Epidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural hemorrhage presents acutely, usually immediately (seconds to hours) following head trauma, with an altered level of consciousness that may span from a momentary loss of consciousness to coma. Diagnosis is based on clinical suspicion following head trauma and is confirmed with neuroimaging (i.e., noncontrast head CT). Management includes stabilization, stopping (possibly, the reversal) of all anticoagulants, monitoring in a neurologic ICU, and neurosurgical intervention.
Epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage or hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception (EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage) is an event characterized by bleeding into the epidural spaceEpidural spaceSpace between the dura mater and the walls of the vertebral canal.Epidural Hemorrhage between the dural layer of the meningesMeningesThe brain and the spinal cord are enveloped by 3 overlapping layers of connective tissue called the meninges. The layers are, from the most external layer to the most internal layer, the dura mater, arachnoid mater, and pia mater. Between these layers are 3 potential spaces called the epidural, subdural, and subarachnoid spaces. Meninges: Anatomy and the skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy. Epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage usually results from trauma.
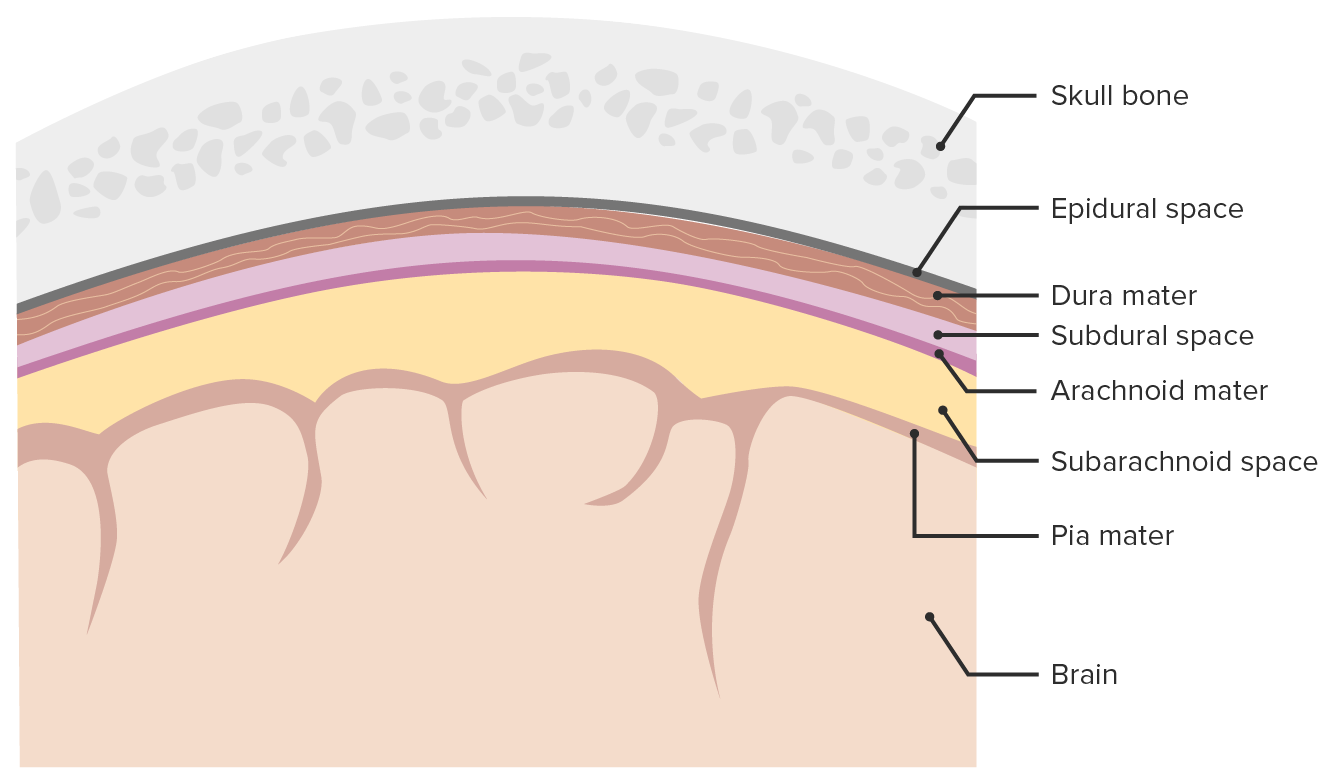
Image depicting the 3 layers (dura mater, arachnoid mater, pia mater) surrounding the brain and spinal cord. The meninges serve as mechanical protection of the CNS, support the cerebral and spinal blood vessels, and allow for the passage of CSF. Only the subarachnoid space is a true space present in physiologic conditions, whereas the epidural and subdural spaces form only during pathologic processes. The epidural space may open as a result of head trauma or, rarely, due to other pathologic processes.
Image by Lecturio.
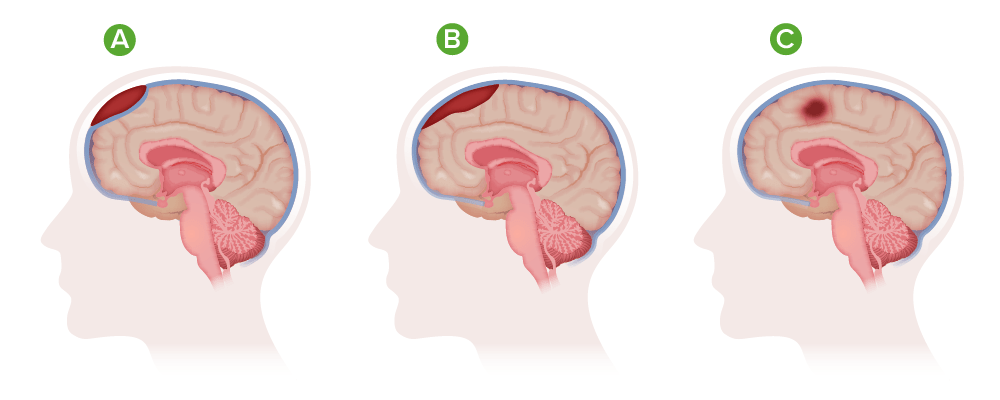
Types of hematoma: A) Epidural hematoma; B) Subdural hematoma; C) Intracranial hematoma
Image by Lecturio.
Epidemiology[1–3]
Estimated incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 1%–4% of traumatic head injuriesTraumatic Head InjuriesEpidural Hemorrhage
Accompanied by skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: AnatomyfractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures in > 75% of cases
Highest incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in young adults aged 20–30 years
Rare in older adults > 50 years of age
Etiology[1–3]
Head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma/injury:
Most common cause of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage
Causes injury to the vascular structures that course between the dural meningeal layers and the skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy
The trauma transmits forces to the skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy base, causing injury to the:
Nontraumatic EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage:
Rare
Possible etiologies include:
Infection:
MeningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis
Epidural abscessEpidural abscessCircumscribed collections of suppurative material occurring in the spinal or intracranial epidural space. The majority of epidural abscesses occur in the spinal canal and are associated with osteomyelitis of a vertebral body; analgesia, epidural; and other conditions. Clinical manifestations include local and radicular pain, weakness, sensory loss, urinary incontinence, and fecal incontinence. Cranial epidural abscesses are usually associated with osteomyelitis of a cranial bone, sinusitis, or otitis media.Retropharyngeal Abscess
Coagulopathy (inherited or iatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome)
Dural vascular malformations
Tumors affecting the dura materDura materThe outermost of the three meninges, a fibrous membrane of connective tissue that covers the brain and the spinal cord.Meninges: Anatomy
Approximately 90% of the cases of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage result from arterial bleeding:
Dural arteriovenous (AV) fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula at the vertex
Approximately 10% of the cases of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage result from venous bleeding (dural venous sinus).
Location:
EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage occurs in the temporal regionTemporal RegionEpidural Hemorrhage in 75% of cases.
EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage occurs in children with equal frequency in the following regions:
Temporal
OccipitalOccipitalPart of the back and base of the cranium that encloses the foramen magnum.Skull: Anatomy
FrontalFrontalThe bone that forms the frontal aspect of the skull. Its flat part forms the forehead, articulating inferiorly with the nasal bone and the cheek bone on each side of the face.Skull: Anatomy
Posterior fossa
Accompanied by fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures of the temporal boneTemporal boneEither of a pair of compound bones forming the lateral (left and right) surfaces and base of the skull which contains the organs of hearing. It is a large bone formed by the fusion of parts: the squamous (the flattened anterior-superior part), the tympanic (the curved anterior-inferior part), the mastoid (the irregular posterior portion), and the petrous (the part at the base of the skull).Jaw and Temporomandibular Joint: Anatomy in the majority of cases
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception expansion[1–3]
The total content of the intracranial space remains constant.
Vascular injury causes extravasation of blood into the epidural spaceEpidural spaceSpace between the dura mater and the walls of the vertebral canal.Epidural Hemorrhage, which is initially compensated by venous shunting of blood:
Intracranial pressureIntracranial PressureIdiopathic Intracranial Hypertension (ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP)) increases with hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception expansion.
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception expansion may be asymptomatic until the volume reaches a critical massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast.
As ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) increases due to hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception expansion, neurologic deterioration ensues:
Oculomotor nerveOculomotor nerveThe 3D cranial nerve. The oculomotor nerve sends motor fibers to the levator muscles of the eyelid and to the superior rectus, inferior rectus, and inferior oblique muscles of the eye. It also sends parasympathetic efferents (via the ciliary ganglion) to the muscles controlling pupillary constriction and accommodation. The motor fibers originate in the oculomotor nuclei of the midbrain.The 12 Cranial Nerves: Overview and Functions → pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
BrainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification stem → Cushing reflexCushing ReflexEpidural Hemorrhage (bradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias, hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, respiratory compromise)
Cerebral peduncle → hemiparesisHemiparesisThe term hemiparesis refers to mild to moderate weakness involving one side of the body.Epidural Hemorrhage
Progression to comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Progression to death
Clinical Presentation
Head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma is the most common etiology of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage. A “lucid intervalLucid IntervalEpidural Hemorrhage” followed by rapid neurologic deterioration is common.
Neurologic symptoms[1,2]
The nature of neurologic symptoms/signs depend largely on the following characteristics of the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception:
Location
Size
Rate of growth
Acuity
Loss of consciousness:
May range from momentary loss of consciousness to comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Typical: momentary loss of consciousness immediately after the traumatic eventTraumatic eventAn emotionally painful, shocking, stressful, and sometimes life-threatening experience. It can result from witnessing distressing events such as natural disasters, physical or sexual abuse, and terrorism or other acts of violence.Posttraumatic Stress Disorder (PTSD) → spontaneous recovery for a period of time → progressive neurologic deterioration due to progressive bleeding and hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception expansion:
Observed in approximately 50% of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage cases
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics/vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Drowsiness
Confusion
Common signs:
HemiparesisHemiparesisThe term hemiparesis refers to mild to moderate weakness involving one side of the body.Epidural Hemorrhage
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
BradycardiaBradycardiaBradyarrhythmia is a rhythm in which the heart rate is less than 60/min. Bradyarrhythmia can be physiologic, without symptoms or hemodynamic change. Pathologic bradyarrhythmia results in reduced cardiac output and hemodynamic instability causing syncope, dizziness, or dyspnea.Bradyarrhythmias
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
Respiratory compromise
Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma)[4,5]
MotorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology response (M)
Total points = E + V + M
If unable to assess one of the components, document a reason (do not default to a score of 1).
Classifying traumatic brain injuryTraumatic brain injuryA form of acquired brain injury which occurs when a sudden trauma causes damage to the brain.Le Fort Fractures (TBI):
Mild TBI: GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma 13–15
Moderate TBI: GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma 9–12
Severe TBI: GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma 3–8
Table: Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma)[5]
Description
Points
Eye opening
Spontaneous
4
Responds to speech
3
Responds to painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
2
None
1
Best verbal response
Oriented
5
Confused
4
Inappropriate words
3
Incomprehensible words
2
None
1
Best motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology response
Obeys commands
6
Localizes painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
5
Withdraws from painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Decerebrate posturingDecerebrate posturingA condition characterized by abnormal posturing of the limbs that is associated with injury to the brainstem. This may occur as a clinical manifestation or induced experimentally in animals. The extensor reflexes are exaggerated leading to rigid extension of the limbs accompanied by hyperreflexia and opisthotonus. This condition is usually caused by lesions which occur in the region of the brainstem that lies between the red nuclei and the vestibular nuclei. In contrast, decorticate rigidity is characterized by flexion of the elbows and wrists with extension of the legs and feet. The causative lesion for this condition is located above the red nuclei and usually consists of diffuse cerebral damage.Increased Intracranial Pressure (ICP) (extensionExtensionExamination of the Upper Limbs)
2
None
1
Glasgow Coma Scale scoring is between 3 and 15 (3 is the worst, 15 is the best).
Diagnosis
NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant[1–4,6]
Noncontrast head CT:
Imaging modality of choice for:
Acute head traumaHead traumaHead trauma occurs when external forces are directed to the skull and brain structures, resulting in damage to the skull, brain, and intracranial structures. Head injuries can be classified as open (penetrating) or closed (blunt), and primary (from the initial trauma) or secondary (indirect brain injury), and range from mild to severe and life-threatening. Head Trauma
Acute loss of consciousness (LOC)
Suspected EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage (and other intracranial bleeds)
Indications for CT in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with TBI:[4,6]
Mild TBI (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma 13–15) with LOC, amnesia, disorientationDisorientationSt. Louis Encephalitis Virus, and 1 of the following:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma < 15 at 2 hours after injury
Suspected open or depressed skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: AnatomyfractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures
Sign of basilar skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: AnatomyfractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures (e.g., hemotympanum, “panda eyes,” leakage of cerebrospinal fluidCerebrospinal FluidA watery fluid that is continuously produced in the choroid plexus and circulates around the surface of the brain; spinal cord; and in the cerebral ventricles.Ventricular System: Anatomy from the ear or noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal), Battle sign)
≥ 2 episodes of vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Age > 65 years
Anticoagulant use
LOC > 5 minutes
Amnesia for events immediately before impact
Dangerous mechanism of injury (pedestrian vs. motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology vehicle, ejection from motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology vehicle, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).)
Moderate (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma 9–12) or Severe TBI (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma ≤ 8)
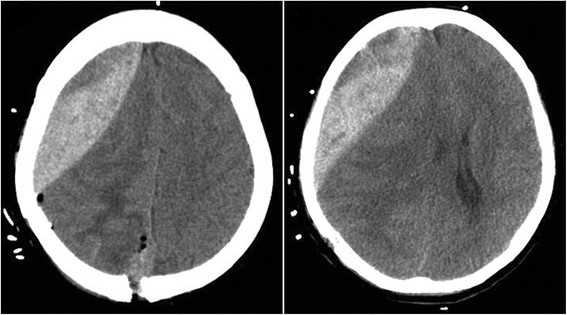
Acute EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage appears as a high-density lens-shaped (biconvex) collection of blood along the convexity of the affected hemisphere.
Fresh blood appears as high intensity on CT.
Acute blood collection is easily distinguishable from the surrounding anatomy.
In contrast, subdural hematomas (SDHs) follow the contours of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification.[4]
An indication for immediate neurosurgical intervention
Poor prognostic indicatorIndicatorMethods for assessing flow through a system by injection of a known quantity of an indicator, such as a dye, radionuclide, or chilled liquid, into the system and monitoring its concentration over time at a specific point in the system.Body Fluid Compartments
In < 10% of cases, the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception may not be readily apparent on initial CT:
CT performed before adequate blood accumulation
Severe anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types lessens the density of blood collection.
Severe hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension (due to associated trauma, blood loss, hypovolemiaHypovolemiaSepsis in Children) leads to slow bleeding.
A venous source of bleed leads to slow bleeding.
Head MRI:
Less widely used and not as readily available as CT
More sensitive in the detection of intracranial hemorrhageIntracranial hemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most sahs originate from a saccular aneurysm in the circle of willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use.Subarachnoid Hemorrhage compared with noncontrast CT
Adjunct to CT in cases where the initial CT is nondiagnostic but the clinical suspicion for EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage is high
May reveal the presence of other intracranial bleeding and/or the extent of associated intraparenchymal injuries
AngiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery:
Not typically indicated for the evaluation of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage
May be useful for the detection of atypical sources of bleeding
Contraindicated in cases where EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage is suspected
↑ ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) due to expanding hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception increases the risk of herniationHerniationOmphalocele
Epidural hematoma: CT showing an epidural hematoma in front of the surgical field after tumor resection
Image: “Ipsilateral remote hemorrhage in case 2. c, d CT showed an epidural hematoma in front of the surgical field after the tumor resection” by Yu J., et al. License: CC BY 4.0, cropped by Lecturio.
Management may vary based on location. The following recommendations are based on US and European guidelines.
Acute EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage, especially if presenting with neurologic compromise or comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma, is an emergent neurologic situation often requiring surgical intervention. Failure of prompt stabilization, diagnosis, evaluation, and intervention could result in hemorrhagic expansion, parenchymal brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification injury, elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and ClassificationherniationHerniationOmphalocele, and death.
Stabilization
Affected individuals should be evaluated and stabilized using advanced trauma life support (ATLS)/advanced cardiac life support (ACLS) protocols:[4]
AirwayAirwayABCDE Assessment patency: GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma < 8, intubate
Breathing: oxygenation/ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing adequacy
Chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests
Focused Assessment by SonographySonographyThe visualization of deep structures of the body by recording the reflections or echoes of ultrasonic pulses directed into the tissues. Use of ultrasound for imaging or diagnostic purposes employs frequencies ranging from 1. 6 to 10 megahertz.Diagnostic Procedures in Gynecology in Trauma (FAST) exam
Efforts to achieve/maintain hemodynamic stability:[4,5]
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension: IV fluid/blood products
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension: painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
AntiplateletsAntiplateletsDrugs or agents which antagonize or impair any mechanism leading to blood platelet aggregation, whether during the phases of activation and shape change or following the dense-granule release reaction and stimulation of the prostaglandin-thromboxane system.Heart Failure and Chronic Coronary Syndrome Medication (aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs), clopidogrelClopidogrelA ticlopidine analog and platelet purinergic p2y receptor antagonist that inhibits adenosine diphosphate-mediated platelet aggregation. It is used to prevent thromboembolism in patients with arterial occlusive diseases; myocardial infarction; stroke; or atrial fibrillation.Antiplatelet Drugs) reversed with plateletsPlateletsPlatelets are small cell fragments involved in hemostasis. Thrombopoiesis takes place primarily in the bone marrow through a series of cell differentiation and is influenced by several cytokines. Platelets are formed after fragmentation of the megakaryocyte cytoplasm. Platelets: Histology
WarfarinWarfarinAn anticoagulant that acts by inhibiting the synthesis of vitamin K-dependent coagulation factors. Warfarin is indicated for the prophylaxis and/or treatment of venous thrombosis and its extension, pulmonary embolism, and atrial fibrillation with embolization. It is also used as an adjunct in the prophylaxis of systemic embolism after myocardial infarction. Warfarin is also used as a rodenticide.Anticoagulants reversed with:
4-Factor (containing II, VII, IX, and X) prothrombinProthrombinA plasma protein that is the inactive precursor of thrombin. It is converted to thrombin by a prothrombin activator complex consisting of factor Xa, factor V, phospholipid, and calcium ions.Hemostasis complex concentrate (PCC)
Vitamin KVitamin KA lipid cofactor that is required for normal blood clotting. Several forms of vitamin K have been identified: vitamin K 1 (phytomenadione) derived from plants, vitamin K 2 (menaquinone) from bacteria, and synthetic naphthoquinone provitamins, vitamin K 3 (menadione). Vitamin k 3 provitamins, after being alkylated in vivo, exhibit the antifibrinolytic activity of vitamin k. Green leafy vegetables, liver, cheese, butter, and egg yolk are good sources of vitamin k.Fat-soluble Vitamins and their Deficiencies
Unfractionated heparinUnfractionated heparinA highly acidic mucopolysaccharide formed of equal parts of sulfated d-glucosamine and d-glucuronic acid with sulfaminic bridges. The molecular weight ranges from six to twenty thousand. Heparin occurs in and is obtained from liver, lung, mast cells, etc. , of vertebrates. Its function is unknown, but it is used to prevent blood clotting in vivo and vitro, in the form of many different salts.Anticoagulants, as well as low-molecular-weight heparin, is reversed with protamine sulfateProtamine sulfateA group of simple proteins that yield basic amino acids on hydrolysis and that occur combined with nucleic acid in the sperm of fish. Protamines contain very few kinds of amino acids. Protamine sulfate combines with heparin to form a stable inactive complex; it is used to neutralize the anticoagulant action of heparin in the treatment of heparin overdose.Anticoagulants.
DabigatranDabigatranA thrombin inhibitor which acts by binding and blocking thrombogenic activity and the prevention of thrombus formation. It is used to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation.Anticoagulants, a direct thrombin inhibitorDirect Thrombin InhibitorAnticoagulants, is reversed with:
RivaroxabanRivaroxabanA morpholine and thiophene derivative that functions as a factor Xa inhibitor and is used in the treatment and prevention of deep-vein thrombosis and pulmonary embolism. It is also used for the prevention of stroke and systemic embolization in patients with non-valvular atrial fibrillation, and for the prevention of atherothrombotic events in patients after an acute coronary syndrome.Anticoagulants, apixabanApixabanAnticoagulants and edoxabanEdoxabanAnticoagulants (direct oral factor Xa inhibitors) is reversed with:
Activated charcoalCharcoalAn amorphous form of carbon prepared from the incomplete combustion of animal or vegetable matter, e.g., wood. The activated form of charcoal is used in the treatment of poisoning.Antidotes of Common Poisonings (within 2–6 hours after ingestion)
Noncontrast head CT as soon as possible
Reasons for neurosurgical consultation:
Surgical/clinical decision-making
Placement of an ICP-monitoring device
Immediate neurosurgical consult in:[6]
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma ≥ 8 after initial resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome
Unexplained confusion that persists for more than 4 hours
Deterioration in GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score after admission (greater attentionAttentionFocusing on certain aspects of current experience to the exclusion of others. It is the act of heeding or taking notice or concentrating.Psychiatric Assessment should be paid to motorMotorNeurons which send impulses peripherally to activate muscles or secretory cells.Nervous System: Histology response deterioration)
Cerebrospinal fluidCerebrospinal FluidA watery fluid that is continuously produced in the choroid plexus and circulates around the surface of the brain; spinal cord; and in the cerebral ventricles.Ventricular System: Anatomy leak
Stratification[3,7]
Decision-making tools used clinically to determine operative or nonoperative management include:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score
Head CT findings:
Clot thickness
Degree of midline shift
Presence of associated brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification lesions
Neurologic examination
Presence of pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Acuity of EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage
Presence of comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus
Severity of associated trauma
Age: older age is associated with a worse prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas.
Nonoperative management[3,6,7]
May be appropriate for individuals with ALL of the following:[7]
Clinically stable individuals (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score > 8)
Small hematomas:
Clot thickness < 15 mm
Estimated EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage volume < 30 mL
Absence of signs of brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and ClassificationherniationHerniationOmphalocele based on clinical and/or radiographic evaluation:
Absence of physical examination findings of elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) (i.e., papilledemaPapilledemaSwelling of the optic disk, usually in association with increased intracranial pressure, characterized by hyperemia, blurring of the disk margins, microhemorrhages, blind spot enlargement, and engorgement of retinal veins. Chronic papilledema may cause optic atrophy and visual loss.Idiopathic Intracranial Hypertension, anisocoriaAnisocoriaUnequal pupil size, which may represent a benign physiologic variant or a manifestation of disease. Pathologic anisocoria reflects an abnormality in the musculature of the iris (iris diseases) or in the parasympathetic or sympathetic pathways that innervate the pupil. Physiologic anisocoria refers to an asymmetry of pupil diameter, usually less than 2mm, that is not associated with disease.Pupil: Physiology and Abnormalities)
Absence of elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) on neuromonitoring (i.e., < 30 mm Hg)
Monitor in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus with serial 1- hour neurologic exams.[6]
Continuous ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitoring is necessary.
Serial head CT scans should be performed every 6–8 hours for 36 hours.
HematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception may resolve or undergo gradual resorption over weeks.
Occasionally, EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage persists and does not resolve spontaneously.
Persistent EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage is an indication for neurosurgical evacuation.
Surgical management[3,4,6,7]
May be appropriate for:
Clinically unstable individuals:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score < 9
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score reduction by ≥ 2 from the time of injury to the time of evaluation
Presence of pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Large hematomas:
Clot thickness > 15 mm
Estimated EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage volume > 30 mL
Midline shift on CT by > 5 mm, regardless of the GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score
ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) > 30 mm Hg
Persistent EDHEDHEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury.Epidural Hemorrhage that does not resorb spontaneously over a course of weeks
Should be undertaken as soon as clinically feasible for affected individuals meeting these criteria (within 1–2 hours of the onset of neurologic deterioration)
Surgical techniques:
CraniotomyCraniotomySurgical incision into the cranium.Neurosurgery with hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception evacuation is the most commonly performed surgical technique.
Decompressive craniectomyDecompressive CraniectomyExcision of part of the skull. This procedure is used to treat elevated intracranial pressure that is unresponsive to conventional treatment.Neurosurgery
IdentificationIdentificationDefense Mechanisms of the culprit vessel and tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis may be undertaken simultaneously:
Traditional tamponadeTamponadePericardial effusion, usually of rapid onset, exceeding ventricular filling pressures and causing collapse of the heart with a markedly reduced cardiac output.Pericarditis with ligatures
Endovascular embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding of the middle meningeal arteryMiddle Meningeal ArteryEpidural Hemorrhage
Managing ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) (3 Tiers)[4–6]
Tier 1:
Head of bed elevated 30 degrees (reverse Trendelenburg)
Short-acting sedation or anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts agents in intubated patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship (propofolPropofolAn intravenous anesthetic agent which has the advantage of a very rapid onset after infusion or bolus injection plus a very short recovery period of a couple of minutes. Propofol has been used as anticonvulsants and antiemetics.Intravenous Anesthetics, fentanylFentanylA potent narcotic analgesic, abuse of which leads to habituation or addiction. It is primarily a mu-opioid agonist. Fentanyl is also used as an adjunct to general anesthetics, and as an anesthetic for induction and maintenance.Opioid Analgesics, midazolamMidazolamA short-acting hypnotic-sedative drug with anxiolytic and amnestic properties. It is used in dentistry, cardiac surgery, endoscopic procedures, as preanesthetic medication, and as an adjunct to local anesthesia. The short duration and cardiorespiratory stability makes it useful in poor-risk, elderly, and cardiac patients. It is water-soluble at ph less than 4 and lipid-soluble at physiological pH.Benzodiazepines)
Ventricular drainage performed intermittently
Repeat CT imaging and neurologic examination to check for any new or expanding massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast lesions.
If ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) remains ≥ 20–25 mm Hg, proceed to Tier 2.
Tier 2:
In patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a parenchymal ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) monitor, an external ventricular drain should be considered to allow for intermittent CSF drainage.
Hyperosmolar therapy should be administered intermittently as needed for ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) elevation.
MannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics in intermittent boluses: 0.25–1 g/kg body weight (with caution in hypovolemic patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship):
Serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia and osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation check every 6 hours
Dose is held if serum osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation is > 320 mOsm/L.
Intermittent boluses of 3% NaCl solution (hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia), 250 mL over 30 minutes:
Check serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia and osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation every 6 hours.
Dose is held if serum Na is > 160 mEq/L.
Repeat CT imaging and neurologic examination to check for new or expanding massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast lesions.
Trial of neuromuscular blockadeNeuromuscular BlockadeThe intentional interruption of transmission at the neuromuscular junction by external agents, usually neuromuscular blocking agents. It is distinguished from nerve block in which nerve conduction (neural conduction) is interrupted rather than neuromuscular transmission. Neuromuscular blockade is commonly used to produce muscle relaxation as an adjunct to anesthesia during surgery and other medical procedures. It is also often used as an experimental manipulation in basic research. It is not strictly speaking anesthesia but is grouped here with anesthetic techniques. The failure of neuromuscular transmission as a result of pathological processes is not included here.Aminoglycosides (test dose) if initial measures fail to lower ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP)
If ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) remains ≥ 20–25 mmHg, proceed to Tier 3.
Tier 3:
Surgical management (decompressive hemicraniectomyHemicraniectomyNeurosurgery or bilateral craniectomy) if Tiers 1 and 2 measures are insufficient.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[1–3,7]
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score > 8 on presentation
Surgical intervention is prompt (1–2 hours from the time of injury).
Up to 55% if surgical intervention is delayed
Favorable recovery at 6 months in 50%–90% of cases if:
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score > 8 on presentation
Surgical intervention is prompt (1–2 hours from the time of injury).
Poor prognostic indicators:
Low GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma score on initial evaluation
Presence of pupillary palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
Older age
Delayed surgical intervention
Elevated ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP) in the postoperative periodPostoperative periodThe period following a surgical operation.Postoperative Care
Large hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception volume
Other intracranial bleeds (e.g., subarachnoid hemorrhageSubarachnoid HemorrhageSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage (SAHSAHSubarachnoid hemorrhage (SAH) is a type of cerebrovascular accident (stroke) resulting from intracranial hemorrhage into the subarachnoid space between the arachnoid and the pia mater layers of the meninges surrounding the brain. Most SAHs originate from a saccular aneurysm in the circle of Willis but may also occur as a result of trauma, uncontrolled hypertension, vasculitis, anticoagulant use, or stimulant use. Subarachnoid Hemorrhage), subdural hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception (SDHSDHSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage))
Cerebral contusion
Cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Differential Diagnosis
Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke: an ischemic infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage of a cerebral artery by atherosclerotic lesions or cardioembolic emboli. Ischemic strokeIschemic StrokeAn ischemic stroke (also known as cerebrovascular accident) is an acute neurologic injury that occurs as a result of brain ischemia; this condition may be due to cerebral blood vessel occlusion by thrombosis or embolism, or rarely due to systemic hypoperfusion. Ischemic Stroke presents with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/altered level of consciousnessAltered Level of ConsciousnessIntracerebral Hemorrhage that depends on the size and location of the infarctInfarctArea of necrotic cells in an organ, arising mainly from hypoxia and ischemiaIschemic Cell Damage. The diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management includes initial stabilization, possible cerebrovascular intervention, addressing identifiable underlying etiologies (severe hypertensionSevere hypertensionA confirmed blood pressure ≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic.Uncontrolled Hypertension, embolus), and management of cardiovascular risk factors.
Other hemorrhagic cerebral conditions: Carotid/cerebral artery dissection, intraparenchymal hemorrhage, and subdural hemorrhageSubdural HemorrhageSubdural hemorrhage (SDH) is bleeding into the space between the dural and arachnoid meningeal layers surrounding the brain. The most common mechanism triggering the bleeding event is trauma (e.g., closed head injury) causing a tearing injury to the extracerebral “bridging” veins.Subdural Hemorrhage are other hemorrhagic manifestations of the cerebral vasculature that can present with neurologic deficitsNeurologic DeficitsHigh-Risk Headaches and/or altered mental statusAltered Mental StatusSepsis in Children/altered level of consciousnessAltered Level of ConsciousnessIntracerebral Hemorrhage. Diagnosis is clinical and confirmed by neuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant. Management depends on the hemorrhagic etiology and includes initial stabilization, neurosurgical/endovascular consultation, management of ICPICPNormal intracranial pressure (ICP) is defined as < 15 mm Hg, whereas pathologically increased ICP is any pressure ≥ 20 mm Hg. Increased ICP may result from several etiologies, including trauma, intracranial hemorrhage, mass lesions, cerebral edema, increased CSF production, and decreased CSF absorption.Increased Intracranial Pressure (ICP), and monitoring in a neurologic ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus.
These codes are used to diagnose a traumatic epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage, a bleed between the dura materDura materThe outermost of the three meninges, a fibrous membrane of connective tissue that covers the brain and the spinal cord.Meninges: Anatomy and the skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy, often from a tear in the middle meningeal arteryMiddle Meningeal ArteryEpidural Hemorrhage. Codes require laterality and specify loss of consciousness.
Coding System
Code
Description
ICD-10-CM
S06.4X0A
Epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage without loss of consciousness, initial encounter
Evaluation & Workup:
This CPT code is for a non-contrast CT scan of the head, the essential and rapid imaging study to diagnose an epidural hemorrhageEpidural HemorrhageEpidural hemorrhage (EDH) is an event characterized by bleeding into the epidural space between the dural layers of the meninges and the skull. The primary mechanism triggering bleeding is trauma (i.e., closed head injury), which causes arterial injury, most commonly middle meningeal artery injury. Epidural Hemorrhage, which classically appears as a biconvex (lens-shaped) hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception.
Coding System
Code
Description
CPT
70450
Computed tomography, head or brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification; without contrast material
Procedures/Interventions:
This code is for an emergent craniotomyCraniotomySurgical incision into the cranium.Neurosurgery, the neurosurgical procedure to evacuate the hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception, relieve pressure on the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification, and control the source of bleeding.
Coding System
Code
Description
CPT
61312
Craniectomy or craniotomyCraniotomySurgical incision into the cranium.Neurosurgery for evacuation of hematomaHematomaA collection of blood outside the blood vessels. Hematoma can be localized in an organ, space, or tissue.Intussusception, supratentorial; extradural or subdural
Maugeri, R., Anderson, D. G., Graziano, F., et al. (2015). Conservative vs. surgical management of post-traumatic epidural hematoma: a case and review of literature. American Journal of Case Reports, 16, 811–817. https://doi.org/10.12659/ajcr.895231
National Institute for Health and Care Excellence. (2019). Head injury: assessment and early management. Retrieved September 27, 2022, from https://www.nice.org.uk/guidance/cg176
Dhakal, P., Rayamajhi, S., Verma, V., Gundabolu, K., Bhatt, V. R. (2017). Reversal of anticoagulation and management of bleeding in patients on anticoagulants. Clinical and Applied Thrombosis/Hemostasis, 23(5), 410–415. https://doi.org/10.1177/1076029616675970
Chaudhary, R., Singh, A., Chaudhary, R., Bashline, M., Houghton, D. E., Rabinstein, A., Adamski, J., Arndt, R., Ou, N. N., Rudis, M. I., Brown, C. S., Wieruszewski, E. D., Wanek, M., Brinkman, N. J., Linderbaum, J. A., Sorenson, M. A., Atkinson, J. L., Thompson, K. M., Aiyer, A. N., McBane, R. D., 2nd. (2022). Evaluation of direct oral anticoagulant reversal agents in intracranial hemorrhage: a systematic review and meta-analysis. JAMA Network Open, 5(11), e2240145. https://doi.org/10.1001/jamanetworkopen.2022.40145
Create your free account or log in to continue reading!