HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia is defined as a decreased serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (sNa+) concentration less than 135 mEq/L. Serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia is the greatest contributor to plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration, which is very tightly controlled via antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (ADH) release from the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus and by the thirst mechanism. The basic pathophysiology of all etiologies of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia is an abnormal relative increase in total body waterTotal body waterBody Fluid Compartments (TBWTBWBody Fluid Compartments), which dilutes the total body sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (TBNa+) concentration. The clinical presentation varies greatly, from asymptomatic to subtle cognitive deficits, seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures, and death. Management is guided by etiology, acuity, and duration of symptoms, usually involving oral fluid restriction or administration of IV fluidsIV fluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids that contain Na. SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia must be replaced slowly, as overly rapid correction of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia can lead to irreversible neurologic complications and death, known as osmotic demyelinationDemyelinationMultiple Sclerosis syndrome (ODS).
Note: SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) has a separate clinical concept page.
A normal serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (sNa+) concentration is 135–145 mEq/L (mmol/L).
Na+ is the most important contributor to plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation.
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia is defined as an sNa+ concentration < 135 mEq/L.
Overt neurologic symptoms, most often in an sNa+ levels < 120 mEq/L, but note that:
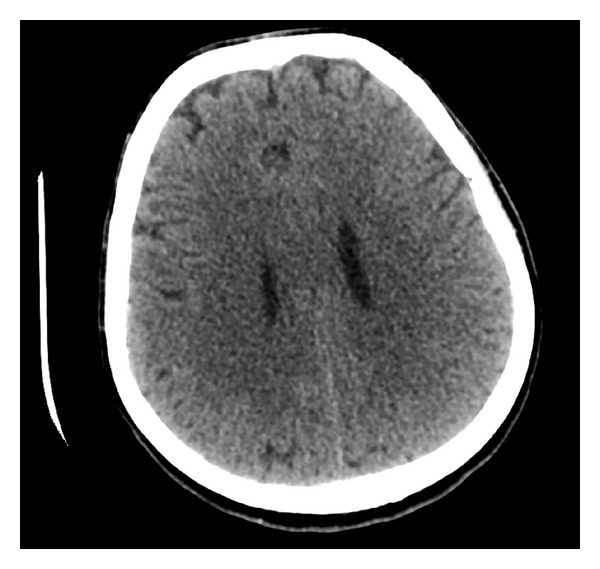
Neurologic symptoms occur due to cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP) and are dependent on both severity and rate of onset of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Severe symptoms (e.g., seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures, comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma) are more likely at levels < 120 mEq/L or with rapid onset, but symptoms can occur even at higher levels in susceptible patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
EuvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH): normal TBNa+ with ↑ in TBWTBWBody Fluid Compartments (modest increase in extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments volume, but not enough to cause edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema)
The most common electrolyte abnormality encountered in clinical practice
Occurs in up to 22% of hospitalized patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship (commonly caused by administration of hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation fluids)
Etiology[1,4]
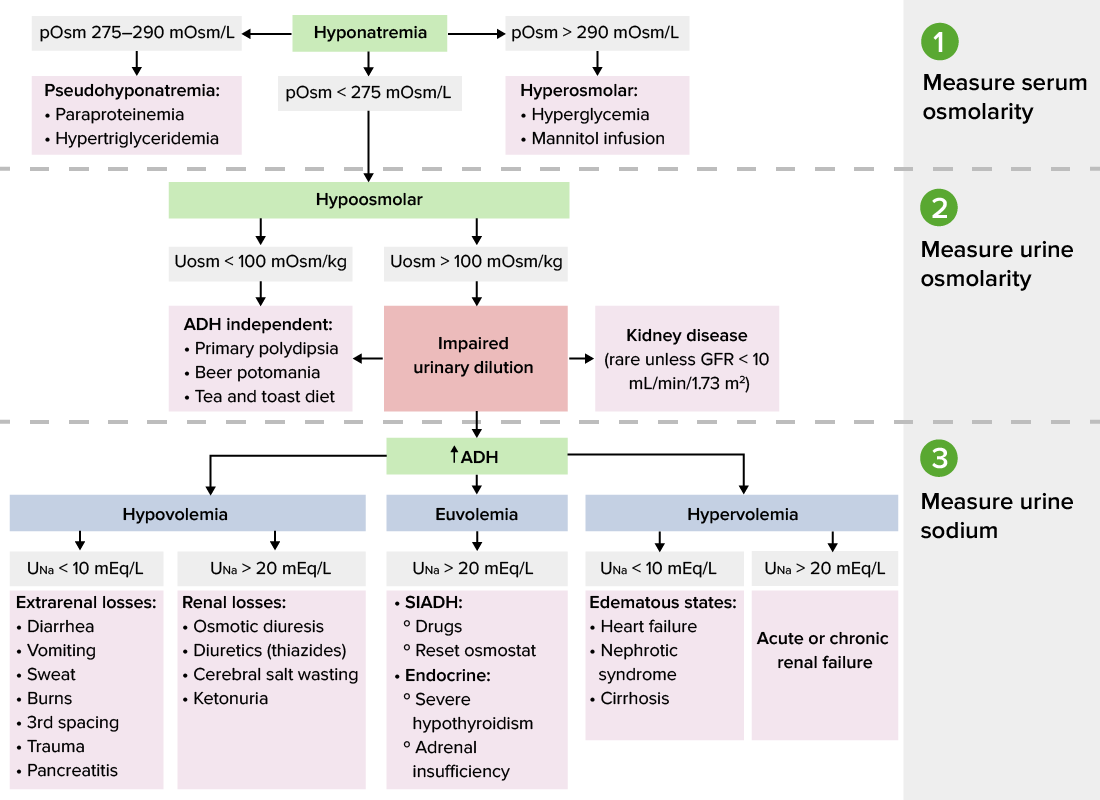
The etiology of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia is determined by knowing the volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols, as well as the serum and urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation.
Hypovolemic:
GI losses (diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, nasogastric tubeNasogastric tubeMalnutrition in children in resource-limited countries (NG tube)/surgical drain output)
↑ Insensible lossesInsensible lossesLoss of water by diffusion through the skin and by evaporation from the respiratory tract.Volume Depletion and Dehydration (tachypneaTachypneaIncreased respiratory rate.Pulmonary Examination, sweating, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, burnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns)
Third-spacing (pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis)
SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Primary polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus) (psychogenic polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus))
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) (HF)
CirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
Nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome
Advanced renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia usually reflects an excess of total body waterTotal body waterBody Fluid Compartments and not a deficiency in total body sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia.[2,4,7,8]
ADH is usually the reason the kidney excretes less water than is taken in.
Antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (ADH, vasopressin) is synthesized by the hypothalamusHypothalamusThe hypothalamus is a collection of various nuclei within the diencephalon in the center of the brain. The hypothalamus plays a vital role in endocrine regulation as the primary regulator of the pituitary gland, and it is the major point of integration between the central nervous and endocrine systems.Hypothalamus; it is stored and is released from the pituitaryPituitaryA small, unpaired gland situated in the sella turcica. It is connected to the hypothalamus by a short stalk which is called the infundibulum.Hormones: Overview and Types gland.
Acts on the V2-type receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors in the collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma in the kidney
Minor volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration can still stimulate ADH release.
The purpose is to maintain blood pressure at all costs.
It occurs even if plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation is normal or low.
ADH also has systemic vasoconstrictor effects.
When intake of water is greater than excretion water → ↑ TBWTBWBody Fluid Compartments (disproportionately to sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia, leading to dilutional hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia) → net dilution of TBNa+
In inappropriate ADH secretionSecretionCoagulation Studies, total body waterTotal body waterBody Fluid Compartments increases (exceeding kidney’s ability to excrete free water) and serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia becomes diluted, leading to euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
In case of CHF or cirrhosis, there is low “effective” volume detected by baroreceptorsBaroreceptorsReceptors in the vascular system, particularly the aorta and carotid sinus, which are sensitive to stretch of the vessel walls.Arginine Vasopressin Disorders (Diabetes Insipidus), and due to this, ADH is stimulated causing hypervolemic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Clinical Presentation
Acute (< 48 hours)[6–9,12]
Symptoms are due to acute shift of water into the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification → cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
Relatively smaller drop in serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia (sNa+) sufficient to cause symptoms (i.e., sNa+ approximately 130 mEq/L)
Mild symptoms:
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
LethargyLethargyA general state of sluggishness, listless, or uninterested, with being tired, and having difficulty concentrating and doing simple tasks. It may be related to depression or drug addiction.Hyponatremia
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Severe symptoms:
SeizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures
HerniationHerniationOmphalocele → comaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma, respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure, death
Chronic (> 48 hours)[7–9,12]
BrainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification adaptation to hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia:
Occurs quickly (within approximately 48 hours)
BrainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification cells excrete solutes (“organic osmolytes”) to equalize the tonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation.
Results in much lower degree of fluid shiftFluid ShiftTranslocation of body fluids from one compartment to another, such as from the vascular to the interstitial compartments. Fluid shifts are associated with profound changes in vascular permeability and water-electrolyte imbalance. The shift can also be from the lower body to the upper body as in conditions of weightlessness.Volume Depletion and Dehydration into the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification
Symptoms are more subtle due to brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification adaptations:
Urinary sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration
Note: If someone is presenting with severe symptoms, do not wait for diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests before starting urgent treatment.
↑ Plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration (> 290 mOsm/L): hypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water RegulationhyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
Water shifts out of the cells.
Serum Na+ does not correlate with plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation.
Examples: hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus, mannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics infusion, radiocontrast
Note in hyperglycemia, use the “Correction Factor”: for every 100 mg/dL of glucose above normal, the measured sodium is “falsely” low by about 1.6 mEq/L.
Serum Na+ does not correlate with plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation.
Examples: ↑ serum lipidsLipidsLipids are a diverse group of hydrophobic organic molecules, which include fats, oils, sterols, and waxes.Fatty Acids and Lipids or protein, lab errorErrorRefers to any act of commission (doing something wrong) or omission (failing to do something right) that exposes patients to potentially hazardous situations.Disclosure of Information
No further workup or management
↓ Plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration (< 275 mOsm/L): hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water RegulationhyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia → check urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation
Serum Na+ correlates with plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation.
True hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
Urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation < 100 mOsm/kg: ADH appropriately suppressed
Low solute intake
Primary polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus)
Urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation > 100 mOsm/kg: ADH present/active → check urine sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration
Urinary sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration[7,8,11,15]
Bicarbonaturia (with renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis and metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis)
UNa < 10 mEq/L (varies by text, some use a cutoff of < 20 mEq/L): extrarenal losses:
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
3rd spacing of fluids
Trauma
BurnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns
PancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
EuvolemiaEuvolemiaVolume Depletion and Dehydration (no edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema): UNa> 20 mEq/L:
Glucocorticoid deficiency
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism
Stress
Drugs
Syndrome of inappropriate antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.HypernatremiasecretionSecretionCoagulation Studies (SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH))
UNa > 20 mEq/L: acute or chronic renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
UNa < 10 mEq/L (varies by text, some use a cutoff of < 20 mEq/L):
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
CirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
Nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome
Note: UNa cutoff values vary depending on the literature source (generally, ranges from 20 to 40 mEq/L).
Clinical estimation of volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols estimation is not always reliable , especially in older adults, hospitalized patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship, or those with multiple comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus. If clinical volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols is clearly hypovolemic or hypervolemic, further testing may be limited to supportive labs. In euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) or unclear cases, additional testing is essential to confirm diagnosis and guide therapy.
Screen for hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism and adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease (cortisolCortisolGlucocorticoids, adrenocorticotropic hormoneAdrenocorticotropic hormoneAn anterior pituitary hormone that stimulates the adrenal cortex and its production of corticosteroids. Acth is a 39-amino acid polypeptide of which the n-terminal 24-amino acid segment is identical in all species and contains the adrenocorticotropic activity. Upon further tissue-specific processing, acth can yield alpha-msh and corticotropin-like intermediate lobe peptide (clip).Adrenal Hormones (ACTH) stimulation test)
Review medication list for common offenders
Review history for common nonosmotic ADH stimuli
Check additional labs:
Urine Na+: ↓ suggests hypovolemiaHypovolemiaSepsis in Children, ↑ suggests SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
BNPBNPA peptide that is secreted by the brain and the heart atria, stored mainly in cardiac ventricular myocardium. It can cause natriuresis; diuresis; vasodilation; and inhibits secretion of renin and aldosterone. It improves heart function. It contains 32 amino acids.Renal Sodium and Water Regulation: ↓ suggests hypovolemiaHypovolemiaSepsis in Children
Serum uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis: ↓ suggests SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
BUN: ↓ suggests SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Fluid challenge with repeat urine studies if diagnosis is still unclear
Diagnosis of underlying condition[7,8,11]
SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH):
Excessive levels of ADH result in excessive renal free water reabsorption.
ADH release can be stimulated by many causes:
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, anxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder, stress
Centrally acting medications, CNS disorders
Postoperative state
MalignancyMalignancyHemothorax (most commonly small cell lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung Cancer)
Lung disorders (i.e., pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia)
Primary polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus) and low solute intake:
Water intake in excess of kidney’s maximal excretion capabilities
Highly dependent on dietary solute intake and the concept of obligate osmolar excretion
HypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism and thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.Hyponatremia induced: The mechanisms are incompletely understood.
HF/cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis/nephrotic syndromeNephrotic syndromeNephrotic syndrome is characterized by severe proteinuria, hypoalbuminemia, and peripheral edema. In contrast, the nephritic syndromes present with hematuria, variable loss of renal function, and hypertension, although there is sometimes overlap of > 1 glomerular disease in the same individual. Nephrotic Syndrome: nonosmotic release of ADH due to the kidney’s perceptionPerceptionThe process by which the nature and meaning of sensory stimuli are recognized and interpreted.Psychiatric Assessment of a hypovolemic state
Advanced renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome:
Water intake in excess of kidney’s impaired excretion capabilities
Only in very severe renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome (usually GFRGFRThe volume of water filtered out of plasma through glomerular capillary walls into Bowman’s capsules per unit of time. It is considered to be equivalent to inulin clearance.Kidney Function Tests < 15 mL/min)
Usually clinically obvious and not requiring comprehensive workup
Management varies depending on practice location. The following information was compiled from US, European, and UK literature and guidelines.[3,7,8]
General considerations
Acuity and severity of symptoms are the primary determinants of this, and the aggressiveness and urgency of treatment will vary according to the risk assessmentRisk assessmentThe qualitative or quantitative estimation of the likelihood of adverse effects that may result from exposure to specified health hazards or from the absence of beneficial influences.Preoperative Care.
Acuity:[7,11,18]
Acute (< 48 hours):
Adaptive mechanisms have not yet occurred:
↑ Risk for acute cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia should be corrected quickly (i.e., within 24 hours)
Chronic (> 48 hours):
Adaptive mechanisms have occurred:
↑ Risk for ODS
↓ Risk for acute cerebral edemaCerebral edemaIncreased intracellular or extracellular fluid in brain tissue. Cytotoxic brain edema (swelling due to increased intracellular fluid) is indicative of a disturbance in cell metabolism, and is commonly associated with hypoxic or ischemic injuries. An increase in extracellular fluid may be caused by increased brain capillary permeability (vasogenic edema), an osmotic gradient, local blockages in interstitial fluid pathways, or by obstruction of CSF flow (e.g., obstructive hydrocephalus).Increased Intracranial Pressure (ICP)
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia must be corrected slowly (i.e., < 6–8 mEq/L/day).
If unknown, then hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia must always be assumed to be chronic!
Symptom severity:[7,11]
Severe:
Includes:
Seizure
ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. Coma
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
Mostly nonspecific symptoms (headacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, confusion)
Nonsevere cases usually do not need urgent treatment with 3% NaCl.
Specific risk factors for ODS:[7]
MalnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
AlcoholismAlcoholismA primary, chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be continuous or periodic.Wernicke Encephalopathy and Korsakoff Syndrome
sNa+ < 105 mEq/L on presentation
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Urgent therapy (severe symptoms)
General measures:[6]
Seek early support from an endocrinologist or nephrologist.
The decision to treat with hypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation fluid should be the responsibility of a senior clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship with appropriate training and experience.
Ensure a treatment environment where close monitoring is possible (e.g., ICUICUHospital units providing continuous surveillance and care to acutely ill patients.West Nile Virus).
Goals:[11,12]
Initial goal: ↑ serum Na+ by 4–6 mEq/L within the 1st 6 hours
Should resolve any acute symptoms caused by hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
If symptoms persist, then investigate other etiologies.
Subsequent goals:
↑ in serum Na+ by no more than 6–8 mEq/L/day, particularly if at risk of ODS (limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation varies based on guideline, but generally < 8–10 mEq/L/day)[7]
Hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia:[6–8,11]
Symptomatic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
100–150 mL IV 3% NaCl bolus over 10–20 minutes:
Consider using weight-based (2 mL/kg) preparations for people with extreme body compositions
May repeat bolus up to 2 additional times to relieve symptoms.
Serum Na+ level every 20 minutes until symptoms resolve, then every 2–4 hours (some articles recommend every 1–2 hours)
Fluid status (volume overload can occur, particularly if the patient has underlying heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR) or cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis)
Neurologic status
Urine output
If symptoms do not improve, explore other causes.
Once initial goal reached:[7]
Stop hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia infusion.
Desmopressin → some clinicians give this in conjunction with hypertonic saline to avoid overcorrection in high risk patients (“DDAVP clamp” stops the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy from dumping water, controlling sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia increase)
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia that does not require urgent therapy is almost exclusively chronic and usually asymptomatic or mildly symptomatic.
Management decisions are guided by the severity of the sNa+ level, with wide variation in the clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship’s preferences for aggressiveness of treatments.
Monitoring of sNa+ levels is indicated in all cases.
Moderate (sNa+ 125–130 mEq/L): based on clinical judgmentJudgmentThe process of discovering or asserting an objective or intrinsic relation between two objects or concepts; a faculty or power that enables a person to make judgments; the process of bringing to light and asserting the implicit meaning of a concept; a critical evaluation of a person or situation.Psychiatric Assessment
Loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication (furosemideFurosemideA benzoic-sulfonamide-furan. It is a diuretic with fast onset and short duration that is used for edema and chronic renal insufficiency.Loop Diuretics, bumetanideBumetanideA sulfamyl diuretic.Loop Diuretics, torsemideTorsemideA pyridine and sulfonamide derivative that acts as a sodium-potassium chloride symporter inhibitor. It is used for the treatment of edema associated with congestive heart failure; chronic renal insufficiency; and liver diseases. It is also used for the management of hypertension.Loop Diuretics)
General measures:
Oral fluid restriction
Discontinue offending medications
Liberal salt diet not recommended (potential for worsening fluid overload)
Oral fluid restriction (500–800 mL/day, if possible)
Liberal salt diet
Discontinue offending medications.
Address any nonosmotic ADH stimuli (painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, anxietyAnxietyFeelings or emotions of dread, apprehension, and impending disaster but not disabling as with anxiety disorders.Generalized Anxiety Disorder, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).).
Additional therapies (consider discussion with specialist before use):
Oral solute tablets → for euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
Loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication → also used for SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
VasopressorVasopressorAcute CholangitisreceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonists (vaptans) → for euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) or hypervolemic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
Syndrome of inappropriate secretionSecretionCoagulation Studies of antidiuretic hormoneAntidiuretic hormoneAntidiuretic hormones released by the neurohypophysis of all vertebrates (structure varies with species) to regulate water balance and osmolarity. In general, vasopressin is a nonapeptide consisting of a six-amino-acid ring with a cysteine 1 to cysteine 6 disulfide bridge or an octapeptide containing a cystine. All mammals have arginine vasopressin except the pig with a lysine at position 8. Vasopressin, a vasoconstrictor, acts on the kidney collecting ducts to increase water reabsorption, increase blood volume and blood pressure.Hypernatremia (SIADHSIADHSyndrome of inappropriate antidiuretic hormone secretion (SIADH) is a disorder of impaired water excretion due to the inability to suppress the secretion of antidiuretic hormone (ADH). SIADH is characterized by impaired water excretion leading to dilutional hyponatremia, which is mainly asymptomatic but may cause neurologic symptoms. SSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)): an inappropriately high level of circulating ADH. Etiology includes medications, malignancies, lung disease, HIVHIVAnti-HIV Drugs, hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism, intracranial processes, and nonosmotic stimuli. Management is water restriction.
Other euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) hyponatremias: thiazide-induced hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, adrenal insufficiencyAdrenal InsufficiencyConditions in which the production of adrenal corticosteroids falls below the requirement of the body. Adrenal insufficiency can be caused by defects in the adrenal glands, the pituitary gland, or the hypothalamus.Adrenal Insufficiency and Addison Disease, and hypothyroidismHypothyroidismHypothyroidism is a condition characterized by a deficiency of thyroid hormones. Iodine deficiency is the most common cause worldwide, but Hashimoto’s disease (autoimmune thyroiditis) is the leading cause in non-iodine-deficient regions. Hypothyroidism are causes of euvolemicEuvolemicSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia that have incompletely understood mechanisms. Such conditions can be diagnosed relatively easily (medication list review, cortisolCortisolGlucocorticoids/ACTH stimulation test, and thyroid-stimulating hormoneThyroid-stimulating hormoneA glycoprotein hormone secreted by the adenohypophysis. Thyrotropin stimulates thyroid gland by increasing the iodide transport, synthesis and release of thyroid hormones (thyroxine and triiodothyronine).Thyroid Hormones (TSH)). If a condition is found, treating the underlying condition should correct the hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Osmotic demyelinationDemyelinationMultiple Sclerosis syndrome (ODS): characterized by irreversible neurologic symptoms, which can occur if sNa+ is corrected too quickly. Symptoms occur several days after the overcorrectionOvercorrectionVolume Depletion and Dehydration and are related to fluid shifts after the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification has already adapted to chronic hyponatremiaChronic HyponatremiaSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). Diagnosis is by history and MRI. Management involves therapeutic lowering of the sNa+ and supportive care.
HypertonicHypertonicSolutions that have a greater osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water RegulationhyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia: low sNa+, but not managed as true hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia because the sNa+ is discordant with the plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration and tonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation. Examples are hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus and mannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics use. Water is drawn into the extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (ECF) and results in a dilution of the sNa+, despite the plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration remaining high from the glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance or mannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics.
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia in advanced renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome: when plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration is high but the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation and sNa+ are low. UreaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea Cycle is in high concentrations but is an ineffective osmole, so it causes no water shifts, dilution of the TBNa+, or decrease in the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion ProductstonicityTonicityPlasma tonicity refers to the concentration of only the osmotically active solutes in bloodRenal Sodium and Water Regulation. Advanced renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome causes a decrease in water excretion, retention of water, increased TBWTBWBody Fluid Compartments, diluted TBNa+, and a true hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water RegulationhyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia.
Pseudohyponatremia: occurs when a characteristic lab errorErrorRefers to any act of commission (doing something wrong) or omission (failing to do something right) that exposes patients to potentially hazardous situations.Disclosure of Information results in a low measured sNa+, despite the true sNa+ and true plasma osmolalityPlasma osmolalityVolume Depletion and Dehydration being within the normal range. High serum lipid (i.e., hypertriglyceridemiaHypertriglyceridemiaA condition of elevated levels of triglycerides in the blood.Lipid Disorders associated with pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, hypercholesterolemiaHypercholesterolemiaA condition with abnormally high levels of cholesterol in the blood. It is defined as a cholesterol value exceeding the 95th percentile for the population.Lipid Disorders with biliary obstruction) or protein levels (plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products cell dyscrasias) result in inaccuracy in lab processing and falsely low reported sNa+.
Water intoxication: a true acute hyponatremiaAcute HyponatremiaSyndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) that may have significant symptoms with a relatively small decrease in sNa+, which will require rapid correction of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia with 3% NaCl. Etiologies are psychogenic polydipsiaPolydipsiaExcessive thirst manifested by excessive fluid intake. It is characteristic of many diseases such as diabetes mellitus; diabetes insipidus; and nephrogenic diabetes insipidus. The condition may be psychogenic in origin.Arginine Vasopressin Disorders (Diabetes Insipidus), exercise-associated hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, fraternity hazing rituals, and MDMAMDMAAn n-substituted amphetamine analog. It is a widely abused drug classified as a hallucinogen and causes marked, long-lasting changes in brain serotonergic systems. It is commonly referred to as mdma or ecstasy.Stimulants abuse. These patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must be monitored very closely.
Billing and Coding
Diagnosis Codes:
This code is used to diagnose hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, a condition of low sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia concentration in the blood, which is the most common electrolyte disorder in hospitalized patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Coding System
Code
Description
ICD-10-CM
E87.1
Hypo-osmolality and hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia
SNOMED CT
267437009
HyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (disorder)
Evaluation & Workup:
These codes are for the essential lab tests to determine the cause of hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia, which involves assessing the patient’s volume statusVolume StatusACES and RUSH: Resuscitation Ultrasound Protocols and measuring serum osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation, urine osmolalityOsmolalityPlasma osmolality refers to the combined concentration of all solutes in the blood.Renal Sodium and Water Regulation, and urine sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia.
SodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia; urine
Medications:
This code is for hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia (3% NaCl), which is used for the emergent treatment of severe, symptomatic hyponatremiaHyponatremiaHyponatremia is defined as a decreased serum sodium (sNa+) concentration less than 135 mmol/L. Serum sodium is the greatest contributor to plasma osmolality, which is very tightly controlled via antidiuretic hormone (ADH) release from the hypothalamus and by the thirst mechanism.Hyponatremia (e.g., with seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures) to rapidly but cautiously raise the serum sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.Hyponatremia level.
Coding System
Code
Description
HCPCS
J7131
Injection, hypertonic salineHypertonic salineHypertonic sodium chloride solution. A solution having an osmotic pressure greater than that of physiologic salt solution (0. 9 g NaCl in 100 ml purified water).Hyponatremia solution, 1 ml
Ball, S., Barth, J., Levy, M. (2016). Society for Endocrinology endocrine emergency guidance: emergency management of severe symptomatic hyponatremia in adult patients. Endocrine Connections, 5(5), G4–G6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5314809/
Spasovski, G., Vanholder, R., et al.(2014). Clinical practice guideline on diagnosis and treatment of hyponatraemia, European Journal of Endocrinology, 170(3), G1–G47. https://pubmed.ncbi.nlm.nih.gov/24569125/
Braun, M. M., Barstow, C. H., Pyzocha, N. J. (2015). Diagnosis and management of sodium disorders: hyponatremia and hypernatremia. American Family Physician, 91(5), 299–307. https://www.aafp.org/pubs/afp/issues/2015/0301/p299.html
Seay, N. W., Lehrich, R. W., Greenberg, A. (2019). Diagnosis and management of disorders of body tonicity—hyponatremia and hypernatremia: core curriculum 2020. American Journal of Kidney Diseases, 75(2), 272–286. https://www.ajkd.org/article/S0272-6386(19)30943-6/fulltext