Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease (HD), also known as congenital aganglionosisCongenital aganglionosisHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. M.Hirschsprung Disease or congenital megacolonCongenital megacolonHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances.Hirschsprung Disease, is a congenital anomaly of the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy caused by the failure of neural crest-derived ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders to migrate into the distal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy. The lack of innervation always involves the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and extends proximally and contiguously over variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables distances. Most cases are diagnosed in the neonatal period, with a classic triad of symptoms including delayed passage of meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate, abdominal distension, and bilious vomitingBilious VomitingCongenital Duodenal Obstruction. Individuals having less severe degrees of functional obstruction may not be diagnosed until later in infancy or childhood when they present with symptoms of chronic refractory constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, abdominal distension, and failure to thriveFailure to ThriveFailure to thrive (FTT), or faltering growth, describes suboptimal weight gain and growth in children. The majority of cases are due to inadequate caloric intake; however, genetic, infectious, and oncological etiologies are also common. Failure to Thrive. The diagnosis of HD is confirmed by the absence of ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders on rectal biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma after noninvasive testing such as anorectal manometryAnorectal ManometryPediatric Constipation and the use of contrast enema. Surgical resection of the aganglionic segment is the standard treatment.
Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease (HD), also known as congenital aganglionosisCongenital aganglionosisHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. M.Hirschsprung Disease or congenital megacolonCongenital megacolonHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances.Hirschsprung Disease, is a congenital anomaly of the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy caused by the failure of neural crest-derived ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders to migrate into the distal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy.
Familial forms: Approximately half of the cases have ≥ 1 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.ReceptorstyrosineTyrosineA non-essential amino acid. In animals it is synthesized from phenylalanine. It is also the precursor of epinephrine; thyroid hormones; and melanin.Synthesis of Nonessential Amino Acids kinase geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics (RET) mutations.
As part of a genetic syndrome:
Down syndromeDown syndromeDown syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21) (DS)/trisomy 21Trisomy 21Down syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21):
Approximately 10% of individuals with HD have DS.
< 1% of individuals with DS have HD.
Waardenburg syndromeWaardenburg syndromeRare, autosomal dominant disease with variable penetrance and several known clinical types. Characteristics may include depigmentation of the hair and skin, congenital deafness, heterochromia iridis, medial eyebrow hyperplasia, hypertrophy of the nasal root, and especially dystopia canthorum. The underlying cause may be defective development of the neural crest (neurocristopathy). Waardenburg’s syndrome may be closely related to piebaldism. Klein-waardenburg syndrome refers to a disorder that also includes upper limb abnormalities.Hirschsprung Disease:
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance inherited pigment disorder
Almost 100% of individuals with type 4Type 4Spinal Muscular AtrophyWaardenburg syndromeWaardenburg syndromeRare, autosomal dominant disease with variable penetrance and several known clinical types. Characteristics may include depigmentation of the hair and skin, congenital deafness, heterochromia iridis, medial eyebrow hyperplasia, hypertrophy of the nasal root, and especially dystopia canthorum. The underlying cause may be defective development of the neural crest (neurocristopathy). Waardenburg’s syndrome may be closely related to piebaldism. Klein-waardenburg syndrome refers to a disorder that also includes upper limb abnormalities.Hirschsprung Disease have HD.
Intellectual disabilityDisabilityDetermination of the degree of a physical, mental, or emotional handicap. The diagnosis is applied to legal qualification for benefits and income under disability insurance and to eligibility for social security and workman’s compensation benefits.ABCDE Assessment, microcephalyMicrocephalyA congenital abnormality in which the cerebrum is underdeveloped, the fontanels close prematurely, and, as a result, the head is small. (desk reference for neuroscience, 2nd ed. ).Fetal Alcohol Spectrum Disorder
41%–71% of cases have HD.
MEN type 2A (MEN2A): medullary thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cancer and pheochromocytomaPheochromocytomaPheochromocytoma is a catecholamine-secreting tumor derived from chromaffin cells. The majority of tumors originate in the adrenal medulla, but they may also arise from sympathetic ganglia (also referred to as paraganglioma). Symptoms are associated with excessive catecholamine production and commonly include hypertension, tachycardia, headache, and sweating. Pheochromocytoma with or without primary hyperparathyroidismPrimary hyperparathyroidismA condition of abnormally elevated output of parathyroid hormone due to parathyroid hyperplasia or parathyroid neoplasms. It is characterized by the combination of hypercalcemia, phosphaturia, elevated renal 1, 25-dihydroxyvitamin d3 synthesis, and increased bone resorption.Hyperparathyroidism
Specific RET mutations are associated with both Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease and MEN2A within the same family.
Epidemiology [1,2,6,7]
Annual incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency is approximately 1 in 5,000 live births in the US.
The men:women ratio is 3–4:1, but is closer to 1:1 when the entire colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy is involved.
More common in populations of Asian descent
Etiology [1,2,6]
HD is associated with mutations in multiple genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure that are important for the growth and differentiation of neural crest cellsNeural crest cellsGastrulation and Neurulation, most commonly in the RETgeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics.
Key genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure:
RET (most important susceptibility geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics)
EDNRB
EDN3
SOX10
PHOX2B
GDNF
NRTN
ECE1
ZEB2 (Mowat-Wilson)
Environmental factors and modifying genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure (some sex-linked) are likely contributors.
Pathophysiology
The pathophysiology in HD is the complete absence of ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders (aganglionosis) in the intrinsic nerve supply of the bowel due to the failure of enteric neural crestNeural crestThe two longitudinal ridges along the primitive streak appearing near the end of gastrulation during development of nervous system (neurulation). The ridges are formed by folding of neural plate. Between the ridges is a neural groove which deepens as the fold become elevated. When the folds meet at midline, the groove becomes a closed tube, the neural tube.Hirschsprung Disease–derived cells to appropriately migrate, proliferate, differentiate, and survive in the distal intestine, leading to absence of ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders in the affected segment.[1,2,6–8]
Extends proximally from the anal sphincter and involves varying lengths of the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Always involves the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Results in functional obstruction due to the arrest of peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility at the point of the arrest of the migration
Aganglionic segment also has abnormal alterations in the expression of receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors, channelsChannelsThe Cell: Cell Membrane, cytoskeletal proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis, and neurotrophic factors.
ExtensionExtensionExamination of the Upper Limbs proximal to the sigmoidSigmoidA segment of the colon between the rectum and the descending colon.VolvuluscolonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy (“long-segment disease”): 15%–20%
Total colonic aganglionosis: 5% of cases; rarely involves the ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy or entire small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy
Muscular hypertrophyMuscular hypertrophyHirschsprung Disease and dilatation of bowel proximal to obstruction, with possible progression to megacolonMegacolonMegacolon is a severe, abnormal dilatation of the colon, and is classified as acute or chronic. There are many etiologies of megacolon, including neuropathic and dysmotility conditions, severe infections, ischemia, and inflammatory bowel disease.Megacolon and rupture (usually in the cecumCecumThe blind sac or outpouching area of the large intestine that is below the entrance of the small intestine. It has a worm-like extension, the vermiform appendix.Colon, Cecum, and Appendix: Anatomy)
Microscopic pathology:
Absent enteric ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders in the submucosal (Meissner) and myenteric (Auerbach) plexuses in the distal rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables length of the proximal contiguous intestine
HypertrophyHypertrophyGeneral increase in bulk of a part or organ due to cell enlargement and accumulation of fluids and secretions, not due to tumor formation, nor to an increase in the number of cells (hyperplasia).Cellular Adaptation of aganglionic myenteric nerves (variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables)
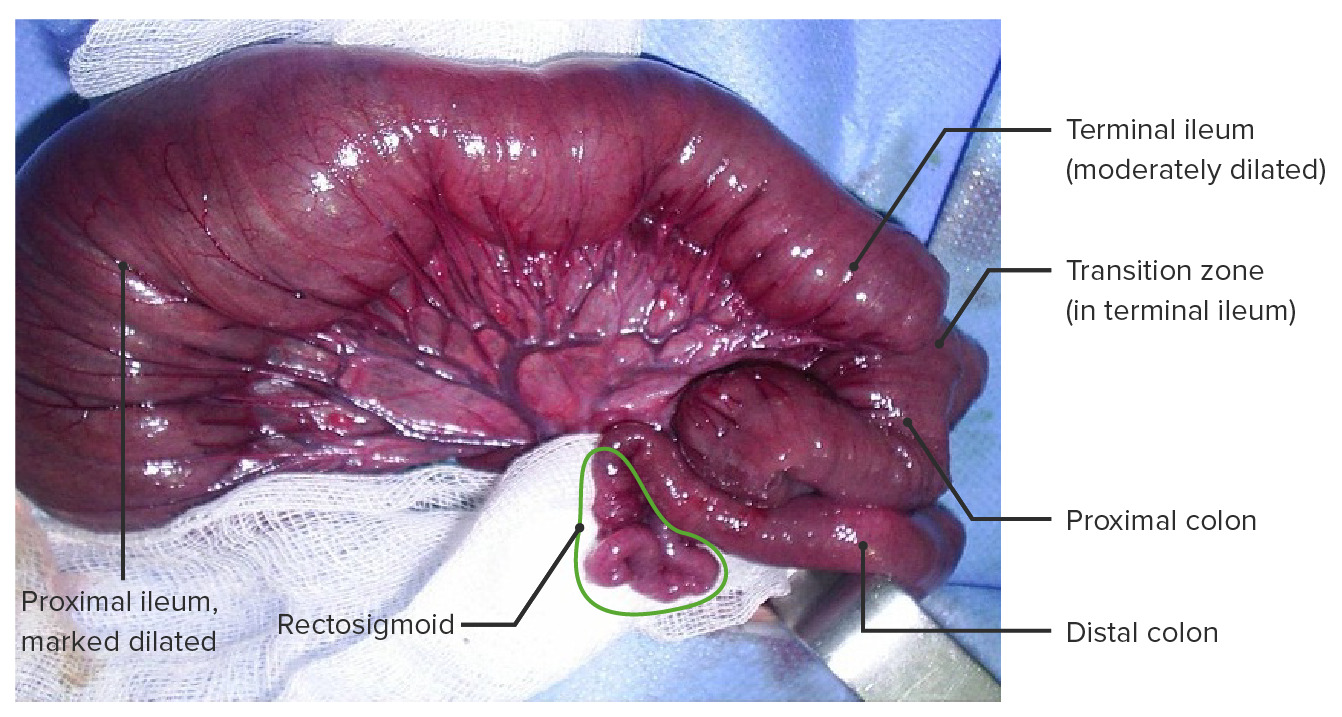
Hirschsprung disease with total colonic aganglionosis including a short segment of the terminal ileum. This type of aganglionosis occurs in < 5% of cases.
Image: “Intra-operatively, the colon and distal ileum were found contracted” by Mahmoudi A, Rami M, Khattala K, Elmadi A, Afifi MA, Youssef B. License: CC BY 2.0, edited by Lecturio.
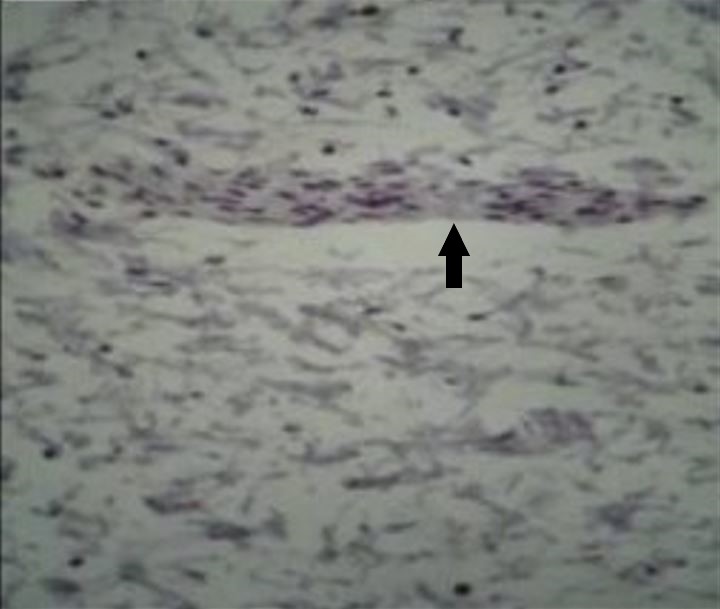
Microphotograph of Hirschsprung disease (HD)-affected segment of intestine stained with the immunohistochemical (IHC) marker calretinin, which shows no brown staining of ganglion cells within a nerve (arrow) in the myenteric plexus
Image: “Total absence of staining after calretinin immunohistochemistry in the aganglionic segment” by Hiradfar M, Sharifi N, Khajedaluee M, Zabolinejad N, Taraz Jamshidi S. License: CC BY 3.0, edited by Lecturio.
Most individuals with HD are diagnosed in the 1st month of life. Individuals with less severe disease may not present with symptoms until 3 years of age in approximately 10% of cases.[2,6,9]
Classic triad of symptoms:
Delayed passage of meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate (> 48 hours in a term infant)
Additional signs and symptoms in the neonatal period:
Explosive expulsion of gas and stool after digital rectal examinationDigital Rectal ExaminationA physical examination in which the qualified health care worker inserts a lubricated, gloved finger of one hand into the rectum and may use the other hand to press on the lower abdomen or pelvic area to palpate for abnormalities in the lower rectum, and nearby organs or tissues. The method is commonly used to check the lower rectum, the prostate gland in men, and the uterus and ovaries in women.Prostate Cancer Screening, signifying temporary relief of obstruction (“squirt sign”)
EnterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis (more common if the diagnosis is delayed):[7]
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock with feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, and abdominal distentionAbdominal distentionMegacolon, which can lead to toxic megacolonToxic megacolonAn acute form of megacolon, severe pathological dilatation of the colon. It is associated with clinical conditions such as ulcerative colitis; Crohn disease; amebic dysentery; or Clostridium enterocolitis.Megacolon
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus or other volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
Appendiceal perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Chronic refractory constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Abdominal distension
Failure to thriveFailure to ThriveFailure to thrive (FTT), or faltering growth, describes suboptimal weight gain and growth in children. The majority of cases are due to inadequate caloric intake; however, genetic, infectious, and oncological etiologies are also common. Failure to Thrive
Associated congenital anomalies:
Present in 20%–25% of individuals with HD
Congenital heart disease in 50% of syndromic cases, especially in those with DS
Genitourinary anomalies:
HydronephrosisHydronephrosisHydronephrosis is dilation of the renal collecting system as a result of the obstruction of urine outflow. Hydronephrosis can be unilateral or bilateral. Nephrolithiasis is the most common cause of hydronephrosis in young adults, while prostatic hyperplasia and neoplasm are seen in older patients. Hydronephrosis
Visual anomalies: refractory and other visual defects
Hearing impairmentHearing impairmentHearing loss, also known as hearing impairment, is any degree of impairment in the ability to apprehend sound as determined by audiometry to be below normal hearing thresholds. Clinical presentation may occur at birth or as a gradual loss of hearing with age, including a short-term or sudden loss at any point.Hearing Loss
Anorectal malformations
Diagnosis and Management
Diagnosis[7,8]
If HD is suspected based on the clinical presentations in the neonatal or postnatal periods, the following diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests are used:
Contrast enema: may show the pathognomonic sign of the “transition zoneTransition ZonePediatric Gastrointestinal Abnormalities” (funnel-shaped segment between the aganglionic rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and the proximal dilated colonDilated colonMegacolon is a severe, abnormal dilatation of the colon, and is classified as acute or chronic. There are many etiologies of megacolon, including neuropathic and dysmotility conditions, severe infections, ischemia, and inflammatory bowel disease.Megacolon)
The rectosigmoid index (the ratio of the diameter of the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy to the diameter of the sigmoidSigmoidA segment of the colon between the rectum and the descending colon.VolvuluscolonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy) is < 1 in HD (normally, > 1).
Has 70% sensitivity
May produce false-negative results after rectal washouts or digital rectal exams
False positiveFalse positiveAn FP test result indicates that a person has the disease when they do not.Epidemiological Values of Diagnostic Tests results noted in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate plugs
In case of total colonic aganglionosis (TCA):
Contrast enema may show a small-caliber colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy.
Abdominal X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests: shows decreased or no air in the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Shows air–fluid levels in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis
Pneumatosis intestinalisPneumatosis intestinalisA condition characterized by the presence of multiple gas-filled cysts in the intestinal wall, the submucosa and/or subserosa of the intestine. The majority of the cysts are found in the jejunum and the ileum.Necrotizing Enterocolitis and free air in the abdomen can be seen in enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis with perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis.
Gold standard, with > 95% sensitivity and specificitySensitivity and SpecificityBinary classification measures to assess test results. Sensitivity or recall rate is the proportion of true positives. Specificity is the probability of correctly determining the absence of a condition.Epidemiological Values of Diagnostic Tests
Rectal suction biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma can be done at bedside in neonates.
Full-thickness biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma under anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts is needed in non-neonates.
Calretinin staining has largely replaced acetylcholinesterase (AChE) staining in many centers due to better reliabilityReliabilityReliability refers to the reproducibility of a test or research finding.Causality, Validity, and Reliability.
Approach in diagnosis[12]
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation with suspicious features of HD (delayed meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate passage, squirt sign, abdominal distentionAbdominal distentionMegacolon in infants, or refractory constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship 6 months to 3 years old):
Check for signs of enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis (e.g., feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, abdominal distentionAbdominal distentionMegacolon).
Obtain abdominal X-ray.
Check for signs of obstruction and follow management for enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis if present.
If there are no signs of enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis, decreased or absent air in rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy with dilated bowel proximal to the aganglionic colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy suggests HD.
Follow diagnostic testing with contrast enema.
Look for the transition zoneTransition ZonePediatric Gastrointestinal Abnormalities (dilated colonDilated colonMegacolon is a severe, abnormal dilatation of the colon, and is classified as acute or chronic. There are many etiologies of megacolon, including neuropathic and dysmotility conditions, severe infections, ischemia, and inflammatory bowel disease.Megacolon, followed distally by a nondistended rectosigmoid) → HD
Confirm diagnosis with rectal biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
Genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies[9]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a family historyFamily HistoryAdult Health Maintenance of HD are also recommended to have genetic consultation (as RET mutations are higher in these cases).
Testing allows:
Estimation of the risk of recurrence
Determination of the possibility of MEN2A-associated RETmutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations (which has an increased risk of medullary thyroidThyroidThe thyroid gland is one of the largest endocrine glands in the human body. The thyroid gland is a highly vascular, brownish-red gland located in the visceral compartment of the anterior region of the neck.Thyroid Gland: Anatomy cancer)
Syndromic HD: Offer genetic consultation and screeningScreeningPreoperative Care for the specific geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics associated with the phenotypePhenotypeThe complete genetic complement contained in the DNA of a set of chromosomes in a human. The length of the human genome is about 3 billion base pairs.Basic Terms of Genetics.
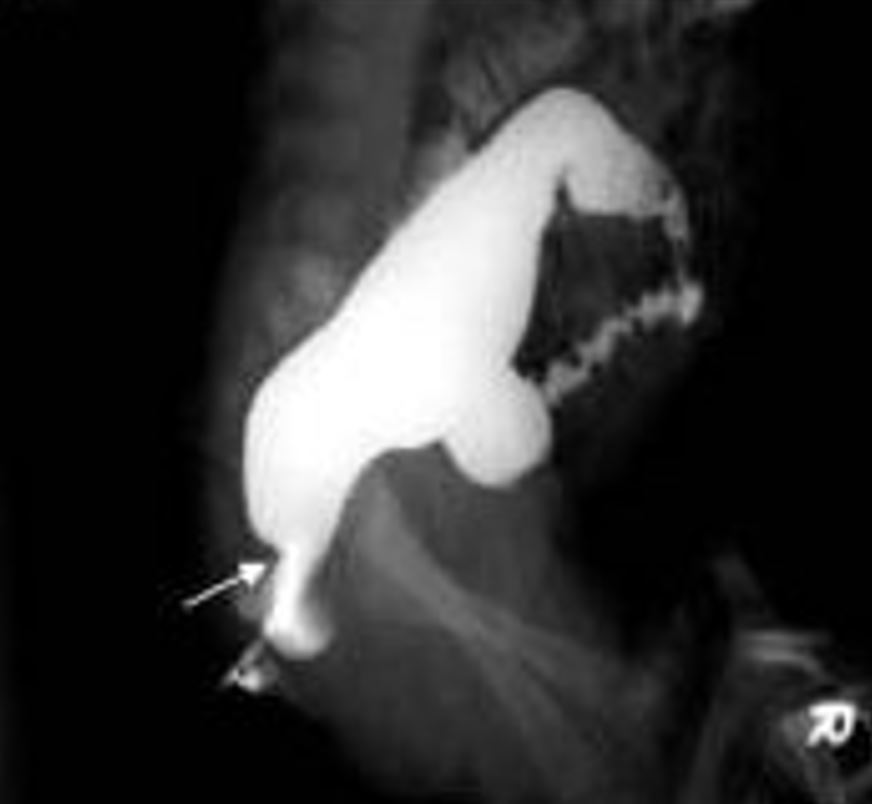
Hirschsprung disease as seen on contrast barium enema study, with the arrow showing the “transition zone” between the normal and aganglionic bowel
Image: “Contrast enema showing a CETZ at rectosigmoid, arrow” by Pratap, A., et al. License: CC BY 2.0, cropped by Lecturio.
Management[7,9–12]
Assess for associated anomalies:
Genitourinary ultrasound to assess for urinary system malformations
ScreeningScreeningPreoperative Care for hearing impairmentHearing impairmentHearing loss, also known as hearing impairment, is any degree of impairment in the ability to apprehend sound as determined by audiometry to be below normal hearing thresholds. Clinical presentation may occur at birth or as a gradual loss of hearing with age, including a short-term or sudden loss at any point.Hearing Loss
Daily rectal irrigation with warm normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids (for bowel decompression)
Goal is to prevent colonic distention and enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis.
Surgical procedures:
The goal is to resect aganglionic segment and restore bowel continuity.
The 3 types of procedures (or variations of them) that have been used are:
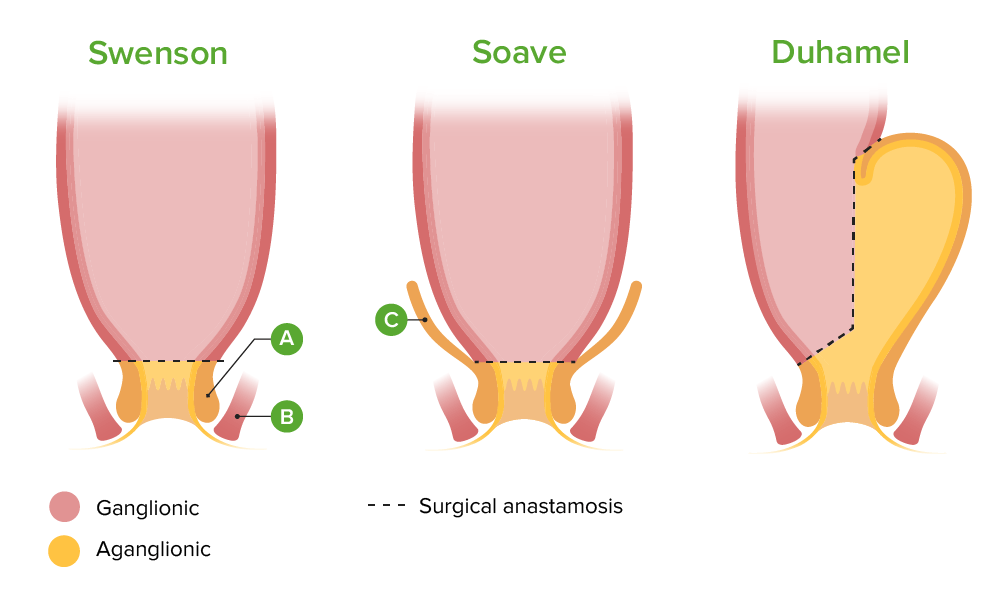
Swenson: resection of aganglionic colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy/rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy; end-to-end anastomosis of the normal (ganglionic) colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy to the short rectal cuff
Soave: submucosal stripping of aganglionic bowel; normal bowel is pulled through and anastomosed to the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy just above the dentate lineDentate lineRectum and Anal Canal: Anatomy
Duhamel: aganglionic colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy is resected; aganglionic rectal segment left in place and anastomosed side-to-side to normal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Combined laparoscopy-assisted transanal approach (an adaptation of the Soave or Swenson technique) is frequently used nowadays.
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy resection with colostomy may be needed prior to definitive procedure in cases of enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, massive dilation, malnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries, or total colonic aganglionosis.
Often not diagnosed until adulthood and mistaken for refractory constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Medical management with diet, stool softeners, laxativesLaxativesLaxatives are medications used to promote defecation. Most often, laxatives are used to treat constipation or for bowel preparation for certain procedures. There are 4 main classes of laxatives: bulk-forming, stimulant, osmotic, and emollient. Laxatives, or botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism injections
Surgical management with myomectomy may be needed
Diagrammatic outcomes of the 3 common pull-through procedures for Hirschsprung disease. A: Internal sphincter. B: External sphincter. C: Cuff of the muscularis propria retained in Soave procedure.
In the Swenson procedure, the aganglionic segment and transition zone are pulled through the anus and resected. The transected end of ganglionic bowel proximal to the aganglionic segment is sutured end to end to the terminal rectum. In the Soave procedure, the initial radial incision is made through the mucosa, and the dissection is extended proximally in the submucosal plane for several centimeters before dividing the muscularis propria. As a consequence, the muscularis propria of the distal rectum is retained as a “cuff,” through which the ganglionic bowel is drawn inferiorly and attached just above the dentate line. This avoids dissection in the pelvis, thus decreasing risk of pelvic nerve injury. In the Duhamel procedure, the ganglionic bowel is attached in a side-to-side manner to the posterior rectum. The anterior rectum remains as an aganglionic pouch.
Image by Lecturio.
Complications[3,5,6–9]
EnterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis:
Potentially lethal complication
Common in the dilated segment due to multiple factors: stasis, impaired muscosal barrier, altered immune response and bacterial overgrowthBacterial overgrowthLactose Intolerance.
Can occur preoperatively or postoperatively
Stercoral ulcers: sharply demarcated shallow ulcers with mucosal inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation due to pressure of feces on an obstructed colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Potential complications of surgery:
Bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Persistent or acquired aganglionosis → use rebiopsy to evaluate
Increased internal anal sphincterInternal anal sphincterRectum and Anal Canal: Anatomy tone → botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism may help
Behavioral stool-withholding behavior
EnterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis (HD-associated enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis):
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency rate: up to 40% postoperatively
Etiology: probably due to intestinal stasis
Signs and symptoms: abdominal painAbdominal PainAcute Abdomen, foul-smelling bloody diarrheaBloody diarrheaDiarrhea, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, intestinal necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, and perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Increased risk in long-segment disease, especially total colonic aganglionosis, in Down syndromeDown syndromeDown syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21) and in those with prior enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis
Time course: usually occurs < 1 year after surgery
Treatment: IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids, antibiotics (covering gram-negative and anaerobic organisms), repeated rectal irrigation, nasogastric decompression
More common in long-segment disease:
Perianal excoriationsExcoriationsExcoriation is a linear abrasion produced by mechanical means (scratching, rubbing, or picking) that usually involves only the epidermis but can reach the papillary dermis.Secondary Skin Lesions
Electrolyte imbalance
Anastomotic leakAnastomotic leakBreakdown of the connection and subsequent leakage of effluent (fluids, secretions, air) from a surgical anastomosis of the digestive, respiratory, genitourinary, and cardiovascular systems. Most common leakages are from the breakdown of suture lines in gastrointestinal or bowel anastomosis.Bariatric Surgery
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus
Incontinence and diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea:
Most individuals with DS/HD have long-term bowel disturbances:
Incontinence, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, soiling, enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis
May need a permanent colostomy
Urologic and sexual complications may occur (risk is lower with modern minimally invasive approaches):
Urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence
Erectile dysfunctionErectile DysfunctionErectile dysfunction (ED) is defined as the inability to achieve or maintain a penile erection, resulting in difficulty to perform penetrative sexual intercourse. Local penile factors and systemic diseases, including diabetes, cardiac disease, and neurological disorders, can cause ED. Erectile Dysfunction
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[2,6,8]
Long-term outcomes:
Overall: > 90% of affected individuals with HD report satisfactory outcomes.
Many affected individuals have disturbances of bowel function for several years.
Approximately 1% of affected individuals have debilitating incontinence requiring a permanent colostomy.
Worse outcomes are seen in:
Affected individuals with total colonic aganglionosis:
33% have persistent incontinence.
14% require a permanent ileostomyIleostomySurgical creation of an external opening into the ileum for fecal diversion or drainage. This replacement for the rectum is usually created in patients with severe inflammatory bowel diseases. Loop (continent) or tube (incontinent) procedures are most often employed.Large Bowel Obstruction.
Individuals with associated chromosomal abnormalities and syndromes
Differential Diagnosis
Causes of intestinal obstructionIntestinal obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis in the neonatal period can be distinguished from HD based on their clinical features and the presence of ganglia on a rectal biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma.
Intestinal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS): results in complete obstruction of the lumen in neonates, but is rare overall. About 50% of cases involve the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy and 20% of cases involve individuals with an associated chromosomal anomaly.
Duplication cyst: causes symptoms similar to that observed in an abdominal massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast due to compressionCompressionBlunt Chest Trauma of the adjacent bowel; rare, usually in the small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy.
Intestinal malrotationMalrotationPediatric Gastrointestinal Abnormalities with volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus: occurs due to arrest of the normal rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of the embryonic gut. Bilious vomitingBilious VomitingCongenital Duodenal Obstruction in an infant could indicate an obstructive lesion.
MeconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the NeonateileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction (MIMIMI is ischemia and death of an area of myocardial tissue due to insufficient blood flow and oxygenation, usually from thrombus formation on a ruptured atherosclerotic plaque in the epicardial arteries. Clinical presentation is most commonly with chest pain, but women and patients with diabetes may have atypical symptoms.Myocardial Infarction) due to cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans (CF): obstruction at the terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy with inspissated meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate. Approximately 80%–90% of infants with MIMIMI is ischemia and death of an area of myocardial tissue due to insufficient blood flow and oxygenation, usually from thrombus formation on a ruptured atherosclerotic plaque in the epicardial arteries. Clinical presentation is most commonly with chest pain, but women and patients with diabetes may have atypical symptoms.Myocardial Infarction have CF. Prenatal carrierCarrierVaccination testing and prenatal ultrasound help with proactive management.
Intestinal neuronal dysplasia and other chronic or acute intestinal pseudo-obstructions: functional dysmotility disorders and not mechanical obstructions. Intestinal neuronal dysplasia and other chronic or acute intestinal pseudo-obstructions usually constitute neuropathic or myopathic causes in infants.
Meconium plug syndromeMeconium Plug SyndromePediatric Gastrointestinal Abnormalities: a condition occurring in 1 among 500 newborns due to colonic dysmotility or abnormal consistencyConsistencyDermatologic Examination of the meconiumMeconiumThe thick green-to-black mucilaginous material found in the intestines of a full-term fetus. It consists of secretions of the intestinal glands; bile pigments; fatty acids; amniotic fluid; and intrauterine debris. It constitutes the first stools passed by a newborn.Prenatal and Postnatal Physiology of the Neonate. About 15% of cases have HD. A contrast enema is both diagnostic and therapeutic.
Causes of intestinal obstructionIntestinal obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis in older infants and children:
Internal anal sphincterInternal anal sphincterRectum and Anal Canal: AnatomyachalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia: Diagnosis is made by anorectal manometryAnorectal ManometryPediatric Constipation, revealing an absence of the rectosphincteric reflex on rectal balloon inflation.
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism: a condition associated with increased birth weight and macroglossiaMacroglossiaThe presence of an excessively large tongue, which may be congenital or may develop as a result of a tumor or edema due to obstruction of lymphatic vessels, or it may occur in association with hyperpituitarism or acromegaly. It also may be associated with malocclusion because of pressure of the tongue on the teeth.Wilms Tumor. Neonatal screeningScreeningPreoperative Care permits the early diagnosis of congenital hypothyroidismCongenital hypothyroidismA condition in infancy or early childhood due to an in-utero deficiency of thyroid hormones that can be caused by genetic or environmental factors, such as thyroid dysgenesis or hypothyroidism in infants of mothers treated with thiouracil during pregnancy. Endemic cretinism is the result of iodine deficiency. Clinical symptoms include severe mental retardation, impaired skeletal development, short stature, and myxedema.Hypothyroidism.
Chronic intestinal pseudo-obstructionIntestinal pseudo-obstructionA type of ileus, a functional not mechanical obstruction of the intestines. This syndrome is caused by a large number of disorders involving the smooth muscles or the nervous system.Large Bowel Obstruction: functional dysmotility disorders and not mechanical obstructions. Chronic intestinal pseudo-obstructionIntestinal pseudo-obstructionA type of ileus, a functional not mechanical obstruction of the intestines. This syndrome is caused by a large number of disorders involving the smooth muscles or the nervous system.Large Bowel Obstruction usually constitutes neuropathic or myopathic causes in infants.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease, a congenital condition affecting the large intestineLarge intestineThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy that causes problems with passing stool due to missing nerve cells in the muscles of the baby’s colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy.
Coding System
Code
Description
ICD-10-CM
Q43.1
Hirschsprung’s disease
SNOMED CT
52686006
Hirschsprung’s disease (disorder)
Evaluation & Workup:
This CPT code is for a rectal suction biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma, the definitive test for diagnosing Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease. The biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma is examined for the absence of ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders, which confirms the diagnosis.
Coding System
Code
Description
CPT
45100
BiopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma of anorectal wall, anal approach (eg, for Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease)
Procedures/Interventions:
This code represents the pull-through procedure, the primary surgical treatment for Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease, where the aganglionic segment of the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy is removed and the healthy portion is connected to the anus.
Coding System
Code
Description
CPT
44140
Colectomy, partial; with anastomosis
Complications:
This code is for enterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis, the most serious and life-threatening complication of Hirschsprung diseaseHirschsprung DiseaseHirschsprung disease (HD), also known as congenital aganglionosis or congenital megacolon, is a congenital anomaly of the colon caused by the failure of neural crest-derived ganglion cells to migrate into the distal colon. The lack of innervation always involves the rectum and extends proximally and contiguously over variable distances. MHirschsprung Disease, characterized by feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, abdominal distension, and explosive, foul-smelling diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea.
Coding System
Code
Description
ICD-10-CM
K59.39
Other specified functional disorder of intestine (used for Hirschsprung-Associated EnterocolitisEnterocolitisInflammation of the mucosa of both the small intestine and the large intestine. Etiology includes ischemia, infections, allergic, and immune responses.Yersinia spp./Yersiniosis)
References
Kumar, V., Abbas, A. K., Aster, J. C. (Eds.). (2020). Hirschsprung disease. In Robbins & Cotran Pathologic Basis of Disease (10th ed., pp. 755–756).
Zhang, Z., et al. (2017). Sporadic Hirschsprung disease: mutational spectrum and novel candidate genes revealed by next-generation sequencing. Scientific Reports, 7(1), 14796. https://doi.org/10.1038/s41598-017-14835-6
Kapur, R. P., Smith, C., Ambartsumyan, L. (2020). Postoperative pull-through obstruction in Hirschsprung disease: etiologies and diagnosis. Pediatric and Developmental Pathology. 23, 40–59. https://doi.org/10.1177/1093526619890735
Green, H. L., Rizzolo, D., Austin, M. (2016). Surgical management for Hirschsprung disease: a review for primary care providers. JAAPA 29(4), 24-29. doi: 10.1097/01.JAA.0000481397.68475.41
Kessmann J. (2006). Hirschsprung’s disease: diagnosis and management. American Family Physician, 74(8):1319–1322. PMID: 17087425.
Kyrklund, K., Sloots, C. E. J., de Blaauw, I., et al. (2020). ERNICA guidelines for the management of rectosigmoid Hirschsprung’s disease. Orphanet J Rare Dis 15, 164. https://doi.org/10.1186/s13023-020-01362-3
Bradnock, T. J., Walker, G. M. (2011). Evolution in the management of Hirschsprung’s disease in the UK and Ireland: a national survey of practice revisited. Annals of the Royal College of Surgeons of England 93(1):34–38. doi: 10.1308/003588410X12771863936846
Pattana-arun, J., Ruanroadroun, T., Tantiphalachiva, K., Sahakitrungruang, C., Attithansakul, P., Rojanasakul, A. (2010). Internal sphincter myectomy for adult Hirschsprung’s disease: a single institute experience. Journal of the Medical Association of Thailand 93(8):911–915. PMID: 20718166.