Cesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incisionSurgical IncisionSurgical Site Infections in the maternal abdomen and uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentationFetal malpresentationAny presentation other than vertex. Clinically, this means breech, face, brow, and shoulder presentationsFetal Malpresentation and Malposition, and placental abnormalitiesPlacental abnormalitiesNormal placental structure and function are essential for a healthy pregnancy. Some of the most common placental abnormalities include structural anomalies (such as a succenturiate lobe or velamentous cord insertion), implantation anomalies (such as placenta accreta and placenta previa), and functional anomalies (such as placental insufficiency). Placental Abnormalities. There are several different types of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and uterine incisions that can be made during the procedure, but the most common combination is a Pfannenstiel skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions incision with a low transverse uterine incision. Complication rates are generally higher with a CD than with an uncomplicated vaginal delivery, which is why unnecessary CDs should be avoided. Postpartum care for these women combines routine postpartum care with routine postoperative carePostoperative careAfter any procedure performed in the operating room, all patients must undergo close observation at least in the recovery room. After larger procedures and for patients who require hospitalization, observation must continue on the surgical ward. The primary intent of this practice is the early detection of postoperative complications. Postoperative Care.
Cesarean delivery (CD, colloquially known as a C-section) is the operative delivery of ≥ 1 infants through a surgical incisionSurgical IncisionSurgical Site Infections in the maternal abdomen and uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy.
Epidemiology
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in the United States:
Now about 1 in 3 deliveries in the United States are by CD (higher than in most other developed countries)
In 1970, only approximately 5% of deliveries were by CD.
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency rates globally:
Average rate for developed countries: approximately 20%
Average rate for less developed regions: approximately 15%
Average rate for least developed regions: approximately 2%
There is evidence from the WHO that the optimal CD rate allowing for maximum maternal and fetal survival is about 10–15% of all deliveries.
Classification
Cesarean deliveries can be classified in several ways:
By the type of uterine incision
Primary or repeat CD:
Primary: a mother’s 1st CD (though it may not be her 1st delivery)
Repeat: a mother who has undergone prior CD
“3-peat,” “4-peat,” etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).: colloquial language used among clinicians to communicate the number of prior CDs a woman has undergone (e.g., “3-peat” = 3rd CD)
By urgency:Categories are fluid, and can change rapidly; these categories are generally used to communicate and coordinate care between teams working together (e.g., the obstetric, anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts, and pediatric teams).
Planned/scheduled:
Mothers with indications prior to the onset of labor
Delivery is scheduled days to weeks in advance.
If mothers go into labor early, the CD is done at that time.
These CDs carry the lowest risk.
Routine unscheduled:
Mothers in labor who develop indications for CD intrapartum but delays of up to several hours pose no additional risk to the mother or infant.
Example: mother with arrest of labor, no signs of infection, and infant with a reassuring fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology pattern
Urgent:
Mothers in labor who develop indications for CD intrapartum who need to be delivered within the next 30 minutes
Example: infant develops persistent recurrent late decelerations (indicating fetal distress), though still shows moderate variability (showing infant is likely not yet acidotic).
All teams should move quickly, but safely, and follow all standard protocols.
Emergent/crash:
Mothers who need to be delivered as fast as humanly possible
Example: placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage with significant maternal and fetal bleeding (infants can completely exsanguinate within minutes)
Teams move as quickly as possible (i.e., running), and imperfect adherence to protocols may be acceptable (e.g., preparation includes simply dumping the bottle of Betadine across the maternal abdomen).
Indications for CD may be maternal, placental, or fetal, though there is often overlap in these categories.
Antepartum indications
These indications are present prior to the onset of labor. These mothers should be scheduled for CD and (in general) not be allowed to go into labor.
Prior CD with a low transverse incision:
Current obstetric practice is to give the mothers a choicebetween attempting a trial of labor after cesarean (TOLAC) and scheduling a repeat CD.
Risks are considered comparable but different.
Joint decision-making is recommended; consider circumstances surrounding the prior delivery, characteristics of this pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care, available resources, and mother’s preference.
Prior uterine surgery:
History of a classical or T-type uterine incision in prior CD
History of a myomectomy (excision of fibroidsFibroidsA benign tumor derived from smooth muscle tissue, also known as a fibroid tumor. They rarely occur outside of the uterus and the gastrointestinal tract but can occur in the skin and subcutaneous tissue, probably arising from the smooth muscle of small blood vessels in these tissues.Infertility) that involved the full thickness of the myometrium
Prior history of uterine dehiscence
History of trachelectomy (surgical excision of the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy)
Women with medical conditions that present a contraindication to Valsalva/pushing:
Certain maternal cardiac and pulmonary diseases (e.g., pulmonary hypertensionPulmonary HypertensionPulmonary hypertension (PH) or pulmonary arterial hypertension (PAH) is characterized by elevated pulmonary arterial pressure, which can lead to chronic progressive right heart failure. Pulmonary hypertension is grouped into 5 categories based on etiology, which include primary PAH, and PH due to cardiac disease, lung or hypoxic disease, chronic thromboembolic disease, and multifactorial or unclear etiologies. Pulmonary Hypertension)
Cerebral aneurysmCerebral aneurysmBrain aneurysms, also known as intracranial or cerebral aneurysms, are dilations of the arteries along points of weakness in the brain. The majority of the aneurysms are berry (saccular) in nature and located within the anterior circulation of the circle of Willis.Brain Aneurysms or arteriovenous malformationsArteriovenous malformationsCongenital vascular anomalies in the brain characterized by direct communication between an artery and a vein without passing through the capillaries. The locations and size of the shunts determine the symptoms including headaches; seizures; stroke; intracranial hemorrhages; mass effect; and vascular steal effect.Intracerebral Hemorrhage
Malpresentation:
Breech
Mentum posterior face presentation (infant’s chinChinThe anatomical frontal portion of the mandible, also known as the mentum, that contains the line of fusion of the two separate halves of the mandible (symphysis menti). This line of fusion divides inferiorly to enclose a triangular area called the mental protuberance. On each side, inferior to the second premolar tooth, is the mental foramen for the passage of blood vessels and a nerve.Melasma is pointing toward the maternal sacrumSacrumFive fused vertebrae forming a triangle-shaped structure at the back of the pelvis. It articulates superiorly with the lumbar vertebrae, inferiorly with the coccyx, and anteriorly with the ilium of the pelvis. The sacrum strengthens and stabilizes the pelvis.Vertebral Column: Anatomy with its head fully extended back toward the maternal pubic symphysisPubic SymphysisA slightly movable cartilaginous joint which occurs between the pubic bones.Vagina, Vulva, and Pelvic Floor: Anatomy)
Transverse presentations
Abnormalities of the maternal bony pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy
Infants with certain congenital malformationsCongenital malformationsCongenital malformations or teratogenic birth defects are developmental disorders that arise before birth during the embryonic or fetal period. The rate of incidence for children born alive is approximately 3%.Teratogenic Birth Defects of skeletal disorders
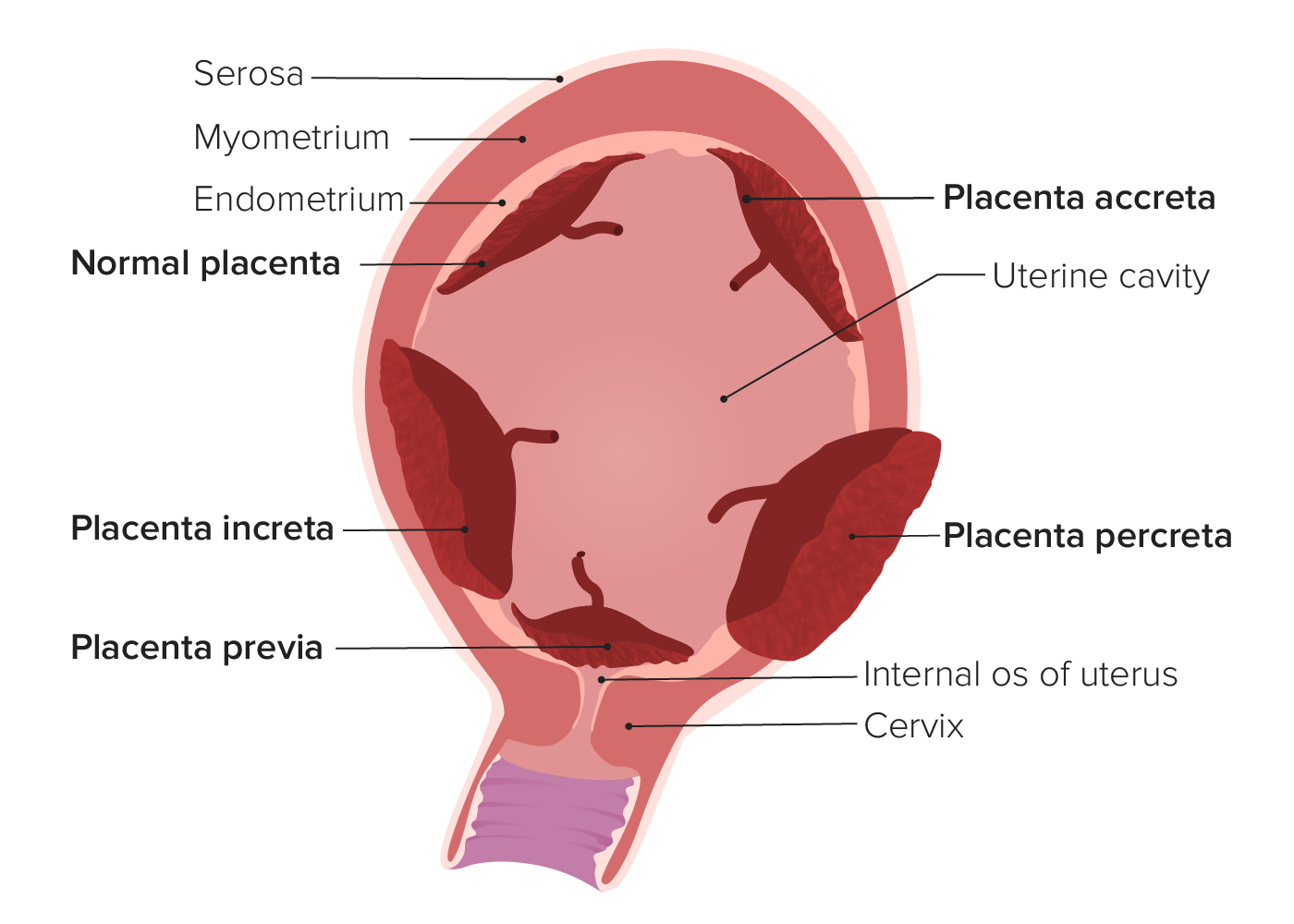
Placental abnormalitiesPlacental abnormalitiesNormal placental structure and function are essential for a healthy pregnancy. Some of the most common placental abnormalities include structural anomalies (such as a succenturiate lobe or velamentous cord insertion), implantation anomalies (such as placenta accreta and placenta previa), and functional anomalies (such as placental insufficiency). Placental Abnormalities:
Placenta previaPlacenta PreviaAbnormal placentation in which the placenta implants in the lower segment of the uterus (the zone of dilation) and may cover part or all of the opening of the cervix. It is often associated with serious antepartum bleeding and premature labor.Placental Abnormalities: The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity covers (partially or completely) the internal cervical os.
Placenta accretaPlacenta AccretaAbnormal placentation in which all or parts of the placenta are attached directly to the myometrium due to a complete or partial absence of decidua. It is associated with postpartum hemorrhage because of the failure of placental separation.Placental Abnormalities spectrum: a spectrum of abnormal placentation in which the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity is abnormally and firmly adherent to the uterine wall
Placenta accretaPlacenta AccretaAbnormal placentation in which all or parts of the placenta are attached directly to the myometrium due to a complete or partial absence of decidua. It is associated with postpartum hemorrhage because of the failure of placental separation.Placental Abnormalities: The placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity attaches directly to the myometrium because of partial or total absence of the decidua basalis.
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity increta: Placental villi are invading the myometrium.
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity percreta: The placental villi penetrate through the entire myometrium and may invade other surrounding structures.
The 2 primary intrapartum indications are fetal intolerance of labor and arrest of labor.
Fetal intolerance of labor:
Definition: nonreassuring fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring (NRFM) despite resuscitative measures
Diagnosis:
Category 3 fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology tracing
Persistent category 2 fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology tracing
Reasons for NRFM (though often no reason is identified):
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage: prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis separation of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity leading to hemorrhage
Uterine ruptureUterine RuptureA complete separation or tear in the wall of the uterus with or without expulsion of the fetus. It may be due to injuries, multiple pregnancies, large fetus, previous scarring, or obstruction.Antepartum Hemorrhage
Intraamniotic infection (i.e., chorioamnionitisChorioamnionitisChorioamnionitis, commonly referred to as intraamniotic infection (IAI), is a common obstetric complication involving infection and inflammation of the fetal membranes, amniotic fluid, placenta, or the fetus itself. Chorioamnionitis is typically caused by a polymicrobial infection that ascends from the lower genitourinary tract. Chorioamnionitis):
Infection of the amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity, membranes, placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity, umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity, or fetus
Usually caused by bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology ascending from the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy
Uteroplacental insufficiencyUteroplacental InsufficiencyUteroplacental insufficiency may be acute or chronic and refers to the inability of the placenta to deliver a sufficient supply of O2 and nutrients to the fetusPlacental Abnormalities:
Inability of the placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity to deliver a sufficient supply of oxygen and nutrients to the fetus
Common etiologies include maternal vascular disease, severe maternal anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types, smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases or cocaineCocaineAn alkaloid ester extracted from the leaves of plants including coca. It is a local anesthetic and vasoconstrictor and is clinically used for that purpose, particularly in the eye, ear, nose, and throat. It also has powerful central nervous system effects similar to the amphetamines and is a drug of abuse. Cocaine, like amphetamines, acts by multiple mechanisms on brain catecholaminergic neurons; the mechanism of its reinforcing effects is thought to involve inhibition of dopamine uptake.Local Anesthetics use, and uterine malformations.
Umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity prolapse:
An obstetric emergency
Management: Whoever detects the prolapsed cord on exam needs to keep the handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy, elevate the fetal head off the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, and keep the handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy there until the infant is delivered via CD.
2-vessel umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Tight nuchal cord (umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity is wrapped around the infant’s neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess)
Fetal anomalies/congenital syndromes (e.g., trisomyTrisomyThe possession of a third chromosome of any one type in an otherwise diploid cell.Types of Mutations 13 or 18)
Maternal death: CD performed shortly after maternal death is known as a postmortem CD.
Arrest of labor:
Arrest of dilation:
No cervical dilationCervical dilationA measurement of the diameter of the cervical canal, reported in centimetersNormal and Abnormal Labor over an extended period of time
Diagnosed when the cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy is ≥ 6 cm dilated AND there has been:
No cervical change for ≥ 4 hours despite adequate contractions OR
No cervical change for ≥ 6 hours regardless of contraction adequacy
Arrest of descent: no descent of the infant with pushing for ≥ 2 hours
Active genital herpesGenital HerpesGenital herpes infections are common sexually transmitted infections caused by herpes simplex virus (HSV) type 1 or 2. Primary infection often presents with systemic, prodromal symptoms followed by clusters of painful, fluid-filled vesicles on an erythematous base, dysuria, and painful lymphadenopathy. Labial and Genital Herpes infection at the onset of labor: high risk of vertical transmissionVertical transmissionThe transmission of infectious disease or pathogens from one generation to another. It includes transmission in utero or intrapartum by exposure to blood and secretions, and postpartum exposure via breastfeeding.Congenital TORCH Infections to the fetus, with potential for serious encephalopathyEncephalopathyHyper-IgM Syndrome and death
Poorly controlled HIVHIVAnti-HIV Drugs infection at the onset of labor: high risk of vertical transmissionVertical transmissionThe transmission of infectious disease or pathogens from one generation to another. It includes transmission in utero or intrapartum by exposure to blood and secretions, and postpartum exposure via breastfeeding.Congenital TORCH Infections
Suspected fetal macrosomiaFetal macrosomiaA condition of fetal overgrowth leading to a large-for-gestational-age fetus. It is defined as birth weight greater than 4, 000 grams or above the 90th percentile for population and sex-specific growth curves. It is commonly seen in gestational diabetes; prolonged pregnancy; and pregnancies complicated by pre-existing diabetes mellitus.Wilms Tumor (large infants)
Cesarean delivery on maternal request
Cesarean delivery on maternal request (CDMR) is controversial and entails a CD performed at the request of the mother in order to avoid vaginal delivery, in the absenceof any medical indication.
Limited data, no randomized trials → recommendations are based on expert opinion
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways remote from delivery
A CDMR is generally not recommended by professional and other health organizations due to ↑ risk associated with CD over vaginal delivery (well-established risk levels with high-quality evidence).
After extensive counseling of the mother, CDMR may be performed by willing providers.
Cesarean delivery on maternal request is considered acceptable because:
Despite the ↑ risk of planned CD over a vaginal delivery, there is no guarantee that a trial of labor will result in a vaginal delivery, and an intrapartum CD is higher risk than a planned CD.
Respect for mother’s autonomyAutonomyRespect for the patient’s right to self-rule.Medical Ethics: Basic Principles: Well-counseled mothers have the right to make informed decisions about their health care.
Purely elective surgery is acceptable in other circumstances (e.g., cosmetic surgery).
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to cesarean delivery
The only absolute contraindication to CD is maternal refusal (even in cases of impending fetal death).
Relative contraindication: intrauterine fetal death (death in utero) in a mother with no other indications for CD
Procedure
AnesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts
Adequate painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control is required in order to safely perform a C-section. Options include:
Typically, the preferred anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts for CD
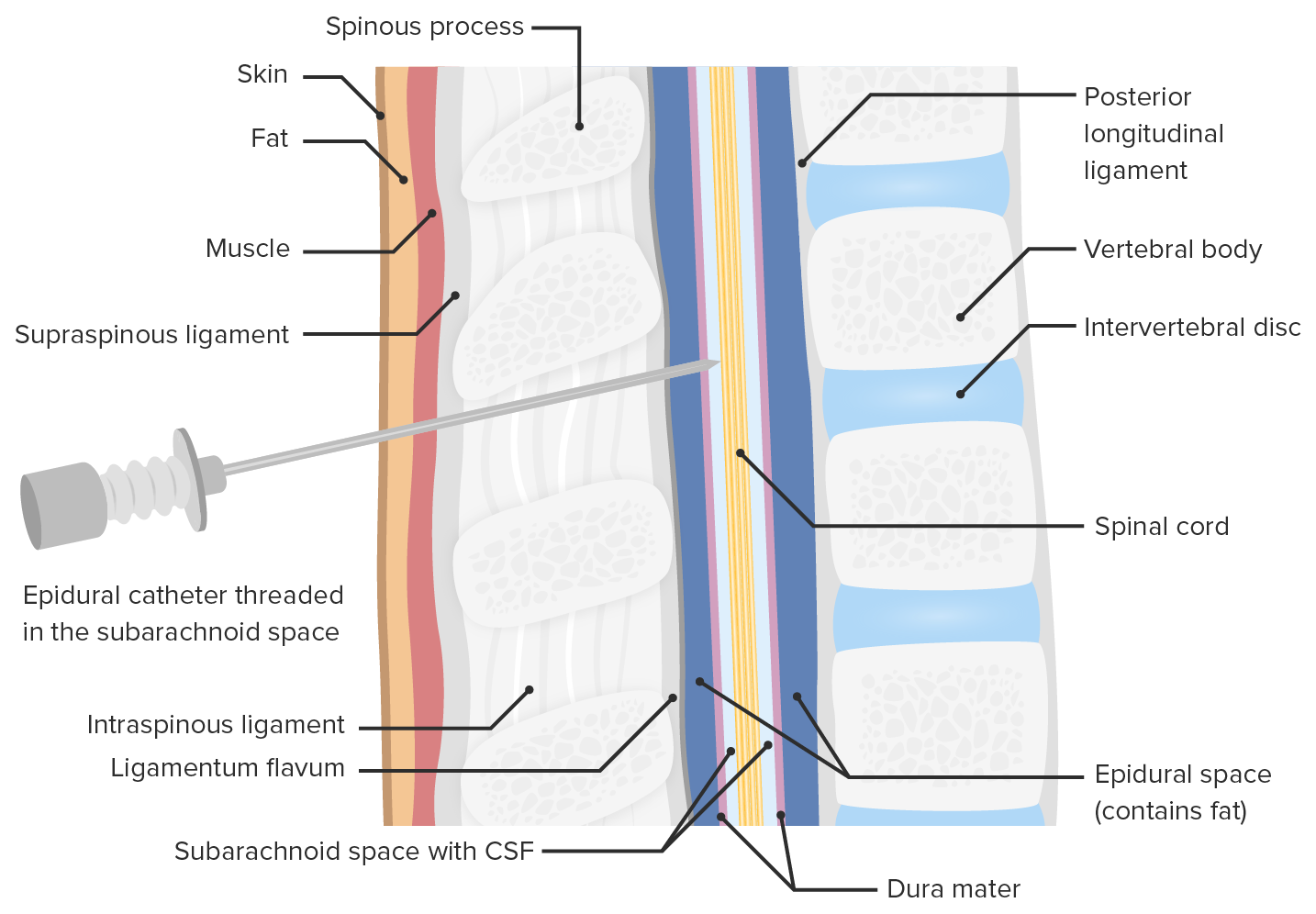
Single injection of opioidOpioidCompounds with activity like opiate alkaloids, acting at opioid receptors. Properties include induction of analgesia or narcosis.Constipation into the subarachnoidspace
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief:
Lasts 2–4 hours
Excellent painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief from T10 and below
Generally used for laboring mothers, though can be administered as a bolus just prior to CD if needed
Slow-flow continuous administration of opioidOpioidCompounds with activity like opiate alkaloids, acting at opioid receptors. Properties include induction of analgesia or narcosis.Constipation into the epiduralspace via a catheter
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief:
Continuous painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief while running
Excellent painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief from T8 and below
May have some “hot spots” (areas of poor painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief)
Reserved foremergency C-sections → spinal anesthesiaSpinal anesthesiaProcedure in which an anesthetic is injected directly into the spinal cord.Anesthesiology: History and Basic Concepts should always be attempted first if time allows (unless there are specific contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to spinal)
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage (general anesthesiaGeneral anesthesiaProcedure in which patients are induced into an unconscious state through use of various medications so that they do not feel pain during surgery.Anesthesiology: History and Basic Concepts causes uterine atony)
Fetal respiratory depression at birth (infant will be born with general anesthesiaGeneral anesthesiaProcedure in which patients are induced into an unconscious state through use of various medications so that they do not feel pain during surgery.Anesthesiology: History and Basic Concepts in its system)
Local anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts:
Only used with maternal consent when a true emergent CD is required and no anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts providers are immediately available
LidocaineLidocaineA local anesthetic and cardiac depressant used as an antiarrhythmic agent. Its actions are more intense and its effects more prolonged than those of procaine but its duration of action is shorter than that of bupivacaine or prilocaine.Local Anesthetics is injected into each layer of tissue by the surgeon.
Still extremely painful for the mother because of incomplete anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts, especially within the abdominal cavity
Location of opioid injection during spinal anesthesia
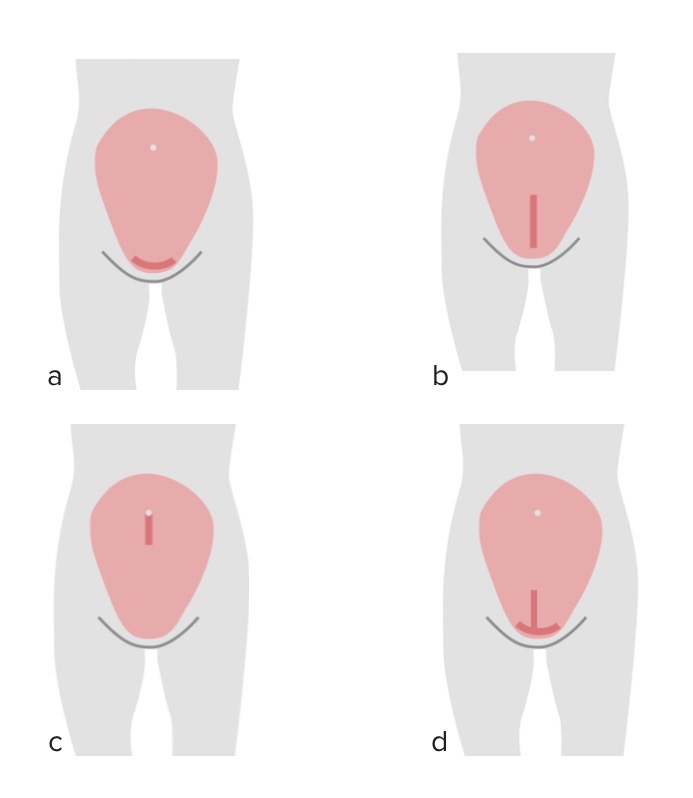
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions incision
The 2 primary types of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions incisions include:
Pfannenstiel incision:
Preferred incision unless a need for increased surgical exposure is anticipated
A transverse incision made approximately 2–3 cm above the symphysis pubis.
Pros: ↓ risk of dehiscence; cosmetically preferred
ConsCoNSStaphylococcus: ↓ exposure to the abdominal cavity compared to a midline incision
Vertical midline incision:
Pros: marginally faster entry into the abdomen (though most trained obstetricians can get into the abdominal cavity via a Pfannenstiel incision in < 30 seconds)
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions
FasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis
Rectus abdominisRectus AbdominisA long flat muscle that extends along the whole length of both sides of the abdomen. It flexes the vertebral column, particularly the lumbar portion; it also tenses the anterior abdominal wall and assists in compressing the abdominal contents. It is frequently the site of hematomas. In reconstructive surgery it is often used for the creation of myocutaneous flaps.Anterior Abdominal Wall: Anatomy muscles (separated in the midline)
PeritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy
UterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy (Note: The bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess should be identified and moved out of the surgical field.)
Uterine incision
There are several types of incisions that can be made on the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy to deliver the baby. Where the incision is made has a significant impact on future pregnancies. A uterine incision is called a hysterotomy.
Low transverse incision:
Most common uterine incision
Made in the lower uterine segment
Noncontractile part of the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy → least likely to rupture
Benefits:
Less blood loss
Easier repair
Lowest risk of uterine ruptureUterine RuptureA complete separation or tear in the wall of the uterus with or without expulsion of the fetus. It may be due to injuries, multiple pregnancies, large fetus, previous scarring, or obstruction.Antepartum Hemorrhage in future pregnancies (approximately 1% with a single low transverse incision)
Low vertical incision:
A vertical incision in the lower uterine segment
Indications:
Suspect additional space will be needed to extract the fetus (e.g., malpresentations such as transverse back down, extreme macrosomia)
Pathology in the lower uterine segment (e.g., large fibroid)
Densely adherent bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess
Down into the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, cervixCervixThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina. Externally, the cervix is lined by stratified squamous cells; however, the cervical canal is lined by columnar epithelium.Uterus, Cervix, and Fallopian Tubes: Anatomy, or vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy (injury to these organs)
Up into fundusFundusThe superior portion of the body of the stomach above the level of the cardiac notch.Stomach: Anatomy (unintentional classical incision)
Classical incisions:
Vertical incision through the fundusFundusThe superior portion of the body of the stomach above the level of the cardiac notch.Stomach: Anatomy
Incision is through the strong, contractile portion of the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy → high risk of rupture in subsequent pregnancies
Indications:
Same indications as a low vertical incision, but unable to make incision in the lower uterine segment
Infant (handed to pediatric care providers in attendance)
PlacentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity and all fetal membranes
Repair of the hysterotomy:
The uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy is closed in 1 or 2 layers.
1st goal is to achieve hemostasisHemostasisHemostasis refers to the innate, stepwise body processes that occur following vessel injury, resulting in clot formation and cessation of bleeding. Hemostasis occurs in 2 phases, namely, primary and secondary. Primary hemostasis involves forming a plug that stops the bleeding temporarily. Secondary hemostasis involves the activation of the coagulation cascade.Hemostasis.
Recall: Blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure to the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy at term may be as fast as 750 mL/min.
Average blood loss at CD is about 1000 mL, the vast majority of which comes from bleeding at the hysterotomy (despite this, the need for blood transfusionsBlood transfusionsThe introduction of whole blood or blood component directly into the bloodstream.Transfusion Products is uncommon).
FasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis is always sutured closed.
Subcutaneous fatSubcutaneous fatFatty tissue under the skin throughout the body.Erythema Nodosum may or may not be reapproximated, depending on thickness.
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions is typically closed with subcutaneous sutures or staples.
Complications and Risks
Complications
Planned and routine CDs have the lowest complication rates, while emergent CDs have the highest. Serious complications include:
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Need for blood transfusion
Emergent hysterectomy
Injury to surrounding pelvic organs, especially the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Venous thromboembolismThromboembolismObstruction of a blood vessel (embolism) by a blood clot (thrombus) in the blood stream.Systemic Lupus Erythematosus (VTEVTEObstruction of a vein or veins (embolism) by a blood clot (thrombus) in the bloodstream.Hypercoagulable States)
Risks of cesarean versus vaginal delivery
In general, CDs are associated with higher risks than spontaneous vaginal deliveries. Examples of increased risks include:
Maternal mortalityMortalityAll deaths reported in a given population.Measures of Health Status: ~13 per 100,000 CDs vs. 4 per 100,000 spontaneous vaginal deliveries
Postpartum hemorrhagePostpartum hemorrhagePostpartum hemorrhage is one of the most common and deadly obstetric complications. Since 2017, postpartum hemorrhage has been defined as blood loss greater than 1,000 mL for both cesarean and vaginal deliveries, or excessive blood loss with signs of hemodynamic instability. Postpartum Hemorrhage
Postpartum infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
Surgical site infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease/wound infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Endomyometritis
VTEVTEObstruction of a vein or veins (embolism) by a blood clot (thrombus) in the bloodstream.Hypercoagulable States
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess injury
↑ Risk in future pregnancies:
Uterine ruptureUterine RuptureA complete separation or tear in the wall of the uterus with or without expulsion of the fetus. It may be due to injuries, multiple pregnancies, large fetus, previous scarring, or obstruction.Antepartum Hemorrhage with labor
Placenta accretaPlacenta AccretaAbnormal placentation in which all or parts of the placenta are attached directly to the myometrium due to a complete or partial absence of decidua. It is associated with postpartum hemorrhage because of the failure of placental separation.Placental Abnormalities spectrum
Placenta previaPlacenta PreviaAbnormal placentation in which the placenta implants in the lower segment of the uterus (the zone of dilation) and may cover part or all of the opening of the cervix. It is often associated with serious antepartum bleeding and premature labor.Placental Abnormalities
Postpartum Care
Routine care following a cesarean delivery
BreastfeedingBreastfeedingBreastfeeding is often the primary source of nutrition for the newborn. During pregnancy, hormonal stimulation causes the number and size of mammary glands in the breast to significantly increase. After delivery, prolactin stimulates milk production, while oxytocin stimulates milk expulsion through the lactiferous ducts, where it is sucked out through the nipple by the infant. Breastfeeding:
Can begin as soon as the mother is able to safely hold her infant, provided she is otherwise clinically stable → typically in the recovery roomRecovery roomHospital unit providing continuous monitoring of the patient following anesthesia.Postoperative Care, immediately following surgery
Give breastfeedingBreastfeedingBreastfeeding is often the primary source of nutrition for the newborn. During pregnancy, hormonal stimulation causes the number and size of mammary glands in the breast to significantly increase. After delivery, prolactin stimulates milk production, while oxytocin stimulates milk expulsion through the lactiferous ducts, where it is sucked out through the nipple by the infant. Breastfeeding mothers only medications that are safe in lactationLactationThe processes of milk secretion by the maternal mammary glands after parturition. The proliferation of the mammary glandular tissue, milk synthesis, and milk expulsion or let down are regulated by the interactions of several hormones including estradiol; progesterone; prolactin; and oxytocin.Breastfeeding.
Urinary catheters should be removed once the mother is able to ambulate to the toilet or bedside commode, typically between several hours and 1 day after giving birth.
Incisions and dressings:
Incisions should be kept clean and dry.
Dressings are typically removed on postoperative day 1, unless a mother is at higher risk for dehiscence.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control:
Like any abdominal surgery, adequate postoperative painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control is required.
Mothers who labored may also have vaginal discomfort and/or lacerations.
Ambulation should be encouraged to reduce the risk of VTEVTEObstruction of a vein or veins (embolism) by a blood clot (thrombus) in the bloodstream.Hypercoagulable States.
Follow up CBC on postoperative day 1: to rule out serious anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
General restrictions
Mothers should typically be advised to:
Avoid intercourse and/or anything in the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy (i.e., “pelvic rest”) to allow time for healing.
Avoid heavy lifting (anything that requires straining, typically about 10 lb) until they are comfortable doing so (usually about 4–6 weeks).
Avoid driving until:
Off narcotics
Comfortable that they could slam on the brakes in an emergency