Trigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal neuralgia occurs in multiple, short-acting episodes. Most cases are usually due to vascular compression of the trigeminal nerve, although secondary causes can be due to aneurysms, neuromas, or other neurologic disorders. A detailed history is the hallmark for diagnosis. Neuroimaging with MRI is useful to determine the exact pathology involving the trigeminal nerve root. The 1st line of therapy is pharmacologic (carbamazepine). Other treatment options include botulinum toxin injections or surgical procedures in refractory cases.
Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia (TN) is a disorder presenting with recurrent, sharp painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the distribution of the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions.
Anatomy of the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions[7,12]
Trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions (cranial nerve (CN) V):
The largest of all the cranial nervesCranial nervesThere are 12 pairs of cranial nerves (CNs), which run from the brain to various parts of the head, neck, and trunk. The CNs can be sensory or motor or both. The CNs are named and numbered in Roman numerals according to their location, from the front to the back of the brain.The 12 Cranial Nerves: Overview and Functions
Starts at the mid-lateral surface of the ponsPonsThe front part of the hindbrain (rhombencephalon) that lies between the medulla and the midbrain (mesencephalon) ventral to the cerebellum. It is composed of two parts, the dorsal and the ventral. The pons serves as a relay station for neural pathways between the cerebellum to the cerebrum.Brain Stem: Anatomy
SensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology ganglion (Gasser ganglion) reside in the floor of the middle cranial fossaMiddle cranial fossaThe compartment containing the anterior extremities and half the inferior surface of the temporal lobes (temporal lobe) of the cerebral hemispheres. Lying posterior and inferior to the anterior cranial fossa, it is formed by part of the temporal bone and sphenoid bone. It is separated from the posterior cranial fossa by crests formed by the superior borders of the petrous parts of the temporal bones.Skull: Anatomy.
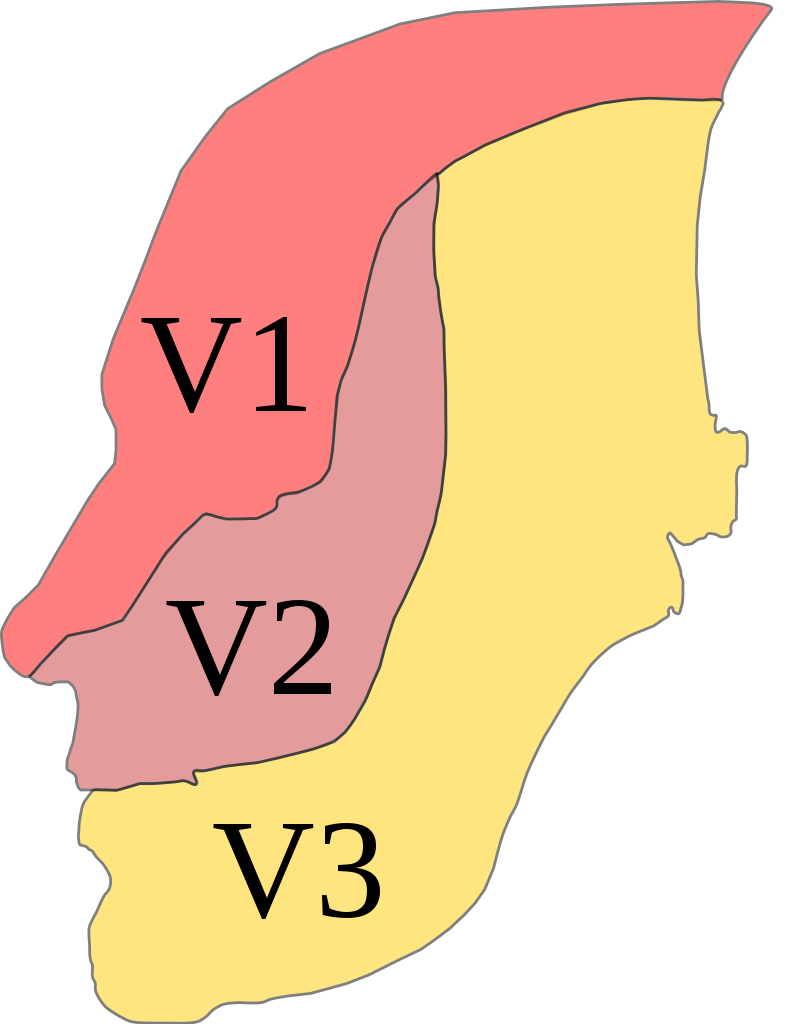
3 major divisions of CN V:
Ophthalmic (V1):
Exits the craniumCraniumThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy via the superior orbital fissureFissureA crack or split that extends into the dermisGeneralized and Localized Rashes
SensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology innervation of the foreheadForeheadThe part of the face above the eyes.Melasma, eyes, and noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal)
Maxillary (V2):
Exits the craniumCraniumThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy via the foramen rotundum
Innervation of the lower eyelid, teethTeethNormally, an adult has 32 teeth: 16 maxillary and 16 mandibular. These teeth are divided into 4 quadrants with 8 teeth each. Each quadrant consists of 2 incisors (dentes incisivi), 1 canine (dens caninus), 2 premolars (dentes premolares), and 3 molars (dentes molares). Teeth are composed of enamel, dentin, and dental cement.Teeth: Anatomy, nasal cavityNasal cavityThe proximal portion of the respiratory passages on either side of the nasal septum. Nasal cavities, extending from the nares to the nasopharynx, are lined with ciliated nasal mucosa.Nose Anatomy (External & Internal), gums of the upper jawUpper jawOne of a pair of irregularly shaped bones that form the upper jaw. A maxillary bone provides tooth sockets for the superior teeth, forms part of the orbit, and contains the maxillary sinus.Skull: Anatomy, palatePalateThe palate is the structure that forms the roof of the mouth and floor of the nasal cavity. This structure is divided into soft and hard palates. Palate: Anatomy, and tonsilsTonsilsTonsillitis
Autonomic innervation of the lacrimal and nasal glands
Mandibular (V3):
Exits the craniumCraniumThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy via the foramen ovaleForamen ovaleAn opening in the wall between the right and the left upper chambers (heart atria) of a fetal heart. Oval foramen normally closes soon after birth; when it fails to close the condition is called patent oval foramen.Patent Foramen Ovale
SensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology supply of the teethTeethNormally, an adult has 32 teeth: 16 maxillary and 16 mandibular. These teeth are divided into 4 quadrants with 8 teeth each. Each quadrant consists of 2 incisors (dentes incisivi), 1 canine (dens caninus), 2 premolars (dentes premolares), and 3 molars (dentes molares). Teeth are composed of enamel, dentin, and dental cement.Teeth: Anatomy, gums of the lower jawJawThe jaw is made up of the mandible, which comprises the lower jaw, and the maxilla, which comprises the upper jaw. The mandible articulates with the temporal bone via the temporomandibular joint (TMJ). The 4 muscles of mastication produce the movements of the TMJ to ensure the efficient chewing of food. Jaw and Temporomandibular Joint: Anatomy, buccal mucosaBuccal mucosaOral Cancer, dorsum of the tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, and external acoustic meatusExternal acoustic meatusEar: Anatomy
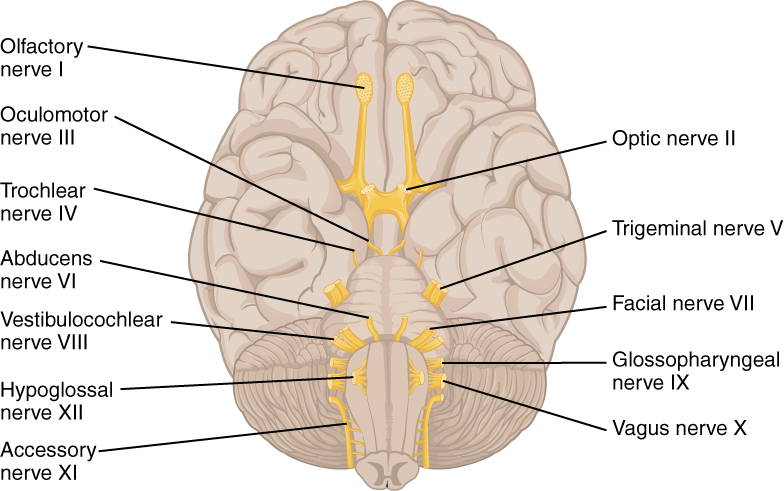
The 12 cranial nerves exiting the brain
Image: “The Cranial Nerves” by Phil Schatz. License: CC BY 4.0
Trigeminal distribution
Image: “Trig innervation” by Madhero88. License: CC BY 3.0, edited by Lecturio.
Epidemiology[1,2,5]
Annual incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 4–5 per 100,000
Ratio of men to women: 1:1.5
Onset is typically after 40 years old but may occur at any age.
Etiology[1–3,5,13]
Classic TN:
Approximately 75% of cases result from vascular (artery or vein) compressionCompressionBlunt Chest Trauma of the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions at the entry zone of the root.
Multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor
Vestibular schwannomaVestibular schwannomaAcoustic neuroma, also referred to as vestibular schwannoma, is a benign tumor arising from Schwann cells of the vestibular component of the cranial nerve VIII. Acoustic neuroma forms within the internal auditory meatus and extends into the cerebellopontine angle. Acoustic Neuroma (acoustic neuromaAcoustic neuromaAcoustic neuroma, also referred to as vestibular schwannoma, is a benign tumor arising from Schwann cells of the vestibular component of the cranial nerve VIII. Acoustic neuroma forms within the internal auditory meatus and extends into the cerebellopontine angle. Acoustic Neuroma)
MeningiomaMeningiomaMeningiomas are slow-growing tumors that arise from the meninges of the brain and spinal cord. The vast majority are benign. These tumors commonly occur in individuals with a history of high doses of skull radiation, head trauma, and neurofibromatosis 2. Meningioma
An epidermoid cyst or another cyst
Arteriovenous malformationArteriovenous malformationAbnormal formation of blood vessels that shunt arterial blood directly into veins without passing through the capillaries. They usually are crooked, dilated, and with thick vessel walls. A common type is the congenital arteriovenous fistula. The lack of blood flow and oxygen in the capillaries can lead to tissue damage in the affected areas.Erysipelas
Neurovascular contact is common in healthy individuals.
Diagnosed when no atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation or displacementDisplacementThe process by which an emotional or behavioral response that is appropriate for one situation appears in another situation for which it is inappropriate.Defense Mechanisms noted on MRI
In rare cases (3% of individuals with TN), painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways can be active on both sides at the same time.
The painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is a severe, sharp, shooting, or electric-shock–like sensation, lasting seconds to 2 minutes.
Facial grimacing or spasm may accompany the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways (tic douloureuxTic douloureuxTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles.Trigeminal Neuralgia).
Individuals report “triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation zones” (usually midline around the noseNoseThe nose is the human body’s primary organ of smell and functions as part of the upper respiratory system. The nose may be best known for inhaling oxygen and exhaling carbon dioxide, but it also contributes to other important functions, such as tasting. The anatomy of the nose can be divided into the external nose and the nasal cavity. Nose Anatomy (External & Internal) and lipsLipsThe lips are the soft and movable most external parts of the oral cavity. The blood supply of the lips originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy):
Even nonpainful stimuli in the triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation zones can cause painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways.
Stimuli include:
Chewing
Washing the face
Talking
Brushing the teethTeethNormally, an adult has 32 teeth: 16 maxillary and 16 mandibular. These teeth are divided into 4 quadrants with 8 teeth each. Each quadrant consists of 2 incisors (dentes incisivi), 1 canine (dens caninus), 2 premolars (dentes premolares), and 3 molars (dentes molares). Teeth are composed of enamel, dentin, and dental cement.Teeth: Anatomy
Shaving
Cold air
After the initial painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, a refractory period may last up to several minutes.
Stimulation of the triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation zone will not cause painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways during the refractory period.
May occur for extended periods of time (weeks to months)
In many cases, remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches can last at least 6 months.
Recurrence is common (frequency and severity wax and wane).
During periods with multiple attacks, affected individuals report depressed mood (↑ suicideSuicideSuicide is one of the leading causes of death worldwide. Patients with chronic medical conditions or psychiatric disorders are at increased risk of suicidal ideation, attempt, and/or completion. The patient assessment of suicide risk is very important as it may help to prevent a serious suicide attempt, which may result in death. Suicide risk) and disturbances in eating and sleeping.
Associated symptoms[1,2]
When other neurologic conditions (e.g., multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor or aneurysms) are present, additional symptoms may include:
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
Hearing lossHearing lossHearing loss, also known as hearing impairment, is any degree of impairment in the ability to apprehend sound as determined by audiometry to be below normal hearing thresholds. Clinical presentation may occur at birth or as a gradual loss of hearing with age, including a short-term or sudden loss at any point. Hearing Loss
TinnitusTinnitusA nonspecific symptom of hearing disorder characterized by the sensation of buzzing, ringing, clicking, pulsations, and other noises in the ear. Objective tinnitus refers to noises generated from within the ear or adjacent structures that can be heard by other individuals. The term subjective tinnitus is used when the sound is audible only to the affected individual. Tinnitus may occur as a manifestation of cochlear diseases; vestibulocochlear nerve diseases; intracranial hypertension; craniocerebral trauma; and other conditions.Cranial Nerve Palsies
Cutaneous tumors
Diagnosis
Diagnosis of TN is clinical, with a thorough history and physical. Further workup with imaging or laboratory studies may be required if red-flag symptoms are present.
History
Diagnostic criteria based on the International Classification of HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess Disorders, 3rd edition:[2]
Paroxysms or attacks of unilateral facial painUnilateral Facial PainTrigeminal Neuralgia are recurrent in areas supplied by 1 or more divisions of the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways characteristics:
Duration: a few seconds to ≤ 2 minutes
Severe intensity
Shooting, stabbing, sharp, or electric shock-like painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Innocuous stimuli within the affected trigeminal distribution triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways.
No other alternative diagnosis
Red-flag symptoms:
Age of onset < 40 years old
Changes in sensation
Deafness
History of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesions
Poor response to medications (carbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs)
Any permanent area of numbness excludes the diagnosis.
If sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology loss is found, exclude multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor (MSMSMultiple sclerosis (MS) is a chronic inflammatory autoimmune disease that leads to demyelination of the nerves in the CNS. Young women are more predominantly affected by this most common demyelinating condition.Multiple Sclerosis) or a structural lesion.
Ancillary studies
MRI:[3–5,7]
Recommended to rule out nerve compressionNerve CompressionBrachial Plexus Injuries or structural brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification lesion
High-resolution MRI with thin cuts through the region of the trigeminal ganglionTrigeminal ganglionThe semilunar-shaped ganglion containing the cells of origin of most of the sensory fibers of the trigeminal nerve. It is situated within the dural cleft on the cerebral surface of the petrous portion of the temporal bone and gives off the ophthalmic, maxillary, and part of the mandibular nerves.Trigeminal Neuralgia + heavy T2 weighting with or without contrast detects neurovascular compressionCompressionBlunt Chest Trauma (NVC).
Confirms morphologic changes such as dislocation, distortionDistortionDefense Mechanisms, atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation, or compressionCompressionBlunt Chest Trauma of the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions at the origin from the ponsPonsThe front part of the hindbrain (rhombencephalon) that lies between the medulla and the midbrain (mesencephalon) ventral to the cerebellum. It is composed of two parts, the dorsal and the ventral. The pons serves as a relay station for neural pathways between the cerebellum to the cerebrum.Brain Stem: Anatomy
CT:[3]
An alternative only when MRI is unavailable
Not as sensitive as MRI of the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Rules out a massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast lesion
Trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions reflexesandtrigeminal evoked potentials:[3,5,13]
If MRI is unavailable or not possible, testing trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions reflexes helps distinguish primary/classic TN from secondary TN (specificity, 87%).
In contrast, trigeminal evoked potentials are not recommended to identify secondary TN (low specificity).
However, in those with neuropathic facial painFacial painPain in the facial region including orofacial pain and craniofacial pain. Associated conditions include local inflammatory and neoplastic disorders and neuralgic syndromes involving the trigeminal, facial, and glossopharyngeal nerves. Conditions which feature recurrent or persistent facial pain as the primary manifestation of disease are referred to as facial pain syndromes.Trigeminal Neuralgia, both trigeminal reflexes and evoked potentials are used to detect trigeminal afferentAfferentNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology damage.
Laboratory workup:
Used at baseline to monitor adverse effects from medications
Includes CBC, serum electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy function panel
Management
Management may vary based on practice location. The following information is based on US and UK guidelines.
1st-line therapy: carbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs or oxcarbazepineOxcarbazepineA carbamazepine derivative that acts as a voltage-gated sodium channel blocker. It is used for the treatment of partial seizures with or without secondary generalization. It is also an inducer of cytochrome p-450 cyp3a4.First-Generation Anticonvulsant Drugs:[1–6,12]
Mechanism of action is inhibition of neuronal sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia channel activity to reduce the excitabilityExcitabilitySkeletal Muscle Contraction of neuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology.
58%–100% of individuals achieve complete or partial painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control (lack of response is a red-flag finding)
Common side effects: vertigoVertigoVertigo is defined as the perceived sensation of rotational motion while remaining still. A very common complaint in primary care and the ER, vertigo is more frequently experienced by women and its prevalence increases with age. Vertigo is classified into peripheral or central based on its etiology. Vertigo, sedation, ataxiaAtaxiaImpairment of the ability to perform smoothly coordinated voluntary movements. This condition may affect the limbs, trunk, eyes, pharynx, larynx, and other structures. Ataxia may result from impaired sensory or motor function. Sensory ataxia may result from posterior column injury or peripheral nerve diseases. Motor ataxia may be associated with cerebellar diseases; cerebral cortex diseases; thalamic diseases; basal ganglia diseases; injury to the red nucleus; and other conditions.Ataxia-telangiectasia, and nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics
Dosing:[14–15]
CarbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs 200–1200 mg/day divided into 1–2 doses, titrated up slowly to painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief or side-effect intolerance
Oxcarbamazepine 600–1800 mg/day divided into 2 doses, titrated up slowly to painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief or side-effect intolerance
Precautions:[14,15]
Prior to initiating carbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs or oxcarbazepineOxcarbazepineA carbamazepine derivative that acts as a voltage-gated sodium channel blocker. It is used for the treatment of partial seizures with or without secondary generalization. It is also an inducer of cytochrome p-450 cyp3a4.First-Generation Anticonvulsant Drugs, test for the HLA-BHLA-BClass I human histocompatibility (HLA) surface antigens encoded by more than 30 detectable alleles on locus B of the HLA complex, the most polymorphic of all the HLA specificities. Several of these antigens (e.g., hla-b27, -b7, -b8) are strongly associated with predisposition to rheumatoid and other autoimmune disorders. Like other class I HLA determinants, they are involved in the cellular immune reactivity of cytolytic T lymphocytes.Organ Transplantation*15:02alleleAlleleVariant forms of the same gene, occupying the same locus on homologous chromosomes, and governing the variants in production of the same gene product.Basic Terms of Genetics in genetically at-risk populations (e.g., Asian ancestry).
Avoid these drugs in the HLA-BHLA-BClass I human histocompatibility (HLA) surface antigens encoded by more than 30 detectable alleles on locus B of the HLA complex, the most polymorphic of all the HLA specificities. Several of these antigens (e.g., hla-b27, -b7, -b8) are strongly associated with predisposition to rheumatoid and other autoimmune disorders. Like other class I HLA determinants, they are involved in the cellular immune reactivity of cytolytic T lymphocytes.Organ Transplantation*15:02-positive group, as there is increased risk of toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome (TEN) and Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome.
Alternative agents (can be used individually or combined):[3–8]
BaclofenBaclofenA gamma-aminobutyric acid derivative that is a specific agonist of gaba-b receptors. It is used in the treatment of muscle spasticity, especially that due to spinal cord injuries. Its therapeutic effects result from actions at spinal and supraspinal sites, generally the reduction of excitatory transmission.Spasmolytics
GabapentinGabapentinA cyclohexane-gamma-aminobutyric acid derivative that is used for the treatment of partial seizures; neuralgia; and restless legs syndrome.Second-Generation Anticonvulsant Drugs
PregabalinPregabalinA gamma-aminobutyric acid (gaba) derivative that functions as a calcium channel blocker and is used as an anticonvulsant as well as an anti-anxiety agent. It is also used as an analgesic in the treatment of neuropathic pain and fibromyalgia.Second-Generation Anticonvulsant Drugs
PhenytoinPhenytoinAn anticonvulsant that is used to treat a wide variety of seizures. The mechanism of therapeutic action is not clear, although several cellular actions have been described including effects on ion channels, active transport, and general membrane stabilization. Phenytoin has been proposed for several other therapeutic uses, but its use has been limited by its many adverse effects and interactions with other drugs.First-Generation Anticonvulsant Drugs
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism injections: Consider in the elderly or if oral medications and more invasive management cannot be tolerated or as an adjunct with oral medication.[9]
OpioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics are not recommended for the treatment of TN.[3]
For acute exacerbations of intractable TN painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways → in-hospital treatment:[3,4,10,11]
IV lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics infusion or IV fosphenytoinFosphenytoinFirst-Generation Anticonvulsant Drugs
Surgical management
Surgical options for classic TN depend on patient preference, risks, adverse effects, and availability.
Surgical procedures: for individuals refractory to medical management:[3–8]
Microvascular decompression (MVD): treatment of choice if clear evidence of NVC on MRI
Rhizotomy: lesioning of the trigeminal root or ganglion with glycerol or radiofrequency thermoregulationThermoregulationBody temperature can be divided into external temperature, which involves the skin, and core temperature, which involves the CNS and viscera. While external temperature can be variable, the core temperature is maintained within a narrow range of 36.5-37.5ºC (97.7-99.5ºF).Body Temperature Regulation
Gamma knife radiosurgery: focused gamma radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma on the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions
MVD: most invasive (open craniotomyCraniotomySurgical incision into the cranium.Neurosurgery) but relieves NVC and provides the longest-lasting painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief among the procedures
Neuroablative treatments (e.g., percutaneous rhizotomy) are offered if NVC is not seen on MRI or if the patient is not fit for surgery.
Additional recommendations:[3]
For secondary TN, management of the underlying etiology is critical.
Screen and treat comorbid psychiatric conditions (e.g., depression and anxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder).
Course is variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables, and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways episodes can last weeks.
Psychological support is strongly encouraged.
Differential Diagnosis
Postherpetic neuralgiaPostherpetic neuralgiaPain in nerves, frequently involving facial skin, resulting from the activation the latent varicella-zoster virus. The two forms of the condition preceding the pain are herpes zoster oticus; and herpes zoster ophthalmicus. Following the healing of the rashes and blisters, the pain sometimes persists.Herpes Zoster (Shingles): viral reactivationReactivationHerpes Simplex Virus 1 and 2 of the varicella zoster virusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology (VZV). Age, stress, or immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.Gastroenteritis states can triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation the reactivationReactivationHerpes Simplex Virus 1 and 2 of the virusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology. Postherpetic neuralgiaPostherpetic neuralgiaPain in nerves, frequently involving facial skin, resulting from the activation the latent varicella-zoster virus. The two forms of the condition preceding the pain are herpes zoster oticus; and herpes zoster ophthalmicus. Following the healing of the rashes and blisters, the pain sometimes persists.Herpes Zoster (Shingles) presents as a painful, unilateral rashRashRocky Mountain Spotted Fever distributed in a single dermatomalDermatomalDermatologic Examination distribution (often in the thoracic regionThoracic regionSpinal Cord: Anatomy or along the trigeminal distribution). Diagnosis is clinical. Management includes antiviralAntiviralAntivirals for Hepatitis B therapy and symptomatic treatment.
MigraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine Headache: a prevalent primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorder characterized by episodic, moderate-to-severe headaches, which may be associated with nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and/or vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and increased sensitivity to light and sound. MigraineMigraineMigraine headache is a primary headache disorder and is among the most prevalent disorders in the world. Migraine is characterized by episodic, moderate to severe headaches that may be associated with increased sensitivity to light and sound, as well as nausea and/or vomiting. Migraine HeadacheheadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess is a clinical diagnosis with several variants. Management strategies include abortive therapy, including NSAIDsNSAIDSPrimary vs Secondary Headaches and triptansTriptansTriptans and ergot alkaloids are agents used mainly for the management of acute migraines. The therapeutic effect is induced by binding to serotonin receptors, which causes reduced vasoactive neuropeptide release, pain conduction, and intracranial vasoconstriction.Triptans and Ergot Alkaloids to manage acute episodes, as well as preventative strategies to minimize morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status and pain-related disabilityDisabilityDetermination of the degree of a physical, mental, or emotional handicap. The diagnosis is applied to legal qualification for benefits and income under disability insurance and to eligibility for social security and workman’s compensation benefits.ABCDE Assessment.
Cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches: a primary headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess disorder characterized by moderate-to-severe unilateral headaches occurring in conjunction with autonomic symptomsAutonomic SymptomsCluster Headaches. Cluster headachesCluster headachesCluster headache is a primary headache disorder characterized by moderate-to-severe unilateral headaches that occur in conjunction with autonomic symptoms. Cluster headache can last from weeks to months, during which the affected individual may experience attacks up to several times a day, followed by a pain-free remission period. Cluster Headaches are characterized by attacks ≤ several times per day for weeks to months, followed by a pain-free remissionRemissionA spontaneous diminution or abatement of a disease over time, without formal treatment.Cluster Headaches period. The diagnosis is clinical and often easy to establish due to the distinct features. The 1st line of treatment involves administration of oxygen by nasal cannulaNasal CannulaRespiratory Failure and/or abortive therapy with a triptan. Preventative strategies (e.g., glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids or verapamilVerapamilA calcium channel blocker that is a class IV anti-arrhythmia agent.Pulmonary Hypertension Drugs) are crucial.
Short-lasting unilateral neuralgiform headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess attacks with conjunctival injection and tearing (SUNCT):a rare form of headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess characterized by bursts of severe burning/throbbing with unilateral painUnilateral PainCluster Headaches lasting a few seconds to minutes, affecting the head and around the eye or temple. Short-lasting unilateral neuralgiform headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess attacks with conjunctival injection and tearing are also associated with autonomic nervous systemAutonomic nervous systemThe ANS is a component of the peripheral nervous system that uses both afferent (sensory) and efferent (effector) neurons, which control the functioning of the internal organs and involuntary processes via connections with the CNS. The ANS consists of the sympathetic and parasympathetic nervous systems. Autonomic Nervous System: Anatomy responses such as tearing, conjunctival injection, nasal congestion, and sweating. The attacks may be relieved with corticosteroidsCorticosteroidsChorioretinitis and antiepileptic drugs but are generally unresponsive to the usual analgesics. Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia has a refractory period after the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, but SUNCT does not. NeuroimagingNeuroimagingNon-invasive methods of visualizing the central nervous system, especially the brain, by various imaging modalities.Febrile Infant also shows neurovascular contact in many cases of TN.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia, a chronic painChronic painAching sensation that persists for more than a few months. It may or may not be associated with trauma or disease, and may persist after the initial injury has healed. Its localization, character, and timing are more vague than with acute pain.Pain Management disorder affecting the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions, causing episodes of excruciating, electric shock-like facial painFacial painPain in the facial region including orofacial pain and craniofacial pain. Associated conditions include local inflammatory and neoplastic disorders and neuralgic syndromes involving the trigeminal, facial, and glossopharyngeal nerves. Conditions which feature recurrent or persistent facial pain as the primary manifestation of disease are referred to as facial pain syndromes.Trigeminal Neuralgia.
Coding System
Code
Description
ICD-10-CM
G50.0
Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia
SNOMED CT
34506006
Trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia (disorder)
Medications:
These codes are for the anticonvulsantAnticonvulsantAnticonvulsant drugs are pharmacological agents used to achieve seizure control and/or prevent seizure episodes. Anticonvulsants encompass various drugs with different mechanisms of action including ion-channel (Na+ and Ca+2) blocking and GABA reuptake inhibition. First-Generation Anticonvulsant Drugs medications that are the first-line treatment for trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia. CarbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs is the most well-established and effective agent.
Coding System
Code
Description
RxNorm
2002
CarbamazepineCarbamazepineA dibenzazepine that acts as a sodium channel blocker. It is used as an anticonvulsant for the treatment of grand mal and psychomotor or focal seizures. It may also be used in the management of bipolar disorder, and has analgesic properties.First-Generation Anticonvulsant Drugs (ingredient)
RxNorm
31383
OxcarbazepineOxcarbazepineA carbamazepine derivative that acts as a voltage-gated sodium channel blocker. It is used for the treatment of partial seizures with or without secondary generalization. It is also an inducer of cytochrome p-450 cyp3a4.First-Generation Anticonvulsant Drugs (ingredient)
Procedures/Interventions:
This code is for microvascular decompression, a neurosurgical procedure for refractory trigeminal neuralgiaTrigeminal neuralgiaTrigeminal neuralgia (TN) is an often chronic and recurring pain syndrome involving the sensory distribution of the trigeminal nerve (cranial nerve (CN) V). The pain is typically unilateral and described as an acute, sharp, electric-shock-like pain involving the maxillary or mandibular areas and often associated with spasm of facial muscles. Trigeminal Neuralgia, which involves moving a blood vessel that is compressing the trigeminal nerveTrigeminal nerveThe 5th and largest cranial nerve. The trigeminal nerve is a mixed motor and sensory nerve. The larger sensory part forms the ophthalmic, mandibular, and maxillary nerves which carry afferents sensitive to external or internal stimuli from the skin, muscles, and joints of the face and mouth and from the teeth. Most of these fibers originate from cells of the trigeminal ganglion and project to the trigeminal nucleus of the brain stem. The smaller motor part arises from the brain stem trigeminal motor nucleus and innervates the muscles of mastication.The 12 Cranial Nerves: Overview and Functions.
Coding System
Code
Description
CPT
61458
Craniectomy, suboccipital; for exploration or decompression of cranial nervesCranial nervesThere are 12 pairs of cranial nerves (CNs), which run from the brain to various parts of the head, neck, and trunk. The CNs can be sensory or motor or both. The CNs are named and numbered in Roman numerals according to their location, from the front to the back of the brain.The 12 Cranial Nerves: Overview and Functions
Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. (2018). Cephalalgia, 38(1), 1–211. https://doi.org/10.1177/0333102417738202
Bendtsen, L., Zakrzewska, J. M., et al. (2019). European Academy of Neurology guideline on trigeminal neuralgia. European Journal of Neurology, 26(6), 831–849. https://doi.org/10.1111/ene.13950
Gronseth, G., Cruccu, G., et al. (2008). Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology, 71(15), 1183–1190. https://doi.org/10.1212/01.wnl.0000326598.83183.04
Steiner, T. J., Jensen, R., et al. (2019). Aids to management of headache disorders in primary care (2nd edition). Journal of Headache and Pain, 20(1), 57. https://doi.org/10.1186/s10194-018-0899-2
Rubis, A., Juodzbalys, G. (2020). The use of botulinum toxin A in the management of trigeminal neuralgia: a systematic literature review. Journal of Oral and Maxillofacial Research, 11(2), e2. https://doi.org/10.5037/jomr.2020.11202
Stavropoulou, E., Argyra, E., Zis, P., et al. (2014). The effect of intravenous lidocaine on trigeminal neuralgia: a randomized double blind placebo controlled trial. ISRN Pain, 2014, 853826. https://doi.org/10.1155/2014/853826
Vargas, A., Thomas, K. (2015). Intravenous fosphenytoin for acute exacerbation of trigeminal neuralgia: case report and literature review. Therapeutic Advances in Neurological Disorders, 8(4), 187–188. https://doi.org/10.1177/1756285615583202
Gambeta, E., Chichorro, J. G., Zamponi, G. W. (2020). Trigeminal neuralgia: an overview from pathophysiology to pharmacological treatments. Molecular Pain, 16, 1744806920901890. https://doi.org/10.1177/1744806920901890
Cruccu, G., Finnerup, N. B., Jensen, T. S., Scholz, J., Sindou, M., Svensson, P., Treede, R. D., Zakrzewska, J. M., Nurmikko, T. (2016). Trigeminal neuralgia: new classification and diagnostic grading for practice and research. Neurology, 87(2), 220–228. https://doi.org/10.1212/WNL.0000000000002840