Renal Na+ and water regulation work in tandem to control how fluid is distributed throughout the compartments of the body. SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia is the body’s dominant extracellular solute, and is responsible for the osmotic force that keeps differing amounts of water in each compartment. Changes in Na+ balance are sensed by the body through changes in blood volume. Changes in water balance are sensed by the body through changes in plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration. Both ultimately send feedback signals to the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy to ensure that homeostasisHomeostasisThe processes whereby the internal environment of an organism tends to remain balanced and stable.Cell Injury and Death is maintained. Abnormalities in these processes can result in problems in volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols (e.g., hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema, pitting edemaPitting edemaEdema caused by excess fluid without excess colloid. Leaves “pits” due to fluid displacement when pressure is applied to the areaEdema) and dysnatremias (hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia and hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia).
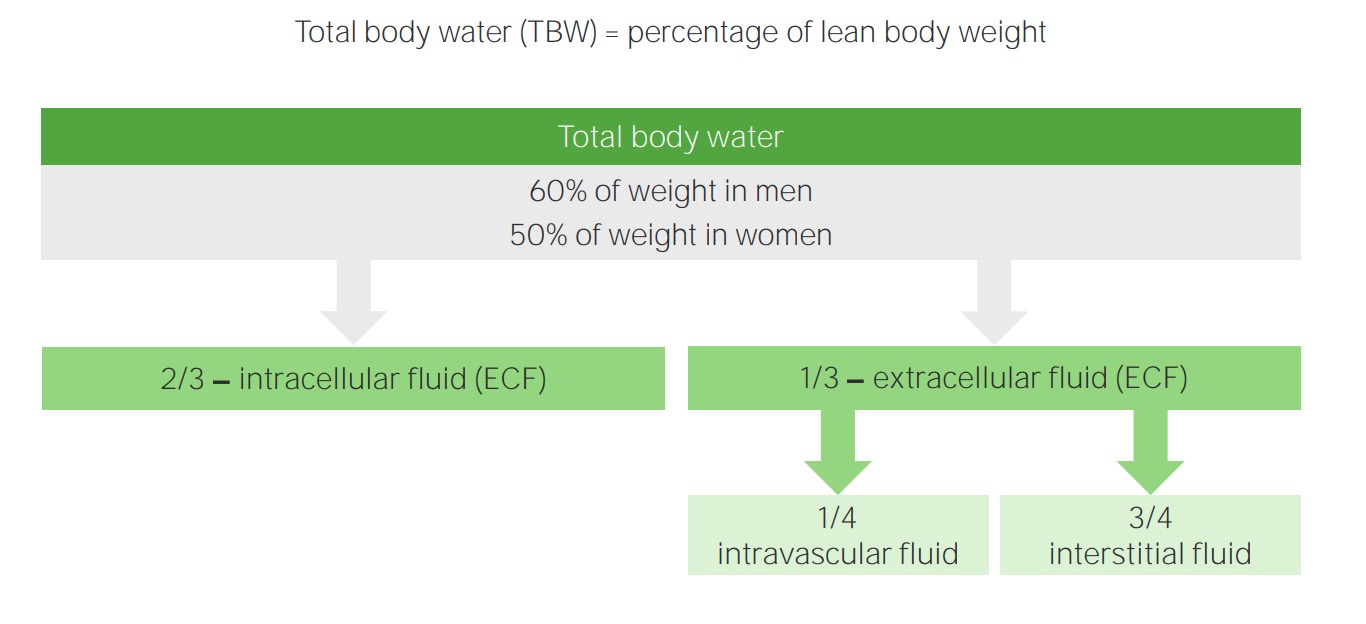
To understand renal sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia and water regulation, it is important to understand how water is normally distributed in the body.
All fluid enclosed within cells by their plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products membranes
The fluid component of blood (also known as plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products)
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance and BUN contribute, but to a much smaller degree when in the normal range.
All other solutes contribute only a negligible amount → not included in formula
Equation:Plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration = (2 x sNa+) + (glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance/18) + (BUN/2.8)
Normal range: 275–295 mOsm/kg H2O
Regulation:
Osmoreceptors in the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus sense osmolality.
Important for water regulation
Tonicity
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products tonicity refers to the concentration of only the osmotically activeOsmotically ActiveOsmotic Diuretics solutes in blood and is often referred to as effective osmolality.
Equal concentrations on each side of membrane → no osmotic force
These solutes are called “ineffective osmoles.”
Equation: effective plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration = (2 x sNa+) + (glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance/18)
Na+ and glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance are effective osmoles:
PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products tonicity is mostly determined by sNa+.
Normal glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance concentrations do not contribute much to tonicity.
UreaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea Cycle (e.g., BUN) is an ineffective osmole → not considered for the tonicity equation
Other effective osmoles contribute only a negligible amount → not included in the formula
Regulation:
Osmoreceptors in the kidney sense tonicity.
Important for Na+regulation
Tonicity determines how water shifts between the body’s fluid compartments.
Compared to normal plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products, a fluid may be:
Renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome → elevated BUN → ↑ plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration but normal tonicity
EthanolEthanolA clear, colorless liquid rapidly absorbed from the gastrointestinal tract and distributed throughout the body. It has bactericidal activity and is used often as a topical disinfectant. It is widely used as a solvent and preservative in pharmaceutical preparations as well as serving as the primary ingredient in alcoholic beverages.Ethanol Metabolism intoxication (ineffective osmole) → ↑ plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration but normal tonicity
Hypervolemia: volume overloaded → ↑ total body Na+
Assessed on physical exam, and not sNa+ levels
Disorders of water balance are characterized by abnormalities in the concentration of sNa+:
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: too much water
HypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia: too little water
Both disorders can exist at any level of total body Na+.
A nephronNephronThe functional units of the kidney, consisting of the glomerulus and the attached tubule.Kidneys: Anatomy is the functional unit of the kidney through which fluid and solutes, including Na+, are filtered, reabsorbed, and secreted.
Glomerulus and proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System
Glomerulus: Water and Na+ are freely filtered.
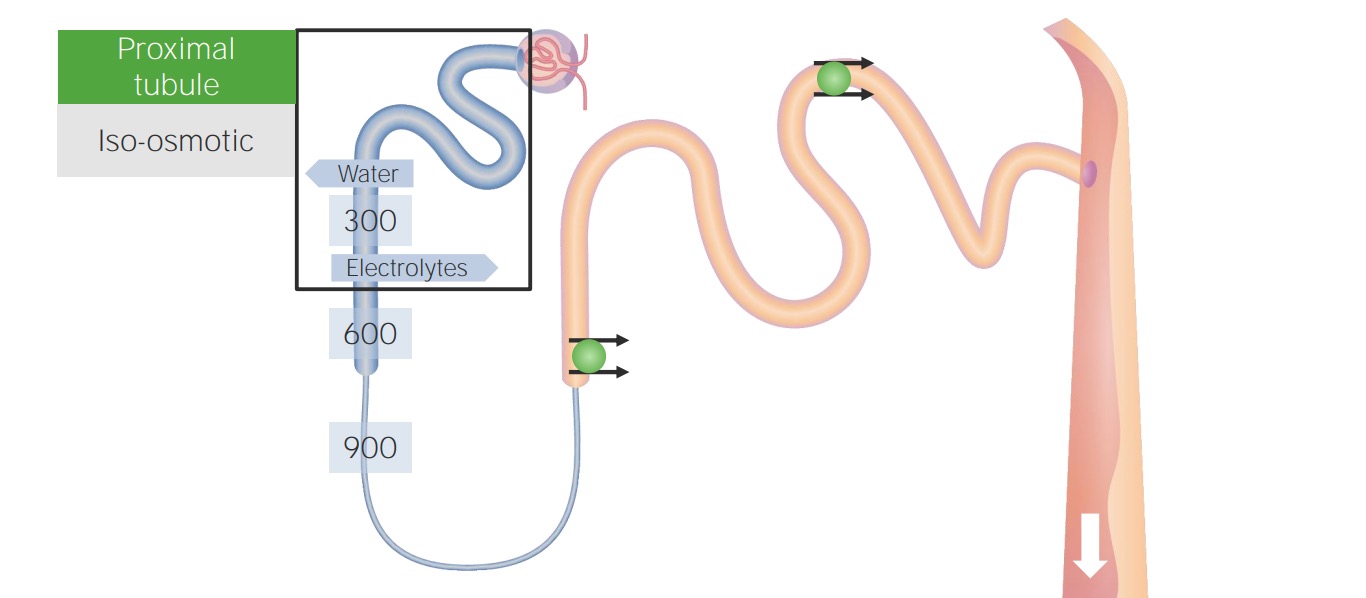
Proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System:
Approximately ⅔ of filtered water and Na+ are reabsorbed.
Tubular fluid is isotonic to plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products.
Reabsorption in the proximal tubule: The numbers overlying the tubules represent the osmolality of the surrounding tissue.
Image by Lecturio.
Thick ascending limb of the loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System (TAL)
Water does not follow solutes (Na+, K+, Cl–) into the medulla.
Generates an osmotic gradient between the tubular fluid and renal medulla
Tubular fluid is hypotonic to plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products.
Known as a “diluting segment” (urine is diluted)
Reabsorption in the thick ascending limb: Sodium, potassium, and chloride are reabsorbed through the NKCC2 cotransporter, but the thick ascending limb is not permeable to water. The thick ascending limb is a diluting segment of the nephron.
Image by Lecturio.
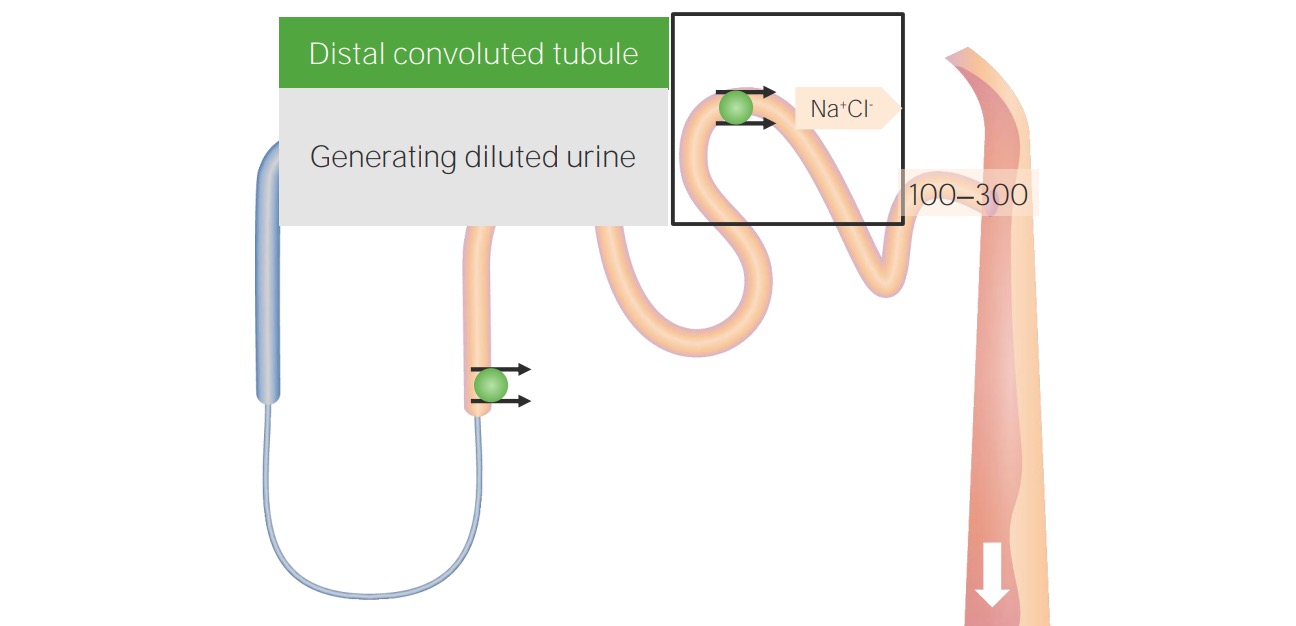
Distal convoluted tubuleDistal convoluted tubuleThe portion of renal tubule that begins from the enlarged segment of the ascending limb of the loop of henle. It reenters the kidney cortex and forms the convoluted segments of the distal tubule.Gitelman Syndrome (DCT)
Location of thiazide-sensitive NaCl cotransporterNaCl cotransporterA subclass of symporters found in kidney tubules, distal that are the major pathway for salt resorption. Inhibition of these symporters by benzothiadiazine is the basis of action of some diuretics.Tubular System
Na+ and Cl– are reabsorbed.
DCT is not permeable to water.
Water does not follow solutes (Na+, Cl–) into the medulla.
Generates an even stronger osmotic gradient between the tubular fluid and renal medulla
Tubular fluid is even more hypotonic to plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products at this point.
Another “diluting segment”
Reabsorption in the distal convoluted tubule (DCT): Sodium and chloride are reabsorbed in the DCT, but the DCT is not permeable to water. The DCT is another diluting segment.
Image by Lecturio.
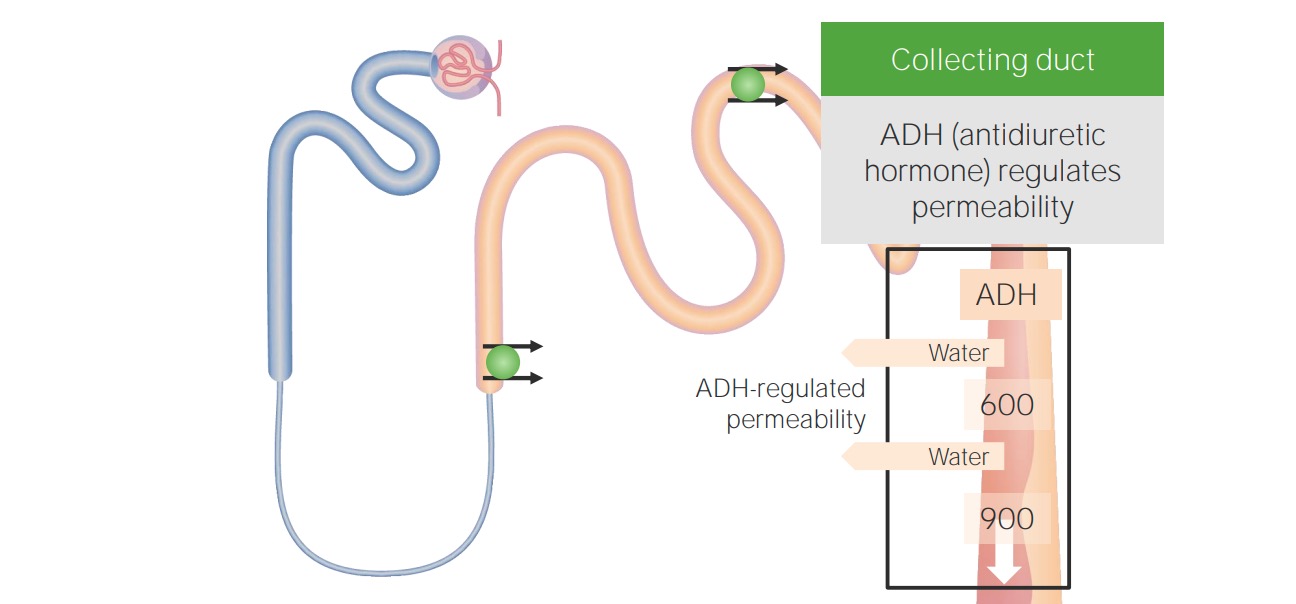
Collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma
Allow water to move from the tubular fluid into renal medulla by diffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis
Renal medulla is hypertonic due to solute reabsorption in the diluting segments (TAL and DCT).
Antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (ADH) stimulates the production and insertion of aquaporinsAquaporinsA class of porins that allow the passage of water and other small molecules across cell membranes.Tubular System
↑ ADH levels → ↑ aquaporinsAquaporinsA class of porins that allow the passage of water and other small molecules across cell membranes.Tubular System → ↑ water reabsorption → concentrated urine
↓ ADH levels → ↓ aquaporinsAquaporinsA class of porins that allow the passage of water and other small molecules across cell membranes.Tubular System → ↓ water reabsorption → dilute urine
The body regulates Na+ balance by sensing changes in the effective circulating volume (ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition), which is also known as the effective arterial blood volume (EABV).
The ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition is the portion of the intravascular volume that is found on the arterial side only.
Changes in Na+ balance result in changes in the ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition.
Changes in the ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition are relayed to the kidney primarily through:
The RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones
Natriuretic peptidesNatriuretic peptidesPeptides that regulate the water-electrolyte balance in the body, also known as natriuretic peptide hormones. Several have been sequenced (atrial natriuretic factor; brain natriuretic peptide; c-type natriuretic peptide).Arterial Pressure Regulation
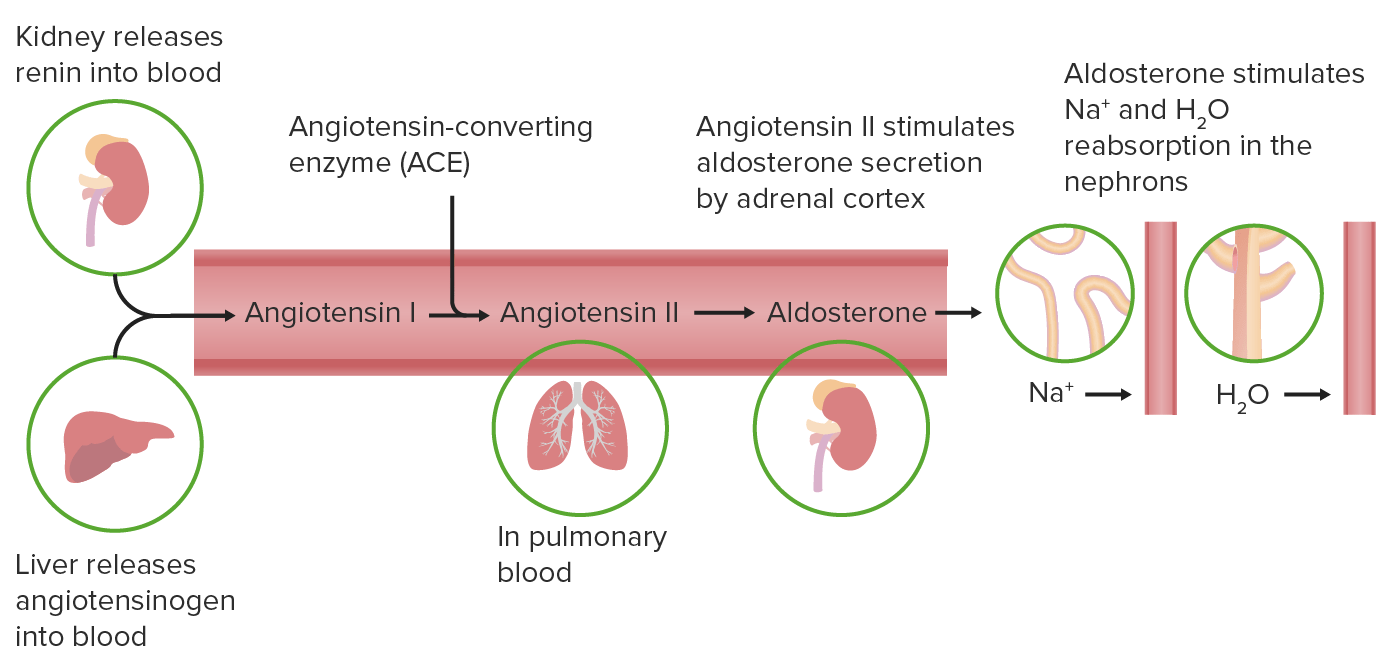
Renin-angiotensin-aldosterone systemRenin-angiotensin-aldosterone systemA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones
The RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones is stimulated by a low ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition:
Juxtaglomerular apparatus and carotid sinusCarotid sinusThe dilated portion of the common carotid artery at its bifurcation into external and internal carotids. It contains baroreceptors which, when stimulated, cause slowing of the heart, vasodilatation, and a fall in blood pressure.Carotid Arterial System: Anatomy/aortic archAortic archMediastinum and Great Vessels: AnatomybaroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus)triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation renin release from kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy when ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition is ↓
Renin (kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy) → converts angiotensinogen (liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy) to angiotensin I
ACE (lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy) → converts angiotensin I to angiotensin II
Stimulates aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia release (from the adrenal cortexAdrenal CortexThe outer layer of the adrenal gland. It is derived from mesoderm and comprised of three zones (outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis) with each producing various steroids preferentially, such as aldosterone; hydrocortisone; dehydroepiandrosterone; and androstenedione. Adrenal cortex function is regulated by pituitary adrenocorticotropin.Adrenal Glands: Anatomy)
The renin-angiotensin-aldosterone system
Image by Lecturio.
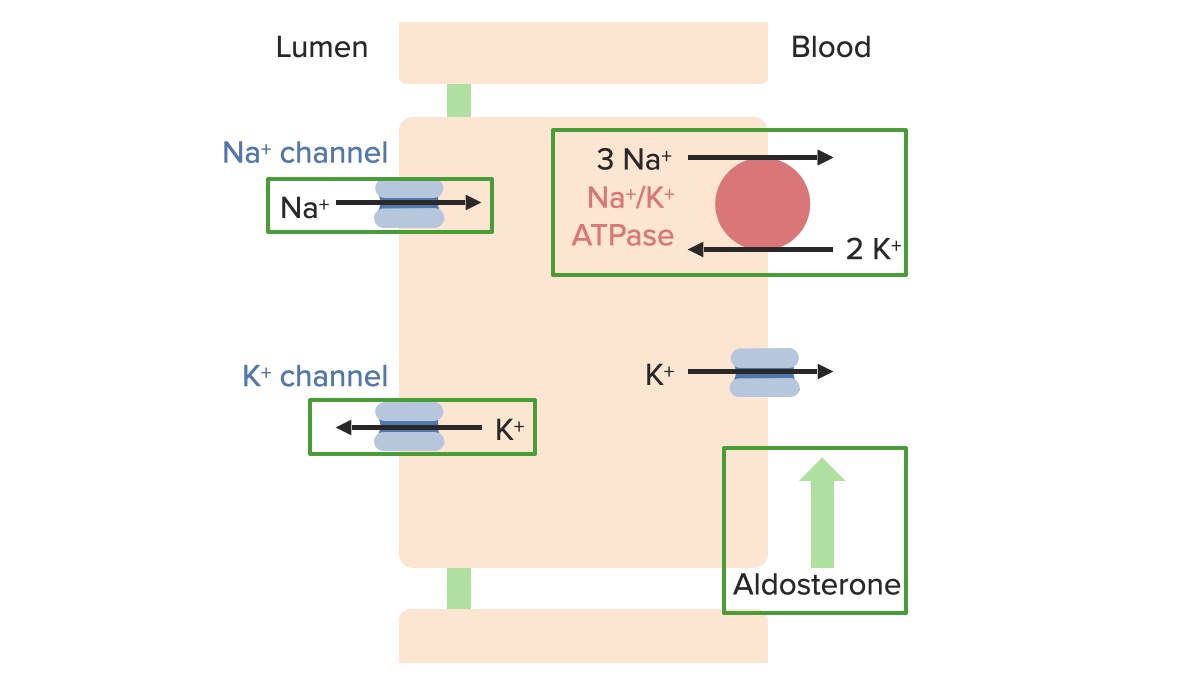
Effects of aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:
Stimulates production of the following proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis within the principal cellsPrincipal cellsTubular System in the collecting ducts:
Na+/K+-ATPase on the basolateral side
Epithelial sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiachannelsChannelsThe Cell: Cell Membrane (ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome) on the lumen side: allow Na+ reabsorption from the lumen into the principal cellsPrincipal cellsTubular System
Renal outer medullary potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia (ROMK) channelsChannelsThe Cell: Cell Membraneon the lumen side: allow excretion of K+ into the urine
Stimulates Na+ reabsorption from the renal tubules
End result of ↑ aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:
↑ Serum Na+ (↓ urinary excretion of Na+)
↑ BP (↑ water reabsorption from the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy)
↓ Serum K+ (↑ urinary excretion of K+)
↑ Serum pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance (↑ urinary excretion of H+)
Effects of aldosterone on sodium and potassium regulatory transport proteins in the principal cells of the collecting ducts
Image by Lecturio.
Natriuretic peptidesNatriuretic peptidesPeptides that regulate the water-electrolyte balance in the body, also known as natriuretic peptide hormones. Several have been sequenced (atrial natriuretic factor; brain natriuretic peptide; c-type natriuretic peptide).Arterial Pressure Regulation
Natriuretic peptidesNatriuretic peptidesPeptides that regulate the water-electrolyte balance in the body, also known as natriuretic peptide hormones. Several have been sequenced (atrial natriuretic factor; brain natriuretic peptide; c-type natriuretic peptide).Arterial Pressure Regulation include:
Atrial natriuretic peptide (ANP)
BNP
Regulation:
Cardiac baroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus) sense an ↑ in ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition
TriggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation the release of natriuretic peptidesNatriuretic peptidesPeptides that regulate the water-electrolyte balance in the body, also known as natriuretic peptide hormones. Several have been sequenced (atrial natriuretic factor; brain natriuretic peptide; c-type natriuretic peptide).Arterial Pressure Regulation from the atria and ventricles
Functions of the natriuretic peptides:
Stimulate urinary Na+ excretion (known as “natriuresis”)
Water follows the Na+.
ANP also has counterregulatory actions to inhibit the RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones.
Summary
Changes in ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition are sensed by the juxtaglomerular apparatus, carotid-sinus and aortic-arch baroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus), and cardiac baroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus).
↑ Na+ causes ↑ ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition (↑ stretch), which results in:
↓ Renin release
↑ Natriuretic peptide release
End result: ↑ Na+ and water excretion
↓ Na+ causes ↓ ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition (↓ stretch), which results in:
↑ Renin release
↓ Natriuretic peptide release
End result: ↑ Na+ and water retention
Water Regulation
Overview
To excrete water, the urine is diluted, which requires:
Solute and fluid delivery to the kidney
Functioning diluting segments
Suppressed ADH
To retain free water, the urine is concentrated, which requires:
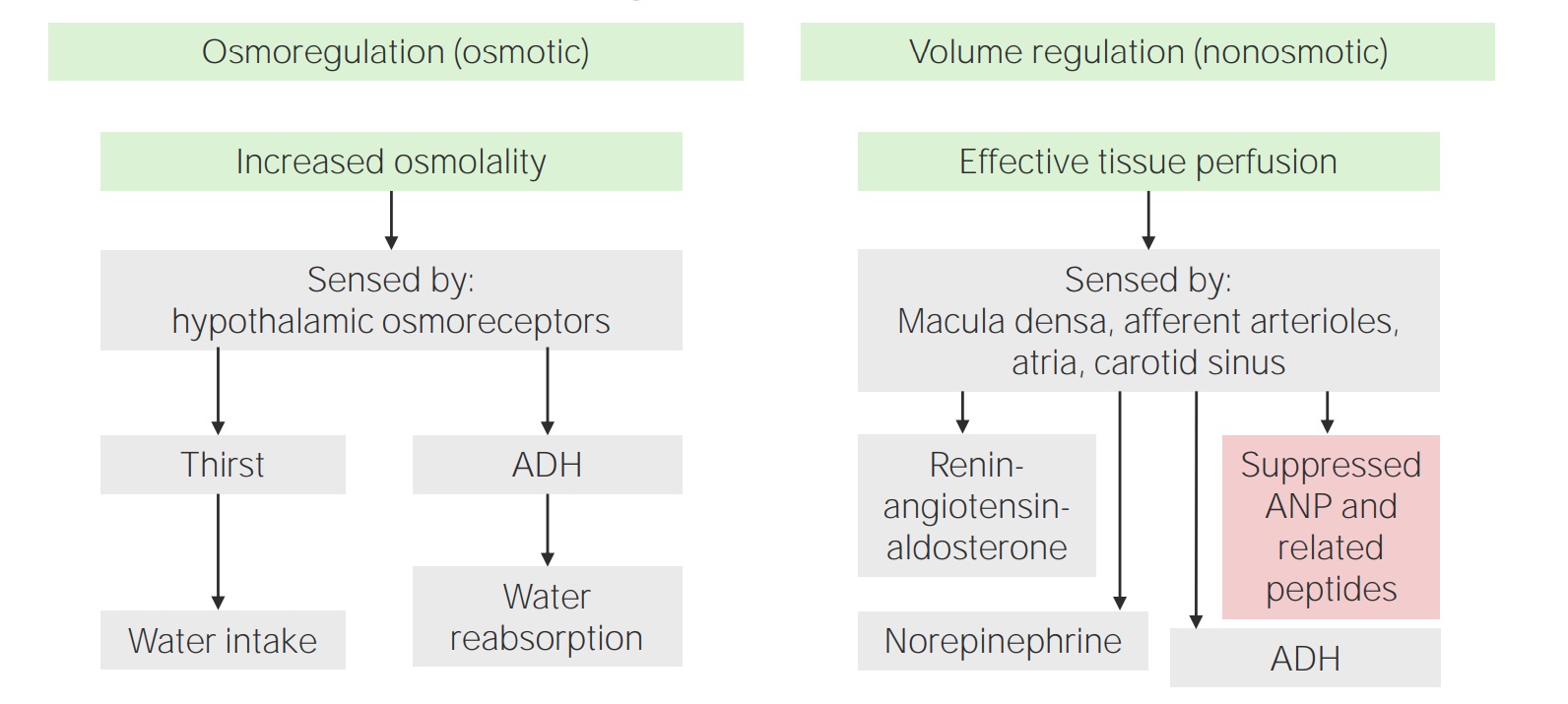
ADH can be released in response to osmotic and non-osmotic regulation.
Osmotic ADH regulation
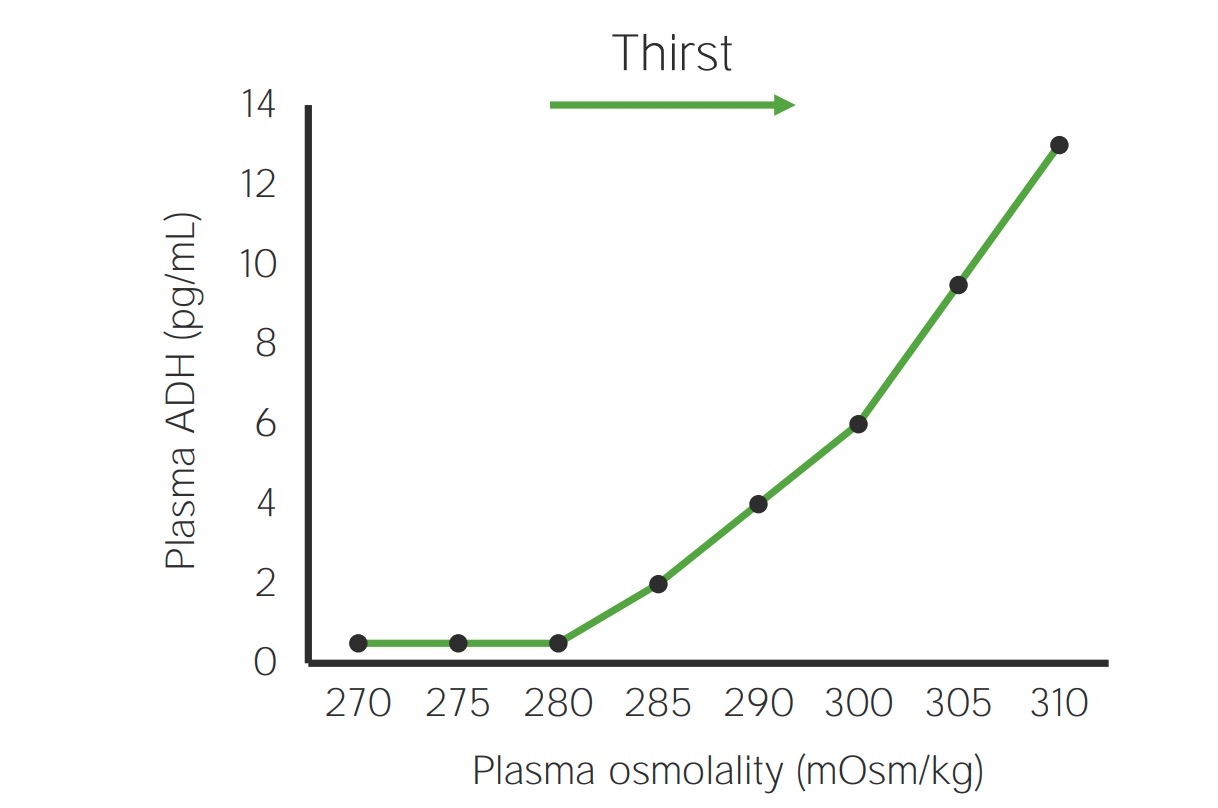
Water regulation is primarily controlled by osmoreceptors in the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus, which maintain plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration very tightly. Very small changes in plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration result in changes in ADH release and the sensation of thirst.
Osmoreceptors:
Located in the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus
↑ Plasma osmolalityPlasma osmolalityVolume Depletion and Dehydrationsensed by the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus triggers:
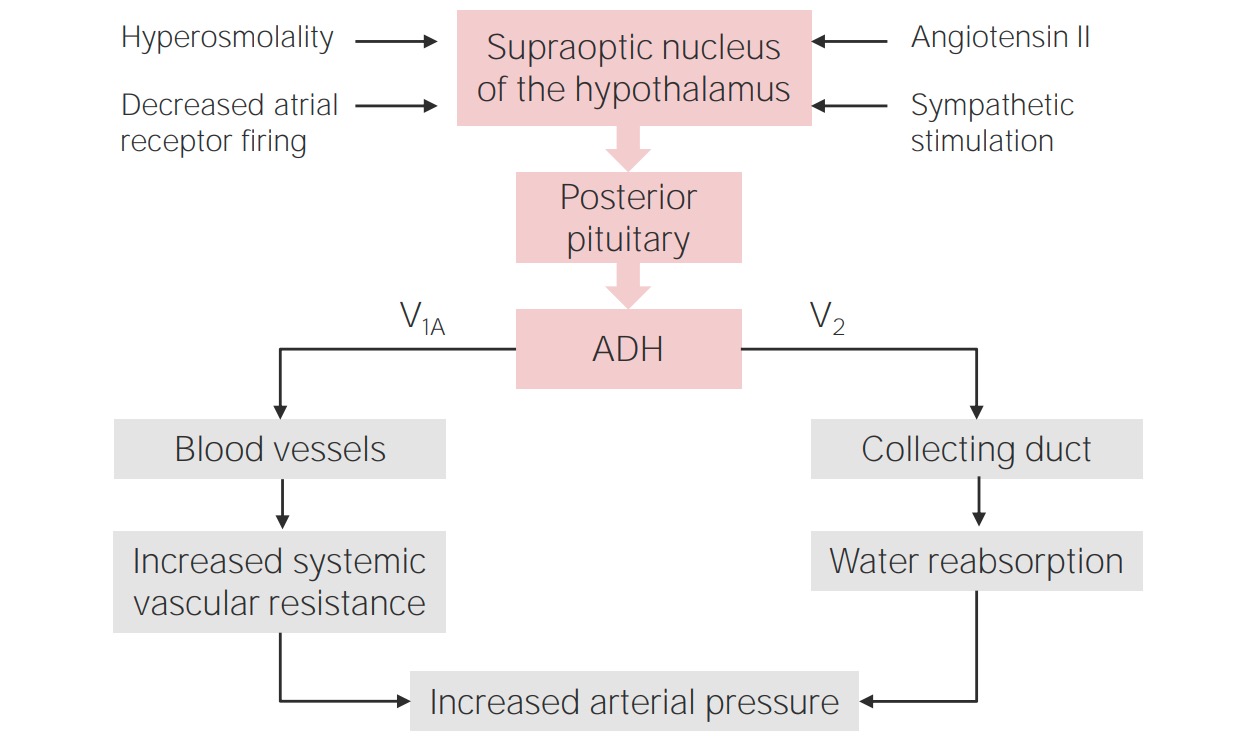
ADH release from the posterior pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types
Thirst
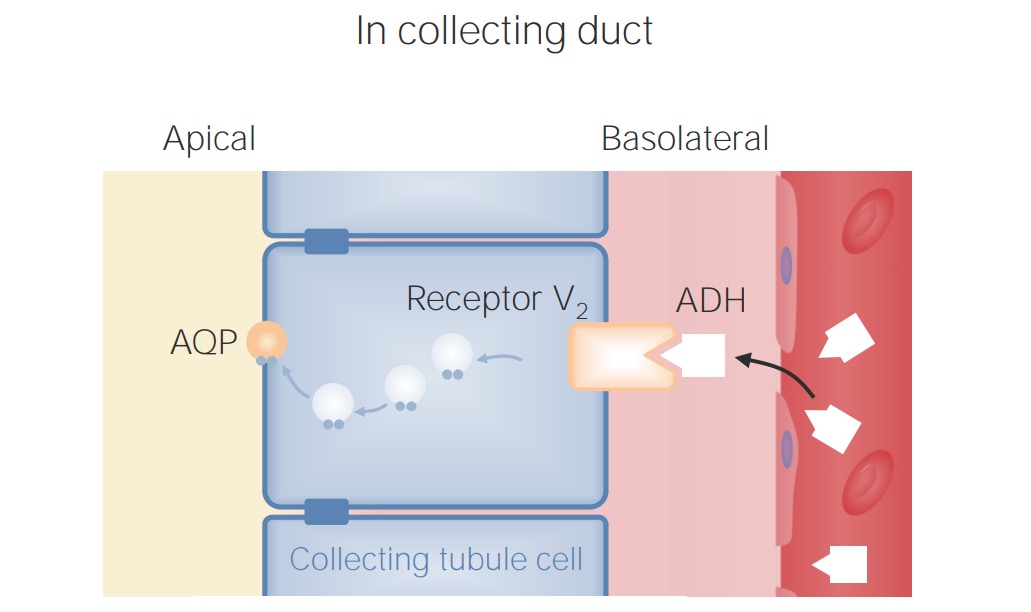
ADH binds to:
V2receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors on the basolateral membrane of collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma cells → stimulate insertion of aquaporin channelsChannelsThe Cell: Cell Membrane into the apical membrane
V1AreceptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors in vasculature → cause vasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure
Osmotic antidiuretic hormone (ADH) regulation: Slight increases in plasma osmolality stimulate ADH release in a linear fashion.
Image by Lecturio.
Location and function of the antidiuretic hormone (ADH) V2 receptor in the collecting ducts
AQP: Aquaporin Image by Lecturio.
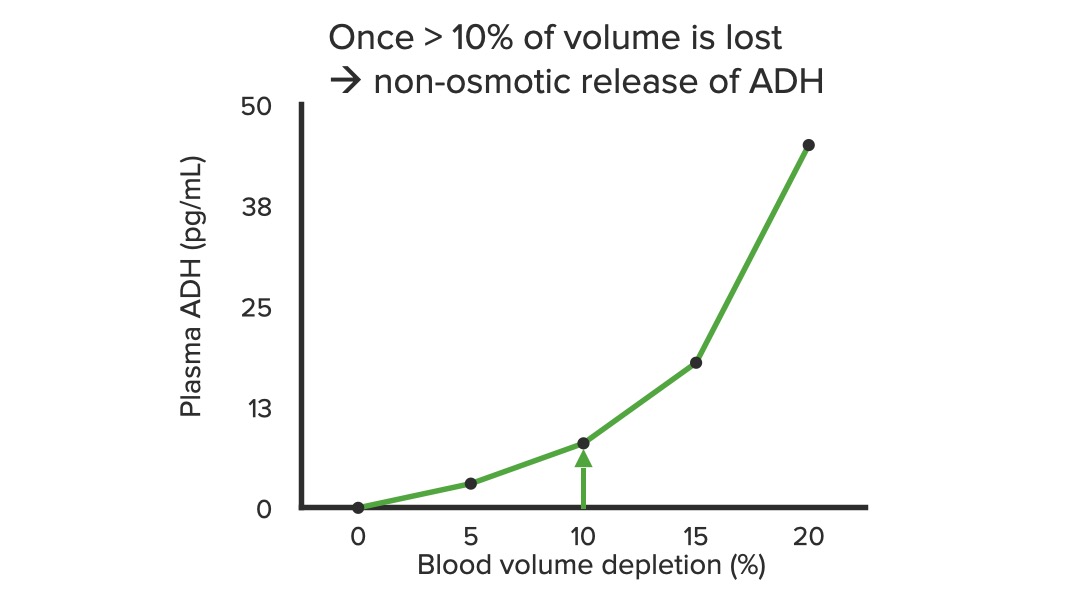
Non-osmotic ADH release
Very large decreases in the ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition can independently cause ADH release in an attempt to preserve volume.
Can occur even if plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products tonicity is not elevated
Occurs only in extreme settings, where ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition losses are high enough to cause hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension:
Acute severe bleeding
Severe diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Constitutes a salvage mechanism:
The body reabsorbs as much water as possible to support the BP when other mechanisms (e.g., RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones) are not sufficient.
↓ Volume will supersede a ↓ in osmolality: If the volume is low enough, ADH will be released even if the patient is already hypoosmotic.
↓ ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition is sensed by:
MaculaMaculaAn oval area in the retina, 3 to 5 mm in diameter, usually located temporal to the posterior pole of the eye and slightly below the level of the optic disk. It is characterized by the presence of a yellow pigment diffusely permeating the inner layers, contains the fovea centralis in its center, and provides the best phototropic visual acuity. It is devoid of retinal blood vessels, except in its periphery, and receives nourishment from the choriocapillaris of the choroid.Eye: Anatomy densa cells
Renal afferentAfferentNeurons which conduct nerve impulses to the central nervous system.Nervous System: HistologyarteriolesArteriolesThe smallest divisions of the arteries located between the muscular arteries and the capillaries.Arteries: Histology
Atrial and carotid sinusCarotid sinusThe dilated portion of the common carotid artery at its bifurcation into external and internal carotids. It contains baroreceptors which, when stimulated, cause slowing of the heart, vasodilatation, and a fall in blood pressure.Carotid Arterial System: AnatomybaroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus)
↓ ECVECVA procedure in which the physician attempts to manually rotate the fetus from a breech to a cephalic presentation by pushing on the maternal abdomenFetal Malpresentation and Malposition triggers:
Activation of the RAASRAASA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones
NorepinephrineNorepinephrinePrecursor of epinephrine that is secreted by the adrenal medulla and is a widespread central and autonomic neurotransmitter. Norepinephrine is the principal transmitter of most postganglionic sympathetic fibers, and of the diffuse projection system in the brain that arises from the locus ceruleus.Receptors and Neurotransmitters of the CNS release
HypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia: elevated sNa+ concentration, defined as Na+ levels > 145 mmol/L. The pathophysiology most commonly involves a lack of access to water (e.g., altered mental statusAltered Mental StatusSepsis in Children, dementiaDementiaMajor neurocognitive disorders (NCD), also known as dementia, are a group of diseases characterized by decline in a person’s memory and executive function. These disorders are progressive and persistent diseases that are the leading cause of disability among elderly people worldwide.Major Neurocognitive Disorders, mechanically ventilated patient). Another important etiology is diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus insipidus (DIDIDiabetes insipidus (DI) is a condition in which the kidneys are unable to concentrate urine. There are 2 subforms of di: central di (CDI) and nephrogenic di (NDI). Both conditions result in the kidneys being unable to concentrate urine, leading to polyuria, nocturia, and polydipsia.Arginine Vasopressin Disorders (Diabetes Insipidus)). Mild hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia is characterized by an increased sensation of thirst, whereas more severe hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia can result in altered mental statusAltered Mental StatusSepsis in Children. The etiology of hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia is often easy to determine based on clinical history. Treatment primarily involves replacement of the free water deficit.
DIDIDiabetes insipidus (DI) is a condition in which the kidneys are unable to concentrate urine. There are 2 subforms of di: central di (CDI) and nephrogenic di (NDI). Both conditions result in the kidneys being unable to concentrate urine, leading to polyuria, nocturia, and polydipsia.Arginine Vasopressin Disorders (Diabetes Insipidus): a cause of hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia due to increased urinary losses of water. DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus insipidus can be either central, due to decreased release of ADH, or nephrogenic, due to renal resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing to ADH. Without effective ADH, water cannot be effectively absorbed in the collecting ducts, leading to impaired urinary concentration and inappropriately dilute urine. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will present with polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation, nocturiaNocturiaFrequent urination at night that interrupts sleep. It is often associated with outflow obstruction, diabetes mellitus, or bladder inflammation (cystitis).Arginine Vasopressin Disorders (Diabetes Insipidus), polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus), hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia, and increased osmolality. Management may include desmopressinDesmopressinHemophilia (for central DIDIDiabetes insipidus (DI) is a condition in which the kidneys are unable to concentrate urine. There are 2 subforms of di: central di (CDI) and nephrogenic di (NDI). Both conditions result in the kidneys being unable to concentrate urine, leading to polyuria, nocturia, and polydipsia.Arginine Vasopressin Disorders (Diabetes Insipidus)), a low-Na+/low-protein diet, diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, and NSAIDsNSAIDSPrimary vs Secondary Headaches.
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: decreased sNa+ concentration, defined as Na+ levels < 135 mmol/L. The pathophysiology is more varied than hypernatremiaHypernatremiaHypernatremia is an elevated serum sodium concentration > 145 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled by the hypothalamus via the thirst mechanism and antidiuretic hormone (ADH) release. Hypernatremia occurs either from a lack of access to water or an excessive intake of sodium.Hypernatremia, but most commonly involves a dilution of the total body Na+ due to an increase in the total body waterTotal body waterBody Fluid Compartments. The clinical presentation varies greatly from asymptomatic to subtle cognitive deficits to seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures and death. Treatment is guided by acuity and severity of symptoms, and usually involves a combination of oral fluid restriction and hypertonic IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids. Overly rapid correction of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia can lead to an irreversible neurological complication known as the osmotic demyelinationDemyelinationMultiple Sclerosis syndrome.
Hypervolemia: an increase in ECF volume that occurs due to an increase in total body Na+. Clinical presentation includes hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema, ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites, pitting edemaPitting edemaEdema caused by excess fluid without excess colloid. Leaves “pits” due to fluid displacement when pressure is applied to the areaEdema in the lower extremities, and weight gain. Common etiologies include heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR), cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis, and renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome. In these diseases, the mechanisms of Na+ regulation are disturbed and the increased total body Na+ is not excreted. Treatment is with loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, which results in increased urinary Na+ and water losses.
HypovolemiaHypovolemiaSepsis in Children: a decrease in ECF volume that occurs due to a decrease in total body Na+. Clinical presentation includes hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension, decreased skin turgorSkin turgorMalnutrition in children in resource-limited countries, dry mucous membranes, orthostatic vital signs, and weight lossWeight lossDecrease in existing body weight.Bariatric Surgery. Common etiologies include diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, diuretic use, bleeding, poor oral intake, and 3rd spacing of fluids. Treatment includes administration of isotonic IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids, such as 0.9% NaCl or packed RBCsPacked RBCsTransfusion Products.