Tumor lysis syndrome is a potentially lethal group of metabolic disturbances that occurs when large numbers of cancer cells are killed rapidly. The lysed cells release their intracellular contents into the bloodstream, resulting in the development of hyperkalemia, hyperuricemia, hyperphosphatemia, hypocalcemia, and acute kidney injury. This can lead to severe neurologic, cardiac, gastrointestinal, and urinary signs and symptoms. The diagnosis is made based on the metabolic derangements seen on laboratory evaluation in conjunction with the clinical history. In addressing tumor lysis syndrome, the goal is to initiate therapy early for those at high risk, including IV hydration, close electrolyte monitoring and correction, and hypouricemic agents.
National incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency reports are hampered by a lack of standard criteria for diagnosis.
AMLAMLAcute myeloid leukemia (AML) is a hematologic malignancy characterized by the uncontrolled proliferation of myeloid precursor cells. Seen predominantly in older adults, AML includes an accumulation of myeloblasts and a replacement of normal marrow by malignant cells, which leads to impaired hematopoiesis. Acute Myeloid Leukemia
CLLCLLChronic lymphocytic leukemia (CLL) is a hematologic malignancy characterized by excess production of monoclonal B lymphocytes in the peripheral blood. When the involvement is primarily nodal, the condition is called small lymphocytic lymphoma (SLL). The disease usually presents in older adults, with a median age of 70 years. Chronic Lymphocytic Leukemia
CMLCMLChronic myeloid leukemia is a malignant proliferation of the granulocytic cell line characterized by a fairly normal differentiation. The underlying genetic abnormality is the Philadelphia chromosome, an abbreviated chromosome 22, resulting from reciprocal (9;22)(q34;q11) translocation. Chronic Myeloid Leukemia
OliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Acidic urine
Preexisting hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout
Pathophysiology[1–3,5,11,13]
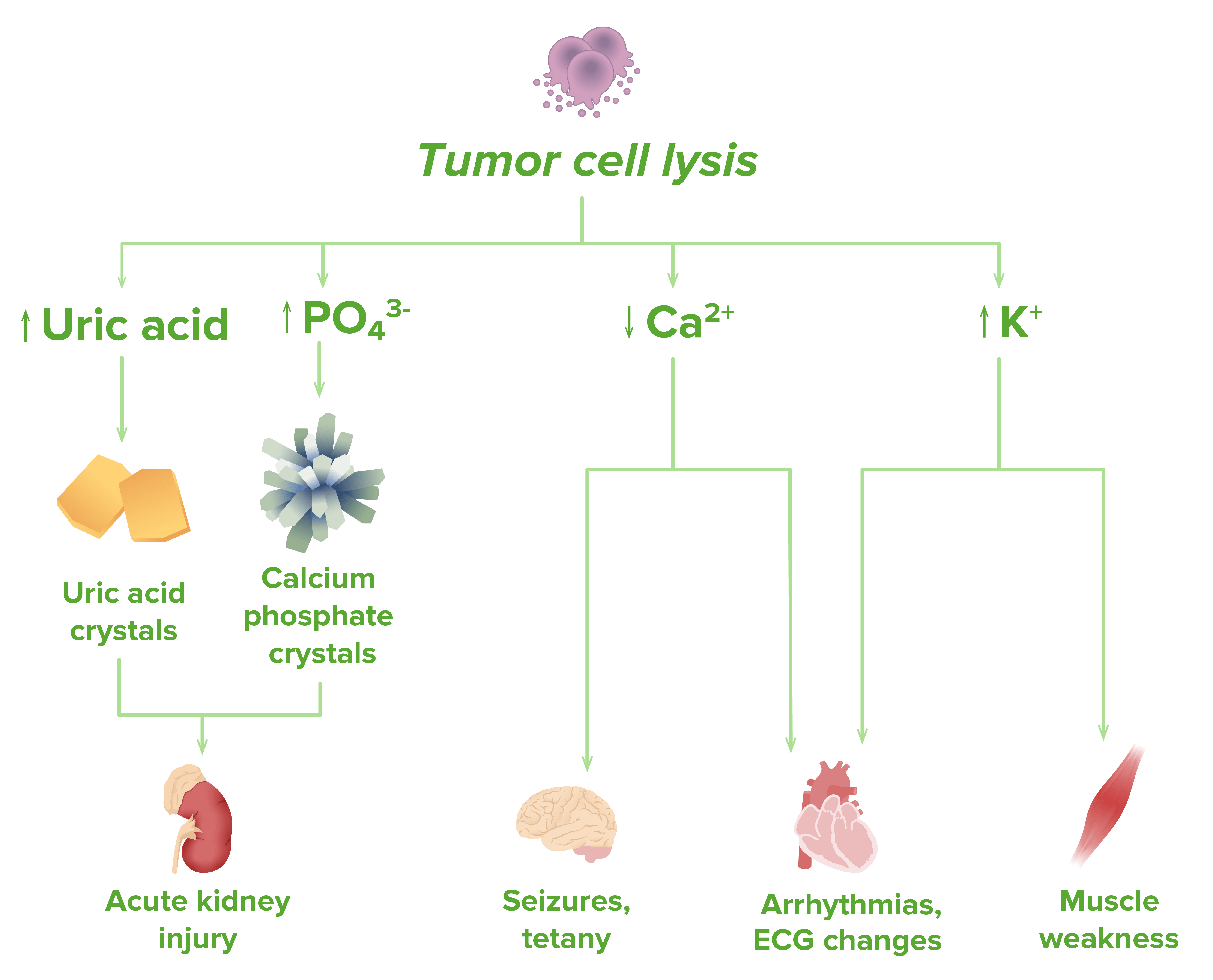
Tumor lysisTumor LysisTumor Lysis Syndrome syndrome occurs secondary to the chemotherapeutic treatment of malignancies, resulting in massive cell destruction.
K and phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes → hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia and hyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia
Nucleic acidsAcidsChemical compounds which yield hydrogen ions or protons when dissolved in water, whose hydrogen can be replaced by metals or basic radicals, or which react with bases to form salts and water (neutralization). An extension of the term includes substances dissolved in media other than water.Acid-Base Balance
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes sequestration by phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes to create calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.ElectrolytesphosphatePhosphateInorganic salts of phosphoric acid.Electrolytes → hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia
Nucleic acid breakdown → hypoxanthine and xanthine → catalyzed to uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis (via xanthine oxidaseOxidaseNeisseria) → hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout
Consequences:
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.ElectrolytesphosphatePhosphateInorganic salts of phosphoric acid.Electrolytes crystals precipitate in the kidney → acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia → impaired muscle function and cardiac conduction (causing arrhythmias)
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia → neuromuscular irritability (tetanyTetanyA disorder characterized by muscle twitches, cramps, and carpopedal spasm, and when severe, laryngospasm and seizures. This condition is associated with unstable depolarization of axonal membranes, primarily in the peripheral nervous system. Tetany usually results from hypocalcemia or reduced serum levels of magnesium that may be associated with hyperventilation; hypoparathyroidism; rickets; uremia; or other conditions.Hypocalcemia and seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures)
Pathophysiology of tumor lysis syndrome
Image by Lecturio.
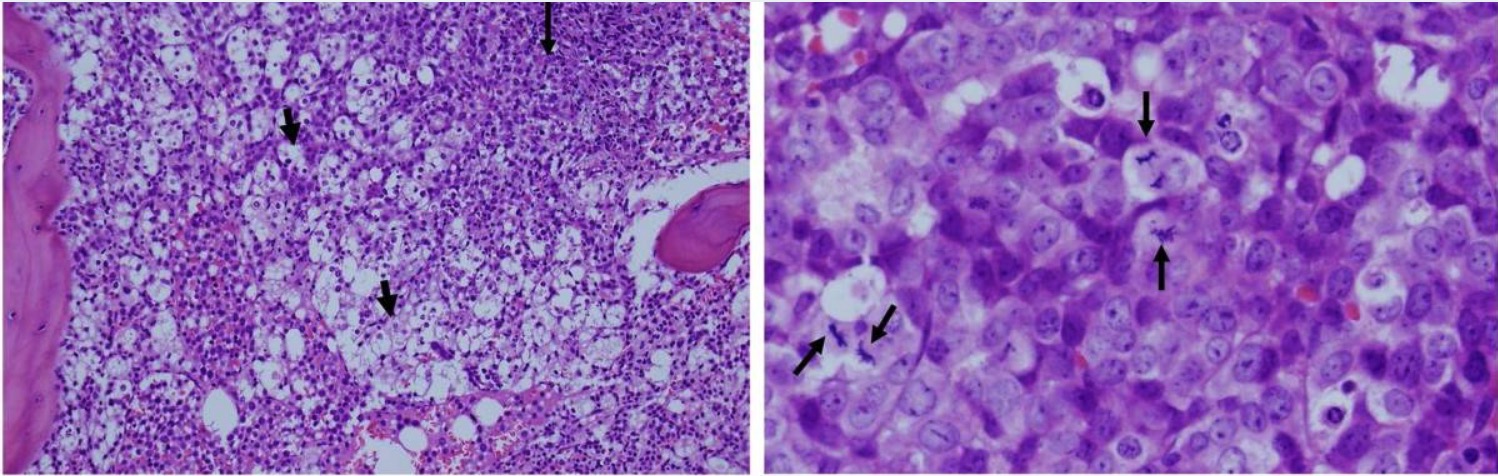
Histologic images taken from a patient with leukemia: Left: The white areas represent extreme apoptosis of leukemic cells. Cell destruction leads to a release of potassium, phosphate, and nucleic acids, which contributes to tumor lysis syndrome. Right: higher magnification of viable and proliferating leukemic cells
Image: “Hyperphosphatemia during spontaneous tumor lysis syndrome” by The Amalia Biron Research Institute of Thrombosis and Hemostasis, Sheba Medical Center and Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. License: CC BY 2.0, cropped by Lecturio.
Symptoms typically occur within 72 hours of the initiation of cytotoxicCytotoxicParvovirus B19 therapy and are the consequence of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, hyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia, hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia, and hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout.[2–5,13–15]
Muscle spasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
TetanyTetanyA disorder characterized by muscle twitches, cramps, and carpopedal spasm, and when severe, laryngospasm and seizures. This condition is associated with unstable depolarization of axonal membranes, primarily in the peripheral nervous system. Tetany usually results from hypocalcemia or reduced serum levels of magnesium that may be associated with hyperventilation; hypoparathyroidism; rickets; uremia; or other conditions.Hypocalcemia
SyncopeSyncopeSyncope is a short-term loss of consciousness and loss of postural stability followed by spontaneous return of consciousness to the previous neurologic baseline without the need for resuscitation. The condition is caused by transient interruption of cerebral blood flow that may be benign or related to a underlying life-threatening condition. Syncope
Sudden death
GI symptoms:
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
OliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation
Flank painFlank painPain emanating from below the ribs and above the ilium.Renal Cell Carcinoma (from renal or ureteral stone formation)
Diagnosis of tumor lysisTumor LysisTumor Lysis Syndrome syndrome is typically made by laboratory evaluation or a combination of clinical signs and laboratory evaluation.
Studies:[3]
For a thorough evaluation, the following should be ordered:
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis measurement
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children, including microscopy
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG)
Laboratory definition (≥ 2 of the following in a patient undergoing cancer treatment within 3 days prior to and up to 7 days after initiation of treatment):
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis:
≥ 8 mg/dL (476 μmol/L) OR
25% increase from baseline
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia:
≥ 6 mEq/L (6 mmol/L) OR
25% increase from baseline
Phosphorus:
Children: ≥ 6.5 mg/dL (2.1 mmol/L) or 25% increase from baseline
Adults: ≥ 4.5 mg/dL (1.45 mmol/L) or 25% increase from baseline
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes:
≤ 7 mg/dL (1.75 mmol/L) OR
25% decrease from baseline
Clinical definition (laboratory findings above plus ≥ 1 of the following):
Creatinine ≥ 1.5 times the upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal (ULN; age > 12 years or age-adjusted)
Cardiac arrhythmia
Sudden death
Seizure
Section: Risk and Prevention
Recommendations may vary depending on practice location. The following information is based on US and UK guidelines.
Risk stratification[2,12]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be risk-stratified based on the type of malignancyMalignancyHemothorax, white blood cell (WBC) count, and LDHLDHOsteosarcoma level (list is not exhaustive):
Low risk:
Most solid tumors
Chronic myeloid leukemiaChronic myeloid leukemiaChronic myeloid leukemia is a malignant proliferation of the granulocytic cell line characterized by a fairly normal differentiation. The underlying genetic abnormality is the Philadelphia chromosome, an abbreviated chromosome 22, resulting from reciprocal (9;22)(q34;q11) translocation. Chronic Myeloid Leukemia (in chronic phaseChronic phaseHIV Infection and AIDS)
Indolent/low proliferating non-Hodgkin lymphomaLymphomaA general term for various neoplastic diseases of the lymphoid tissue.Imaging of the Mediastinum (NHL):
Anaplastic large cell lymphomaLymphomaA general term for various neoplastic diseases of the lymphoid tissue.Imaging of the Mediastinum (adults)
Acute myeloid leukemiaAcute Myeloid LeukemiaAcute myeloid leukemia (AML) is a hematologic malignancy characterized by the uncontrolled proliferation of myeloid precursor cells. Seen predominantly in older adults, AML includes an accumulation of myeloblasts and a replacement of normal marrow by malignant cells, which leads to impaired hematopoiesis. Acute Myeloid Leukemia (AMLAMLAcute myeloid leukemia (AML) is a hematologic malignancy characterized by the uncontrolled proliferation of myeloid precursor cells. Seen predominantly in older adults, AML includes an accumulation of myeloblasts and a replacement of normal marrow by malignant cells, which leads to impaired hematopoiesis. Acute Myeloid Leukemia) with WBC < 25,000 and LDHLDHOsteosarcoma < 2 times upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal (ULN)
Acute lymphocytic leukemia (ALL) + WBC count < 100,000/μL and LDHLDHOsteosarcoma < 2 times ULN
AMLAMLAcute myeloid leukemia (AML) is a hematologic malignancy characterized by the uncontrolled proliferation of myeloid precursor cells. Seen predominantly in older adults, AML includes an accumulation of myeloblasts and a replacement of normal marrow by malignant cells, which leads to impaired hematopoiesis. Acute Myeloid Leukemia with:
Chronic lymphocytic leukemiaChronic Lymphocytic LeukemiaChronic lymphocytic leukemia (CLL) is a hematologic malignancy characterized by excess production of monoclonal B lymphocytes in the peripheral blood. When the involvement is primarily nodal, the condition is called small lymphocytic lymphoma (SLL). The disease usually presents in older adults, with a median age of 70 years. Chronic Lymphocytic Leukemia (CLLCLLChronic lymphocytic leukemia (CLL) is a hematologic malignancy characterized by excess production of monoclonal B lymphocytes in the peripheral blood. When the involvement is primarily nodal, the condition is called small lymphocytic lymphoma (SLL). The disease usually presents in older adults, with a median age of 70 years. Chronic Lymphocytic Leukemia) treated with fludarabineFludarabineAntimetabolite Chemotherapy or targeted agents
Intermediate grade NHL + LDHLDHOsteosarcoma ≥ 2 times ULN (adults)
AMLAMLAcute myeloid leukemia (AML) is a hematologic malignancy characterized by the uncontrolled proliferation of myeloid precursor cells. Seen predominantly in older adults, AML includes an accumulation of myeloblasts and a replacement of normal marrow by malignant cells, which leads to impaired hematopoiesis. Acute Myeloid Leukemia with WBC count ≥ 100,000/μL
Dietary restriction of foods high in potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia, phosphorus, and uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis
Daily assessment of fluid status → low thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction to initiate IV fluid hydration
Vital sign monitoring
Consider allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout DrugsprophylaxisProphylaxisCephalosporins
Baseline and daily laboratory monitoring:
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes
Blood ureaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea CyclenitrogenNitrogenAn element with the atomic symbol n, atomic number 7, and atomic weight [14. 00643; 14. 00728]. Nitrogen exists as a diatomic gas and makes up about 78% of the earth’s atmosphere by volume. It is a constituent of proteins and nucleic acids and found in all living cells.Urea Cycle (BUN)
Laboratory monitoring (baseline and every 6–8 hours)
IV isotonicIsotonicSolutions having the same osmotic pressure as blood serum, or another solution with which they are compared.Renal Sodium and Water Regulation saline should be initiated 2 days before cancer treatment:
Ideal rates vary, but up to 2–3 L/m2 per 24 hours may be needed.
The use of sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes to alkalinize the urine is no longer recommended.
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs:
Use in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who develop hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout.
Dose (adults and children):
0.1–0.2 mg/kg IV as a single dose
May be repeated for up to 7 days, depending on response
Laboratory studies should be obtained every 4–6 hours.
Substitute rasburicaseRasburicaseGout Drugs for allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs as initial management (unless contraindicated).
Management
Recommendations may vary depending on practice location. The following information is based on US and UK guidelines.
Management of established tumor lysisTumor LysisTumor Lysis Syndrome syndrome should follow a multidisciplinary approach, including consultation with hematology/oncology, nephrology, and critical care medicine.[11]
Monitoring[11,13,16]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be on continuous cardiac telemetryTelemetryTransmission of the readings of instruments to a remote location by means of wires, radio waves, or other means.Crush Syndrome
Laboratory studies should be performed at least every 4‒6 hours and should include:
Serum electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis
Consider daily ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG)
Fluid balance[11]
Aggressive hydration with isotonicIsotonicSolutions having the same osmotic pressure as blood serum, or another solution with which they are compared.Renal Sodium and Water Regulation fluids:
Generally, 3 L/m2/day in adults
Do not add K+ to the fluid.
Measure urinary output hourly.
Urinary output goals:
Infants: > 4 mL/kg/hr
Older patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship: 100 mL/m2/hr
If urinary output drops:
Assess renal status (laboratory studies).
Consider renal ultrasonography to rule out obstruction.
May be used if urinary output is not satisfactory despite volume expansion
Can cause tubular uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis deposition
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout management[11,13]
RasburicaseRasburicaseGout Drugs is the medication of choice (even patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship taking allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs prophylactically should switch to rasburicaseRasburicaseGout Drugs).
Dose: 0.2 mg/kg IV once daily for up to 7 days (adults and children)
If allergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction or G6PDG6PDPentose Phosphate Pathway deficiency → consider dialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia management[5,11,13–15]
Moderate and asymptomatic (≥ 6.0 mEq/L or 25% increase from baseline):
Avoid IV and oral potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia.
Check ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG).
Give sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia polystyrene sulfonate:
Children: 1 g/kg oral
Adults: 25–50 g oral
Severe (> 7.0 mEq/L) and/or symptomatic (C BIG K):
Calcium gluconate (10%):
Children:
100–200 mg/kg IV as a single dose
Maximum: 2 g
Adults: 1 g IV as a single dose
May be repeated if ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes or arrhythmias persist
Beta-2 agonist (albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs):
Children:
< 25 kg: 2.5 mg nebulized over 10 minutes; dose may be repeated as needed
25–50 kg: 5 mg nebulized over 10 minutes; dose may be repeated as needed
Adults and children over 50 kg: 10–20 mg nebulized over 10–15 minutes
Should be given with dextroseDextroseIntravenous Fluids (unless blood glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance > 250 mg/dL)
Should be given with regularRegularInsulininsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin
Kayexalate (sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia polystyrene sulfonate): same dose as above
HyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia management[11,13]
May be avoided with adequate hydration and rasburicaseRasburicaseGout Drugs administration
Aluminum hydroxide (phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes binder) may be added in severe cases:
Children: 50–150 mg/kg/day orally in divided doses every 4–6 hours
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia management[2,11,13]
Asymptomatic:
No treatment (treatment may precipitate renal calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.ElectrolytesphosphatePhosphateInorganic salts of phosphoric acid.Electrolytes deposition)
Continuous cardiac monitoring
Symptomatic (arrhythmia, seizure, or tetanyTetanyA disorder characterized by muscle twitches, cramps, and carpopedal spasm, and when severe, laryngospasm and seizures. This condition is associated with unstable depolarization of axonal membranes, primarily in the peripheral nervous system. Tetany usually results from hypocalcemia or reduced serum levels of magnesium that may be associated with hyperventilation; hypoparathyroidism; rickets; uremia; or other conditions.Hypocalcemia): give calcium gluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia
Children:[13,14]
50–100 mg/kg IV as a single dose
May repeat until symptoms improve
Adults:[15]
1 g IV as a single dose
May repeat until symptoms improve
Note: The goal is to manage symptoms from hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia, not to normalize calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes levels.[2,11]
DialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis[11,13]
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome is recommended for intractable:
Fluid overload
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia: an elevated level of potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia in the blood. Common causes include renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, hyperaldosteronismHyperaldosteronismHyperaldosteronism is defined as the increased secretion of aldosterone from the zona glomerulosa of the adrenal cortex. Hyperaldosteronism may be primary (resulting from autonomous secretion), or secondary (resulting from physiological secretion due to stimulation of the RAAS). Classically, hyperaldosteronism presents with hypertension, hypokalemia, and metabolic alkalosis.Hyperaldosteronism, and medications. Though mostly asymptomatic, hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia can be associated with palpitationsPalpitationsEbstein’s Anomaly, muscle painMuscle PainIon Channel Myopathy, weakness, and fatal cardiac arrhythmias. The diagnosis is made with a serum potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level. Emergency management of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia includes administering calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes, IV insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin, albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs, sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes, and cation exchange resins.
HyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia: an electrolyte disorder in which there is an elevated level of phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes in the blood. The disorder can occur as a result of impaired phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes excretion or by high phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes loads and is associated with impaired kidney function, hypoparathyroidismHypoparathyroidismHypoparathyroidism is defined as reduced parathyroid hormone (PTH) levels due to poor function of the parathyroid glands. The cause of hypoparathyroidism is most commonly iatrogenic following neck surgery, but it can also be associated with genetic or autoimmune disorders as well as infiltrative diseases causing destruction of the normal parathyroid tissue. Hypoparathyroidism, crush injuries, rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, fulminant hepatitisFulminant hepatitisEchovirus, and cytotoxicCytotoxicParvovirus B19 therapy. Management starts with a low-phosphate diet and phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes binders in the diet of those at risk. In extreme cases, hemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome can be used.
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout: a condition in which high uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels exist in the blood. These increased levels can result from increased production, decreased excretion, or both. HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout can lead to goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout, nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis, and chronic renal disease. There are no specific physical findings for hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout, and patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be asymptomatic. Lab studies of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout will reveal elevated serum uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels. Management consists of a low-purine diet as well as urate-lowering medications.
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis: a condition that results from direct or indirect injury to skeletal musclesSkeletal musclesA subtype of striated muscle, attached by tendons to the skeleton. Skeletal muscles are innervated and their movement can be consciously controlled. They are also called voluntary muscles.Muscle Tissue: Histology, resulting in the release of electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis, creatineCreatineAn amino acid that occurs in vertebrate tissues and in urine. In muscle tissue, creatine generally occurs as phosphocreatine. Creatine is excreted as creatinine in the urine.Acute Kidney Injury kinase, and lactate dehydrogenaseLactate DehydrogenaseOsteosarcoma. Depending on the amount of intracellular contents released, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship can have no symptoms or life-threatening renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome and cardiac arrhythmias. An elevated creatineCreatineAn amino acid that occurs in vertebrate tissues and in urine. In muscle tissue, creatine generally occurs as phosphocreatine. Creatine is excreted as creatinine in the urine.Acute Kidney Injury kinase is the most sensitive test for evaluating rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis. Management is mostly supportive, including vigorous hydration.
Diabetic ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis: a life-threatening complication of diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus characterized by hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus and ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis. Symptoms include polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation, polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus), abdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Laboratory studies will show elevated glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance and ketone levels, which are not seen in tumor lysisTumor LysisTumor Lysis Syndrome syndrome. Other abnormalities can include hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia, metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis, and acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury. Management includes fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome, insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin, and electrolyte correction.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose Tumor LysisTumor LysisTumor Lysis Syndrome Syndrome (TLS), an oncologic emergency caused by the massive and rapid release of intracellular contents from dying cancer cells, leading to severe metabolic derangements.
These codes are for the key lab tests to diagnose and monitor TLS, which include measuring uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis, potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia, phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes (all high), and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes (low).
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis; blood
CPT
84100
Phosphorus inorganic (phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes);
Medications:
These codes are for medications to prevent or treat the hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout of TLS. AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs prevents the formation of new uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis, while rasburicaseRasburicaseGout Drugs is a potent agent that breaks down existing uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis.
Coding System
Code
Description
RxNorm
546
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs (ingredient)
Jones, G. L., Will, A., Jackson, G. H., Webb, N. J. A., Rule, S., British Committee for Standards in Haematology. (2015). Guidelines for the management of tumour lysis syndrome in adults and children with haematological malignancies on behalf of the British Committee for Standards in Haematology. British Journal of Haematology, 169(5), 661–671. https://onlinelibrary.wiley.com/doi/full/10.1111/bjh.13403?sid=nlm%3Apubmed
Cairo, M. S., Coiffier, B., Reiter, A., Younes, A., on behalf of the TLS Expert Panel. (2010). Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: An expert TLS panel consensus: TLS risk classification in adults/children with malignancies. British Journal of Haematology, 149(4), 578–586. https://doi.org/10.1111/j.1365-2141.2010.08143.x
Coiffier, B., Altman, A., Pui, C. H., et al. (2008). Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. Journal of Clinical Oncology, 26(16), 2767–2778. https://doi.org/10.1200/JCO.2007.15.0177
McBride, A., et al. (2017). Managing tumor lysis syndrome in the era of novel cancer therapies. Journal of the Advanced Practitioner in Oncology, 8(7), 705–720. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6188097/
Create your free account or log in to continue reading!