Normal placental structure and function are essential for a healthy pregnancy. Placental abnormalities can be classified as structural anomalies (such as a succenturiate lobe or velamentous cord insertion), implantationImplantationEndometrial implantation of embryo, mammalian at the blastocyst stage.Fertilization and First Week anomalies (such as placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity accreta and placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa), and functional anomalies (such as placental insufficiencyPlacental InsufficiencyFailure of the placenta to deliver an adequate supply of nutrients and oxygen to the fetus.Neonatal Polycythemia). The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is typically seen well on ultrasound, and placental assessment is part of routine antenatal screeningScreeningPreoperative Care, which is when most structural and implantationImplantationEndometrial implantation of embryo, mammalian at the blastocyst stage.Fertilization and First Week anomalies are identified. Because of the extensive maternal and fetal circulationFetal circulationPrenatal and Postnatal Physiology of the Neonate through the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity, placental abnormalities can significantly increase the risk of serious antepartum or postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage. Placental abnormalities also frequently impact decisions regarding the timing and route of delivery.
The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is an important structure for fetal growth and development during embryonic and fetal life. Abnormalities in its structure, function, or implantationImplantationEndometrial implantation of embryo, mammalian at the blastocyst stage.Fertilization and First Week can result in serious and potentially fatal complications for both the fetus and mother.
Placental structure and circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment
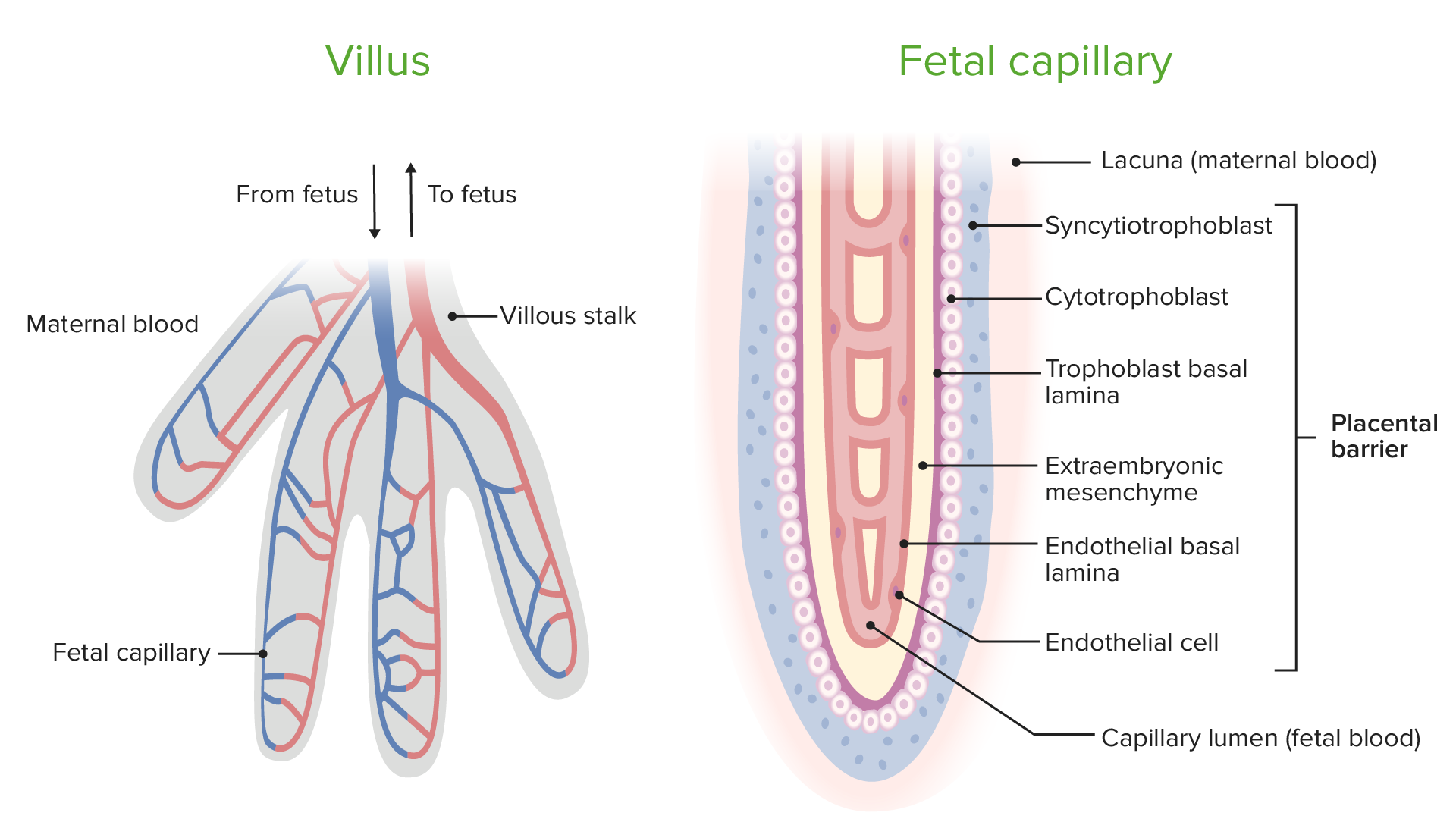
Chorionic villiChorionic villiThreadlike vascular projections of the chorion. Chorionic villi may be free or embedded within the decidua forming the site for exchange of substances between fetal and maternal blood (placenta).Placenta, Umbilical Cord, and Amniotic Cavity provide a large surface area for maternal-fetal exchange.
Spiral arteriesSpiral arteriesPlacenta, Umbilical Cord, and Amniotic Cavity (maternal) fill the intervillous spaces in the decidua basalis layer of the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development:
Do not have the ability to regulate blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure through the organ
2 umbilical arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology bring deoxygenated blood from the fetus to the placental chorionic villiChorionic villiThreadlike vascular projections of the chorion. Chorionic villi may be free or embedded within the decidua forming the site for exchange of substances between fetal and maternal blood (placenta).Placenta, Umbilical Cord, and Amniotic Cavity.
Fetal hemoglobin has ↑ affinity for O2 compared with maternal hemoglobin → causes O2 to move from maternal RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology to fetal RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology
Umbilical veinumbilical veinVenous vessels in the umbilical cord. They carry oxygenated, nutrient-rich blood from the mother to the fetus via the placenta. In humans, there is normally one umbilical vein.Prenatal and Postnatal Physiology of the Neonate transports oxygenated blood back to the fetus.
Maternal veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology carry deoxygenated blood back to the maternal circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment.
Maternal and fetal blood never come into direct contact.
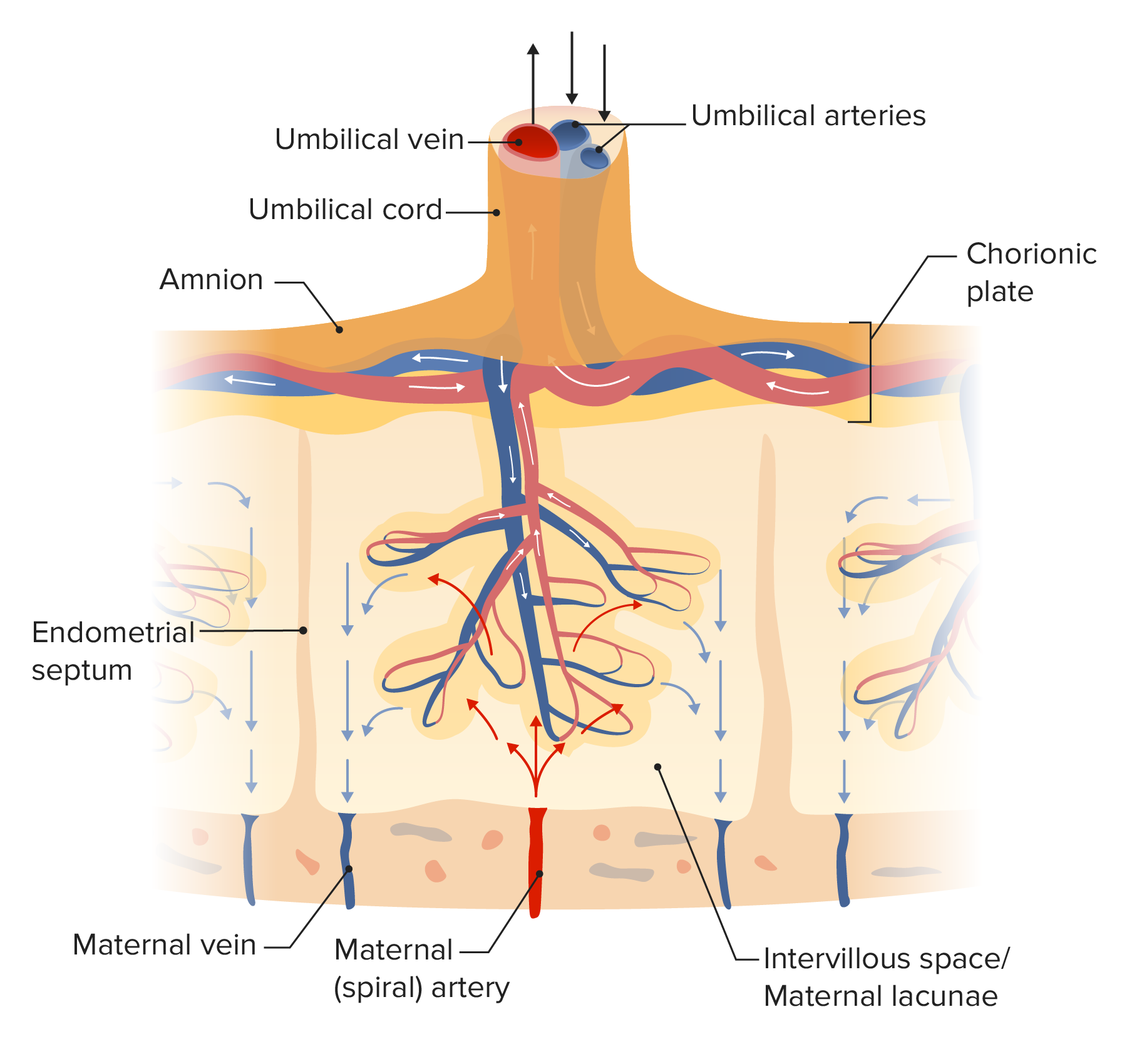
Diagram of placental circulation:
Maternal spiral arteries bring oxygenated blood into the placenta. In the areas surrounding the chorionic villi, the spiral arteries “rupture” and blood circulates through the spaces, which are known as maternal lacunae. Deoxygenated fetal blood enters the placenta through the umbilical arteries. The blood circulates through the chorionic villi. Gas and molecule exchange occurs between maternal blood in the lacunae and fetal blood in the chorionic villi. Oxygenated fetal blood leaves the placenta through the umbilical vein, while deoxygenated maternal blood leaves through the maternal vein. Maternal and fetal blood never directly mix.
Functions of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity
Gas exchangeGas exchangeHuman cells are primarily reliant on aerobic metabolism. The respiratory system is involved in pulmonary ventilation and external respiration, while the circulatory system is responsible for transport and internal respiration. Pulmonary ventilation (breathing) represents movement of air into and out of the lungs. External respiration, or gas exchange, is represented by the O2 and CO2 exchange between the lungs and the blood.Gas Exchange (O2 and CO2)
Nutrient exchange
Fetal waste removal
Hormone production (a fetal and maternal endocrine organ during pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care):
hCG
Human placental lactogen (hPL)
Placental growth hormone (PGH)
Chorionic corticotropin-releasing hormoneCorticotropin-releasing hormoneA peptide of about 41 amino acids that stimulates the release of adrenocorticotropic hormone. Crh is synthesized by neurons in the paraventricular nucleus of the hypothalamus. After being released into the pituitary portal circulation, crh stimulates the release of acth from the pituitary gland. Crh can also be synthesized in other tissues, such as placenta; adrenal medulla; and testis.Hypothalamic and Pituitary Hormones (CRH)
ProgesteroneProgesteroneThe major progestational steroid that is secreted primarily by the corpus luteum and the placenta. Progesterone acts on the uterus, the mammary glands and the brain. It is required in embryo implantation; pregnancy maintenance, and the development of mammary tissue for milk production. Progesterone, converted from pregnenolone, also serves as an intermediate in the biosynthesis of gonadal steroid hormones and adrenal corticosteroids.Gonadal Hormones
Estrogens
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Assists in protection of the fetus from maternal immunologic rejection
Overview of normal and abnormal placental implantationImplantationEndometrial implantation of embryo, mammalian at the blastocyst stage.Fertilization and First Week
Early fetal trophoblastic cells invade into the maternal decidua basalis layer of the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development:
Trophoblastic cells should not invade into the myometrium beneath the endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development.
When trophoblastic cells do invade into the myometrium, the condition is called placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity accreta.
Placentas typically implant in the fundal region of the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy:
The placental edge should be away from the internal cervical os.
When the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity covers the internal cervical os, the condition is called placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa.
When the placental edge is within 2 cm of the cervical os, it is called a low-lying placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity.
The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity shouldremain connected to the maternal endometriumEndometriumThe mucous membrane lining of the uterine cavity that is hormonally responsive during the menstrual cycle and pregnancy. The endometrium undergoes cyclic changes that characterize menstruation. After successful fertilization, it serves to sustain the developing embryo.Embryoblast and Trophoblast Development, providing O2 and nutrients, until after the delivery of the infant.
When the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity separates early, the condition is called placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage.
When the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity fails to provide adequate O2 or nutrients to the fetus, the condition is called placental insufficiencyPlacental InsufficiencyFailure of the placenta to deliver an adequate supply of nutrients and oxygen to the fetus.Neonatal Polycythemia.
Structural Abnormalities of the Placenta and Umbilical Cord
Bilobate and succenturiate placentas
Bilobate placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity:
Separation of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity into nearly equal-sized lobes with the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity inserted between them
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 1 in 350 deliveries
Multilobate placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity:PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity has ≥ 3 lobes.
Succenturiate lobe:
1 or more smaller lobes develop.
Lobes often develop at a distance from the main placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity, but with a vascular connection between the 2 lobes.
More common with twins
Diagnosis: Typically identified on routine antenatal ultrasound through direct visualization of the abnormal placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity.
Complications:
↑ Risk of postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage due to retained placental tissue (e.g., the main lobe delivered but the succenturiate lobe did not)
Vessels connecting the main placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity with the succenturiate lobe may rupture during labor causing fetal hemorrhage/demise.
↑ Risk of vasa previaVasa previaPregnancy complication where fetal blood vessels, normally inside the umbilical cord, are left unprotected and cross fetal membranes. It is associated with antepartum bleeding and fetal death and stillbirth due to exsanguination.Antepartum Hemorrhage (see below)
Velamentous cord insertion
Definition:
The last segment of the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity entering the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity (usually a few centimeters) lack the protective Wharton’s jelly.
The vessels are “exposed” and covered only by the fetal membranes.
Epidemiology:
1% of all pregnancies
Up to 15% of monochorionic twin gestations
Risk factors:
Multiple pregnancies, mainly twin gestations
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa
Diagnosis:
Antenatal ultrasound shows the vessels of the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity diverging from one another as the vessels approach the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity.
Vessels frequently insert near the placental edge (rather than in the normal, central location).
Management:
Antepartum: serial growth assessments
Intrapartum:
Continuous fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology monitoring
Low thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction for cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery (CD)
Minimal-to-no umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity traction during placental delivery
Complications:
Vessels are much more vulnerable to rupture, which can lead to rapid fetal exsanguination.
Much higher risk of vasa previaVasa previaPregnancy complication where fetal blood vessels, normally inside the umbilical cord, are left unprotected and cross fetal membranes. It is associated with antepartum bleeding and fetal death and stillbirth due to exsanguination.Antepartum Hemorrhage and antenatal hemorrhage
Cord avulsion (i.e., ripping the cord off the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity) during placental delivery → ↑ risk of retained placental tissue → ↑ risk of:
Delayed postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Infection
Velamentous cord insertion: Note that for the last several centimeters, there is no protective Wharton’s jelly surrounding the vessels; they are covered only by a thin fetal membrane.
Image: “Velamentous cord insertion” by Schokohäubchen. License: Public Domain
Vasa previaVasa previaPregnancy complication where fetal blood vessels, normally inside the umbilical cord, are left unprotected and cross fetal membranes. It is associated with antepartum bleeding and fetal death and stillbirth due to exsanguination.Antepartum Hemorrhage
Definition: occurs when fetal blood vessels traverse or run near the internal cervical os
Epidemiology: 1 in 1500 pregnancies
Associated risk factors:
Velamentous umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Succenturiate placental lobes
Pregnancies conceived via in vitro fertilizationFertilizationTo undergo fertilization, the sperm enters the uterus, travels towards the ampulla of the fallopian tube, and encounters the oocyte. The zona pellucida (the outer layer of the oocyte) deteriorates along with the zygote, which travels towards the uterus and eventually forms a blastocyst, allowing for implantation to occur. Fertilization and First Week(IVF)
Fetal bradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias (HR < 110/min)
Diagnosis: Antenatal sonogramSonogramChorioretinitis with color flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial PressuredopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography) shows fetal vessels traversing the internal cervical os.
Management:
Pelvic rest (no digital exams, no intercourse; “nothing in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy”) antenatally
Immediate cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery for clinical bleeding and/or signs of labor
Antenatal corticosteroidsCorticosteroidsChorioretinitis if preterm and delivery is anticipated within 7 days (generally 24–34 weeks)
Inpatient observation with daily fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring starting around 30‒34 weeks
Plan to deliver by CD at 34‒37 weeks (prior to the onset of labor).
Complications: blood vessels rupture → bleeding from fetoplacental circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment → fetal exsanguination and death
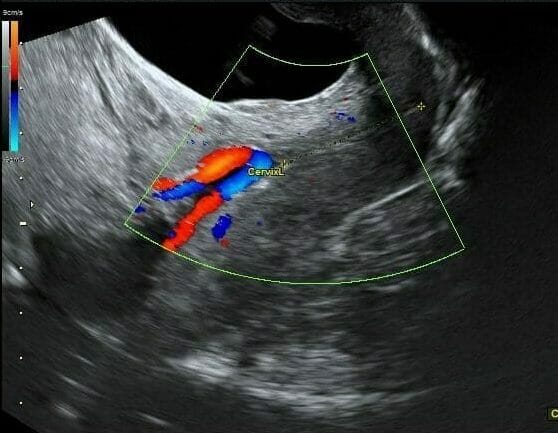
Ultrasound image of a vasa previa: The doppler color flow is illuminating the fixed vessels which are traversing the internal cervical os. The cervical canal is shown with the yellow dotted line.
Image: “Measurement of the cervical length by color Doppler transvaginal examination” by Bohîlțea RE et al. License: CC BY 2.0
Other anomalies of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity and umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Single umbilical arteryUmbilical arterySpecialized arterial vessels in the umbilical cord. They carry waste and deoxygenated blood from the fetus to the mother via the placenta. In humans, there are usually two umbilical arteries but sometimes one.Prenatal and Postnatal Physiology of the Neonate: (may ↑ the risk of aneuploidy or other associated anomalies)
Marginal cord insertion:
Insertion of the cord near the edge of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity rather than in the middle
May ↑ the risk of the cord avulsion during placental delivery
Umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity loops and/or knots: may impede blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure
Funic presentation:
When a loop of the normal umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity is tucked below the fetal presenting part
TeratomaTeratomaA true neoplasm composed of a number of different types of tissue, none of which is native to the area in which it occurs. It is composed of tissues that are derived from three germinal layers, the endoderm, mesoderm, and ectoderm. They are classified histologically as mature (benign) or immature (malignant).Imaging of the Mediastinum
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity accreta spectrum (PAS) describes a spectrum of abnormal placentation in which the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is abnormally and firmly adherent to the uterine wall. The 3 degrees of PAS are:
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity accreta (approximately 65%): The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity attaches directly to the myometrium due to partial or total absence of the decidua basalis.
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity increta (15%): Placental villi invade into the myometrium.
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity percreta (approximately 20%): Placental villi penetrate through the entire myometrium and may invade other surrounding structures.
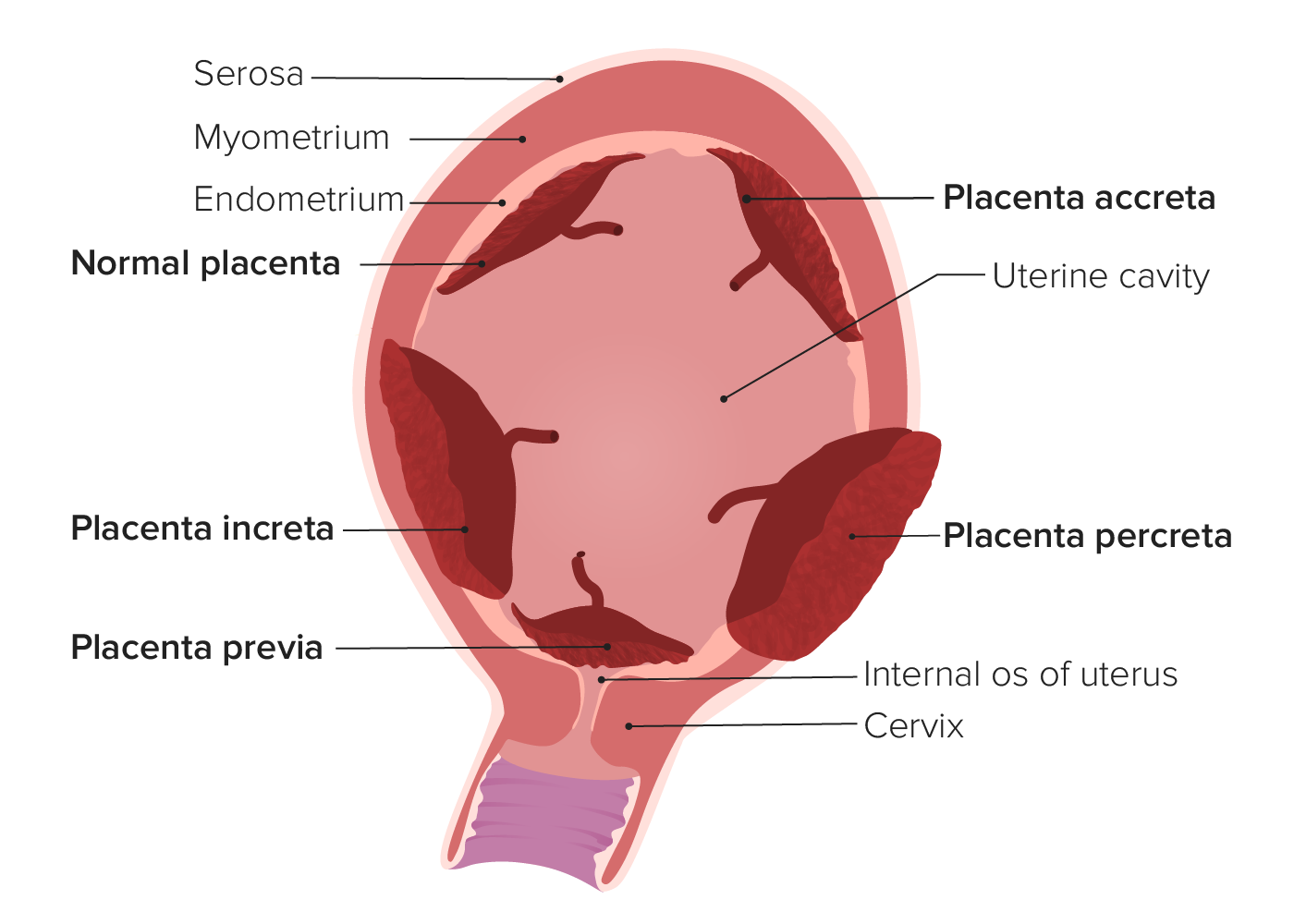
Types of abnormal placentation:
In placenta accreta, the placenta attaches (at least in part) to the underlying myometrium. In placenta increta, the placental villi actually invade into the myometrium. In placenta percreta, the placental villi invade through the entire uterine wall and may invade surrounding structures (e.g., the bladder). Placenta previa occurs when the placenta covers the internal cervical os.
The prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency has been increasing steadily over the past few decades and is now approximately 0.2% of pregnancies.
Likely due to defective decidualization in an area of scarScarDermatologic Examination caused by prior uterine surgery
Risk factors
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa after a prior CD:
Most important risk factor
> 60% chance of PAS after 4 CDs if placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa is present
Prior history of uterine surgery/procedures (regardless of placental location):
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
Myomectomy
Dilation and curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors
Endometrial ablation
InfertilityInfertilityInfertility is the inability to conceive in the context of regular intercourse. The most common causes of infertility in women are related to ovulatory dysfunction or tubal obstruction, whereas, in men, abnormal sperm is a common cause. Infertility procedures
Maternal age > 35 years
Multiparity
A history of postpartum endometritisPostpartum EndometritisInflammation of the endometrium, usually caused by intrauterine infections. Endometritis is the most common cause of postpartum fever.Postpartum Endometritis
Diagnosis
Typically asymptomatic
Usually diagnosed on routine antenatal ultrasound
If missed on ultrasound, PAS is typically diagnosed at delivery when the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity fails to deliver.
Clinical note:
Massive postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage can result when manual separation of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is attempted.
Therefore, when attempting manual removal of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity:
Try to find the natural tissue plane between the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity and the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy, and pull it out intact.
Do not create a plane by ripping the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity.
Management
Planned cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
Concurrent hysterectomy is often required → patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require extensive counseling
Be prepared for a potentially massive and immediate postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage → have blood products and postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage medications immediately available
If PAS is diagnosed at the time of vaginal delivery → surgical management
Complications
Severe postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage secondary to retained placental tissue (blood is entering maternal lacunaeLacunaeBones: Development and Ossification that are now “open” without the fetal chorionic plateChorionic platePlacenta, Umbilical Cord, and Amniotic Cavity being present)
Complications related to hypovolemic/hemorrhagic shockHemorrhagic shockAcute hemorrhage or excessive fluid loss resulting in hypovolemia.Hemothorax, including postpartum hypopituitarismHypopituitarismHypopituitarism is a condition characterized by pituitary hormone deficiency. This condition primarily results from a disease of the pituitary gland, but it may arise from hypothalamic dysfunction. Pituitary tumors are one of the most common causes. The majority of cases affect the anterior pituitary lobe (adenohypophysis), which accounts for 80% of the gland. Hypopituitarism (i.e., Sheehan syndrome)
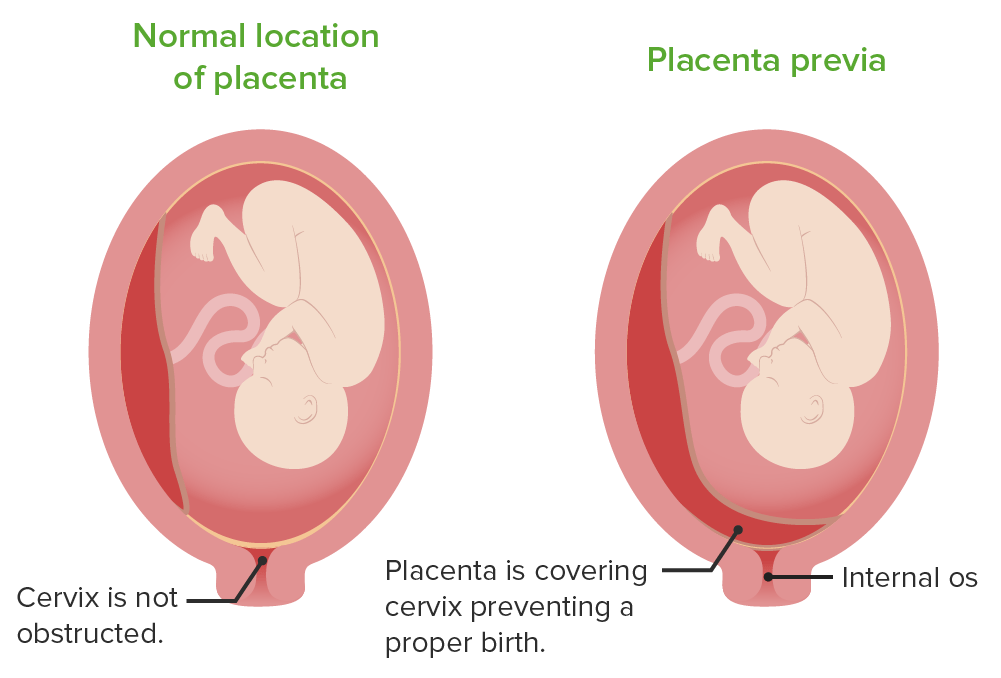
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa refers to the presence of placental tissue covering the internal cervical os. When the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy begins dilating, shearing forcesShearing forcesVascular Resistance, Flow, and Mean Arterial Pressure result in placental detachment over and around the internal osInternal osUterus, Cervix, and Fallopian Tubes: Anatomy, which may lead to life-threatening maternal and fetal hemorrhage.
The location of the placenta in placenta previa
Image by Lecturio.
Risk factors
Previous placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa
Previous cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
Prior uterine procedures (e.g., dilation and curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors)
Multiple gestations
Multiparity
Maternal cocaineCocaineAn alkaloid ester extracted from the leaves of plants including coca. It is a local anesthetic and vasoconstrictor and is clinically used for that purpose, particularly in the eye, ear, nose, and throat. It also has powerful central nervous system effects similar to the amphetamines and is a drug of abuse. Cocaine, like amphetamines, acts by multiple mechanisms on brain catecholaminergic neurons; the mechanism of its reinforcing effects is thought to involve inhibition of dopamine uptake.Local Anesthetics use
Diagnosis
Typically diagnosed on routine antenatal ultrasound, which shows the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity over the cervical os
If missed on ultrasound, may present with painless bright-red bleeding and fetal distress:
Often occurs after a digital exam or intercourse
Can be differentiated from placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage, which presents with painful bleeding and uterine irritability
Management
Note: Approximately 90% of previas identified at < 20 weeks gestation will resolve as the lower uterine segment grows, “moving” the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity further away from the cervical os.
Resolution is more likely when only the edge of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is touching the edge of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy.
Less likely to resolve when the os is completely covered
Pelvic rest
Avoid digital exams (cervical dilationCervical dilationA measurement of the diameter of the cervical canal, reported in centimetersNormal and Abnormal Labor should be assessed visually with a speculum exam).
Follow with serial ultrasounds to look for resolution.
Planned CD at 36‒37+6 weeks if placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity previa remains at full term (or at the onset of labor)
If bleeding:
Assess hemodynamic stability of the mother → resuscitate as needed
Continuous fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring
Rh(D) immune globulin if the mother is Rh-negative
Indications for delivery (by CD), regardless of gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care:
Active labor
Nonreassuring fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring
Continued bleeding and/or hemodynamic instability
If bleeding is mild and resolves, observation may be an option.
Complications
Preterm delivery (approximately 45% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Antenatal hemorrhage (approximately 50% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage (approximately 25% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Risk of recurrence in subsequent pregnancies (4%‒8% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
Uteroplacental Insufficiency
Definition
Uteroplacental insufficiencymay be acute or chronic and refers to the inability of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity to deliver a sufficient supply of O2 and nutrients to the fetus.
Chronic uteroplacental insufficiency
Chronic uteroplacental insufficiency results in fetal growth restrictionFetal growth restrictionFetal growth restriction (FGR), also known as intrauterine fetal growth restriction (IUGR), is an estimated fetal weight (EFW) or abdominal circumference < 10th percentile for gestational age. The term small for gestational age (SGA) is sometimes erroneously used interchangeably with FGR. Fetal Growth Restriction and associated complications.
Etiology/risk factors:
Maternal vascular disease, especially:
Chronic hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
PreeclampsiaPreeclampsiaA complication of pregnancy, characterized by a complex of symptoms including maternal hypertension and proteinuria with or without pathological edema. Symptoms may range between mild and severe. Pre-eclampsia usually occurs after the 20th week of gestation, but may develop before this time in the presence of trophoblastic disease.Hypertensive Pregnancy Disorders
Pregestational diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Severe maternal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
Maternal smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases or cocaineCocaineAn alkaloid ester extracted from the leaves of plants including coca. It is a local anesthetic and vasoconstrictor and is clinically used for that purpose, particularly in the eye, ear, nose, and throat. It also has powerful central nervous system effects similar to the amphetamines and is a drug of abuse. Cocaine, like amphetamines, acts by multiple mechanisms on brain catecholaminergic neurons; the mechanism of its reinforcing effects is thought to involve inhibition of dopamine uptake.Local Anesthetics use
Uterine malformations
Diagnosis via ultrasound, demonstrating:
Fetal growth restrictionFetal growth restrictionFetal growth restriction (FGR), also known as intrauterine fetal growth restriction (IUGR), is an estimated fetal weight (EFW) or abdominal circumference < 10th percentile for gestational age. The term small for gestational age (SGA) is sometimes erroneously used interchangeably with FGR. Fetal Growth Restriction
OligohydramniosOligohydramniosOligohydramnios refers to amniotic fluid volume less than expected for the current gestational age. Oligohydramnios is diagnosed by ultrasound and defined as an amniotic fluid index (AFI) of ‰¤ 5 cm or a single deep pocket (SDP) of < 2 cm in the 2nd or 3rd trimester. Oligohydramnios (frequent)
Increased vascular resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing within the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity on DopplerDopplerUltrasonography applying the doppler effect, with frequency-shifted ultrasound reflections produced by moving targets (usually red blood cells) in the bloodstream along the ultrasound axis in direct proportion to the velocity of movement of the targets, to determine both direction and velocity of blood flow.Ultrasound (Sonography) studies
Management:
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be monitored antenatally with frequent nonstress tests and ultrasound to look for signs of fetal decompensation.
Delivery is indicated when the fetus begins showing signs of distress (e.g., non-reassuring fetal status on testing).
Typically, if patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are otherwise candidates for vaginal delivery, induction of labor is recommended over planned cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery, with close intrapartum monitoring.
If preterm, give a course of steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors (typically IM betamethasoneBetamethasoneA glucocorticoid given orally, parenterally, by local injection, by inhalation, or applied topically in the management of various disorders in which corticosteroids are indicated. Its lack of mineralocorticoid properties makes betamethasone particularly suitable for treating cerebral edema and congenital adrenal hyperplasia.Glucocorticoids) to help promote fetal lung maturity prior to delivery.
Acute uteroplacental insufficiency
Etiology:
Periods of ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage during labor contractions, preventing the delivery of O2 and nutrients at levels required to satisfy fetal requirements
Note: Relative ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage occurs during normal labor, but can be magnified with placental pathology.
Partial or complete placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage
Diagnosis is via abnormalities noted on fetal cardiac monitoring:
Recurrent late decelerations
Persistent fetal bradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias
UterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy is frequently hypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation and/or tachysystolic (> 5 contractions in 10 minutes).
Give mother IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids and routine oxygen supplementation if the mother is hypoxemic.
↓ Uterotonics (e.g., pitocin) and/or administer uterine tocolytics (e.g., terbutalineTerbutalineA selective beta-2 adrenergic agonist used as a bronchodilator and tocolytic.Asthma Drugs)
Cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery (if remote from delivery)
The most common clinical complications of abnormal placentation are antepartum and postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage, which can be both severe and life threatening, depending on the clinical situation. Additionally, the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity may become infected or develop a malignancyMalignancyHemothorax.
Antepartum hemorrhageAntepartum hemorrhageAntepartum hemorrhage is defined as vaginal bleeding that occurs after 20 weeks of gestation and is unrelated to labor. The most important causes are placental abruption (most common), placenta previa (2nd most common), vasa previa, and uterine rupture. Antepartum Hemorrhage: refers to uterine bleeding that occurs prior to the onset of labor. The most clinically important types of antepartum hemorrhageAntepartum hemorrhageAntepartum hemorrhage is defined as vaginal bleeding that occurs after 20 weeks of gestation and is unrelated to labor. The most important causes are placental abruption (most common), placenta previa (2nd most common), vasa previa, and uterine rupture. Antepartum Hemorrhage that should be immediately identified and treated include bleeding from placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage (typically painful), a placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity or vasa previaVasa previaPregnancy complication where fetal blood vessels, normally inside the umbilical cord, are left unprotected and cross fetal membranes. It is associated with antepartum bleeding and fetal death and stillbirth due to exsanguination.Antepartum Hemorrhage (typically painless), or uterine ruptureUterine RuptureA complete separation or tear in the wall of the uterus with or without expulsion of the fetus. It may be due to injuries, multiple pregnancies, large fetus, previous scarring, or obstruction.Antepartum Hemorrhage (in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a history of major uterine surgery including a prior CD). Bleeding frequently affects both the mother and infant; thus, immediate delivery is indicated in most cases.
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage: refers to uterine bleeding after the infant is delivered. The 4 primary causes can be remembered as the 4 T’s: Tone (uterine atony, by far the most common), Tissue (retained placental tissue), Trauma (lacerations of the perineumPerineumThe body region lying between the genital area and the anus on the surface of the trunk, and to the shallow compartment lying deep to this area that is inferior to the pelvic diaphragm. The surface area is between the vulva and the anus in the female, and between the scrotum and the anus in the male.Vagina, Vulva, and Pelvic Floor: Anatomy, vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, or cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy), and Thrombin (coagulation disorders, especially disseminated intravascular coagulationDisseminated intravascular coagulationDisseminated intravascular coagulation (DIC) is a condition characterized by systemic bodywide activation of the coagulation cascade. This cascade results in both widespread microvascular thrombi contributing to multiple organ dysfunction and consumption of clotting factors and platelets, leading to hemorrhage. Disseminated Intravascular Coagulation). The diagnosis is typically clinical. The retained placental tissue should be removed manually or surgically.
ChorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis(intraamniotic infection (IAI)): a common obstetric complication involving infection and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the fetal membranes, amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity, placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity, or the fetus itself. ChorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis is typically caused by an ascending polymicrobial infection from the lower genitourinary tract, most commonly after the prolonged rupture of membranes. There are specific clinical criteria for diagnosis, including maternal feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever. An IAI is managed with antibiotics, and ultimately, delivery, which typically results in its resolution.
Gestational trophoblastic diseaseGestational trophoblastic diseaseGestational trophoblastic diseases are a spectrum of placental disorders resulting from abnormal placental trophoblastic growth. These disorders range from benign molar pregnancies (complete and partial moles) to neoplastic conditions such as invasive moles and choriocarcinoma. Gestational Trophoblastic Disease (GTDGTDGestational trophoblastic diseases are a spectrum of placental disorders resulting from abnormal placental trophoblastic growth. These disorders range from benign molar pregnancies (complete and partial moles) to neoplastic conditions such as invasive moles and choriocarcinoma.Gestational Trophoblastic Disease): a group of pregnancy-related tumors resulting from abnormal placental trophoblastic growth that range from benignBenignFibroadenoma molar pregnancies (complete and partial) to neoplastic conditions (e.g., invasive moleMoleNevi (singular nevus), also known as “moles,” are benign neoplasms of the skin. Nevus is a non-specific medical term because it encompasses both congenital and acquired lesions, hyper- and hypopigmented lesions, and raised or flat lesions.Nevus/Nevi, choriocarcinomaChoriocarcinomaA malignant metastatic form of trophoblastic tumors. Unlike the hydatidiform mole, choriocarcinoma contains no chorionic villi but rather sheets of undifferentiated cytotrophoblasts and syncytiotrophoblasts (trophoblasts). It is characterized by the large amounts of chorionic gonadotropin produced. Tissue origins can be determined by DNA analyses: placental (fetal) origin or non-placental origin.Gestational Trophoblastic Disease, and placental site trophoblastic tumorTumorInflammation). PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will typically have grossly elevated serum β-hCG levels and characteristic ultrasound findings. Treatment involves surgery and/or chemotherapyChemotherapyOsteosarcoma, usually with methotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy.
References
Cunningham, F.G., Leveno, K.J., et al. (2010). Williams Obstetrics (23rd ed. pp. 36‒72, 557‒585).