Oligohydramnios refers to amniotic fluid volume less than expected for the current gestational age. Oligohydramnios is diagnosed by ultrasound and defined as an amniotic fluid index (AFI) of ≤ 5 cm or a single deep pocket (SDP) of < 2 cm in the 2nd or 3rd trimester. Etiologies include uteroplacental insufficiency, drugs, fetal malformations (especially related to the renal/urinary systems), fetal chromosomal abnormalities, and maternal "toxoplasmosis, other agents, rubella, cytomegalovirus, and herpes simplex" (TORCH) infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease. Management involves close antenatal monitoring. Complications include pulmonary hypoplasiaHypoplasiaHypoplastic Left Heart Syndrome (HLHS), preterm delivery, and musculoskeletal deformities due to prolonged compressionCompressionBlunt Chest Trauma. Oligohydramnios is also frequently associated with growth restriction and fetal intolerance to labor, necessitating cesarean deliveryCesarean DeliveryCesarean delivery (CD) is the operative delivery of ≥ 1 infants through a surgical incision in the maternal abdomen and uterus. Cesarean deliveries may be indicated for a number of either maternal or fetal reasons, most commonly including fetal intolerance to labor, arrest of labor, a history of prior uterine surgery, fetal malpresentation, and placental abnormalities. Cesarean Delivery. PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual's condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas is extremely poor when diagnosed in the 1st and 2nd trimesters, but generally favorable in the 3rd trimester.
Decreased amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume for gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care is referred to as oligohydramnios. Oligohydramnios is diagnosed based on ultrasound measurements of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume and can be defined as either:
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity index (AFI) ≤ 5 cm
Single deep pocket (SDP) of < 2 cm
Anhydramnios is an extreme case of oligohydramnios with no measurable pockets of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity present.
Epidemiology
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency rates are highly variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables and based on gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care and associated risk factors.
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency rates based on gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care:
Overall incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in term pregnancies of 37–42 weeks: 4.4%
More common in pregnancies > 40 weeks: 11%
Less common in preterm pregnancies of < 37 weeks: < 1%
Most cases of oligohydramnios are diagnosed in the 3rd trimester of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care with no identifiable cause.
Pathophysiology and Etiology
Normal amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity production
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume is determined by the volume of fluid flowing into and out of the amniotic sac. The main contributors are:
Fetal urination (primary source of fluid 2nd half of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care)
Fetal swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility (removal of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity)
Lung secretions
Transport of maternal plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products across the fetal membranes as a result of hydrostatic and oncotic forces
Pathogenesis
Oligohydramnios is a result of decreased fluid production in relation to fluid removal.
Primarily due to ↓ fetal urine production in the 2nd half of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Note: Other physiologic alterations do not play significant roles in the development of oligohydramnios for the following reasons:
In general, ↑ swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility does not occur.
Lung secretions do not contribute enough to the amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume in the 2nd half of pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care to have an impact.
Transfer of fluid across the amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity is more successful in preventing polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios (excess amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity) than oligohydramnios (fluid outflow is easier than inflow).
↓ Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume → compressionCompressionBlunt Chest Trauma:
Abdominal compressionCompressionBlunt Chest Trauma (especially in the 2nd trimester) → limits movement of the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy → pulmonary hypoplasiaHypoplasiaHypoplastic Left Heart Syndrome (HLHS) (poor outcome)
Musculoskeletal deformities (e.g., club footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy, arthrogryposis)
Specific etiologies leading to oligohydramnios include:
IdiopathicIdiopathicDermatomyositis (possibly due to alterations in aquaporin channelsChannelsThe Cell: Cell Membrane in the fetal membranes and placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity)
Prelabor rupture of membranesPrelabor Rupture of MembranesPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies. Prelabor Rupture of Membranes (PROMPROMPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies.Prelabor Rupture of Membranes) with a “small/slow leak”
Placental insufficiencyPlacental InsufficiencyFailure of the placenta to deliver an adequate supply of nutrients and oxygen to the fetus.Neonatal Polycythemia: poor oxygenation and nutrient delivery to the fetus, resulting in poor urine production and often intrauterine growth restriction (IUGR):
Maternal vascular disease:
PreeclampsiaPreeclampsiaA complication of pregnancy, characterized by a complex of symptoms including maternal hypertension and proteinuria with or without pathological edema. Symptoms may range between mild and severe. Pre-eclampsia usually occurs after the 20th week of gestation, but may develop before this time in the presence of trophoblastic disease.Hypertensive Pregnancy Disorders
Chronic hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
Pregestational diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
CollagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology vascular disease
ThrombophiliasThrombophiliasHypercoagulable states (also referred to as thrombophilias) are a group of hematologic diseases defined by an increased risk of clot formation (i.e., thrombosis) due to either an increase in procoagulants, a decrease in anticoagulants, or a decrease in fibrinolysis.Hypercoagulable States
Placental abnormalitiesPlacental abnormalitiesNormal placental structure and function are essential for a healthy pregnancy. Some of the most common placental abnormalities include structural anomalies (such as a succenturiate lobe or velamentous cord insertion), implantation anomalies (such as placenta accreta and placenta previa), and functional anomalies (such as placental insufficiency). Placental Abnormalities:
Placental thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus
Chronic partial placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage
Maternal use of certain medications affecting renal blood flowRenal blood flowThe amount of the renal blood flow that is going to the functional renal tissue, i.e., parts of the kidney that are involved in production of urine.Glomerular Filtration:
Vascular anastomoses between 2 placentas, typically in monochorionic diamniotic twins, resulting in unequal blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure
Blood is siphoned from one twin to the other resulting in:
A growth-restricted “donor twin” with oligohydramnios and at risk for severe anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types
A “recipient twin” with polyhydramniosPolyhydramniosPolyhydramnios is a pathological excess of amniotic fluid. Common causes of polyhydramnios include fetal anomalies, gestational diabetes, multiple gestations, and congenital infections. Patients are often asymptomatic but may present with dyspnea, extremity swelling, or abdominal distention. Polyhydramnios and at risk for fetal hydropsHydropsCholecystitis (a form of heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR))
Other etiologies associated with oligohydramnios:
Fetal chromosomal abnormalities
Maternal infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
ToxoplasmosisToxoplasmosisToxoplasmosis is an infectious disease caused by Toxoplasma gondii, an obligate intracellular protozoan parasite. Felines are the definitive host, but transmission to humans can occur through contact with cat feces or the consumption of contaminated foods. The clinical presentation and complications depend on the host’s immune status. Toxoplasma/Toxoplasmosis, other agents, rubellaRubellaAn acute infectious disease caused by the rubella virus. The virus enters the respiratory tract via airborne droplet and spreads to the lymphatic system.Rubella Virus, cytomegalovirusCytomegalovirusCMV is a ubiquitous double-stranded DNA virus belonging to the Herpesviridae family. CMV infections can be transmitted in bodily fluids, such as blood, saliva, urine, semen, and breast milk. The initial infection is usually asymptomatic in the immunocompetent host, or it can present with symptoms of mononucleosis. Cytomegalovirus, and herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH Infections (TORCH) infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Parvovirus B19Parvovirus B19Primate erythroparvovirus 1 (generally referred to as parvovirus B19, B19 virus, or sometimes erythrovirus B19) ranks among the smallest DNA viruses. Parvovirus B19 is of the family Parvoviridae and genus Erythrovirus. In immunocompetent humans, parvovirus B19 classically results in erythema infectiosum (5th disease) or “slapped cheek syndrome.”Parvovirus B19
Fetal demise
Clinical Presentation and Diagnosis
Clinical presentation
↓ Uterine size for gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care (measured as the “fundal height” at prenatal visits)
↓ or inconsistent fetal movements
Complaints of leaking fluid/PROMPROMPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies.Prelabor Rupture of Membranes
Incidental finding in routine ultrasound examination (frequent)
History
The following should be elicited from an individual’s medical history:
History of conditions associated with vascular disease
Medication use
History of recent infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Physical examination
Fundal heights should be measured at each prenatal visit → poor fundal growth should be investigated further with ultrasound
Rule out ruptured membranes (speculum exam for pooling, fern test, pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance test of vaginal secretions).
Look for signs of maternal infection (e.g., feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, rashesRashesRashes are a group of diseases that cause abnormal coloration and texture to the skin. The etiologies are numerous but can include irritation, allergens, infections, or inflammatory conditions. Rashes that present in only 1 area of the body are called localized rashes. Generalized rashes occur diffusely throughout the body. Generalized and Localized Rashes).
Imaging: ultrasound
Amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity can be assessed quantitatively and qualitatively with ultrasound. For diagnosis, quantitative assessment is recommended by measuring AFI and/or SDP.
AFI:
Calculation: Divide the uterusUterusThe uterus, cervix, and fallopian tubes are part of the internal female reproductive system. The uterus has a thick wall made of smooth muscle (the myometrium) and an inner mucosal layer (the endometrium). The most inferior portion of the uterus is the cervix, which connects the uterine cavity to the vagina.Uterus, Cervix, and Fallopian Tubes: Anatomy into 4 quadrants, measure the largest vertical pocket of fluid in each quadrant, and add the values together.
Normal AFI: > 5 cm and < 24 cm
Oligohydramnios: ≤ 5 cm
SDP:
The vertical dimension of the largest pocket of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity; the SDP cannot include the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity or fetal parts
Normal SDP: ≥ 2 cm and < 8 cm
Oligohydramnios: < 2 cm
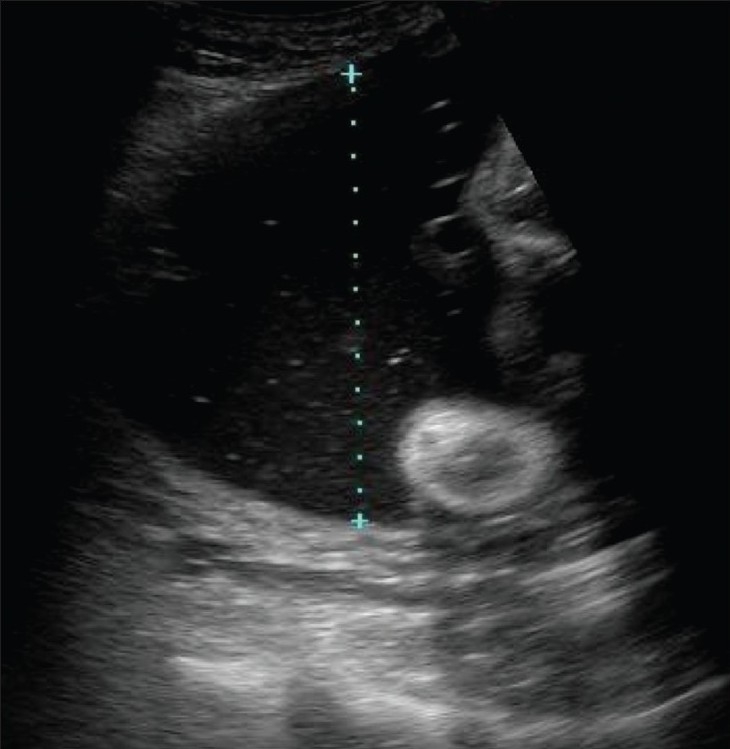
Ultrasound technique to measure a single vertical pocket of amniotic fluid:
Polyhydramnios (excess amniotic fluid) is present in the image.
Image: “Demonstration of the technique to measure a single vertical pocket of liquor. Hydramnios is present in this case” by Kinare A/The Indian journal of radiology & imaging. License: CC BY 2.0
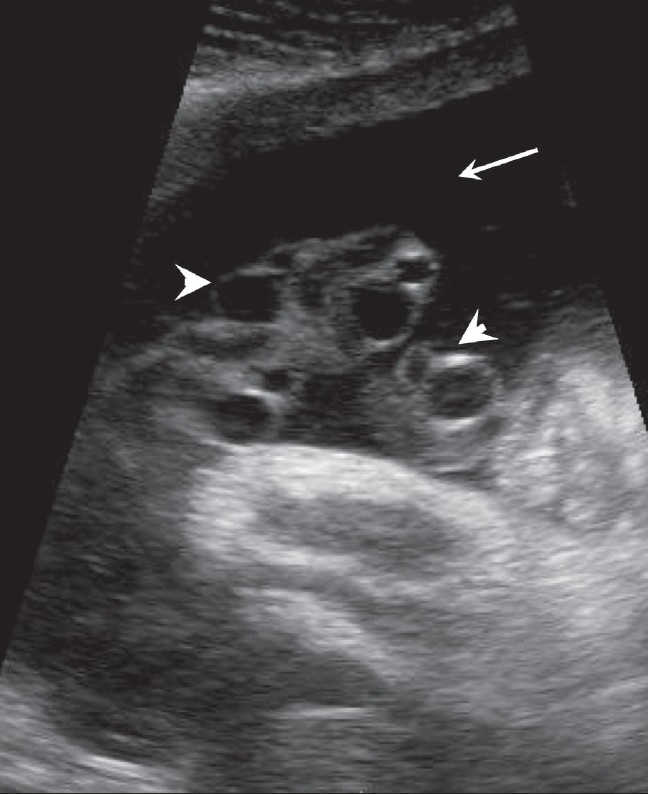
An amniotic fluid pocket (arrow) is seen on ultrasound containing loops of cord (arrowheads): The cord should be excluded when measuring amniotic fluid volume.
Image: “An amniotic fluid pocket (arrow) is seen containing loops of cord (arrowheads)” by Kinare A/The Indian journal of radiology & imaging. License: CC BY 2.0
Follow-up testing
If a patient is diagnosed with oligohydramnios, additional testing may be indicated to identify the underlying etiology:
Ultrasound to assess fetal growth:
Always indicated
IUGR points to uteroplacental insufficiencyUteroplacental InsufficiencyUteroplacental insufficiency may be acute or chronic and refers to the inability of the placenta to deliver a sufficient supply of O2 and nutrients to the fetusPlacental Abnormalities
Fetal anatomical survey via ultrasound (if not already done) to look for fetal anomalies
Noninvasive prenatal testing (NIPT): screen for fetal DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure fragments in maternal blood
AmniocentesisAmniocentesisPercutaneous transabdominal puncture of the uterus during pregnancy to obtain amniotic fluid. It is commonly used for fetal karyotype determination in order to diagnose abnormal fetal conditions.Polyhydramnios: an invasive samplingInvasive samplingCoccidioides/Coccidioidomycosis of amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity (contains fetal DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure) to test for genetic anomalies
If suspicion arises based on the clinical picture, test maternal serum and amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity for TORCH pathogens.
Management
Antenatal management
No effective long-term treatment for oligohydramnios is available.
Results are typically transient but still may provide some benefits.
Monitor regularly to ensure continued fetal well-being.
Monitoring techniques:
Fetal “kick counting” by the mother: The mother should feel 10 movements in a 2-hour time period at least 1x/day.
Fetal nonstress test: monitors fetal heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology and uterine contractions for 20 minutes
Biophysical profileBiophysical ProfileObstetric Imaging: an obstetric ultrasound to identify certain types of fetal movements (includes a fluid measurement)
Once oligohydramnios is diagnosed, a nonstress test and biophysical profileBiophysical ProfileObstetric Imaging are typically performed 1–2x/week.
Delivery
Delivery is typically indicated:
After 36‒37 weeks’ gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care (regardless of etiology)
At 34-weeks gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with preterm prelabor rupture of membranesPrelabor Rupture of MembranesPrelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to the rupture of the amniotic sac before the onset of labor. Prelabor rupture of membranes may occur in term or preterm pregnancies. Prelabor Rupture of Membranes (PPROM)
If monitoring is nonreassuring
Route of delivery:
Vaginal deliveries are preferred if patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are candidates.
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be carefully monitored in labor for signs of fetal distress.
Cesarean or operative vaginal deliveries should be performed for typical obstetric indications, including nonreassuring intrapartum fetal monitoringFetal monitoringThe primary goals of antepartum testing and monitoring are to assess fetal well-being, identify treatable situations that may cause complications, and evaluate for chromosomal abnormalities. These tests are divided into screening tests (which include cell-free DNA testing, serum analyte testing, and nuchal translucency measurements), and diagnostic tests, which provide a definitive diagnosis of aneuploidy and include chorionic villus sampling (CVS) and amniocentesis.Antepartum Testing and Monitoring.
May be helpful when monitoring indicates fetal stress from repetitive compressionCompressionBlunt Chest Trauma of the umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity (seen on the monitor as variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables decelerations)
The catheter also serves as an intrauterine pressure catheter (IUPC), which is capable of measuring the strength of uterine contractions (helpful in managing inductions of labor).
The fetal/neonatal prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas depends on the cause, severity, gestational ageGestational ageThe age of the conceptus, beginning from the time of fertilization. In clinical obstetrics, the gestational age is often estimated as the time from the last day of the last menstruation which is about 2 weeks before ovulation and fertilization.Pregnancy: Diagnosis, Physiology, and Care at diagnosis, and duration of oligohydramnios.
First trimester
Ominous finding typically ending with spontaneous abortionAbortionExpulsion of the product of fertilization before completing the term of gestation and without deliberate interference.Spontaneous Abortion (94%)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be counseled regarding the probabilityProbabilityProbability is a mathematical tool used to study randomness and provide predictions about the likelihood of something happening. There are several basic rules of probability that can be used to help determine the probability of multiple events happening together, separately, or sequentially.Basics of Probability and signs of miscarriageMiscarriageSpontaneous abortion, also known as miscarriage, is the loss of a pregnancy before 20 weeks’ gestation. However, the layperson use of the term “abortion” is often intended to refer to induced termination of a pregnancy, whereas “miscarriage” is preferred for spontaneous loss.Spontaneous Abortion.
Serial ultrasound exams should be done to follow the natural history of the process.
No treatments are available.
Second trimester
Pregnancies with borderline or low–normal amniotic fluidAmniotic fluidA clear, yellowish liquid that envelopes the fetus inside the sac of amnion. In the first trimester, it is likely a transudate of maternal or fetal plasma. In the second trimester, amniotic fluid derives primarily from fetal lung and kidney. Cells or substances in this fluid can be removed for prenatal diagnostic tests (amniocentesis).Placenta, Umbilical Cord, and Amniotic Cavity volume generally have a good prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas:
Obtain serial sonographic examinations to assess the progress of the disease.
True oligohydramnios typically has a poor prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas.
Survival rates based on etiology:
PPROM: 21%
Placental abruptionPlacental AbruptionPremature separation of the normally implanted placenta from the uterus. Signs of varying degree of severity include uterine bleeding, uterine muscle hypertonia, and fetal distress or fetal death.Antepartum Hemorrhage: 22%
Fetal growth restrictionFetal growth restrictionFetal growth restriction (FGR), also known as intrauterine fetal growth restriction (IUGR), is an estimated fetal weight (EFW) or abdominal circumference < 10th percentile for gestational age. The term small for gestational age (SGA) is sometimes erroneously used interchangeably with FGR. Fetal Growth Restriction: 0%
Overall survival rate: 10%
Pulmonary hypoplasiaHypoplasiaHypoplastic Left Heart Syndrome (HLHS) is typically the cause of death because little can be done to support respirationRespirationThe act of breathing with the lungs, consisting of inhalation, or the taking into the lungs of the ambient air, and of exhalation, or the expelling of the modified air which contains more carbon dioxide than the air taken in.Nose Anatomy (External & Internal) in the infant after delivery.
Limb contracturesContracturesProlonged shortening of the muscle or other soft tissue around a joint, preventing movement of the joint.Wound Healing are common due to long-standing compressionCompressionBlunt Chest Trauma.
Depending on the clinical situation (e.g., severe oligohydramnios due to an anomaly identified on an 18-week anatomy scan), elective termination may be an appropriate option.
Third trimester
Typically a better prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas when diagnosed in the 3rd trimester due to more developed respiratory and renal organs
Uteroplacental insufficiencyUteroplacental InsufficiencyUteroplacental insufficiency may be acute or chronic and refers to the inability of the placenta to deliver a sufficient supply of O2 and nutrients to the fetusPlacental Abnormalities
Meconium aspirationMeconium AspirationA condition caused by inhalation of meconium into the lung of fetus or newborn, usually due to vigorous respiratory movements during difficult parturition or respiratory system abnormalities. Meconium aspirate may block small airways leading to difficulties in pulmonary gas exchange and aspiration pneumonia.Physical Examination of the Newborn
Overall survival rate: > 85%
Neonatal complications
PrematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis birth
Meconium aspirationMeconium AspirationA condition caused by inhalation of meconium into the lung of fetus or newborn, usually due to vigorous respiratory movements during difficult parturition or respiratory system abnormalities. Meconium aspirate may block small airways leading to difficulties in pulmonary gas exchange and aspiration pneumonia.Physical Examination of the Newborn
Arthrogryposis (contracturesContracturesProlonged shortening of the muscle or other soft tissue around a joint, preventing movement of the joint.Wound Healing of multiple joints)
Alteration in the shape of the skullSkullThe skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium.Skull: Anatomy
TorticollisTorticollisA symptom, not a disease, of a twisted neck. In most instances, the head is tipped toward one side and the chin rotated toward the other. The involuntary muscle contractions in the neck region of patients with torticollis can be due to congenital defects, trauma, inflammation, tumors, and neurological or other factors.Cranial Nerve Palsies (i.e. wry neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess)
Club footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy
AmputationAmputationAn amputation is the separation of a portion of the limb or the entire limb from the body, along with the bone. Amputations are generally indicated for conditions that compromise the viability of the limb or promote the spread of a local process that could manifest systemically. Amputation of the limb
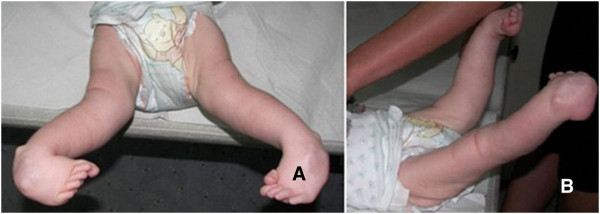
Arthrogryposis as seen in an infant:
Congenital contractures that can result from decreased intrauterine movement and oligohydramnios.
A: front view B: lateral view
Image: “Lower limbs at the age of 14 weeks” by Binkiewicz-Glinska A et al. License: CC BY 2.0
Cunningham, F. G., Leveno, K. J., et al. (2010). Williams Obstetrics (23rd ed. Pp.495‒498).
Bachhav, A.A., and Waikar, M. (2013). Low amniotic fluid index at term as a predictor of adverse perinatal outcome. Journal of Obstetrics & Gynecology of India. 64(2):120-123. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3984654/
Create your free account or log in to continue reading!