Liddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the "collecting tubule sodium channel" or "amiloride-sensitive sodium channel." The activity of ENAC is increased, leading to sodium and water retention. Liddle syndrome presents with the classic triad of resistant hypertension at an early age, hypokalemia, and metabolic alkalosis, which mimics the symptoms of primary aldosteronism; however, this syndrome is associated with low plasma aldosterone levels. Diagnosis is based on history and physical examination, blood and urinalysis, and genetic testing. Management is by using potassium-sparing diuretics and restricting dietary sodium. Treatment delay can lead to serious cardiovascular and renal complications. The prognosis is good if Liddle syndrome is treated early.
Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is a rare autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance genetic disorder associated with abnormal increased function of epithelial sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiachannelsChannelsThe Cell: Cell Membrane (ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome) in the collecting tubulesCollecting tubulesStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of Bellini) which opens on the summit of the papilla.Kidneys: Anatomy. Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is clinically characterized by hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, low plasma renin activityPlasma renin activityRenal Artery Stenosis, metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, and low aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia levels.
Epidemiology[1,3,4]
Extremely rare disorder reported in < 80 families
Overall population prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency is unknown.
Individuals may remain asymptomatic for up to 40 years, but Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome can also be diagnosed as early as 12 years in a majority of cases.
Often remains undiagnosed
Etiology[1–5,7]
An autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance gain-of-function gene mutationGene MutationMyotonic Dystrophies changes the structure of an ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome subunit and also affects the region of the protein involved in signaling for its breakdown, which is normally controlled by aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia.
SCNN1A: encodes the alpha subunit of the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome
SCNN1B: encodes the beta subunit of the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome
SCNN1G: encodes the gamma subunit of the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome
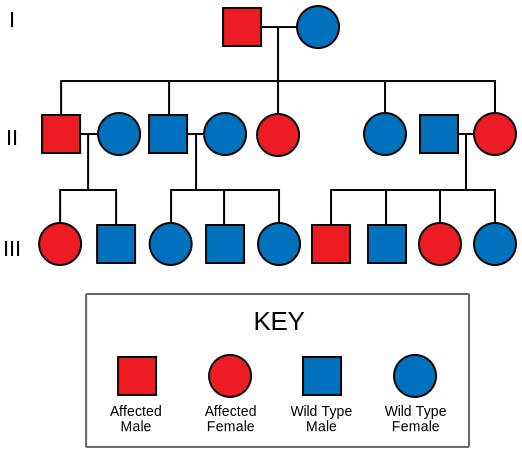
The autosomal dominant inheritance of Liddle syndrome
MutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations occurs in the SCNN1A, SCNN1B, and SCNN1GgenesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure that encode the alpha, beta, and gamma subunits of the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome.
Normally located on the epithelial cell surface of the:
KidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy (collecting tubule)
LungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Sweat glandsSweat glandsSweat-producing structures that are embedded in the dermis. Each gland consists of a single tube, a coiled body, and a superficial duct.Soft Tissue Abscess
Dysregulation of the ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome follows due to structural changes in the respective subunits.
Domain change in the channel → ↓ internalization and degradation of ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle SyndromechannelsChannelsThe Cell: Cell Membrane (by the ubiquitin-proteasome pathway)
Inability to degrade the channelsChannelsThe Cell: Cell Membrane → ↑ presence of the channel in the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma → ↑ Na reabsorption, resulting in:
↑ Water reabsorption and hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia is responsible for controlling the number of Na channelsChannelsThe Cell: Cell Membrane. Loss of this ability in Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome → ↓ in channel degradation → hyperaldosteronism-like state (but occurs independently of aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia)
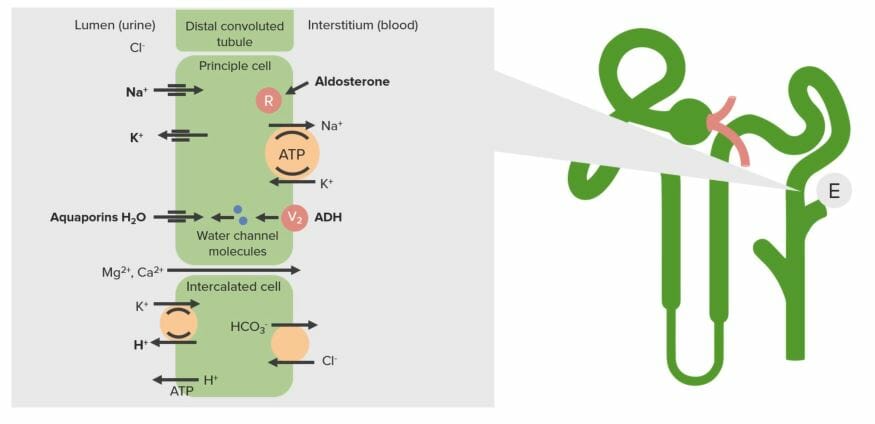
The transport system of the renal collecting duct (E): In Liddle syndrome, an increase in sodium channels on the apical surface (lumen side) results in increased sodium reabsorption. This sodium is transported back to the blood via the Na+/K+-ATPase on the basolateral side, resulting in an increase in intracellular potassium. This potassium is then secreted via potassium channels on the apical surface.
Image by Lecturio.
Clinical Presentation and Diagnosis
Clinical presentation[6,7]
Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is rare and has a presentation similar to many other syndromes associated with mineralocorticoid excessMineralocorticoid excessA hereditary disease characterized by childhood onset hypertension, hypokalemic alkalosis, and low renin and aldosterone secretion. It results from a defect in the activity of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which results in inadequate conversion of cortisol to cortisone. The build up of unprocessed cortisol to levels that stimulate mineralocorticoid receptors creates the appearance of having excessive mineralocorticoids.Metabolic Alkalosis. Thus, Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is often misdiagnosed or remains undetected.
The classic triad of the presentation includes:
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension:
Early onset
Long-standing
Often severe or resistant
Associated features:
Intermittent headaches
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia symptoms:
Weakness
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Exercise intolerance
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes:
Prominent U waves
Inverted/flattened T waves
ST-segment depression
T- and U-wave fusion
Metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis
Diagnosis
The preliminary diagnosis of Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is based mainly on suspicion resulting from the clinical presentation. It is also important to:
Consider family historyFamily HistoryAdult Health Maintenance of early-onset hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension with or without hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
Rule out other causes of hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, and metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis.
Laboratory findings:[6,7]
↓ PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsreninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation
↓ PlasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsaldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia (may also be normal)
↓ Urine aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia
↓ Urine Na
↑ Urinary K (or normal)
Urine aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:K ratio < 60 ng/mmol (would show ↑ K secretionSecretionCoagulation Studies from an ↑ Na resorption independent of aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia drive; note that findings may vary based on salt intake and volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols)
Serum electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes:
↑ Na
↓ K (or normal)
↑ HCO3 (or normal)
Genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies:
Should be considered in individuals with a family historyFamily HistoryAdult Health Maintenance of Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome and in those in whom this condition is suspected.
Full sequencing the SCNN1A, SCNN1B, and SCNN1G genesGenesA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.DNA Types and Structure is the most accurate way to identify Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle SyndromemutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations.
Clinical response to spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics and triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics:[7]
If the clinical picture is unclear, the following can potentially discriminate Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome from other forms of hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension associated with low reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia:
A 3-week trial of spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics 100 mg/day should have no effect on plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ or blood pressure.
A 3-week trial of triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics 100 mg/day (or amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome 10 mg/ day) should correct plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ and blood pressure.
This is rarely done (time-consuming).
Not appropriate for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with normal K levels.
The following recommendations are based on a current review of the international literature.
Treatment
Early diagnosis of Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome leads to resolution or control of the disorder, enabling the affected individual to lead a normal life.
Act by blocking ENaCENaCSodium channels found on salt-reabsorbing epithelial cells that line the distal nephron; the distal colon; salivary ducts; sweat glands; and the lung. They are amiloride-sensitive and play a critical role in the control of sodium balance, blood volume, and blood pressure.Liddle Syndrome activity:
AmilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome
TriamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics
Used to treat hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension while resolving hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia and metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis
Salt restriction: < 2 g NaCl/day
Conventional hypertensive therapies are ineffective as initial treatment but may be needed in refractory cases after hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia is resolved.[7]
ACE inhibitorsACE inhibitorsTruncus Arteriosus, ARBsARBsAgents that antagonize angiotensin receptors. Many drugs in this class specifically target the angiotensin type 1 receptor.Heart Failure and Chronic Coronary Syndrome Medication, beta-blockersBeta-blockersDrugs that bind to but do not activate beta-adrenergic receptors thereby blocking the actions of beta-adrenergic agonists. Adrenergic beta-antagonists are used for treatment of hypertension, cardiac arrhythmias, angina pectoris, glaucoma, migraine headaches, and anxiety.Class 2 Antiarrhythmic Drugs (Beta Blockers), and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes channel blockers are generally ineffective alone (Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is aldosterone-independent).
These medications can be adjuncts in resistant hypertensionResistant hypertensionBlood pressure that remains uncontrolled despite concurrent use of 3 antihypertensive agents of different classes.Uncontrolled Hypertension but are not recommended to be used as monotherapy.
Renal transplantation:
Resolves the disorder completely
Typically not warranted unless the diagnosis is made later in life.
Table: DiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication used in the treatment of Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome
Medication
Adult dosing
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care considerations
AmilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome[7,8]
Initiate: 5–10 mg/day by mouth
Titrate up every 1–2 weeks to the lowest effective dose.
Maximum: 40 mg/day
Typical effective dose: 10–30 mg daily
Case reports (only a few available) have not shown significant maternal or
fetal effects during treatment of other similar conditions (e.g., Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome, Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome, primary aldosteronism)
TriamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics[7,9]
Initiate: 50–100 mg/day by mouth
Titrate up weekly to the lowest effective dose.
Maximum: 300 mg/day in divided doses
Typical effective dose: 100–300 mg daily
Folic acid antagonist
Not recommended during pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Complications[4,6,7]
Owing to its rare occurrence and similarity of symptoms to those of other disorders associated with mineralocorticoid excessMineralocorticoid excessA hereditary disease characterized by childhood onset hypertension, hypokalemic alkalosis, and low renin and aldosterone secretion. It results from a defect in the activity of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which results in inadequate conversion of cortisol to cortisone. The build up of unprocessed cortisol to levels that stimulate mineralocorticoid receptors creates the appearance of having excessive mineralocorticoids.Metabolic Alkalosis, Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome is often misdiagnosed, which may cause an increase in the occurrence of complications:
Hypertensive retinopathyRetinopathyDegenerative changes to the retina due to hypertension.Alport Syndrome
NephrosclerosisNephrosclerosisHardening of the kidney due to infiltration by fibrous connective tissue (fibrosis), usually caused by renovascular diseases or chronic hypertension. Nephrosclerosis leads to renal ischemia.Liddle Syndrome
Cerebral ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage leading to cerebrovascular accidents
Chronic renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[4,6,7]
Early diagnosis and treatment are key in the prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas of Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome.
Adequate treatment → good prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas
Delayed detection → delay in therapy → manifestation as major cardiovascular and renal complications
Differential Diagnosis
Primary hyperaldosteronismPrimary hyperaldosteronismAutonomous (renin-independent) secretion of aldosterone.Hyperaldosteronism: also known as Conn’s syndrome. Primary hyperaldosteronismPrimary hyperaldosteronismAutonomous (renin-independent) secretion of aldosterone.Hyperaldosteronism is characterized by the excess production of aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia (high), which results in low reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation levels. Primary hyperaldosteronismPrimary hyperaldosteronismAutonomous (renin-independent) secretion of aldosterone.Hyperaldosteronism is caused by primary adrenal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation or adrenal adenomaAdrenal AdenomaCushing Syndrome and presents with hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, muscle weakness, muscle spasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy, polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation, and headaches. Diagnosis is based on clinical history, examination, and laboratory testing. Management includes adrenalectomyAdrenalectomyExcision of one or both adrenal glands.Cushing Syndrome and therapy with spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics.
Apparent mineralocorticoid excessMineralocorticoid excessA hereditary disease characterized by childhood onset hypertension, hypokalemic alkalosis, and low renin and aldosterone secretion. It results from a defect in the activity of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which results in inadequate conversion of cortisol to cortisone. The build up of unprocessed cortisol to levels that stimulate mineralocorticoid receptors creates the appearance of having excessive mineralocorticoids.Metabolic Alkalosis: a rare autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance disorder that presents with hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, and low plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsreninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation. Diagnosis is made by calculating the ratio of free urinary cortisolCortisolGlucocorticoids to free urinary cortisoneCortisoneA naturally occurring glucocorticoid that has been used in replacement therapy for adrenal insufficiency and as an anti-inflammatory agent. Cortisone itself is inactive; it is converted in the liver to the active metabolite hydrocortisone.Glucocorticoids, which is higher in affected individuals. Management includes aldosterone antagonistsAldosterone antagonistsDrugs that bind to and block the activation of mineralocorticoid receptors by mineralocorticoids such as aldosterone.Heart Failure and Chronic Coronary Syndrome Medication, such as spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics.
Glucocorticoid resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing: a familial disease characterized by reduced cortisolCortisolGlucocorticoids effects due to a glucocorticoid receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors defect countered by hyperactivityHyperactivityAttention Deficit Hyperactivity Disorder of the hypothalamic–pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types–adrenal axis. Affected individuals present with signs of adrenal overproduction of mineralocorticoidsMineralocorticoidsMineralocorticoids are a drug class within the corticosteroid family and fludrocortisone is the primary medication within this class. Fludrocortisone is a fluorinated analog of cortisone. The fluorine moiety protects the drug from isoenzyme inactivation in the kidney, allowing it to exert its mineralocorticoid effect.Mineralocorticoids—hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, hypokalemic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, hirsutismHirsutismA condition observed in women and children when there is excess coarse body hair of an adult male distribution pattern, such as facial and chest areas. It is the result of elevated androgens from the ovaries, the adrenal glands, or exogenous sources. The concept does not include hypertrichosis, which is an androgen-independent excessive hair growth.Polycystic Ovarian Syndrome in women, male-pattern baldnessBaldnessAlopecia is the loss of hair in areas anywhere on the body where hair normally grows. Alopecia may be defined as scarring or non-scarring, localized or diffuse, congenital or acquired, reversible or permanent, or confined to the scalp or universal; however, alopecia is usually classified using the 1st 3 factors.Alopecia, and menstrual irregularities. Diagnosis is based on high cortisolCortisolGlucocorticoids levels and normal-to-high adrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones (ACTH) levels. Management is using mineralocorticoid-sparing synthetic glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids to suppress ACTH secretionSecretionCoagulation Studies.
Renovascular hypertensionRenovascular hypertensionHypertension due to renal artery obstruction or compression.Renal Artery Stenosis: a condition caused by narrowing or occlusion of the renal arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology and/or their branches, often due to atherosclerosisAtherosclerosisAtherosclerosis is a common form of arterial disease in which lipid deposition forms a plaque in the blood vessel walls. Atherosclerosis is an incurable disease, for which there are clearly defined risk factors that often can be reduced through a change in lifestyle and behavior of the patient. Atherosclerosis or fibromuscular dysplasiaFibromuscular dysplasiaFibromuscular dysplasia (FMD) is a nonatherosclerotic, noninflammatory, medium-sized angiopathy due to fibroplasia of the vessel wall. The condition leads to complications related to arterial stenosis, aneurysm, or dissection. Fibromuscular Dysplasia. The clinical presentation of renovascular hypertensionRenovascular hypertensionHypertension due to renal artery obstruction or compression.Renal Artery Stenosis includes hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, renal dysfunction, and pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema caused by activation of the renin-angiotensin-aldosterone systemRenin-angiotensin-aldosterone systemA blood pressure regulating system of interacting components that include renin; angiotensinogen; angiotensin converting enzyme; angiotensin i; angiotensin ii; and angiotensinase. Renin, an enzyme produced in the kidney, acts on angiotensinogen, an alpha-2 globulin produced by the liver, forming angiotensin I. Angiotensin-converting enzyme, contained in the lung, acts on angiotensin I in the plasma converting it to angiotensin II, an extremely powerful vasoconstrictor. Angiotensin II causes contraction of the arteriolar and renal vascular smooth muscle, leading to retention of salt and water in the kidney and increased arterial blood pressure. In addition, angiotensin II stimulates the release of aldosterone from the adrenal cortex, which in turn also increases salt and water retention in the kidney. Angiotensin-converting enzyme also breaks down bradykinin, a powerful vasodilator and component of the kallikrein-kinin system.Adrenal Hormones. Tests show possibly hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia with high reninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia. Diagnosis is based on renal imagingRenal imagingThe renal system is composed of 2 kidneys, 2 ureters, a bladder, and a urethra. Varying conditions such as infections, cysts, solid masses, ischemia, and mechanical obstruction can affect the renal system. Evaluation of diseases rely on imaging methods such as radiography, ultrasonography, CT, and MRI. Some of these are also used to guide tissue sampling (e.g., renal biopsy).Imaging of the Urinary System, such as duplex ultrasonographyDuplex ultrasonographyUltrasonography applying the doppler effect combined with real-time imaging. The real-time image is created by rapid movement of the ultrasound beam. A powerful advantage of this technique is the ability to estimate the velocity of flow from the doppler shift frequency.Hypercoagulable States. Management is by surgical intervention.
Billing and Coding
Diagnosis Codes:
Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome, a rare inherited form of hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, is classified under secondary hypertensionSecondary hypertensionHypertension as it has a specific, identifiable cause (a genetic mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in a kidney sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia channel).
The workup for Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome involves tests to differentiate it from other causes of hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension with hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia. Codes are used for metabolic panels, measuring plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductsreninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation and aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia levels (which are low in Liddle), and genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies.
ReninReninA highly specific (leu-leu) endopeptidase that generates angiotensin I from its precursor angiotensinogen, leading to a cascade of reactions which elevate blood pressure and increase sodium retention by the kidney in the renin-angiotensin system.Renal Sodium and Water Regulation
CPT
82088
AldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia
Medications:
These codes are used to prescribe the specific potassium-sparing diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication, amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome or triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics, which directly block the overactive sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia channel and are the definitive treatment for Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome. Note that spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics is ineffective.
Coding System
Code
Description
RxNorm
722
AmilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome (ingredient)
RxNorm
10785
TriamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics (ingredient)
Complications:
This primary code is used to document the severe, early-onset hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension that is the hallmark of the disease and the primary driver of its morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status if left untreated.
Coding System
Code
Description
ICD-10-CM
I11.9
Hypertensive heart disease without heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
Zennaro, M.-C., Boulkroun, S., Fernandes-Rosa, F. (2015). Inherited forms of mineralocorticoid hypertension. Best Practice & Research Clinical Endocrinology & Metabolism, 29(4), 633–645. https://doi.org/10.1016/j.beem.2015.04.010
Al Shibli, A., Narchi, H. (2015). Bartter and Gitelman syndromes: spectrum of clinical manifestations caused by different mutations. World Journal of Methodology, 5(2), 55–61. https://pubmed.ncbi.nlm.nih.gov/26140272/
Yamaguchi, E., et al. (2018). Liddle’s-like syndrome associated with nephrotic syndrome secondary to membranous nephropathy: the first case report. BMC Nephrology, 19, 122. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5966895/
Create your free account or log in to continue reading!