Laparotomy is an open surgical exploration of the abdomen, usually through a single large incision. Laparoscopy is surgical exploration and interventions performed through ports placed in small incisions with a camera and long instruments. Laparoscopy offers the advantage of being minimally invasive, but it misses the tactile component of abdominal exploration for the surgeon. Both techniques have their applications, advantages, and disadvantages, and a surgeon should be familiar and comfortable with both techniques.
The surgeon must be familiar with the anatomical landmarks and important corresponding structures of the abdomen to avoid iatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome injury to these structures, especially in emergency situations.
Costal cartilages of the 7th–10th ribsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy
Inferior:
Pubic boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and the pubic symphysisPubic SymphysisA slightly movable cartilaginous joint which occurs between the pubic bones.Vagina, Vulva, and Pelvic Floor: Anatomy
Inguinal ligaments
Lateral:
Superior: inferior aspect of the 10th rib
Inferior: iliac crest
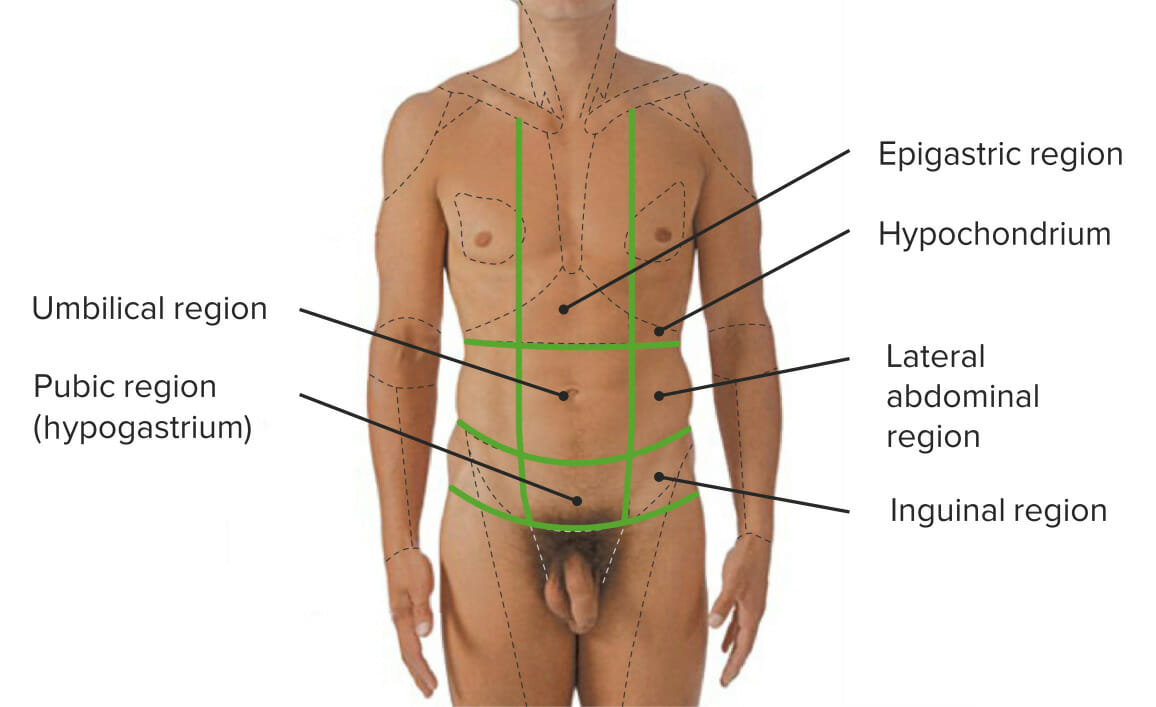
Surface landmarks:
Umbilicus: “belly button”
Linea alba: medial edges of the rectus muscles; the longitudinal midline
Semilunar lines: lateral edges of the rectus muscles
Anterior superior iliac spines
Iliac crest
Pubic symphysisPubic SymphysisA slightly movable cartilaginous joint which occurs between the pubic bones.Vagina, Vulva, and Pelvic Floor: Anatomy: where the halves of the pelvic girdle join together anteriorly in the midline
Inguinal grooves: “groinGroinThe external junctural region between the lower part of the abdomen and the thigh.Male Genitourinary Examination”
The 4 quadrants of the abdomen: The abdomen is divided into 4 quadrants with the umbilicus in the center:
Divided into right and left halves
Divided into upper and lower halves
Quadrants:
RUQ
LUQ
RLQ
LLQ
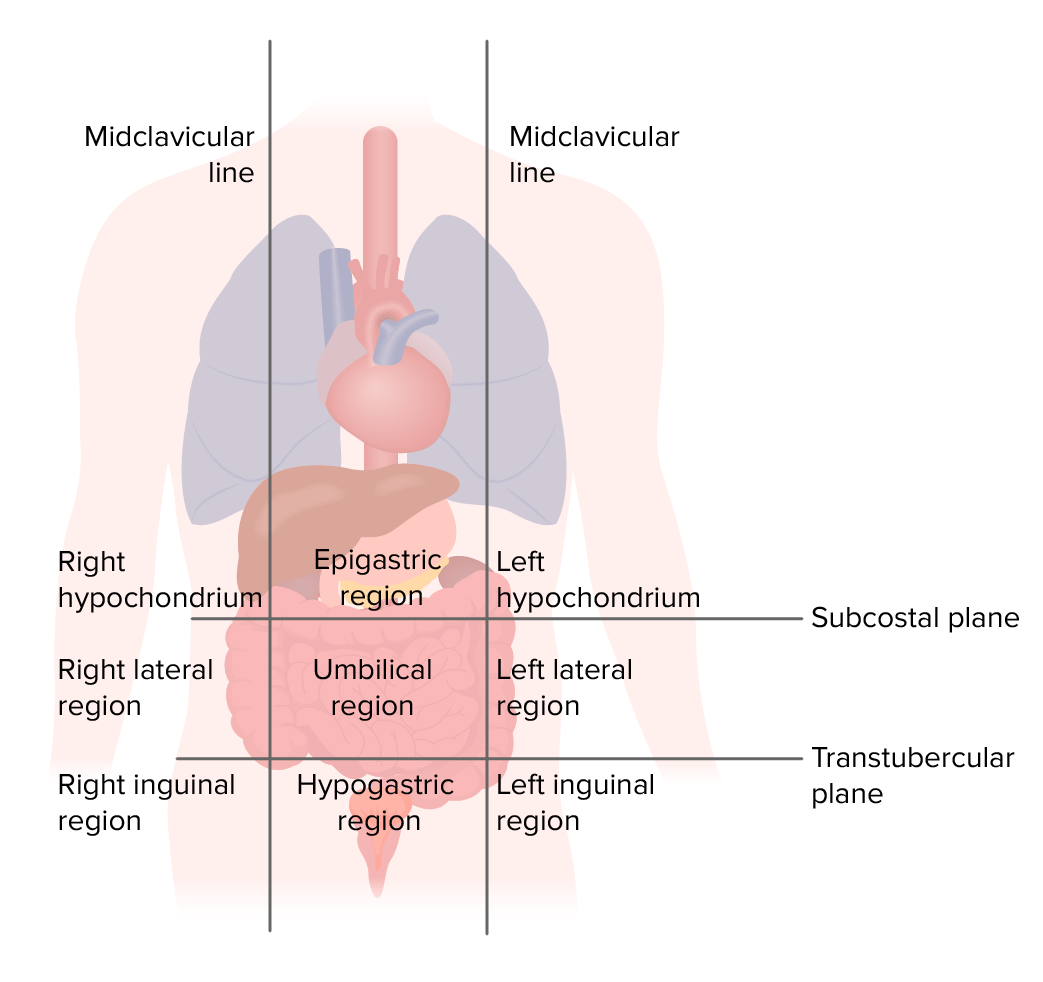
The 9 regions of the abdomen: The abdomen is divided into 9 regions by 3 lines/planes:
Lines/planes:
Right and left midclavicular lines: longitudinal lines extending down from the middle of the clavicleClavicleA bone on the ventral side of the shoulder girdle, which in humans is commonly called the collar bone.Clavicle Fracture
Subcostal planeSubcostal PlaneAnterior Abdominal Wall: Anatomy: horizontal line at the base of the ribsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy
Transtubercular (or intertubercular) plane: horizontal line at the level of the iliac tubercle (elevations in the iliac crest)
Regions of the abdomen and their respective organs
Image by Lecturio.
Layers of the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Anterolateral: in order (from superficial to deep):
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
Superficial fatty layer (Camper’s fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis)
Deeper membranous layer (Scarpa’s fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis)
Investing fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
External obliqueExternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy muscle/aponeurosis
Internal obliqueInternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy muscle/aponeurosis
Transverse abdominal muscle
Transversalis fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Extraperitoneal fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
ParietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: AnatomyperitoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy
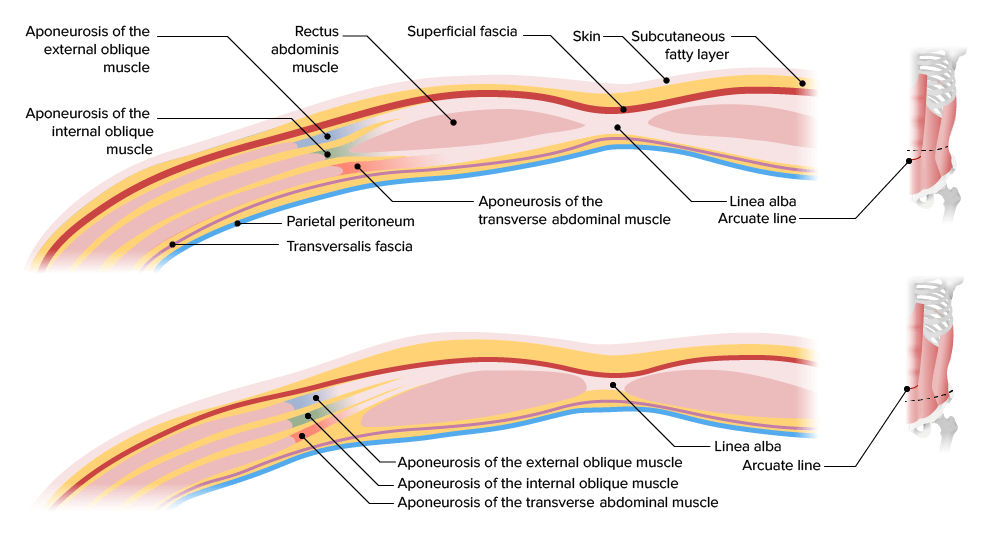
Differences above and below the arcuate line (located approximately ⅓ the distance from the umbilicus to the pubic crest):
Above the arcuate line, the fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis surrounding the rectus consists of:
Anterior to the rectus:
Aponeurosis of the external obliqueExternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy
Anterior lamina of the internal obliqueInternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: AnatomyfasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Posterior to the rectus:
Posterior lamina of the internal obliqueInternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: AnatomyfasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Transversalis fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Below the arcuate line, the fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis surrounding the rectus consists of:
Anteriorly:
Aponeurosis of the external obliqueExternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy
Aponeurosis of the internal obliqueInternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy
Posteriorly: transversalis fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Layers of the internal abdominal wall:
Note that above the arcuate line, the posterior lamina of the internal oblique and the entire aponeurosis of the transverse abdominal muscle run posterior to the rectus abdominis. However, inferior to the arcuate line, the entire aponeurosis of the external obliques, the internal obliques, and the transverse abdominal muscles run anterior to the rectus. Only the transversalis fascia and the parietal peritoneum run posteriorly.
Image by Lecturio.
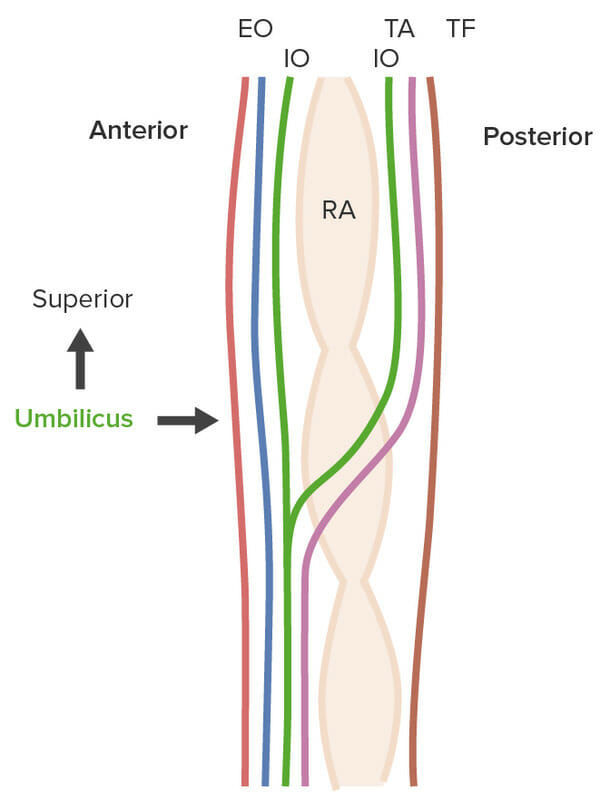
Lateral view of the layers of the anterior abdominal wall above and below the arcuate line:
Above the arcuate line, the subcutaneous fascia (red), the entire aponeurosis of the external oblique (EO, blue), and the anterior lamina of the internal oblique (IO, green) all run anterior to the rectus abdominis (RA) muscle. The posterior lamina of the internal oblique (green), the transverse abdominal muscle (TA, pink), and the transversalis fascia (TF, brown), however, run posterior to the RA muscle. Below the arcuate line (located approximately ⅓ the distance between the umbilicus and the pubic crest), the entire aponeurosis of the external oblique (blue), internal oblique (green), and transverse abdominal muscles (pink) run anterior to the RA muscle. Only the transversalis fascia (brown) runs posteriorly.
Image by Lecturio.
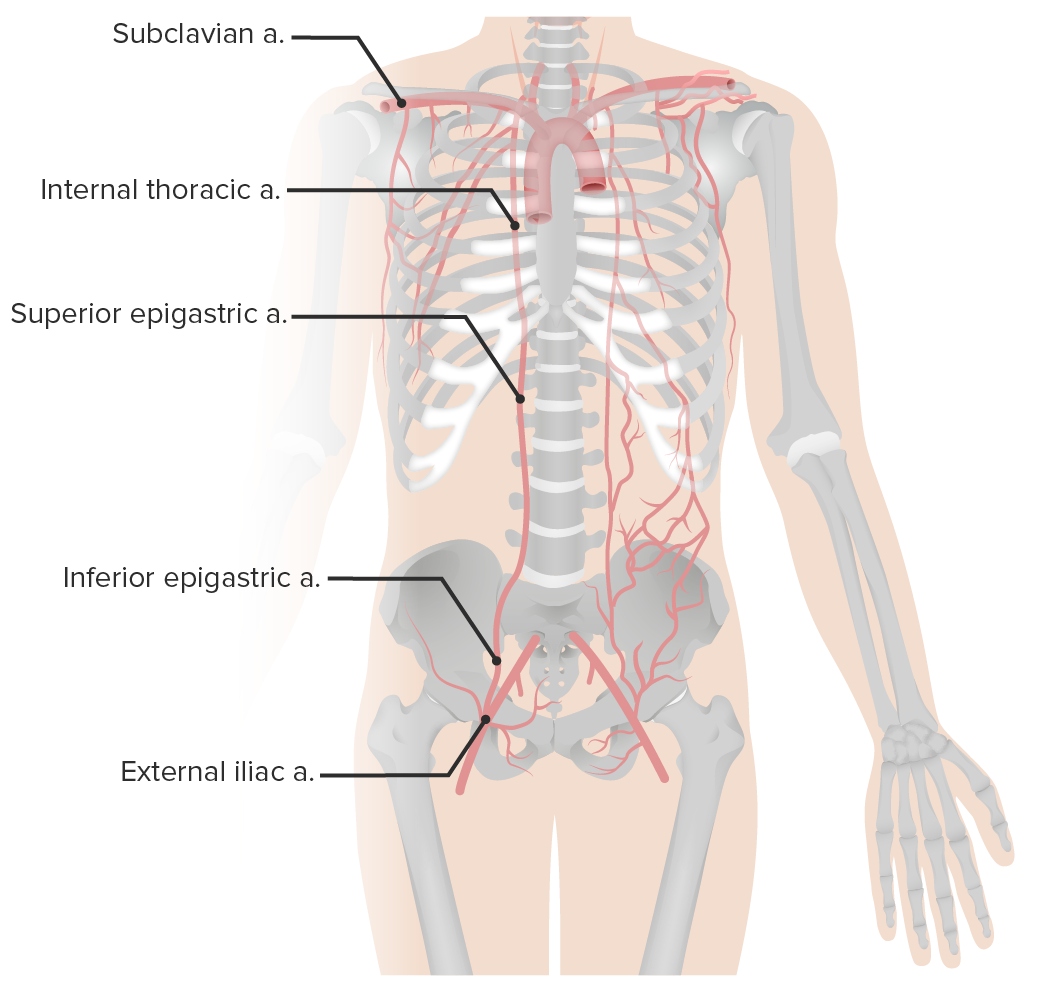
Arterial supply of the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Superior epigastric artery: branch of the internal thoracic, or mammary, artery
Inferior epigastric artery: branch of the external iliac artery
Both arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology run through the rectus sheath (deep to the rectus muscle) and anastomose.
Additional blood supply comes from:
The 10th and 11th posterior intercostal arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology
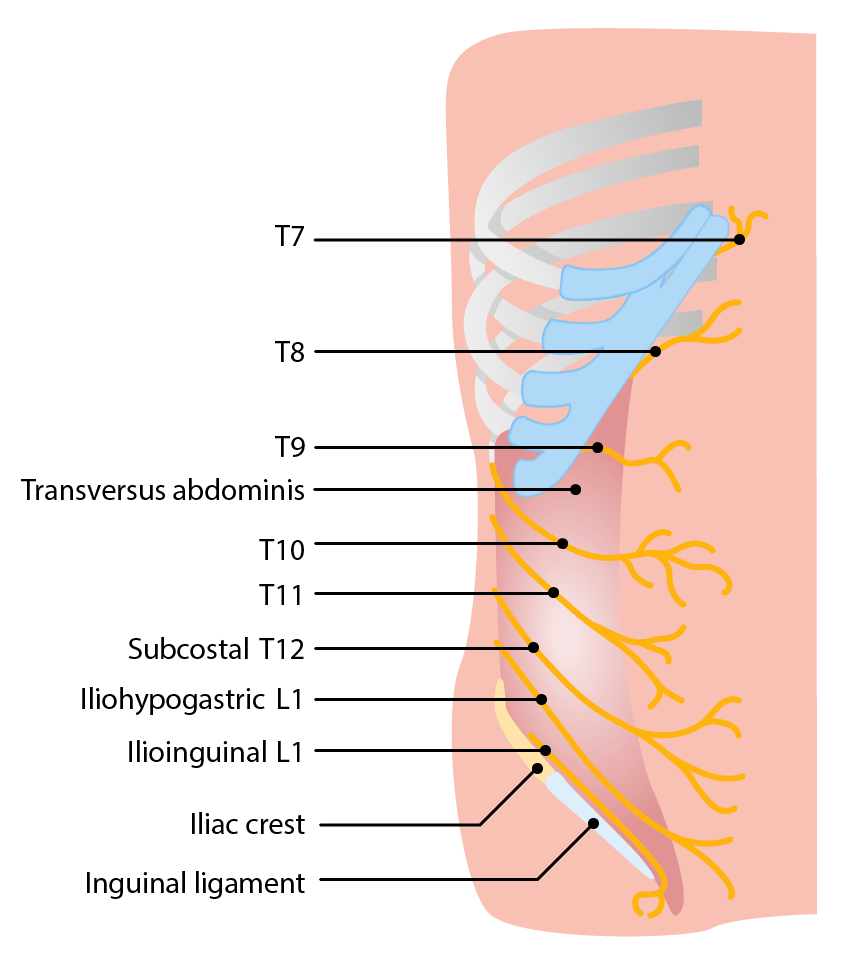
Innervation of the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Nerves running between the internal obliqueInternal obliqueMuscles of the anterolateral abdominal wall consisting of the external oblique and the internal oblique muscles. The external abdominal oblique muscle fibers extend from lower thoracic ribs to the linea alba and the iliac crest. The internal abdominal oblique extend superomedially beneath the external oblique muscles.Anterior Abdominal Wall: Anatomy and transverse abdominal layers:
Visceral painVisceral painPain originating from internal organs (viscera) associated with autonomic phenomena (pallor; sweating; nausea; and vomiting). It often becomes a referred pain.Pain: Types and Pathways is referred to its respective dermatomeDermatomeSpinal Disk Herniation.
Nerves innervating the anterior abdominal wall:
The nerves run between the internal oblique and the transversus abdominis layers.
Image by Lecturio
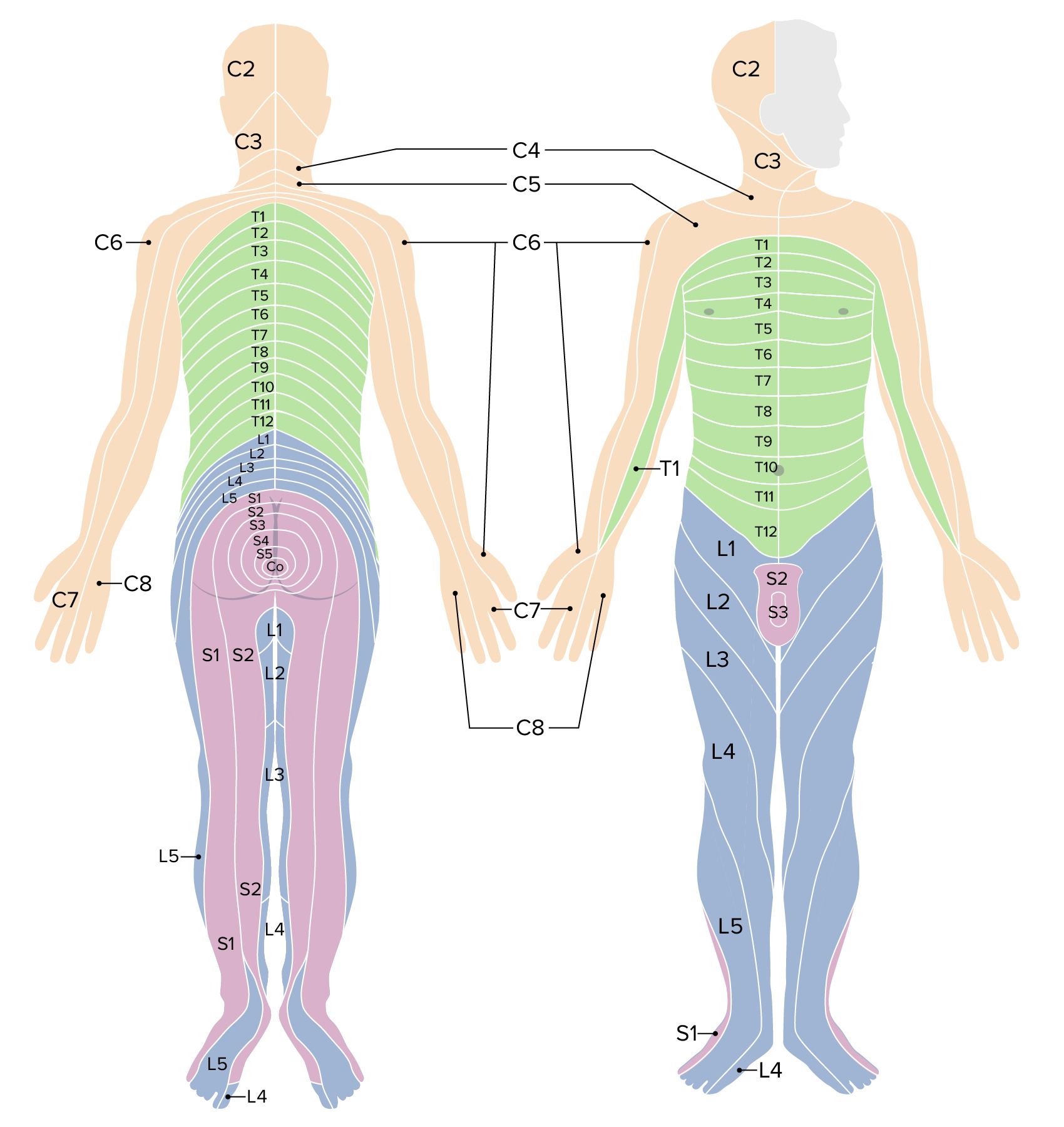
Abdominal dermatomes:
The abdomen is primarily innervated by the anterior rami of nerves, which exit the spinal cord at T7‒L1.
Laparotomy: surgical intervention consisting of a single incision performed to gain access to the abdominal cavity (open surgery)
Laparoscopy: surgical intervention designed to access the intraabdominal organs via various small (typically 5‒12 mm) portal incisions for the insertion of a laparoscope and other instruments
Exploratory: procedure that will aid the surgeon in determining definitive treatment for the patient based on intraoperative findings
The majority of abdominal procedures nowadays could be performed with either the open or the laparoscopic approach. Laparoscopic approaches are generally preferred when possible
Traditional indications for laparotomy
Abdominal trauma accompanied by:
PeritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury
ShockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock
EviscerationEviscerationSurgical Complications: extrusion of the abdominal viscera through an opening in the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Hemoperitoneum
Acute abdomenAcute AbdomenAcute abdomen, which is in many cases a surgical emergency, is the sudden onset of abdominal pain that may be caused by inflammation, infection, perforation, ischemia, or obstruction. The location of the pain, its characteristics, and associated symptoms (e.g., jaundice) are important tools that help narrow the differential diagnosis.Acute Abdomen/peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury caused by:
Perforated viscusPerforated ViscusPerforated viscus or GI perforation represents a condition in which the integrity of the GI wall is lost with subsequent leakage of enteric contents into the peritoneal cavity, resulting in peritonitis. The causes of perforated viscus include trauma, bowel ischemia, infections, or ulcerative conditions, all of which ultimately lead to a full-thickness disruption of the intestinal wall. Perforated Viscus
Intestinal ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
Strangulated herniaHerniaProtrusion of tissue, structure, or part of an organ through the bone, muscular tissue, or the membrane by which it is normally contained. Hernia may involve tissues such as the abdominal wall or the respiratory diaphragm. Hernias may be internal, external, congenital, or acquired.Abdominal Hernias
Necrotic bowel
Uncontrolled GI hemorrhage
Obstetric cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery
Indications for laparoscopy
Laparoscopy has become the standard of careStandard of careThe minimum acceptable patient care, based on statutes, court decisions, policies, or professional guidelines.Malpractice for many procedures because it consistently yields more favorable outcomes when it can be performed safely in place of laparotomy.
Procedures commonly performed laparoscopically include:
CholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
AppendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy
Inguinal and ventral herniaVentral HerniaA hernia caused by weakness of the anterior abdominal wall due to midline defects, previous incisions, or increased intra-abdominal pressure. Ventral hernias include umbilical hernia, incisional, epigastric, and spigelian hernias.Abdominal Hernias repair
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy resections
Nissen fundoplication and hiatal herniaHiatal herniaStomach herniation located at or near the diaphragmatic opening for the esophagus, the esophageal hiatus.Congenital Diaphragmatic Hernias repair
Heller myotomyHeller myotomySurgical incision of the lower esophageal sphincter near the cardia often used to treat esophageal achalasia.Achalasia for achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia
Bariatric procedures (gastric bypassGastric bypassSurgical procedure in which the stomach is transected high on the body. The resulting small proximal gastric pouch is joined to any parts of the small intestine by an end-to-side surgical anastomosis, depending on the amounts of intestinal surface being bypasses. This procedure is used frequently in the treatment of morbid obesity by limiting the size of functional stomach, food intake, and food absorption.Gastroesophageal Reflux Disease (GERD), sleeve gastrectomy)
Can be performed for a stable patient with diagnostic uncertainty
Can be converted to an open procedure for a definitive surgery, if necessary
Choosing laparotomy versus laparoscopy
Factors to take into consideration:
Surgeon comfort with the procedures based on the clinical situation
Ensuring route will provide adequate visualization and surgical exposure
Certainty of the diagnosis
Need for rapid/emergent entry into the abdomen (laparotomy is faster)
Prior surgical history
Generally improved outcomes associated with laparoscopy, which typically include:
Less blood loss
Less postoperative painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Shorter hospital stay
Reduced postoperative infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Improved cosmetic outcomes
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation
There are no absolute contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to exploratory laparotomy; it is commonly performed under emergent conditions.
Some relative contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to any abdominal surgery include:
Coagulopathy
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
Ischemic heart diseaseIschemic heart diseaseCoronary heart disease (CHD), or ischemic heart disease, describes a situation in which an inadequate supply of blood to the myocardium exists due to a stenosis of the coronary arteries, typically from atherosclerosis. Coronary Heart Disease
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation specific to laparoscopy:
Inability to tolerate pneumoperitoneumPneumoperitoneumA condition with trapped gas or air in the peritoneal cavity, usually secondary to perforation of the internal organs such as the lung and the gastrointestinal tract, or to recent surgery. Pneumoperitoneum may be purposely introduced to aid radiological examination.Perforated Viscus (e.g., hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension, severe pulmonary diseasePulmonary diseaseDiseases involving the respiratory system.Blastomyces/Blastomycosis, heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR))
Preoperative carePreoperative CareThorough preoperative care is important for patients scheduled to undergo surgery so that they can have the best possible outcomes after their surgical procedure. The preoperative process begins once the decision has been made to proceed with a surgical procedure. Preoperative Care
Adequate preparation may not be possible in emergency situations.
Previous fast (nothing by mouth) of 8 hours, if possible
Preoperative labs to consider:
Type and screen or type and cross-match depending on anticipated blood loss and potential need for transfusion
Baseline CBC
Blood products are made available for transfusion, if needed, after blood type is obtained.
AnticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants are withheld before the procedure.
Pharmacologic anticoagulationAnticoagulationPulmonary Hypertension Drugs (e.g., enoxaparinEnoxaparinLow-molecular-weight fragment of heparin, having a 4-enopyranosuronate sodium structure at the non-reducing end of the chain. It is prepared by depolymerization of the benzylic ester of porcine mucosal heparin. Therapeutically, it is used as an antithrombotic agent.Anticoagulants)
Electrical grounding pad applied to the individual to ground electrosurgical instruments (e.g., Bovie)
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions preparation and surgical drapingDrapingExamination of the Breast:
Typically with chlorhexidine or povidone-iodine
Allow appropriate time for the prep to dry.
Drape the individual based on anticipated incisions to keep the surgical site sterileSterileBasic Procedures
Operative care
Laparotomy:
Allows quick access to the abdominal viscera, which is important in an emergency.
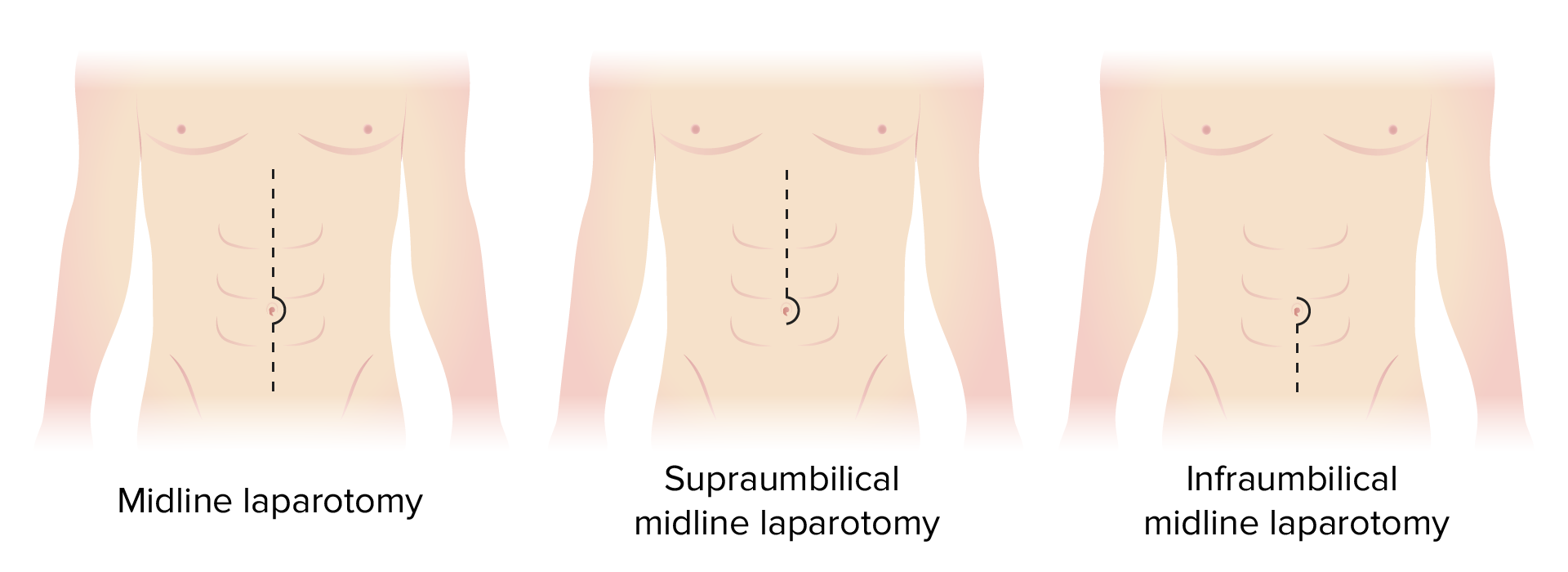
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions incision is chosen based on planned procedure (see table).
A vertical midline incision is carried through the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions, subcutaneous tissues, linea alba (rectus sheath), and peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy.
Retractors are placed to keep the incision open during the procedure.
At the completion of the procedure, the rectus fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis is closed with running or interrupted sutures (absorbable or nonabsorbable).
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions can be closed, or it can be left open in case of gross contamination of the field with bowel contents or pus.
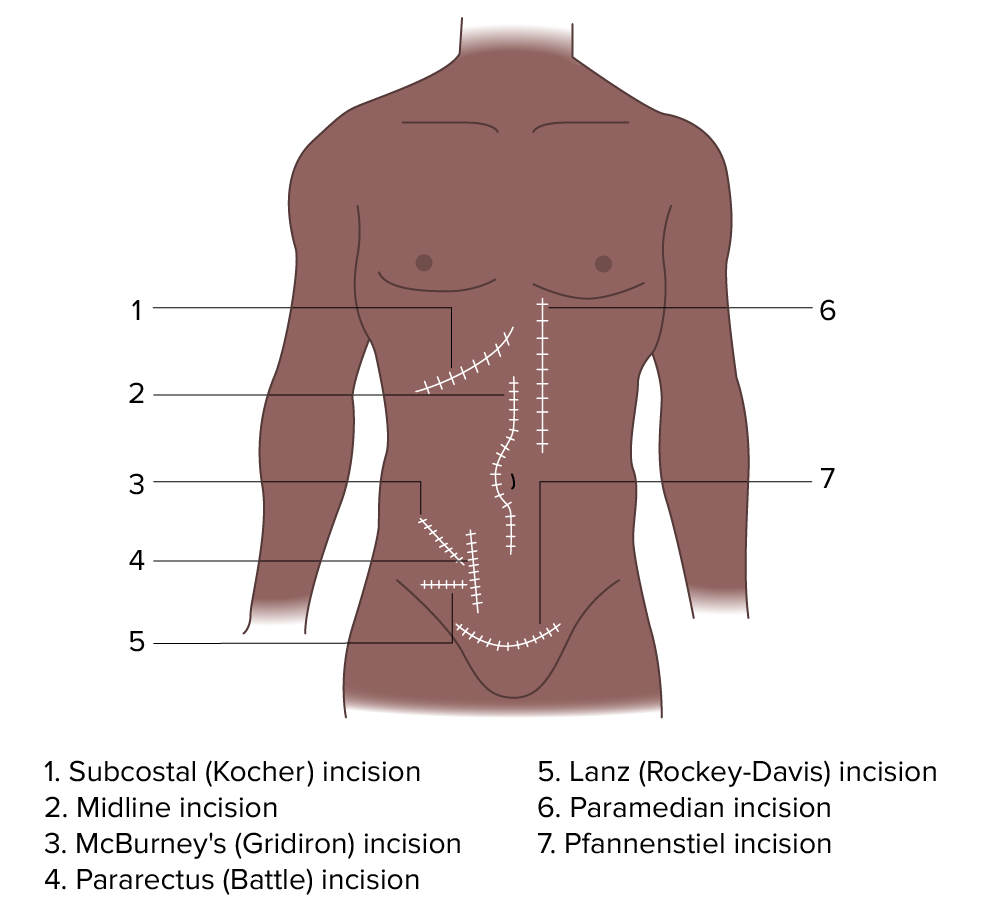
Table: Other abdominal incisions commonly used for open abdominal procedures (examples)
Direction
Incision
Description
Common example of use
Longitudinal
Midline
On the midline
Trauma procedures, cancers
Paramedian
2–5 cm to the left or right of the midline
Unilateral visceral procedures: kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy, adrenal glandsAdrenal GlandsThe adrenal glands are a pair of retroperitoneal endocrine glands located above the kidneys. The outer parenchyma is called the adrenal cortex and has 3 distinct zones, each with its own secretory products. Beneath the cortex lies the adrenal medulla, which secretes catecholamines involved in the fight-or-flight response. Adrenal Glands: Anatomy, and spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy
Pararectus (Battle incision)
On the lateral border of the rectus abdominisRectus AbdominisA long flat muscle that extends along the whole length of both sides of the abdomen. It flexes the vertebral column, particularly the lumbar portion; it also tenses the anterior abdominal wall and assists in compressing the abdominal contents. It is frequently the site of hematomas. In reconstructive surgery it is often used for the creation of myocutaneous flaps.Anterior Abdominal Wall: Anatomy muscle
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy, and duodenal procedures
The main goal of the procedure is to achieve the same results as with an open approach, but less invasively. The qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of surgical intervention should never be sacrificed, though, and the procedure can be converted to an open one at any point, as necessary.
Abdominal cavity can be accessed with a Veress needle or with a Hasson trocar through a small (usually 10‒12 mm) incision.
CO2 is pumped into the cavity through the needle or trocar until an intraabdominal pressure of 12–15 mm Hg is reached (artificial pneumoperitoneum).
Insufflation is needed to establish a working space for the instruments and adequate organ visualization.
Pressure should be low (usually < 5 mm Hg) upon entering the abdomen; if the pressure is higher, the needle/trocar may be preperitoneal or in a visceral organ → back out and replace the needle/trocar
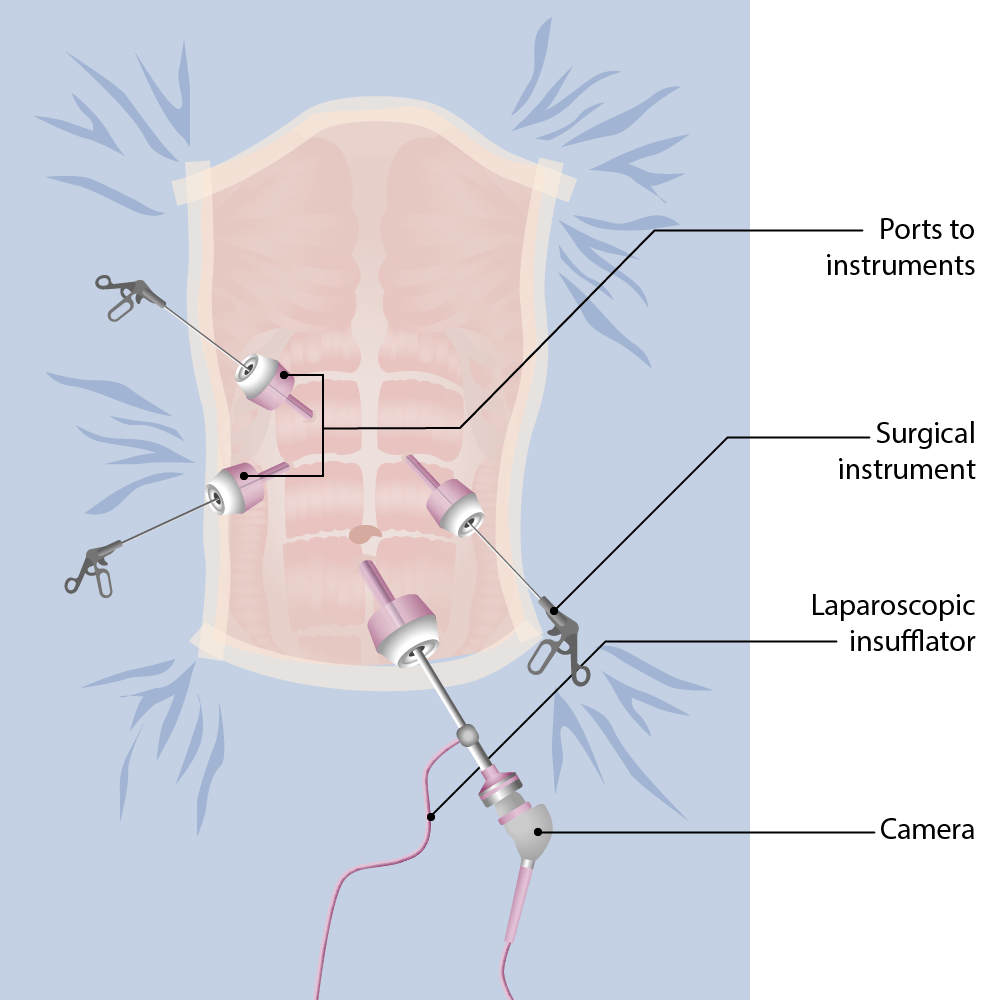
A laparoscopic camera is introduced through the trocar and is aimed at the area to be explored.
Additional trocars are placed using the laparoscope for visualization, and the necessary instruments are introduced through these portals as needed.
When the main intervention is complete, the instruments and trocars are extracted.
The laparoscope is extracted and the abdomen is desufflated.
The fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis needs to be closed at larger port sites.
The skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions at the trocar sites is closed with subcutaneous sutures or glue.
Laparoscopic intervention of the abdomen: Ports for the insertion of instruments are shown.
Image by Lecturio.
Postoperative carePostoperative careAfter any procedure performed in the operating room, all patients must undergo close observation at least in the recovery room. After larger procedures and for patients who require hospitalization, observation must continue on the surgical ward. The primary intent of this practice is the early detection of postoperative complications. Postoperative Care
The details of care depend on the particular intervention that was performed.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics control
Assess surgical sites for bleeding/drainage.
Assess for signs of cardiovascular and/or pulmonary complications (e.g., chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, which may suggest myocardial ischemiaMyocardial ischemiaA disorder of cardiac function caused by insufficient blood flow to the muscle tissue of the heart. The decreased blood flow may be due to narrowing of the coronary arteries (coronary artery disease), to obstruction by a thrombus (coronary thrombosis), or less commonly, to diffuse narrowing of arterioles and other small vessels within the heart.Coronary Heart Disease).
Deep vein thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic TyphusprophylaxisProphylaxisCephalosporins if staying in the hospital (may include early ambulation)
Discontinue drains and lines when safe (depends on the procedure and individual’s status).
Labwork (varies)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship can commonly be discharged home within 24 hours after uncomplicated laparoscopic procedures.
Laparotomies commonly require longer hospitalizations owing to the need for painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
Common discharge requirements for most procedures include:
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is controlled with oral medications.
Ability to empty the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess
Ambulatory, movement at baseline, or accommodations are arranged to assist the individual with activities of daily living.
Complications
Some complications are specific to the intervention performed (i.e., cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy or appendectomyAppendectomyAppendectomy is an invasive surgical procedure performed with the goal of resecting and extracting the vermiform appendix through either an open or a laparoscopic approach. The most common indication is acute appendicitis.Appendectomy). However, some complications are common to all procedures.
Complications associated with both laparoscopy and laparotomy
Hypercarbia and acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (CO2 trapping and absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption)
Wound dehiscenceWound dehiscencePathologic process consisting of a partial or complete disruption of the layers of a surgical wound.Wound Healing
Postoperative ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis