the CDC.
Human botulinum immunoglobulin (BIG-IV or BabyBIG):[10]
Preferred treatment (and only indicated) for infants < 1 year diagnosed with infant botulismInfant BotulismBotulism
No serious adverse effects have been reported yet.
Dosing:
1.0 mL/kg (50 mg/kg) IV infusion
Begin at 0.5 mL/kg/hr, and increase to 1.0 mL/kg/hr if no adverse reactions after 15 minutes.
Type-specific therapy[5–7]
Foodborne botulismFoodborne BotulismBotulism: In the absence of ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction, laxativesLaxativesLaxatives are medications used to promote defecation. Most often, laxatives are used to treat constipation or for bowel preparation for certain procedures. There are 4 main classes of laxatives: bulk-forming, stimulant, osmotic, and emollient. Laxatives and enemas can be considered to eliminate the toxin and relieve constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation.
Strictly avoid antibiotics in infant (and adult intestinal) botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism → lysis of bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology releases additional toxins, which can then be absorbed and worsen symptoms
Extensive debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome of the wound is important.
If ≥ 5 years since the last immunization, tetanusTetanusTetanus is a bacterial infection caused by Clostridium tetani, a gram-positive obligate anaerobic bacterium commonly found in soil that enters the body through a contaminated wound. C. tetani produces a neurotoxin that blocks the release of inhibitory neurotransmitters and causes prolonged tonic muscle contractions. Tetanus boosters are considered.
PenicillinPenicillinRheumatic Fever G and metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess are the preferred antibiotics for mixed infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease.
PenicillinPenicillinRheumatic Fever G: 18–20 million units/day IV in divided doses every 4–6 hours (e.g., 3 million units every 4 hours)
MetronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess: 500 mg IV every 8 hours
AminoglycosidesAminoglycosidesAminoglycosides are a class of antibiotics including gentamicin, tobramycin, amikacin, neomycin, plazomicin, and streptomycin. The class binds the 30S ribosomal subunit to inhibit bacterial protein synthesis. Unlike other medications with a similar mechanism of action, aminoglycosides are bactericidal. Aminoglycosides, polymyxins, and tetracyclineTetracyclineA naphthacene antibiotic that inhibits amino Acyl tRNA binding during protein synthesis.Drug-Induced Liver Injury are avoided (may induce neuromuscular blockadeNeuromuscular BlockadeThe intentional interruption of transmission at the neuromuscular junction by external agents, usually neuromuscular blocking agents. It is distinguished from nerve block in which nerve conduction (neural conduction) is interrupted rather than neuromuscular transmission. Neuromuscular blockade is commonly used to produce muscle relaxation as an adjunct to anesthesia during surgery and other medical procedures. It is also often used as an experimental manipulation in basic research. It is not strictly speaking anesthesia but is grouped here with anesthetic techniques. The failure of neuromuscular transmission as a result of pathological processes is not included here.Aminoglycosides).
Experimental therapies
No current evidence for the effectiveness of treatments other than antitoxin[5]
PyridostigminePyridostigmineA cholinesterase inhibitor with a slightly longer duration of action than neostigmine. It is used in the treatment of myasthenia gravis and to reverse the actions of muscle relaxants.Cholinomimetic Drugs and/or guanidine induce the release of AChAChA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS at the NMJ.
PlasmapheresisPlasmapheresisProcedure whereby plasma is separated and extracted from anticoagulated whole blood and the red cells retransfused to the donor. Plasmapheresis is also employed for therapeutic use.Stevens-Johnson Syndrome
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure is the major cause of death in botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism.
Diaphragmatic controlled breathing: maintains the respiratory cycle
Pursed lip breathing: improves gas mixing at rest and prevents prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing EnterocolitisairwayAirwayABCDE Assessment collapse
Range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs exercises: keeps the joints moving and retains muscle function
Strengthening exercises: maintains function in the muscles
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[7]
Most strength can be recovered within the 1st 3 months.
Long-term consequences can include:
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia and weakness
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea on exertion
Impaired psychosocial well-being
Prevention[7]
Avoid feeding infants honey until ≥ 12 months of age.
Use good home-canning techniques.
Bulging food containers may indicate contamination (due to gas produced by C. botulinumC. botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia).
HeatHeatInflammation contaminated foods to ≥ 85°C for ≥ 5 minutes.
Differential Diagnosis
Myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis: an autoimmune neuromuscular disorder characterized by varying degrees of muscle weakness in the arms and legs. Presentation also includes ptosisPtosisCranial Nerve Palsies, dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia, fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, and breathlessness. Diagnosis is through a Tensilon test and specific antibody detection. Myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis is managed medically with steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors and surgically by thymectomyThymectomySurgical removal of the thymus gland.Myasthenia Gravis.
Lambert-Eaton syndrome: an autoimmune neuromuscular syndrome often associated with small cell lung carcinoma. Symptoms include ptosisPtosisCranial Nerve Palsies, dry mouth, bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and bowel changes, erectile dysfunctionErectile DysfunctionErectile dysfunction (ED) is defined as the inability to achieve or maintain a penile erection, resulting in difficulty to perform penetrative sexual intercourse. Local penile factors and systemic diseases, including diabetes, cardiac disease, and neurological disorders, can cause ED. Erectile Dysfunction, paresthesia, and weakness of muscles, which is temporarily relieved on exertion. Diagnosis includes antibody detection, EMG, X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests, and lung CT. Treatment includes resolving the underlying cause and immunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants.
Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome: a disorder of the peripheral nervous systemPeripheral nervous systemThe nervous system outside of the brain and spinal cord. The peripheral nervous system has autonomic and somatic divisions. The autonomic nervous system includes the enteric, parasympathetic, and sympathetic subdivisions. The somatic nervous system includes the cranial and spinal nerves and their ganglia and the peripheral sensory receptors.Nervous System: Anatomy, Structure, and Classification triggered by an acute bacterial or viral infection. Presentation includes initial paresthesia in the feet and legs with progression to ascending paralysis. Additional symptoms include walking abnormalities, fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children, hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, and urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium. Diagnosis is by CSF analysisCSF analysisMeningitis, EMG, and nerve conduction studies. Guillain-Barré syndromeGuillain-Barré syndromeGuillain-Barré syndrome (GBS), once thought to be a single disease process, is a family of immune-mediated polyneuropathies that occur after infections (e.g., with Campylobacter jejuni).Guillain-Barré Syndrome is managed with plasmapheresisPlasmapheresisProcedure whereby plasma is separated and extracted from anticoagulated whole blood and the red cells retransfused to the donor. Plasmapheresis is also employed for therapeutic use.Stevens-Johnson Syndrome and immunoglobulin therapy, analgesics, blood thinners, and physiotherapyPhysiotherapySpinal Stenosis.
Stroke: a medical emergency causing damage to the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification due to interrupted blood supply. Presentation includes headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, dysarthriaDysarthriaDisorders of speech articulation caused by imperfect coordination of pharynx, larynx, tongue, or face muscles. This may result from cranial nerve diseases; neuromuscular diseases; cerebellar diseases; basal ganglia diseases; brain stem diseases; or diseases of the corticobulbar tracts. The cortical language centers are intact in this condition.Wilson Disease, blurred visionBlurred VisionRetinal Detachment, facial paralysis, and numbness of the face, arms, and legs. Stroke is diagnosed by physical exam, CT, MRI, cerebral angiogram, or carotid ultrasound. Management depends on the type of stroke (ischemic or hemorrhagic).
Tick paralysis: occurs due to injection of toxin by the bite of a tick. Symptoms occur within 2–7 days. Clinical presentation includes initial numbness and weakness in both legs with progression to ascending paralysis and respiratory distress within hours. Deep tendon reflexesDeep Tendon ReflexesNeurological Examination are decreased or absent. Diagnosis is based on symptoms and finding an embedded tick (usually on the scalp). The disease is managed by detecting and removing the tick, cleaning the site of the bite, and monitoring for respiratory distress.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism, a rare but serious paralytic illness caused by a nerve toxin produced by the bacterium Clostridium botulinumClostridium botulinumA species of anaerobic, gram-positive, rod-shaped bacteria in the family clostridiaceae that produces proteins with characteristic neurotoxicity. It is the etiologic agent of botulism in humans, wild fowl, horses; and cattle. Seven subtypes (sometimes called antigenic types, or strains) exist, each producing a different botulinum toxin (botulinum toxins). The organism and its spores are widely distributed in nature.Clostridia.
Coding System
Code
Description
ICD-10-CM
A05.1
BotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism
SNOMED CT
243050004
BotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism (disorder)
Medications:
This CPT code is for the administration of the botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism antitoxin, the critical, life-saving treatment for botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism that neutralizes the circulating toxin and prevents further progression of paralysis.
Coding System
Code
Description
CPT
90287
BotulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism antitoxin, equine, any route
Complications:
This code is for acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure, the most common cause of death in botulismBotulismBotulism is a rare, neuroparalytic syndrome caused by Clostridium botulinum (C. botulinum). A fatal neurotoxin (botulinum toxin) is released causing varying degrees of muscle paralysis and distinct clinical syndromes. The most common types of botulism are foodborne and infant. Botulism, which occurs when the paralysis affects the muscles of respirationRespirationThe act of breathing with the lungs, consisting of inhalation, or the taking into the lungs of the ambient air, and of exhalation, or the expelling of the modified air which contains more carbon dioxide than the air taken in.Nose Anatomy (External & Internal), necessitating mechanical ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing.
Coding System
Code
Description
ICD-10-CM
J96.00
Acute respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure, unspecified whether with hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage or hypercapniaHypercapniaA clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood.Neonatal Respiratory Distress Syndrome
Jameson, J. L., Fauci, A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., Loscalzo, J. (2018). Diseases caused by gram-positive bacteria. In: Harrison’s Principles of Internal Medicine (20th ed.). McGraw-Hill Education. accessmedicine.mhmedical.com/content.aspx?aid=1190790657
Rao, A. K. (2021). Clinical guidelines for diagnosis and treatment of botulism, 2021. CDC Morbidity and Mortality Weekly Report Recommendations and Reports, 70(2), 1‒30. https://doi.org/10.15585/mmwr.rr7002a1
Rao, A. K., Lin, N. H., Griese, S. E., et al. (2018). Clinical criteria to trigger suspicion for botulism: an evidence-based tool to facilitate timely recognition of suspected cases during sporadic events and outbreaks. Clinical Infectious Diseases, 66(suppl_1), S38–S42. https://doi.org/10.1093/cid/cix814
Cangene Corporation: emergent biosolutions. (2017). Botulism antitoxin heptavalent [A, B, C, D, E, F, G—equine] [package insert]. Retrieved on October 24, 2022, from https://www.fda.gov/media/85514/download