Dacryocystitis is the inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. The chronic type has a gradual course, often manifesting with epiphora. Dacryocystitis can be congenital or acquired. The most common etiology of congenital dacryocystitis is nasolacrimal duct obstruction, which affects 6% of newborns. Acquired cases typically occur in adults and are due to trauma, systemic diseases, or tumors. Diagnosis is made clinically. In some cases, laboratory tests and imaging help determine abnormal structures and underlying disease. Initial treatment includes conservative measures such as Crigler massage, warm compresses, and antibiotics, if indicated. If these fail, surgical options are available.
DacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis is an inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the lacrimal sacLacrimal SacDacryocystitis due to nasolacrimal ductNasolacrimal DuctNasolacrimal duct.Dacryocystitis (NLD) obstruction and the subsequent stasis of tears.
Obstruction is a common cause of congenital nasolacrimal ductNasolacrimal DuctNasolacrimal duct.Dacryocystitis obstruction in infants (persistent membrane at Hasner’s valve).
Spontaneous resolution in 80‒90% of affected infants by 10 months of life
In adults, women > men, with the following factors in women contributing to NLD obstruction:
Narrower bony NLD
Membranous NLD is more tortuous.
Lacrimal sacLacrimal SacDacryocystitis mucosal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation resulting from postmenopausal hormonal changes
Most common cause: membranous obstruction at the valve of HasnerValve of HasnerDacryocystitis due to incomplete canalization of the nasolacrimal apparatus
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of 1%–12%
Obstruction at both proximal and distal portions of nasolacrimal ductNasolacrimal DuctNasolacrimal duct.Dacryocystitis system
Proximal: blockage at the common canaliculus or the valve of Rosenmüller
Tumors: primary lacrimal sacLacrimal SacDacryocystitis tumors and benignBenignFibroadenomapapillomaPapillomaA circumscribed benign epithelial tumor projecting from the surrounding surface; more precisely, a benign epithelial neoplasm consisting of villous or arborescent outgrowths of fibrovascular stroma covered by neoplastic cells.Cowden Syndrome or malignancies
Trauma: nasal fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures and surgery
Inflammatory disease: sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis, granulomatosis with polyangiitisGranulomatosis with PolyangiitisA multisystemic disease of a complex genetic background. It is characterized by inflammation of the blood vessels (vasculitis) leading to damage in any number of organs. The common features include granulomatous inflammation of the respiratory tract and kidneys. Most patients have measurable autoantibodies (antineutrophil cytoplasmic antibodies) against myeloblastin.Granulomatosis with Polyangiitis
SinusitisSinusitisSinusitis refers to inflammation of the mucosal lining of the paranasal sinuses. The condition usually occurs concurrently with inflammation of the nasal mucosa (rhinitis), a condition known as rhinosinusitis. Acute sinusitis is due to an upper respiratory infection caused by a viral, bacterial, or fungal agent. Sinusitis: maxillary and ethmoidal
Medications: timololTimololA beta-adrenergic antagonist that is similar in action to propranolol; the levo-isomer is more active. Timolol has been proposed as an anti-hypertensive, anti-arrhythmic, anti-angina, and anti-glaucoma agent. It is also used in the treatment of migraine disorders and tremor.Class 2 Antiarrhythmic Drugs (Beta Blockers), pilocarpinePilocarpineA slowly hydrolyzed muscarinic agonist with no nicotinic effects. Pilocarpine is used as a miotic and in the treatment of glaucoma.Cholinomimetic Drugs, dorzolamide, idoxuridine, and trifluridine
Obstruction leads to stagnation of tears, providing an environment for bacterial growth.
Common organisms in local infection or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease:
Staphylococcus epidermidisStaphylococcus epidermidisA species of staphylococcus that is a spherical, non-motile, gram-positive, chemoorganotrophic, facultative anaerobe. Mainly found on the skin and mucous membrane of warm-blooded animals, it can be primary pathogen or secondary invader.Staphylococcus and S. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus
Alpha-hemolytic streptococci: S. pneumoniae, S. viridans
Pseudomonas aeruginosaPseudomonas aeruginosaA species of gram-negative, aerobic, rod-shaped bacteria commonly isolated from clinical specimens (wound, burn, and urinary tract infections). It is also found widely distributed in soil and water. P. Aeruginosa is a major agent of nosocomial infection.Pseudomonas
Systemic diseases (including sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis, systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus (SLESLESystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus), and granulomatosis with polyangiitisGranulomatosis with PolyangiitisA multisystemic disease of a complex genetic background. It is characterized by inflammation of the blood vessels (vasculitis) leading to damage in any number of organs. The common features include granulomatous inflammation of the respiratory tract and kidneys. Most patients have measurable autoantibodies (antineutrophil cytoplasmic antibodies) against myeloblastin.Granulomatosis with Polyangiitis)
Acute dacryocystitisAcute DacryocystitisDacryocystitis: Symptoms present within hours or days (with pediatric cases having more rapid progression).[7,8,13]
Fluctuating visual acuityVisual AcuityClarity or sharpness of ocular vision or the ability of the eye to see fine details. Visual acuity depends on the functions of retina, neuronal transmission, and the interpretative ability of the brain. Normal visual acuity is expressed as 20/20 indicating that one can see at 20 feet what should normally be seen at that distance. Visual acuity can also be influenced by brightness, color, and contrast.Ophthalmic Exam: Increased tear film refracts light abnormally.
MucoceleMucoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis:
Also called dacryoceleDacryoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis or dacryocystoceleDacryocystoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis
Palpable massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast (formed from trapped fluid) at the medial canthus
Complications
Complications involving other ocular structures:[8,11]
Preseptal cellulitisPreseptal cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection anterior to the orbital septum is preseptal cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis:
Infectious inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the structures anterior to the orbital septumOrbital SeptumOrbital and Preseptal Cellulitis (skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess)
Presents with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, swellingSwellingInflammation, rednessRednessInflammation, and discharge
Orbital cellulitisOrbital cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection posterior to the septum is orbital cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis:
Infectious inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the structures posteriorto the orbital septumOrbital SeptumOrbital and Preseptal Cellulitis (orbital fat, muscles, boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types)
Presents with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, rednessRednessInflammation, discharge, swellingSwellingInflammation, proptosisProptosisRetinoblastoma, diplopiaDiplopiaA visual symptom in which a single object is perceived by the visual cortex as two objects rather than one. Disorders associated with this condition include refractive errors; strabismus; oculomotor nerve diseases; trochlear nerve diseases; abducens nerve diseases; and diseases of the brain stem and occipital lobe.Myasthenia Gravis, and abnormal eye movement
Less common complication (of dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis) than preseptal cellulitisPreseptal cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection anterior to the orbital septum is preseptal cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis
Complications beyond the eye:[11,13]
MeningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the meningesMeningesThe brain and the spinal cord are enveloped by 3 overlapping layers of connective tissue called the meninges. The layers are, from the most external layer to the most internal layer, the dura mater, arachnoid mater, and pia mater. Between these layers are 3 potential spaces called the epidural, subdural, and subarachnoid spaces. Meninges: Anatomy
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock: infection associated with life-threatening organ dysfunction
Cavernous sinus thrombosisCavernous sinus thrombosisFormation or presence of a blood clot (thrombus) in the cavernous sinus of the brain. Infections of the paranasal sinuses and adjacent structures, craniocerebral trauma, and thrombophilia are associated conditions. Clinical manifestations include dysfunction of cranial nerves III, IV, V, and VI, marked periorbital swelling, chemosis, fever, and visual loss.Cranial Nerve Palsies: embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding of infectious organism(s) causing thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus in the cavernous sinus
Left orbital cellulitis:
Photograph shows left upper and lower eyelid edema and erythema with conjunctival chemosis.
Image: “fig2: External photograph showing left upper and lower eyelid edema and erythema and conjunctival chemosis.” by Margaret L Pfeiffer, Alexander Hacopian, Helen Merritt, Margaret E Phillips, Karina Richani. License: CC BY 4.0
Right preseptal cellulitis:
Image shows marked, isolated, unilateral periocular inflammation. The individual presented with painless eye movement.
Image: “Figure 3.” by Monika Fida, Kocinaj Allma, Abazi Flora and Arjeta Grezda. License: CC BY 3.0
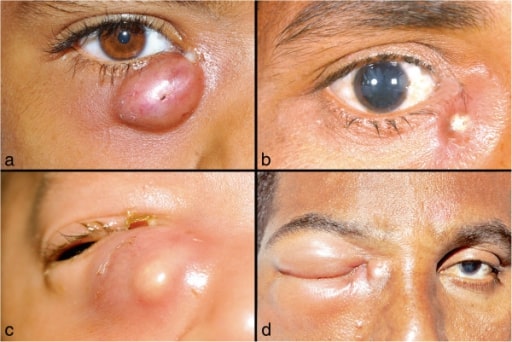
Images of lacrimal abscess: a. and b. Localized right lacrimal abscess, with discharge at the medial canthus; c. a neonate with right lacrimal abscess; d. Lacrimal abscess with orbital cellulitis
Image: “Dacryocystitis” by Dacryology Service, Ophthalmic Plastics Surgery, L,V, Prasad Eye Institute, Banjara Hills, Hyderabad 500034, India. License: CC BY 2.0
Chronic dacryocystitisChronic DacryocystitisDacryocystitis: epiphoraEpiphoraDacryocystitis, changes in visual acuityVisual AcuityClarity or sharpness of ocular vision or the ability of the eye to see fine details. Visual acuity depends on the functions of retina, neuronal transmission, and the interpretative ability of the brain. Normal visual acuity is expressed as 20/20 indicating that one can see at 20 feet what should normally be seen at that distance. Visual acuity can also be influenced by brightness, color, and contrast.Ophthalmic Exam, +/– palpable massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Visual acuityVisual AcuityClarity or sharpness of ocular vision or the ability of the eye to see fine details. Visual acuity depends on the functions of retina, neuronal transmission, and the interpretative ability of the brain. Normal visual acuity is expressed as 20/20 indicating that one can see at 20 feet what should normally be seen at that distance. Visual acuity can also be influenced by brightness, color, and contrast.Ophthalmic Exam testing:
Acute changes not explained by tear filming should prompt evaluation for a more involved condition (ophthalmology referral).
Nasal examination: to look for intranasal lesions
Further workup is also needed if patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with:
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion involving the whole orbit
Discharge expressed via Crigler (tear duct) massage
Guides antibiotic treatment
Additional testing obtained if underlying systemic disease is suspected:
Antinuclear antibody (ANA), double-stranded DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure (dsDNA): SLESLESystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus
Antineutrophil cytoplasmic antibody (ANCAANCAGroup of systemic vasculitis with a strong association with anca. The disorders are characterized by necrotizing inflammation of small and medium size vessels, with little or no immune-complex deposits in vessel walls.Rapidly Progressive Glomerulonephritis): granulomatosis with polyangiitisGranulomatosis with PolyangiitisA multisystemic disease of a complex genetic background. It is characterized by inflammation of the blood vessels (vasculitis) leading to damage in any number of organs. The common features include granulomatous inflammation of the respiratory tract and kidneys. Most patients have measurable autoantibodies (antineutrophil cytoplasmic antibodies) against myeloblastin.Granulomatosis with Polyangiitis
Serum angiotensin-converting enzyme (ACE): sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis
Fluorescein dyeFluorescein DyeOphthalmic Exam is placed into the patient’s eye, and after 5 minutes, an evaluation is done (with cobalt blue filter of slit lampSlit LampA microscope with a light source that can be projected into a linear beam. It allows cross-sectional viewing of the aqueous humor; conjuncteiva; cornea; eyelids; iris; and lens of the eye.Ophthalmic Exam).
Persistence of dye and asymmetric dye clearance: NLD obstruction confirmed
Imaging[10,13]
Computed tomography (CT) scan:
To evaluate structures in cases of trauma/fractures
To determine extent of infection/abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease
To differentiate a dacryocystoceleDacryocystoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis (a cysticCysticFibrocystic ChangemassMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast extending from the lacrimal duct) from endonasal cystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change
Ultrasonography: can also be used to evaluate a dacryocystoceleDacryocystoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis
Nasal endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)[10]
Evaluates intranasal pathology such as septal deviation, inferior meatal narrowing, and inferior turbinate hypertrophyHypertrophyGeneral increase in bulk of a part or organ due to cell enlargement and accumulation of fluids and secretions, not due to tumor formation, nor to an increase in the number of cells (hyperplasia).Cellular Adaptation
BiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma of the lacrimal gland[20]
Obtained (during dacryocystorhinostomy) if there is no response to standard medical treatment
Most common histopathology: chronic inflammationChronic InflammationInflammation with or without fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans (primary dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis)
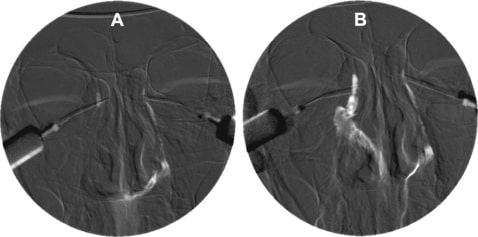
Digital subtraction dacryocystogram. A. Completely obstructed right NLD showing no flow of contrast medium. Normal left NLD B. Free flow of the contrast medium through the recanalized right NLD to the inferior meatus after surgery
Image: “Digital subtraction dacryocystogram” by Department of ENT, First Affiliated Hospital, Sun Yat-sen University, Guangzhou 510060, PR China. License: CC BY 2.0
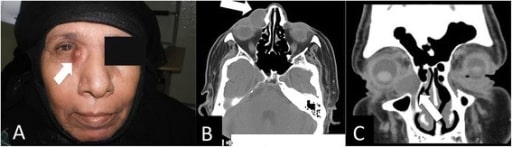
A. Clinical photo of a patient with right eye dacryocele B. CT axial cut showing the medial canthus dacryocele (white arrow) C. CT coronal cut showing the same finding (white arrow)
Image: “Clinical photo of a patient with right eye dacrocele” by Department of Otolaryngology, Zagazig University, Zagazig, Egypt. License: CC BY 4.0
Management
Congenital NLD obstruction[10,12]
Treatment is planned in consultation with an ophthalmologist.
Push index finger down on the lacrimal sacLacrimal SacDacryocystitis and slide the finger downward against the bony side of the noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal).
10 motions performed 3 times a day
Done until child is 1 year of age
90% of NLD obstructions resolve by 6–12 months of age (with highest rate noted in the 1st few months of life).
The patient is reevaluated by ophthalmology if NLD obstruction persists beyond 6–7 months.[15–17]
NLD probing is the 1st-line procedure.
Timing of the procedure is at the discretion of the specialist.
Performing the procedure at 6 months leads to in-office probing of some infants whose obstruction would have resolved spontaneously.
An alternative is to wait until the patient is ≥ 12 months as spontaneous resolution can still occur.
Waiting until age > 12 months:
Would lead to the need for general anesthesiaGeneral anesthesiaProcedure in which patients are induced into an unconscious state through use of various medications so that they do not feel pain during surgery.Anesthesiology: History and Basic Concepts for the procedure
Indicated to treat copious mucopurulent discharge without other signs of infection (e.g., no erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion or edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema present)
Commonly used agents:
Polymyxin B–trimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim
ErythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides
FluoroquinolonesFluoroquinolonesFluoroquinolones are a group of broad-spectrum, bactericidal antibiotics inhibiting bacterial DNA replication. Fluoroquinolones cover gram-negative, anaerobic, and atypical organisms, as well as some gram-positive and multidrug-resistant (MDR) organisms. Fluoroquinolones (if others are not effective)
The cyst is generally sterileSterileBasic Procedures when diagnosed; initial measure is Crigler massage with prophylactic topical antibiotics.
An uninfected dacryocystoceleDacryocystoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis can spontaneously resolve with conservative management.
Persistence requires NLD probing.
An infected dacryocystoceleDacryocystoceleA retention cyst of the salivary gland, lacrimal sac, paranasal sinuses, appendix, or gallbladder.Dacryocystitis requires systemic antibiotics and, in some cases, incision and drainageIncision And DrainageChalazion.
S. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus and S. pneumoniae are the most common.
Indicated when erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion or edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema is present
Typical duration of therapy: 7–10 days[8]
Choices include (but not limited to):
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate
Complicated cases with spread of infection or failure of oral antibiotics to resolve symptoms: IV antibiotics (coverage for gram-positiveGram-PositivePenicillins and gram-negative organisms)
Adults: cefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins
VancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides (dosing adjusted based on therapeutic monitoring)
Tailor antibiotics to culture results.
In cases of NLD obstruction (which is the main cause of acute dacryocystitisAcute DacryocystitisDacryocystitis in the pediatric age group):[7,13]
Continue the conservative measures until reevaluation (between 6 and 12 months of age).
If obstruction persists, perform NLD probing (success rate of which is around 70%).
If unsuccessful, a 2nd NLD probing can be performed (if age < 12 months).
For other alternative procedures after failure of NLD probing, consider procedures used to treat chronic dacryocystitisChronic DacryocystitisDacryocystitis.
In adults, dacryocystorhinostomy (performed externally or endonasally) is usually required.[13]
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate
875 mg every 12 hours
20–40 mg/kg/day in 3 divided doses
Cephalexin
500 mg every 6 hours
25–50 mg/kg/day divided every 6–12 hours
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides
300 mg every 6–8 hours
30–40 mg/kg/day in 3 divided doses
Complicated cases
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins
ConjunctivitisConjunctivitisConjunctivitis is a common inflammation of the bulbar and/or palpebral conjunctiva. It can be classified into infectious (mostly viral) and noninfectious conjunctivitis, which includes allergic causes. Patients commonly present with red eyes, increased tearing, burning, foreign body sensation, and photophobia. Conjunctivitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the conjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy, the outer lining of the eye. Etiology can be infectious or non-infectious. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with rednessRednessInflammation and discharge in one or both eyesBoth EyesRefractive Errors. Bacterial conjunctivitisBacterial ConjunctivitisConjunctivitis often has purulent dischargePurulent DischargeDacryocystitis, whereas viral causes have watery discharge.
HordeolumHordeolumA hordeolum is an acute infection affecting the meibomian, Zeiss, or Moll glands of the eyelid. Stasis of the gland secretions predisposes to bacterial infection. Staphylococcus aureus is the most common pathogen. Hordeolum (Stye)(styeStyeA hordeolum is an acute infection affecting the meibomian, Zeiss, or Moll glands of the eyelid. Stasis of the gland secretions predisposes to bacterial infection. Staphylococcus aureus is the most common pathogen. Hordeolum (Stye)): an abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease affecting the eyelash follicle or eyelid gland. StyeStyeA hordeolum is an acute infection affecting the meibomian, Zeiss, or Moll glands of the eyelid. Stasis of the gland secretions predisposes to bacterial infection. Staphylococcus aureus is the most common pathogen. Hordeolum (Stye) usually presents as a locally painful, erythematous, swollen eyelid margin. Most lesions resolve spontaneously, but gentle warm compressesWarm CompressesChalazion facilitate drainage. If the abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease does not resolve, incision and drainageIncision And DrainageChalazion by an ophthalmologist are performed.
ChalazionChalazionA chalazion is one of the most common inflammatory lesions of the eyelid. It is caused by obstruction of the Meibomian or Zeis glands, leading to granulomatous inflammation and resulting in a firm, rubbery, slow-growing nodule that is typically non-tender.Chalazion: a firm, nontender massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast at the eyelid resulting from obstruction of the Zeis or meibomian glands. The condition is usually managed conservatively with warm compressesWarm CompressesChalazion. Persistence of the lesion requires incision and curettageCurettageA scraping, usually of the interior of a cavity or tract, for removal of new growth or other abnormal tissue, or to obtain material for tissue diagnosis. It is performed with a curet (curette), a spoon-shaped instrument designed for that purpose.Benign Bone Tumors or glucocorticoid injection by an ophthalmologist.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis, an infection or inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the nasolacrimal sac. The codes distinguish between acute and chronic forms.
Coding System
Code
Description
ICD-10-CM
H04.30-
Acute and unspecified dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis
DacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis (disorder)
Procedures/Interventions:
These codes are for procedures to treat dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis. Acute abscesses may require incision and drainageIncision And DrainageChalazion, while chronic, recurrent cases are definitively treated with a dacryocystorhinostomy (DCR) to create a new drainage pathway.
Dacryocystorhinostomy (fistulization of lacrimal sacLacrimal SacDacryocystitis to nasal cavityNasal cavityThe proximal portion of the respiratory passages on either side of the nasal septum. Nasal cavities, extending from the nares to the nasopharynx, are lined with ciliated nasal mucosa.Nose Anatomy (External & Internal))
Medications:
This code is for an oral antibiotic like amoxicillin-clavulanate, which is used to treat the acute bacterial infection in dacryocystitisDacryocystitisDacryocystitis is inflammation of the lacrimal sac due to nasolacrimal duct obstruction and the subsequent stasis of tears. The condition can have an acute or chronic onset. Acute dacryocystitis presents within hours or days with redness, swelling, tenderness, and excessive tearing. Dacryocystitis.
Coding System
Code
Description
RxNorm
105822
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins / Clavulanate (ingredient)
Complications:
This code is for orbital cellulitisOrbital cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection posterior to the septum is orbital cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis, a serious complication where the infection spreads from the lacrimal sacLacrimal SacDacryocystitis to the soft tissues behind the orbital septumOrbital SeptumOrbital and Preseptal Cellulitis, requiring urgent treatment.
Coding System
Code
Description
ICD-10-CM
H05.01-
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis of orbit
References
Denniston, A., Murray, P. (2014). Oxford Handbook of Ophthalmology (3rd ed.). Oxford, UK: Oxford University Press.
Goldstein, T., Vargason, C., Goel, S., Chong, K., Barmettler, A., Yen, M., Alsuhaibani, A., Burkat, C.N., Lee, S., Sebastian, J.U. (2025) Dacryocystitis. American Academy of Ophthalmology. https://eyewiki.aao.org/Dacryocystitis
Sathiamoorthi, S., Frank, R. D., Mohney, B. G. (2018). Spontaneous resolution and timing of intervention in congenital nasolacrimal duct obstruction. JAMA Ophthalmology, 136(11), 1281–1286. https://doi.org/10.1001/jamaophthalmol.2018.3841
Alsalamah, A. K., Alkatan, H. M., Al-Faky, Y. H. (2018). Acute dacryocystitis complicated by orbital cellulitis and loss of vision: a case report and review of the literature. International Journal of Surgery Case Reports, 50, 130–134. https://doi.org/10.1016/j.ijscr.2018.07.045
Di Cicco, M., Bellino, E. M., Marabotti, A., Luti, L., Peroni, D. G., Baroncelli, G. I. (2020). Acute dacryocystitis with giant lacrimal abscess: a case report. Italian Journal of Pediatrics, 46(1), 15. https://doi.org/10.1186/s13052-020-0779-7
Miller, A. M., Chandler, D. L., Repka, M. X., et al. (2014). Office probing for treatment of nasolacrimal duct obstruction in infants. Journal of the American Association for Pediatric Ophthalmology and Strabismus, 18(1), 26–30. https://doi.org/10.1016/j.jaapos.2013.10.016
Pediatric Eye Disease Investigator Group. (2012). A randomized trial comparing the cost-effectiveness of 2 approaches for treating unilateral nasolacrimal duct obstruction. Archives of Ophthalmology, 130(12), 1525–1533. https://doi.org/10.1001/archophthalmol.2012.2853
Lee, M. J., Park, J., Kim, N., Choung, H. K., Khwarg, S. I. (2019). Conservative management of congenital dacryocystocele: resolution and complications. Canadian Journal of Ophthalmology, 54(4), 421–425. https://doi.org/10.1016/j.jcjo.2018.08.006
Cavazza, S., Laffi, G. L., Lodi, L., Tassinari, G., Dall’Olio, D. (2008). Congenital dacryocystocele: diagnosis and treatment. Acta Otorhinolaryngologica Italica, 28(6), 298–301.
Koturović, Z., Knežević, M., Rašić, D. M. (2017). Clinical significance of routine lacrimal sac biopsy during dacryocystorhinostomy: a comprehensive review of literature. Biomolecules and Biomedicine, 17(1), 1–8. https://doi.org/10.17305/bjbms.2016.1424
Create your free account or log in to continue reading!