ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme (EM) is an acute hypersensitivity reaction characterized by targetoid skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesions with multiple rings and dusky centers. Lesions may be accompanied by systemic symptoms (e.g., feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever) and mucosal lesions (e.g., bullaeBullaeErythema Multiforme). The majority of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with EM have a history of recent viral (especially herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology) or bacterial infection (usually Mycoplasma pneumoniaeMycoplasma pneumoniaeShort filamentous organism of the genus mycoplasma, which binds firmly to the cells of the respiratory epithelium. It is one of the etiologic agents of non-viral primary atypical pneumonia in man.Mycoplasma). ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme is diagnosed clinically and treatment is directed toward removing the causative agent and alleviation of symptoms.
Estimated annual incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency far less than < 1%
More common in young adults (20‒40 years of age)
Men > women
Etiology[1–3,7]
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme (EM) is a cell-mediated immune reaction (type IV reaction) directed against the antigens of the offending agent, which deposit in the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions.
A significant number of cases are idiopathicIdiopathicDermatomyositis; however, there are many etiologies that may be identified:
Classification
Etiologies
Examples
Infectious causes (most common, 90% of cases)
Bacterial
MycoplasmaMycoplasmaMycoplasma is a species of pleomorphic bacteria that lack a cell wall, which makes them difficult to target with conventional antibiotics and causes them to not gram stain well. Mycoplasma bacteria commonly target the respiratory and urogenital epithelium. Mycoplasma pneumoniae (M. pneumoniae), the causative agent of atypical or “walking” pneumonia.MycoplasmapneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia(2nd most common cause)
RickettsiaRickettsiaRickettsiae are a diverse collection of obligate intracellular, gram-negative bacteria that have a tropism for vascular endothelial cells. The vectors for transmission vary by species but include ticks, fleas, mites, and lice. Rickettsia
Mycobacterium tuberculosisMycobacterium tuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes.Tuberculosis
Herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsvirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology (HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2) types 1 and 2
Most common cause
Approximately 50% of cases
Infectious mononucleosisMononucleosisInfectious mononucleosis (IM), also known as “the kissing disease,” is a highly contagious viral infection caused by the Epstein-Barr virus. Its common name is derived from its main method of transmission: the spread of infected saliva via kissing. Clinical manifestations of IM include fever, tonsillar pharyngitis, and lymphadenopathy. Mononucleosis (EBVEBVEpstein-barr virus (EBV) is a linear, double-stranded DNA virus belonging to the herpesviridae family. This highly prevalent virus is mostly transmitted through contact with oropharyngeal secretions from an infected individual. The virus can infect epithelial cells and B lymphocytes, where it can undergo lytic replication or latency.Epstein-Barr Virus, CMV)
Hepatitis CHepatitis CHepatitis C is an infection of the liver caused by the hepatitis C virus (HCV). The infection can be transmitted through infectious blood or body fluids and may be transmitted during childbirth or through IV drug use or sexual intercourse. Hepatitis C virus can cause both acute and chronic hepatitis, ranging from a mild to a serious, lifelong illness including liver cirrhosis and hepatocellular carcinoma (HCC).Hepatitis C Virus
HistoplasmosisHistoplasmosisHistoplasmosis is an infection caused by Histoplasma capsulatum, a dimorphic fungus. Transmission is through inhalation, and exposure to soils containing bird or bat droppings increases the risk of infection. Most infections are asymptomatic; however, immunocompromised individuals generally develop acute pulmonary infection, chronic infection, or even disseminated disease.Histoplasma/Histoplasmosis
DermatophytesDermatophytesTinea infections are a group of diseases caused by fungi infecting keratinized tissue (hair, nails, and skin). These infections are termed dermatomycoses and are caused by the dermatophyte fungi. There are approximately 40 dermatophyte fungi that are part of 3 genera, including Trichophyton, Epidermophyton, and Microsporum. These infections can affect any part of the body but occur most often in warm, moist regions like the groin and the feet. Dermatophytes/Tinea Infections
Noninfectious causes
Drugs
PenicillinsPenicillinsBeta-lactam antibiotics contain a beta-lactam ring as a part of their chemical structure. Drugs in this class include penicillin G and V, penicillinase-sensitive and penicillinase-resistant penicillins, cephalosporins, carbapenems, and aztreonam. Penicillins
AnticonvulsantAnticonvulsantAnticonvulsant drugs are pharmacological agents used to achieve seizure control and/or prevent seizure episodes. Anticonvulsants encompass various drugs with different mechanisms of action including ion-channel (Na+ and Ca+2) blocking and GABA reuptake inhibition. First-Generation Anticonvulsant Drugs drugs
MenstruationMenstruationThe periodic shedding of the endometrium and associated menstrual bleeding in the menstrual cycle of humans and primates. Menstruation is due to the decline in circulating progesterone, and occurs at the late luteal phase when luteolysis of the corpus luteum takes place.Menstrual Cycle
Inflammatory bowel disease
SarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis
Systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus
Polyarteritis nodosaPolyarteritis nodosaA form of necrotizing non-granulomatous inflammation occurring primarily in medium-sized arteries, often with microaneurysms. It is characterized by muscle, joint, and abdominal pain resulting from arterial infarction and scarring in affected organs. Polyarteritis nodosa with lung involvement is called churg-strauss syndrome.Vasculitides
Classification[3,5]
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme is classified based on the presence of mucosal lesions and systemic symptoms into EM minor and major.
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme usually resolves spontaneously within 1 month, with no long-term sequelae. Rarely, EM may recur around 6 times/year for up to 10 years, on average (usually associated with HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2 infection).[1,2,5,7]
Cutaneous lesions[1,2,5]
Begin as erythematous macules that develop over 3–5 days into papules → target lesions with 3 different zones
Central zone: dark and erythematous
Middle zone: pale surrounding ring
Peripheral zone: erythematous outer ring with well-defined margins
Trunk may also be involved, though is typically less affected
Centripetal spread (distal to proximal)
Rounded, < 3 cm in diameter
PruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema) or burning sensation can be present.
Atypical lesions:
Only 2 distinct zones
Raised edematous lesions
Poorly defined borders
Target lesions with a regular, round shape and 3 concentric zones: a central, darker-red area; a paler pink zone; and a peripheral red ring
Image: “Erythema multiforme” by Pediatric Unit, Maternal & Infant Department, S. Chiara University-Hospital, Via Roma 67, Pisa 56126, Italy. License: CC BY 2.0, edited by Lecturio.
Mucosal lesions[1,2,5]
Present in 25‒60% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Diffuse areas of mucosal erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion
3 locations:
Oral mucosaOral mucosaLining of the oral cavity, including mucosa on the gums; the palate; the lip; the cheek; floor of the mouth; and other structures. The mucosa is generally a nonkeratinized stratified squamous epithelium covering muscle, bone, or glands but can show varying degree of keratinization at specific locations.Stomatitis (most common)
Ocular mucosa
Genital mucosa
Systemic symptoms[1,2]
Systemic symptoms are common with mucosal involvement (EM major):
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
Acute appearance of classic target lesions, typically persisting for 7‒14 days
+/– Mucosal involvement
+/– Systemic symptoms
Signs/symptoms associated with recent infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (especially HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2 or M. pneumoniae)
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: AnatomyenzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes
May be indicated to look for potential causes:
M. pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia: serologic testing, chest X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests, throatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy swab
HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2 (especially in recurrent EM): serologic testing, swab of suspicious lesions for PCRPCRPolymerase chain reaction (PCR) is a technique that amplifies DNA fragments exponentially for analysis. The process is highly specific, allowing for the targeting of specific genomic sequences, even with minuscule sample amounts. The PCR cycles multiple times through 3 phases: denaturation of the template DNA, annealing of a specific primer to the individual DNA strands, and synthesis/elongation of new DNA molecules.Polymerase Chain Reaction (PCR)/culture
Selected tests to rule out other inflammatory, autoimmune, or malignant disorders
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Direct immunofluorescence:
Findings in EM are nonspecific.
Can help differentiate EM from autoimmune blistering diseases (e.g., bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris), which have more specific findings
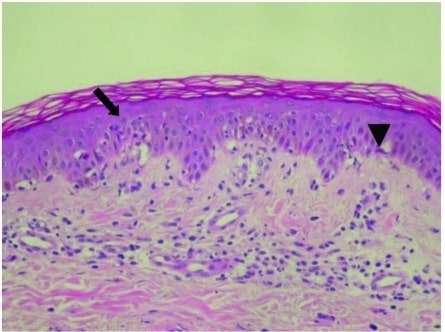
Epidermal changes in EM with vacuolated degeneration of basal cells (arrow) and scattered individual keratinocyte necrosis (arrowhead)
Image: “Epidermal Changes in Erythema Multiforme” by Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei Medical University Hospital, Taipei, Taiwan. License: CC BY 2.5
Management
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme is often self-limitingSelf-LimitingMeningitis in Children and does not require treatment. Management may vary based on local guidelines and treatment availability. The following information is based on US and UK guidelines.
General considerations[1,11]
Primary indication for hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium: severe disease leading to ↓ oral intake → likely to need IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids and electrolyte repletion
Eliminate/address etiology:
Adjust/discontinue inciting medications
Treat infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease with appropriate antimicrobials
Symptomatic therapy[1,2,9–11]
The majority of cases will require only supportive therapy. The following may be used for relief of pruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema) and discomfort due to lesions:
Oral sedating antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines (e.g., hydroxyzineHydroxyzineA histamine h1 receptor antagonist that is effective in the treatment of chronic urticaria, dermatitis, and histamine-mediated pruritus. Unlike its major metabolite cetirizine, it does cause drowsiness. It is also effective as an antiemetic, for relief of anxiety and tension, and as a sedative.Antihistamines)
Topical antiseptics/anestheticsAnestheticsAgents that are capable of inducing a total or partial loss of sensation, especially tactile sensation and pain. They may act to induce general anesthesia, in which an unconscious state is achieved, or may act locally to induce numbness or lack of sensation at a targeted site.Anesthesiology: History and Basic Concepts
Oral anesthetic rinses (e.g., lidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics)
Typical regimen: prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 40‒60 mg/day, followed by a taper over 2‒4 weeks
AcyclovirAcyclovirA guanosine analog that acts as an antimetabolite. Viruses are especially susceptible. Used especially against herpes.Herpes Zoster (Shingles):
Adults: 400 mg twice daily
Pediatric: 10 mg/kg/day in divided doses
ValacyclovirValacyclovirA prodrug of acyclovir that is used in the treatment of herpes zoster and herpes simplex virus infection of the skin and mucous membranes, including genital herpes.Herpes Zoster (Shingles) 500 mg twice daily
FamciclovirFamciclovirAn aminopurine derivative and prodrug of penciclovir which is a competitive inhibitor of herpes simplex 2 DNA polymerase. It is used to treat herpes simplex virus infection.Antivirals for Herpes Virus 250 mg twice daily
Standard treatment is for ≥ 6 months.
Treatment-resistant EM (typically at least a 6-month course):[2,4,10,11]
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants
DapsoneDapsoneA sulfone active against a wide range of bacteria but mainly employed for its actions against Mycobacterium leprae. Its mechanism of action is probably similar to that of the sulfonamides which involves inhibition of folic acid synthesis in susceptible organisms. It is also used with pyrimethamine in the treatment of malaria.Antimycobacterial Drugs
ThalidomideThalidomideA piperidinyl isoindole originally introduced as a non-barbiturate hypnotic, but withdrawn from the market due to teratogenic effects. It has been reintroduced and used for a number of immunological and inflammatory disorders. Thalidomide displays immunosuppressive and anti-angiogenic activity. It inhibits release of tumor necrosis factor-alpha from monocytes, and modulates other cytokine action.Immunosuppressants
HydroxychloroquineHydroxychloroquineA chemotherapeutic agent that acts against erythrocytic forms of malarial parasites. Hydroxychloroquine appears to concentrate in food vacuoles of affected protozoa. It inhibits plasmodial heme polymerase.Immunosuppressants
CyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants
CimetidineCimetidineA histamine congener, it competitively inhibits histamine binding to histamine h2 receptors. Cimetidine has a range of pharmacological actions. It inhibits gastric acid secretion, as well as pepsin and gastrin output.Antihistamines
UrticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives): a self-limitingSelf-LimitingMeningitis in Children disease consisting of superficial, erythematous, pruritic lesions resulting from mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema activation and histamine release in the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions. Lesions may last < 24 hours up to > 6 weeks. Commonly caused by viral infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease or by allergic reactionsAllergic ReactionsType I hypersensitivity reaction against plasma proteins in donor bloodTransfusion Reactions to drugs or food, other infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, stress, cold/heatHeatInflammation, and autoimmune disorders. Treatment, besides addressing the underlying condition, includes antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines and steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors.
Bullous pemphigoidBullous pemphigoidBullous pemphigoid and pemphigus vulgaris are two different blistering autoimmune diseases. In bullous pemphigoid, autoantibodies attack the hemidesmosomes, which connect epidermal keratinocytes to the basement membrane. This attack results in large, tense subepidermal blisters. Bullous Pemphigoid and Pemphigus Vulgaris: an immune-mediated condition characterized by the destruction of extracellular adhesive proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis (e.g., hemidesmosomes) by immunoglobulin G autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) and eczematous papules during the prodromal stage. After that, cutaneous, tense bullaeBullaeErythema Multiforme develop. This may last months to years, and treatment is focused on supportive, symptomatic care with steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors and antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines.
Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome (SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome): a life-threatening immune-mediated hypersensitivity reaction that involves the mucous membranes and skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions (< 10% of body surface area). PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship generally have a history of taking certain medications (e.g., sulfa drugs) or recent infection. Clinical presentation involves macular skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesions with 2 zones of color change, vesiclesVesiclesFemale Genitourinary Examination, bullaeBullaeErythema Multiforme, and systemic symptoms (e.g., feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever). Treatment comprises supportive skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and eye care and symptom control.
Toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome (TEN): a life-threatening immune-mediated hypersensitivity disease process that is an extensionExtensionExamination of the Upper Limbs of SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome. Toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome is an immune-mediated hypersensitivity reaction with mucocutaneous involvement (> 30% of body surface area). MortalityMortalityAll deaths reported in a given population.Measures of Health Status rate depends on severity in both SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome and TEN, at approximately 10% for SJSSJSStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome and up to 50% for TEN. Both conditions require admission to a burn unitBurn unitSpecialized hospital facilities which provide intensive care for burn patients.Staphylococcal Scalded Skin Syndrome (SSSS) for skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions care.
Billing and coding
Diagnosis Codes:
This code is used to diagnose Erythema Multiforme (EM), an acute, self-limited skin reaction characterized by distinctive “target” lesions. It is often triggered by infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, most commonly Herpes SimplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH InfectionsVirusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. Virology.
Coding System
Code
Description
ICD-10-CM
L51.9
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme, unspecified
ICD-10-CM
L51.0
Non-bullous erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion multiforme
Medications:
This code is for an antiviralAntiviralAntivirals for Hepatitis B medication like acyclovirAcyclovirA guanosine analog that acts as an antimetabolite. Viruses are especially susceptible. Used especially against herpes.Herpes Zoster (Shingles). While EM itself is treated supportively, if it is recurrent and triggered by HSVHSVHerpes simplex virus (HSV) is a double-stranded DNA virus belonging to the family Herpesviridae. Herpes simplex virus commonly causes recurrent infections involving the skin and mucosal surfaces, including the mouth, lips, eyes, and genitals.Herpes Simplex Virus 1 and 2, suppressive antiviralAntiviralAntivirals for Hepatitis B therapy can prevent future episodes.
Coding System
Code
Description
RxNorm
253
AcyclovirAcyclovirA guanosine analog that acts as an antimetabolite. Viruses are especially susceptible. Used especially against herpes.Herpes Zoster (Shingles) (ingredient)
Sokumbi, O., Wetter, D. A. (2012). Clinical features, diagnosis, and treatment of erythema multiforme: a review for the practicing dermatologist. International Journal of Dermatology, 51(8), 889–902. https://doi.org/10.1111/j.1365-4632.2011.05348.x
Zoghaib S., Kechichian E., Souaid K., et al. (2019). Triggers, clinical manifestations, and management of pediatric erythema multiforme: a systematic review. Journal of the American Academy of Dermatologists, 81(3), 813‒822. https://doi.org/10.1016/j.jaad.2019.02.057
de Risi-Pugliese, T., Sbidian, E., Ingen-Housz-Oro, S., Le Cleach, L. (2019). Interventions for erythema multiforme: a systematic review. Journal of the European Academy of Dermatology and Venereology, 33(5), 842–849. https://doi.org/10.1111/jdv.15447
Huff, J. C., Weston, W. L., Tonnesen, M. G. (1983). Erythema multiforme: a critical review of characteristics, diagnostic criteria, and causes. Journal of the American Academy of Dermatologists, https://www.jaad.org/article/S0190-9622(83)80003-6/pdf